Download presentation
Presentation is loading. Please wait.

1
Disorders of Small and Large Bowel
Jay Green October 26, 2006

2
Case 1 54 y.o. F, abdominal pain
Started 2 days ago, shortly after Big Mac Hurts all over, comes and goes, crampy +D yesterday, bloated, +N today, ø V PMH: DMII, HTN, TAH/BSO (’04) Ideas? Comes every few minutes, lasts a few minutes Crescendo-decrescendo No BM since yesterday ?not passing gas?, not sure
 Ideas Comes every few minutes, lasts a few minutes. Crescendo-decrescendo. No BM since yesterday. not passing gas , not sure.")
3
DDx - Approach Think anatomy Think VITAMIN D, VINDICATED, whatever…
Intraperitonaeal, retroperitoneal, other Think VITAMIN D, VINDICATED, whatever… Vascular Ischemic gut, MI, AAA Infection Gastro, PUD, psoas abscess Neoplastic Intussusception Inflammatory Diverticulitis, Cholecystitis, Pancreatitis, Appendicitis Traumatic Obstruction Pregnancy Other – implies external to these two Why intussusception under neoplastic?

5
Small Bowel Obstruction
Top 3 causes? Hernia Adhesions CA Most likely to cause strangulation? Hernia – often closed loop Others to think about? Gallstone ileus, volvulus, intussusception, abscess, hematoma, foreign body Adhesions – 50% in developed countries, hernia/CA – 15% Which do you think is the most common? Intussusception – especially in kids

6
More than half of SBO recurr
True False Bathing in tomato juice removes the smell of a skunk

7
SBO – Quick facts 20% of acute abdo admissions
Mortality <5% (30% with strangulation, 60% in 1900) >50% recur 20% of admissions for acute abdominal complaints Recurrance: >80% if you’ve had a second episode
 >50% recur. 20% of admissions for acute abdominal complaints. Recurrance: >80% if you’ve had a second episode.")
8
H&P Recurrent abdo pain, crampy, <>
Vomiting, distension, constipation Prev surgery ∆BS Recurrent abdo pain, crampy, <> Worry if pain becomes constant severe Vomiting, distension, constipation Prev surgery Vitals: normal, tachy, hypoTN, fever Distention, ∆BS (↑ pitch), tympany ±scars/hernia, ±tender mass Bilious V with prox obstn, feculent with distal obstn Complete obstruction leads to obstipation, early or partial obstruction may continue to pass stool or flatus Change in vitals worrisome – may suggest complications/sepsis Inc BS early with tinkling, decrease/absent bowel sounds late Tender mass in closed loop obstn Bohner H, et al: Simple data from history and physical examination help to exclude bowel obstruction and to avoid radiographic studies in patients with acute abdominal pain. Eur J Surg 1998; 164:777 -6 features c high SN/PPV: history of previous surgery, history of constipation, age older than 50, vomiting, abdominal distention, and increased bowel sounds Bohner H, et al: Simple data from history and physical examination help to exclude bowel obstruction and to avoid radiographic studies in patients with acute abdominal pain. Eur J Surg 1998; 164:777
, tympany. ±scars/hernia, ±tender mass. Bilious V with prox obstn, feculent with distal obstn. Complete obstruction leads to obstipation, early or partial obstruction may continue to pass stool or flatus. Change in vitals worrisome – may suggest complications/sepsis. Inc BS early with tinkling, decrease/absent bowel sounds late. Tender mass in closed loop obstn. Bohner H, et al: Simple data from history and physical examination help to exclude bowel obstruction and to avoid radiographic studies in patients with acute abdominal pain. Eur J Surg 1998; 164: features c high SN/PPV: history of previous surgery, history of constipation, age older than 50, vomiting, abdominal distention, and increased bowel sounds. Bohner H, et al: Simple data from history and physical examination help to exclude bowel obstruction and to avoid radiographic studies in patients with acute abdominal pain. Eur J Surg 1998; 164:777.")
9
Review of the basics Types? Common causes of ileus?
Mechanical & functional Simple & closed loop (±strangulation) Common causes of ileus? Trauma, infection, sx, meds, metabolic, renal colic Mechanical – physical barrier to flow Functional – problem with gut motility (adynamic ileus) Simple – lumen occluded & prox distention without compromise of intestinal vascular supply Closed-loop – obstruction at two sequential sites – high risk of compromising vascular supply = strangulation Ileus – trauma (abdominal, rib/vertebral #), inf (retroperitoneal, pelvic, intrathoracic), meds (narcotics) metabolic (hK+), Sentinel loop = focal decrease in peristalsis b/c of infl process (pancreatitis, cholecystitis, appendicitis) Pseudo-obstruction – poorly understood, same signs/symptoms as SBO without underlying cause
 Common causes of ileus Trauma, infection, sx, meds, metabolic, renal colic. Mechanical – physical barrier to flow. Functional – problem with gut motility (adynamic ileus) Simple – lumen occluded & prox distention without compromise of intestinal vascular supply. Closed-loop – obstruction at two sequential sites – high risk of compromising vascular supply = strangulation. Ileus – trauma (abdominal, rib/vertebral #), inf (retroperitoneal, pelvic, intrathoracic), meds (narcotics) metabolic (hK+), Sentinel loop = focal decrease in peristalsis b/c of infl process (pancreatitis, cholecystitis, appendicitis) Pseudo-obstruction – poorly understood, same signs/symptoms as SBO without underlying cause.")
10
Physicians reliably can distinguish bowel strangulation from simple obstruction
True False Cracking knuckles leads to arthritis

11
Simple vs Strangulated - How good are we?
Confident diagnosis of “non-strangulating obstruction” wrong 31% of the time. No parameter is sensitive, specific, or predictive for strangulation Not very good! Even experienced physicians and surgeons cannot reliably distinguish between strangulation and simple intestinal obstruction on the basis of examination Sarr et al. Preoperative recognition of intestinal strangulation obstruction: Prospective evaluation of diagnostic capability. Am J Surg 145: , 1983.

12
Pathophysiology Mechanical SBO → prox dilation → ↑ local peristalsis
→ ↑ secretory activity → ↓ reabsorption fluid/lytes → capillary/lymphatic obstruction → edema → perforation or strangulation Initially causes mild proximal intestinal distention d/t accumulation of normal GI secretions and swallowed air Distention stimulates local peristalsis above and below obstruction (frequent loose BM that can accompany partial or early complete SBO) Distention also stimulates inc GI secretions which further contributes to worsening dilation Distended bowel is unable to absorb fluid/lytes normally – worsens the situation Further increases in intraluminal pressure causes capillary and lymphatic obstruction Which leads to bowel wall edema If this process continues uninterupted perforation or strangulation ((strangulation – venous congestion, small BV rupture, mesenteric hemorrhage, and arterial insufficiency OR distended bowel twists on itself, BOTH = ischemia infarction) Additional issues: vomiting, intraperitoneal fluid 3rd spacing effective hypovolemia and eventually shock
 Distention also stimulates inc GI secretions which further contributes to worsening dilation. Distended bowel is unable to absorb fluid/lytes normally – worsens the situation. Further increases in intraluminal pressure causes capillary and lymphatic obstruction. Which leads to bowel wall edema. If this process continues uninterupted perforation or strangulation. ((strangulation – venous congestion, small BV rupture, mesenteric hemorrhage, and arterial insufficiency OR distended bowel twists on itself, BOTH = ischemia infarction) Additional issues: vomiting, intraperitoneal fluid 3rd spacing effective hypovolemia and eventually shock.")
13
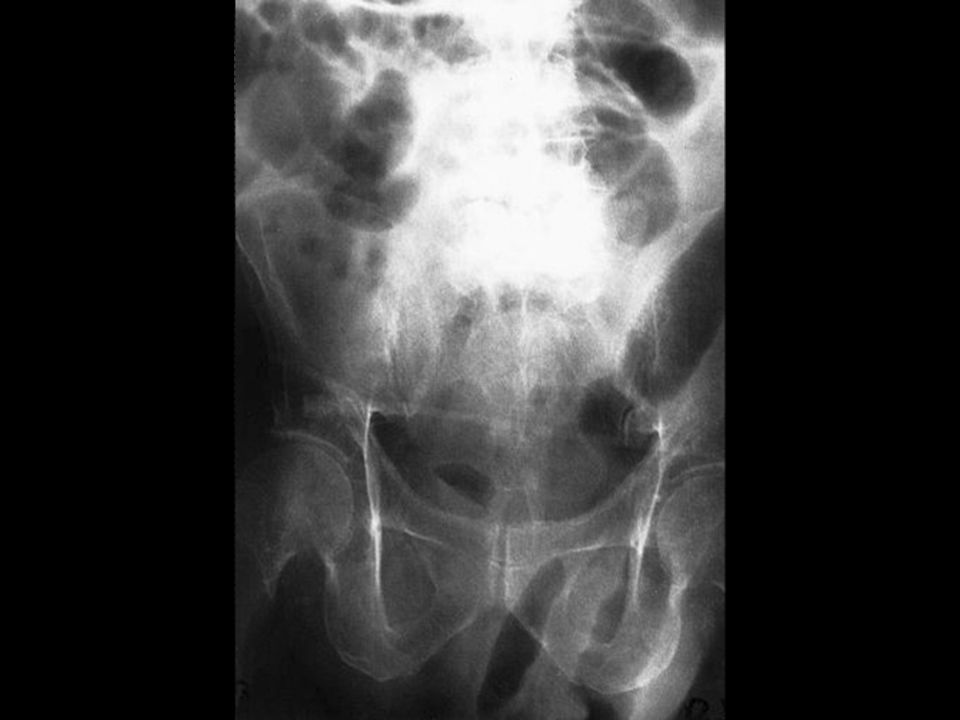
Investigations Labs: Imaging: 3 views (60% +SBO, 25% suggestive)
↑WBC, ±↑CPK, ±↑lactate Imaging: 3 views (60% +SBO, 25% suggestive) Five places to look for air? How many A/F levels? Dilated? Labs are non-specific Late findings suggestive of intestinal compromise and ischemia Lytes/RFT’s may reflect volume loss Imaging - 3 views – is it helpful? How? -may confirm/exclude SBO; identify the site/severity/cause; help distinguish simple obstruction from strangulation --these things help us decide if urgent gen sx consult vs. watch and wait -look for air: A/F levels in SI, rectum (complete obstruction less likely, esp if it has been >24h), under hemidiaphragm, biliary tract (points you towards gall stone ileus), under inguinal ligament -A/F levels – > 2 (in dilated SI, 3-5 can be normal in non-dilated SI) -Dilated – >2.5cm (SI), ((>6cm (LI))) -and this is the big difference between ileus and obstruction – no dilation (or mild 3-4cm) in ileus ((other differences – tends to involve entire GIT, A/F levels are not as prominent, air in colon/rectum))
 Five places to look for air How many A/F levels Dilated Labs are non-specific. Late findings suggestive of intestinal compromise and ischemia. Lytes/RFT’s may reflect volume loss. Imaging - 3 views – is it helpful How -may confirm/exclude SBO; identify the site/severity/cause; help distinguish simple obstruction from strangulation. --these things help us decide if urgent gen sx consult vs. watch and wait. -look for air: A/F levels in SI, rectum (complete obstruction less likely, esp if it has been >24h), under hemidiaphragm, biliary tract (points you towards gall stone ileus), under inguinal ligament. -A/F levels – > 2 (in dilated SI, 3-5 can be normal in non-dilated SI) -Dilated – >2.5cm (SI), ((>6cm (LI))) -and this is the big difference between ileus and obstruction – no dilation (or mild 3-4cm) in ileus. ((other differences – tends to involve entire GIT, A/F levels are not as prominent, air in colon/rectum))")
17
-string of pearls sign – if more fluid than gas see small pockets of gas trapped between valvulae conniventes – oblique series of round lucencies -two subtle signs of closed loop obstruction: coffee bean sign, pseudotumor sign – rarely seen or interpreted correctly (c-b sign: distended, air-filled, and U-shaped bowel loops that are separated by edematous bowel wall, pt sign: presence of a fluid-filled loop of bowel that resembles a mass)
")
18
CT Scan? Not required for diagnosis Can help define site/cause
Other imaging? Small bowel series, U/S *** -string of pearls sign – if more fluid than gas see small pockets of gas trapped between valvulae conniventes – oblique series of round lucencies -two subtle signs of closed loop obstruction: coffee bean sign, pseudotumor sign – rarely seen or interpreted correctly (c-b sign: distended, air-filled, and U-shaped bowel loops that are separated by edematous bowel wall, pt sign: presence of a fluid-filled loop of bowel that resembles a mass) Most SBO can be diagnosed by history and plain films alone CT scan can be used for difficult to diagnose SBO Can go to a SBFT if CT scan is non-diagnostic (helps to differentiate between partial and complete obstruction) SB series – inferior than CT in detection, etiology
 Most SBO can be diagnosed by history and plain films alone. CT scan can be used for difficult to diagnose SBO. Can go to a SBFT if CT scan is non-diagnostic (helps to differentiate between partial and complete obstruction) SB series – inferior than CT in detection, etiology.")
19
What about U/S? SN SP Etiology Plain films 77% 50% 7% U/S 83% 100% 23%
CT 93% 87% SN for presence of obstruction Not as SP as CT Less information about etiology

20
½ of complete SBO resolve spontaneously
True False Eating 3 poppy seed bagels may result in positive urine drug screen for opiates

21
Management Fluid resuscitation Decompression ?Antibiotics
NG tube ?Antibiotics Observation vs. surgery “never let the sun rise or set on an SBO” 75% of partial/30-50% complete resolve They used to use these long decompression tubes that were placed into the jejunum, but there is no evidence that they were any better, and sometimes they formed knots Antibiotics – useful if sx planned or suggestion of strangulation ?bugs?-cover G- + AN ?ceftriaxone + flagyl, ((amp/gent/flagyl, cipro/flagyl)) “” – difficult to distinguish between simple obstn and strangulation - most surgeons advocate a trial of conservative therapy in the absence of findings suggestive of strangulation (peritoneal signs, fever, colicky constant pain, nil relief with NG suction) Observation no longer than 12-24hrs ((-mortality if bowel necrosis 2ry to strangulation 31% vs. simple obstn that is relieved c/in 24hrs (4.5%))) Observation – frequent R/A, little role for repeat XR, repeat CT may help find early signs of bowel ischemia (thickening of the small bowel wall/mesentery, air in the bowel wall, or ascites)
) – difficult to distinguish between simple obstn and strangulation. - most surgeons advocate a trial of conservative therapy in the absence of findings suggestive of strangulation (peritoneal signs, fever, colicky constant pain, nil relief with NG suction) Observation no longer than 12-24hrs. ((-mortality if bowel necrosis 2ry to strangulation 31% vs. simple obstn that is relieved c/in 24hrs (4.5%))) Observation – frequent R/A, little role for repeat XR, repeat CT may help find early signs of bowel ischemia (thickening of the small bowel wall/mesentery, air in the bowel wall, or ascites)")
22
Take home points You are not good at dx strangulation
AXR - >2 A/F levels, >2.5cm, air x 5 ½ of SBO resolve spontaneously

23
Case 2 28M central/RLQ crampy abdominal pain, N
Last BM this am, no fever/chills/V Best guess? 28F same hx? 25% signs initially suggestive of appe = gyne 84F type II DM same hx? 4M same hx? - ectopic, cyst/torsion, PID - AAA, MI - intussusception, testicular torsion

24
Case 2 Vitals – 37.3, 85, 126/85, 18 RLQ tenderness, +guarding
Investigations? Vitals – 37.3, 85, 126/85, 18 On exam RLQ tenderness,

25
Appendicitis – Quick facts
7% lifetime incidence cases/yr in the USA First appendectomy – 1735 Lead shells buried in quail meat

26
What the heck is this? Quail – common cause of appendicitis in 1800’s = lead shells buried in quail meat

27
The Appendix "Its major importance would appear to be financial support of the surgical profession." - Alfred Sherwood Romer Leonardo da Vinci (1492)
")
28
Pathophysiology Obstruction ↑ pressure distension
ischemia + bacteria/PMN invasion swells, irritates necrosis and rupture *** Quail – common cause of appendicitis in 1800’s = lead shells buried in quail meat Usually lumen obstructed by appendicolith or lymphoid hyperplasia Inc intraluminal pressure Distension causes visceral pain, poorly localized, periumbilical (T10 afferent) and you get hyperperistalsis which may cause abdo cramping Ischemia as intraluminal pressure > venous pressure and bacteria/pmn’s invade appendiceal wall With time the appendix swells and begins to irritate surrounding structures – localized RLQ pain Continued swelling and tissue hypoxia lead to necrosis and rupture ((Escherichia coli, Peptostreptococcus, Bacteroides fragilis, and Pseudomonas))
 and you get hyperperistalsis which may cause abdo cramping. Ischemia as intraluminal pressure > venous pressure and bacteria/pmn’s invade appendiceal wall. With time the appendix swells and begins to irritate surrounding structures – localized RLQ pain. Continued swelling and tissue hypoxia lead to necrosis and rupture. ((Escherichia coli, Peptostreptococcus, Bacteroides fragilis, and Pseudomonas))")
29
History Three most common symptoms? Rule out based on pain location?
abdo pain, anorexia, nausea Rule out based on pain location? no, can even have LUQ pain LUQ pain – appendix is in LUQ in those with malrotation

30
Physical exam Vitals – 37.3, 85, 126/85, 18
Do normal vitals r/o appendicitis? What if T = 38.1? Low grade fever in 15% (40% if ruptured) Eponyms McBurney’s, Rovsing’s, Obturator, Psoas, Dunphy Case 2 – normal vitals How common is a low grade fever (<38.3) -low grade fever not uncommon McBurney’s – tenderness 2cm from the ASIS (Rosen) (or 1/3 from ASIS to umbilicus) Rovsing’s-RLQ tenderness when LLQ is palpated and released Psoas-inc pain when psoas is stretched/contracted Obturator-pain with hip flexion/ER Dunphy-increased pain with coughing
 Eponyms. McBurney’s, Rovsing’s, Obturator, Psoas, Dunphy. Case 2 – normal vitals. How common is a low grade fever (<38.3) -low grade fever not uncommon. McBurney’s – tenderness 2cm from the ASIS (Rosen) (or 1/3 from ASIS to umbilicus) Rovsing’s-RLQ tenderness when LLQ is palpated and released. Psoas-inc pain when psoas is stretched/contracted. Obturator-pain with hip flexion/ER. Dunphy-increased pain with coughing.")
31
H&P Three important signs/symptoms?
RLQ pain, rigidity, migration of pain Four to help rule out appendicitis? Pain > 48h, similar pain, lack of migration, lack of ↑ pain with movement/cough associated with high +LR Associated with high –LR

32
CMT is uncommon in women with acute appendicitis True False
The air expelled in a sneeze can travel up to 100mph -25% of women with acute appendicitis

33
Classic Appendicitis Peri-umbilical pain RLQ migration
N, anorexia, V No history of similar pain in past Pain < 48hrs at presentation Pain ↑ with movement/cough Low grade fever Rigidity & guarding Local RLQ tenderness Pain starts as a vague peri-umbilical pain and migrates 50-60% of patients present this way

34
Serial exams Review of 30 years of publications
“active observation” = reassess pt q2-3h Pain resolved in 1/3 of patients No change in perforation rate Negative appendectomy rate 6% vs 20-30% (?lower with CT or U/S) Review looked at any papers that compared active observation to surgery over 30 years in pts with equivocal diagnosis of appendicitis -ve appe rate since CT scan introduction found in some studies to be lower (7%) and in some to be unchanged (20%) -can choose this approach instead of running to the CT scanner -1/3 of patients did not require additional imaging as their pain resolved during the period of active observation Jones PF. Suspected acute appendicitis: Trends in management over 30 years. Br J Surg 2001; 88:
 Review looked at any papers that compared active observation to surgery over 30 years in pts with equivocal diagnosis of appendicitis. -ve appe rate since CT scan introduction found in some studies to be lower (7%) and in some to be unchanged (20%) -can choose this approach instead of running to the CT scanner. -1/3 of patients did not require additional imaging as their pain resolved during the period of active observation. Jones PF. Suspected acute appendicitis: Trends in management over 30 years. Br J Surg 2001; 88:")
35
What labs? β-hcg! Commonly ordered Findings Necessary? CBC, β-hcg, U/A
±LFT’s/lipase, ±CRP Findings ↑ WBC, U/A – pyuria, microscopic hematuria Necessary? β-hcg! LFT’s/lipase depending on location of pain Inc WBC ((with L shift)) in 80% - non-specific ?What may you see on U/A? U/A mild sterile pyuria and microscopic hematuria
) in 80% - non-specific. What may you see on U/A U/A mild sterile pyuria and microscopic hematuria.")
36
U/S vs CT CT Contrast? SN 94%, SP 95%, LR+ 13.3, LR- 0.09
+ usually visualize appendix, not operator dependent, ID other pathology - radiation Contrast? Rectal – best but not practical Oral – delay, ?tolerated, esp. helpful in thin/kids IV – not recommended Radiation – want to avoid in kids, pregnant; 900 rads ((300 rads is one abdominal film, 100 x PA chest)) Oral contrast helps ID periappe fat streaking – can easily be missed in non-contrast CT IV contrast may help ID v. early appe (wall inflammation), but is not recommended (cost, complications, usually adds little information) ((alternative diagnosis is found in up to 15%))
) Oral contrast helps ID periappe fat streaking – can easily be missed in non-contrast CT. IV contrast may help ID v. early appe (wall inflammation), but is not recommended (cost, complications, usually adds little information) ((alternative diagnosis is found in up to 15%))")
37
U/S vs CT U/S MRI? SN 86%, SP 81%, LR+ 5.8, LR- 0.19
+ pregnant, kids, female, thin pts - obese, strictures, retrocecal, normal MRI? Very sensitive but not available U/S spares radiation, used in females as it may help diagnose pelvic pathology as cause of symptoms Bad for obese, those with strictures, retrocecal appendix, normal appendix (seen in 2-45%) -ve U/S not helpful unless other pathology ID’d observe vs. CT scan next ((findings - non-compressible tubular structure at the base of the cecum with a thickened wall (>2 mm), luminal distension with an increased diameter (>6 mm), and possibly free fluid in the pelvis, localized tenderness with graded compression, facalith, mesenteric thickening))
 -ve U/S not helpful unless other pathology ID’d observe vs. CT scan next. ((findings - non-compressible tubular structure at the base of the cecum with a thickened wall (>2 mm), luminal distension with an increased diameter (>6 mm), and possibly free fluid in the pelvis, localized tenderness with graded compression, facalith, mesenteric thickening))")
38
?Change Management? 2 studies of CT in pts w/ suspected appendicitis comparing Tx plan before & after access to results of scans CT changed disposition in 27 – 59% of pts Prevented d/c of ~3% pts w/ appendicitis Prevented negative laparotomy in 3-13% Alternate Dx in 11-20% Frank et al. Unenhanced helical CT scanning of the abdomen and pelvis changes disposition of patients presenting to the emergency department with possible acute appendicitis. J Emerg Med 2002; 23: 1-7 Rao et al. Effect of computed tomography of the appendix on treatment of patients and use of hospital resources. N Eng J Med. 1998; 338: 141-6 Thanks Moritz!

39
To image or not? Imaging based on risk-stratification Don’t image:
Low risk – minimal physical findings, hungry, alternative dx, hx similar pain, sympt > 3 days First few hours of pain Image Intermediate risk – lack classic appendicitis finding ?Image High risk – classic presentation Will go to OR anyway What Rosen’s suggests is imaging based on risk-stratification Don’t image – can do serial exams or send home to return if symptoms progress or don’t improve by hours Image – equivocal pts means lacks classic finding (new onset, migrating pain, tenderness, anorexia) -can do active observation or image (U/S for women of child-bearing age or pregnant, U/S or limited CT scan in kids) ?Image – men, kids, older women with classic presentation. Men with classic presentation have appendicitis >90% of the time
 -can do active observation or image (U/S for women of child-bearing age or pregnant, U/S or limited CT scan in kids) Image – men, kids, older women with classic presentation. Men with classic presentation have appendicitis >90% of the time.")
40
Wake the surgeon? Time from onset of symptoms to rupture?
24-36 hours Average time to seek medical care 17 hours Complication rate 3% vs 12% with rupture Mortality <0.1% vs 3-4% with rupture It’s been 24 hours, can’t it wait until morning? Mortality - with rupture and comorbidities or advanced age ((Complications - most commonly infection, can be prolonged ileus, small bowel obstruction, pneumonia, and urinary retention and infection, fertility problems))
)")
41
Take home points Normal vitals do not rule out appendicitis
Think about U/S over CT in skinny/kids Image pts with equivocal presentation Single most important lab test β-hcg

42
Mesenteric adenitis? Most common associated condition
5-10% admissions for appendicitis ?More common than appendicitis Mostly children Non-specific infl. of mesenteric LN Can follow viral illness Yersinia species (Y. enterocolitica) ((caused by: viral inf, Yersinia enterocolitica, Yersinia pseudotuberculosis, Salmonella species, E. coli, streptococci)) ((-Fever, abdominal pain, vomiting, and diarrhea were frequent ))
 ((caused by: viral inf, Yersinia enterocolitica, Yersinia pseudotuberculosis, Salmonella species, E. coli, streptococci)) ((-Fever, abdominal pain, vomiting, and diarrhea were frequent ))")
43
Mesenteric adenitis? O/E: Ix: Tx: ±Mild fever
Diffuse tenderness, RLQ, no peritonitis 20% other lymphadenopathy Ix: ±↑WBC U/S or CT may be helpful Tx: none, self-limited Usually don’t have fever

44
Case 3 65M Suprapubic and LLQ pain x days, similar bouts of pain in past Anorexia, nausea O/E: Vitals normal, LLQ tender, no peritoneal signs, ?distended #1 in DDx? Initial investigations? Initial labs? – CBC, lytes, Cr, U/A Imaging? – 3 views – r/o obstruction or perforation

45
Diverticular disease facts
10% > 45yrs, 80% > 80yrs ?Dietary deficiency in fibre 85% L-sided (opposite in Japan) -disease virtually unknown prior to the use of the flour-rolling mill (which removes the outer part of wheat) -the pathophysiology is unclear, but seems to be related to age, and fibre seems to be protective -rural Africa and Asia where the diet contains a higher fiber content diverticular disease is virtually unknown
 -disease virtually unknown prior to the use of the flour-rolling mill (which removes the outer part of wheat) -the pathophysiology is unclear, but seems to be related to age, and fibre seems to be protective. -rural Africa and Asia where the diet contains a higher fiber content diverticular disease is virtually unknown.")
46
Definitions Diverticulosis – presence of diverticulae
Asymptomatic - Some of these patients complain of symptoms such as cramping, bloating, flatulence, and irregular defecation – unclear if this is related to diverticula or variant of IBS Diverticulitis – diverticulosis with inflammation of a diverticulum Complicated = extension of disease beyond the pericolonic fat is considered complicated diverticulitis (abscess, gross perforation, fistula) ((obstruction: recurrent diverticulitis can lead to stricture formation; abscesses can become large enough to obstruct adjacent bowel))
 ((obstruction: recurrent diverticulitis can lead to stricture formation; abscesses can become large enough to obstruct adjacent bowel))")
47
Definitions Diverticulosis – presence of diverticulae
Complicated = extension of disease beyond the pericolonic fat is considered complicated diverticulitis (abscess, gross perforation, fistula) ((obstruction: recurrent diverticulitis can lead to stricture formation; abscesses can become large enough to obstruct adjacent bowel))
 ((obstruction: recurrent diverticulitis can lead to stricture formation; abscesses can become large enough to obstruct adjacent bowel))")
48
Anatomy/Pathogenesis
Vasa recta penetrate colonic wall Forms weak points Small (low fibre) stool ↑ pressure herniation of mucosa at vasa recta
 stool ↑ pressure. herniation of mucosa at vasa recta.")
49
((Laplace’s law – tension = pressure * radius))
)")
50
Diverticulosis

51
Clinical features Usually nil Can present like IBS Abdo pain/cramping
Bloating Constipation/diarrhea

52
Management If necessary Modify natural history of disease Analgesia
Anti-spasmodics Modify natural history of disease High-fibre diet ±stool softeners High-fibre diet also shown to decrease abdominal symptoms Prevent disease progression d/c from ED with F/U to FP or gen sx

53
Case 3b 65M Hematochezia No pain O/E: Vitals normal, abdo benign, FOB+
Top 3 in DDx? Ddx: diverticulosis, CA, angiodysplasia, colitis (IBD, infectious, ischemic, radiation, vasculitis), polyps, anorectal disease (fissure, hemorrhoid)
, polyps, anorectal disease (fissure, hemorrhoid)")
54
Definitions Briefly talk about diverticular bleeding

55
Diverticular bleeding
40% of all LGIB 5% severe bleed Typically painless hematochezia Most common cause of LGIB (although angiodysplasia may be the most common cause in >65) 5% of people with diverticulosis will have a severe hemorrhage
 5% of people with diverticulosis will have a severe hemorrhage.")
56
Management Resuscitation Localization of bleeding site Treatment
r/o UGIB, colonoscopy ± angiography or radionuclide scan Treatment Surgery Large bore IV x 2, cross-match blood NG suction or EGD to r/o UGIB, followed by colonoscopy -radionuclide scan (0.1mL/min), angiography (0.5mL/min) 3)Sx – whether urgent or not depends on presentation
, angiography (0.5mL/min) 3)Sx – whether urgent or not depends on presentation.")
57
Definitions Diverticulosis – presence of diverticulae
Complicated = extension of disease beyond the pericolonic fat is considered complicated diverticulitis (abscess, gross perforation, fistula) ((obstruction: recurrent diverticulitis can lead to stricture formation; abscesses can become large enough to obstruct adjacent bowel))
 ((obstruction: recurrent diverticulitis can lead to stricture formation; abscesses can become large enough to obstruct adjacent bowel))")
58
Diverticulitis Diverticulum obstructed inflammation microperforation
pericolic inflammation pain

59
Diagnosis – H&P, Labs History O/E Labs
LLQ pain, several days, prev. pain O/E Fever, LLQ tenderness, ±distension, ±mass Labs ↑WBC Palpable mass in 20%

60
Diagnosis - Imaging Options Plain films Barium enema
Water-soluble contrast enema Colonoscopy CT scan

61
Barium enema is an appropriate investigation in acute diverticulitis
True False Spicy food can cause ulcers

62
Plain films Not useful in diagnosis of diverticulitis
Utility lies in ruling out obstruction/ perforation

63
Barium enema Useful to diagnose asymptomatic diverticulosis
CONTRAINDICATED in acute diverticulitis Potential for barium peritonitis Barium peritonitis can occur with pre-existing occult perforations

66
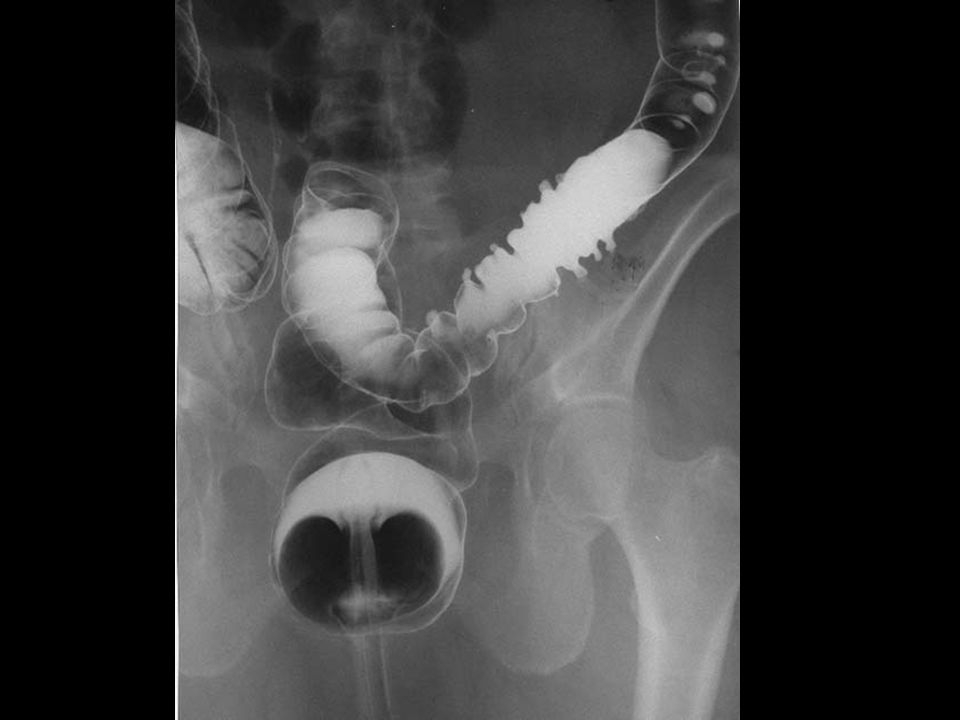
Water-soluble contrast enema
Less detail than barium Can see contrast collect in abscess cavity, peritoneum, along fistulae Less info than CT about disease extent

67
Colonoscopy Not for acute setting
is limited in the acute setting by its more invasive nature, the risk of perforation, [5] [10] and the logistics of arranging this procedure emergently

68
CT scan Investigation of choice SN 69-95%, SP 75-100%
Evaluate extent of disease Exclude other pathology If known uncomplicated diverticulitis – not necessary Don’t need to re-CT scan if pt with known uncomplicated diverticulitis returns with similar presentation – AXR to rule out perf/obstruction followed by conservative mgmt

69
Management Uncomplicated Outpatient Analgesia Oral Abx Fibre F/U
Septra/Flagyl, Cipro/Flagyl, Clavulin Fibre F/U Inpatient tx if severe symptoms, significant comorbid conditions, poor social support, unable to comply with F/U Nsaids, narcotic analgesia Abx – G- & anaerobes Septra DS BID + Flagyl 500 q6h; Cipro 500BID + Flagyl 500 q6h; Clavulin 500/125 TID High-fibre diet prevents recurrance in 70% at 5yrs F/U in 2-3 days with FP to make sure improving ((Complicated = extension of disease beyond the pericolonic fat is considered complicated diverticulitis (abscess, gross perforation, fistula)))
))")
70
Management Complicated Inpatient Analgesia IV Abx
Surgery vs. medical management ticar/clav, amp/sulb, Cipro/Flagyl amp/gent/Flagyl, Cipro/Flagyl, imipenem Mild/mod disease Ticarcillin/clavulanate 3.1 gm IV q 6 hr; Ampicillin/sulbactam, 3 g IV q 6 hr ; Ciprofloxacin, 400 mg IV q 6 hr and metronidazole, 500 mg IV q 6 hr Severe dz Ampicillin, 2 g IV q 6 hr, and metronidazole, 500 mg IV q 6 hr, and gentamicin, 7 mg/kg q 24 hr, or ciprofloxacin, 400 mg IV q 12 hr; Trovafloxacin, 300 mg IV once a day ; Imipenem, 500 mg IV q 6 hr Surgery – emergent if perf/peritonitis ((Complicated = extension of disease beyond the pericolonic fat is considered complicated diverticulitis (abscess, gross perforation, fistula)))
))")
71
Surgery or not? First episode Subsequent episodes, immunocompromised
Usually medical management 3-30% recurr Subsequent episodes, immunocompromised More likely to require surgery or precutaneous abscess drainage Try medical management first – 80% recover

72
Take home points Diverticulosis asympt vs. IBS-like bleeding
inflammation Imaging of choice in diverticulitis is CT Most uncomplicated pts can go home Asypmt or IBS-like symptoms Bleeding = painless Diverticulitis is diverticulosis with inflammation causing pain, but no bleeding

73
Questions?

74
References Ferri: Ferri's Clinical Advisor: Instant Diagnosis and Treatment, 8th ed., 2006 Mosby Leyner, Goldberg. Why Do Men Have Nipples? 2005 Three Rivers Press Mandell, Bennett, & Dolin: Principles and Practice of Infectious Diseases, 6th ed., 2005 Churchill Livingstone Marx, Hockberger & Walls. Rosen’s Emergency Medicine, 6th ed., 2006 Mosby UpToDate

Similar presentations