Download presentation
Presentation is loading. Please wait.

1
Anesthesia for Cardiac Surgery
Jonathan Parmet M.D. Society Hill Anesthesia Consultants

2
Case Discussion 52 year old morbidly obese female scheduled for CABG
she has normal ventricular function she has 100% LAD occlusion not amenable to coronary stenting Has a history of NIDDM, and HTN

3
Case Discussion What anesthetic monitors ?
PA catheter? Should the patient be fast tracked ? What are the anesthetic considerations? Push for extubation on the table?

4
Overview Anesthetic monitoring
PA catheter Transesophageal echocardiography Cerebral oximetry Anesthetic for Patients with CAD requiring cardiopulmonary bypass Pharmacologic agents administered Fast track

5
Open Heart history Philadelphia’s role
1948-Boston/ Philadelphia- Dwight Harken/ Charles Bailey- beating heart mitral commisurotomy 1952- Minnesota- Lillehel/Lewis- Hypothermia (based on work by Bigelow)- open heart with- clamping venous inflow to heart- 1953- Philadelphia-Gibbons- TJH first successful use of CPB with oxygenator 1955- Mayo clinic- bubble oxygenator
- open heart with- clamping venous inflow to heart Philadelphia-Gibbons- TJH first successful use of CPB with oxygenator Mayo clinic- bubble oxygenator.")
6
Monitors Large bore IV- 18-16 gauge
Invasive arterial monitoring right radial, brachial, or femoral Pulmonary arterial catheter – mixed venous, continuous cardiac output Trans-esophageal echocardiography Cerebral Oximetry Bis

7
Pulmonary Arterial Catheter
Used for cardiac filling pressures, tissue perfusion (mixed venous sat), cardiac output Outcome studies do not support the use of a PA catheter Connors ( JAMA 1996) – increased morbidity in ICU patients with PA catheters vs no PA cath Schwann Anesth Analg Nov;113(5): Lack of effectiveness of the pulmonary artery catheter in cardiac surgery.
, cardiac output. Outcome studies do not support the use of a PA catheter. Connors ( JAMA 1996) – increased morbidity in ICU patients with PA catheters vs no PA cath. Schwann Anesth Analg Nov;113(5): Lack of effectiveness of the pulmonary artery catheter in cardiac surgery.")
8
Anesth Analg Nov;113(5):
:")
9
Anesth Analg Nov;113(5):
:")
10
Study Assertions Increased morbidity in patients with PA catheter
Increased use of inotropes in PA group Increased fluid administration in PA group PA catheter not confer any beneficial effect in the CABG population – might be harmful ? Anesth Analg Nov;113(5):
:")
11
Limitations Data collection > 10 years old
How applicable to patients today Variations in institution use from 1-99% Medications not included in propensity matching– beta blockers and statins, anti hypertensives, aprotinin (?) Despite propensity matching Bias that patients with severe disease received catheters TEE patients not included
 Despite propensity matching Bias that patients with severe disease received catheters. TEE patients not included.")
12
How do PA catheters increase morbidity?
Complications of insertion, arrhythmias, pulmonary hemorrhage, infection- not reported 3% increase in fluid 200 ml, 7% increase in fluid balance 200 ml, 8% increase use of inotropes Increased morbidity due to misinterpretation of information Anesth Analg Nov;113(5):
:")
13
Benefits of Transesophageal Echocardiography
Monitor LV function Assess intravascular volume status Assess myocardial ischemia/ dysfunction Valve function Intracardiac defects Aortic pathology Unexplained cardiovascular deterioration Detect new wall motin abnormalities

14
Guidelines for Perioperative Transesophageal EchocardiographyAn Updated Report by the American Society of Anesthesiologists and the Society of Cardiovascular Anesthesiologists Task Force. Anesthesiology:May Volume Issue 5 - pp

15
TEE single most guide in 17% TEE guided fluid therapy in 30%
Transesophageal Echo in Myocardial revascularization: Influence on intraoperative decsion making. Leung A&A 1996 75 cases 584 interventions TEE single most guide in 17% TEE guided fluid therapy in 30% Vasopressor guide in 3% Not an outcome study- Does not define patients do better with TEE monitoring

16
82 high risk CABG patients
Intraoperative Echocardiography is indicated in High-risk coronary artery bypass grafting.Ann thoracic Surg. Savage 1997 82 high risk CABG patients 33% one major surgical intervention based on echo 51% one major anesthetic/hemodynamic change No improved outcomes with TEE 3 patients detected severe atherosclerosis of Aorta off pump 6 patients alternative cannulation sites 16 patients undiagnosed valve disease

17
New prebypass findings in 10%
The role of intraoperative transesophageal echocardiography in patients having CABG. Ann Thorac Surg 2004 Qaddoura New prebypass findings in 10% PFO in closed Sig MR, TR, AR 12- repair in 5 AV (lambl’s) 2- AV explored Aortic Atheroma 5- op cab Surgical plan altered in 3.4% New Postbypass in 3.2% New mr 3 – repair 2 Depressed LVF 6- IABP placed- 5
 2- AV explored. Aortic Atheroma 5- op cab. Surgical plan altered in 3.4% New Postbypass in 3.2% New mr 3 – repair 2. Depressed LVF 6- IABP placed- 5.")
18
Case Discussion 57 year old male for redo-CABG. h/o IDDM, hyperlipidemia, obese 10 hour surgical procedure/ 3 hour pump time/ 2 hour cross clamp Post-op – called to see patient for occipital alopecia 3 years later complains of inability to concentrate and perform his tasks as an accountant Files law suite for having received head trauma during surgical procedure

19
Neurologic changes associated with Cardiopulmonary bypass
3-5 % of CPB suffer perioperative stroke 30-50% of CPB suffer neuro-cognitive dysfunction The incidence varies with the type of neuro psychological testing

20
Adverse Cerebral Outcomes after Coronary Bypass Surgery NEJM 1996 McSPI
Type I- Stoke stupor Type II- deterioration in intellectual function, memory deficit 3.1% type I, 6.1% type II 21% type I died vs 10% type II Incidence increased in patients > 70 yrs

21
NEJM 1996

22
Factors Associated with Adverse Neurologic Outcome
Advanced Age History of previous neurologic event Low flow (Cerebral saturation measure of oxygen extraction Hypertension DM Atherosclerotic Disease Open chamber procedures Use of Cardiopulmonary Bypass

23
Etiology of Adverse Neurologic outcome
Embolic Microemboli (CPB) Macroemboli ( aortic manipulation Aortic cross clamp and cannulation ) Hypoperfusion Carotid Stenosis (increased incidence in DM) Microvascular stenosis (increased incidence in females and DM)
 Macroemboli ( aortic manipulation Aortic cross clamp and cannulation ) Hypoperfusion. Carotid Stenosis (increased incidence in DM) Microvascular stenosis (increased incidence in females and DM)")
24
Strategies to minimize emboli/ factors affecting cerebral blood flow
Minimize aortic manipulation Single clamp technique Off pump CABG (OpCAB) Maintain cerebral blood flow Maintain higher perfusion pressure Blood gas measurement Decrease CMO2- Temperature (80’s-90’s hypothermia 24 degrees) late 90’s til now moderate hypothermia during cpb Anesthetic agents (propofol, Ca channel blockers
 Maintain cerebral blood flow. Maintain higher perfusion pressure. Blood gas measurement. Decrease CMO2- Temperature (80’s-90’s hypothermia 24 degrees) late 90’s til now moderate hypothermia during cpb. Anesthetic agents (propofol, Ca channel blockers.")
26
Does cardiopulmonary bypass contribute to neurologic dysfunction?
Ann thorac Surg 2003 N= 52, 29 opCAB, 23 onCPB TCD, CMRI, Neuropsych testing opCAB less emboli than on CPB No difference cognitive decline 3 months after surgery

27
Cognitive and Cardiac outcomes 5 years after off pump vs on pump CABG
JAMA 2007 231 low risk CABG (123 opCAB, 117 onCPB) Measure Cognitive status after 5 years 62/123 (50.4%) opCAB, 59/117 (50.4%) on CPB cognitive decline In low-risk CABG patients, avoiding the use of CPB had no effect on 5 year cognitive decline
 Measure Cognitive status after 5 years. 62/123 (50.4%) opCAB, 59/117 (50.4%) on CPB cognitive decline. In low-risk CABG patients, avoiding the use of CPB had no effect on 5 year cognitive decline.")
28
Is it aging? A 25-30% cognitive impairment has been demonstrated in the older major vascular, orthopedic, and thoracic surgical populations Lancet 1996 What is the effect of bypass versus the effect of aging?

29
Cerebral oximetry Monitor for cerebral ischemia
Near Infrared- 70% venous/ 30% arterial 3-5 % of CPB patients suffer perioperative stroke There is patient to patient baseline variability

30
Cerebral Oximetry Lower baseline levels associated with increased patient morbidity and mortality ( Murkin Anesth & analg 2007, Heringlake Anesthesiology 2011) Indirect measure of tissue perfusion not just cerebral perfusion
 Indirect measure of tissue perfusion not just cerebral perfusion")
31
Murkin. Anesth & Analgesia 2007

32
Murkin. Anesth & Analgesia 2007

33
Murkin. Anesth & Analgesia 2007

34
Interventions Check head insure in neutral position
Murkin. Anesth & Analgesia 2007 Interventions Check head insure in neutral position PaCO2< 35 Increased to > 40mmHg If MAP < 50 increased > 60 If CVP > 10 If cardiac index < 2.0 (CPB) increased > 2.5 Persistent decrease Increase FIO2/ pulsitile pressure/ propofol / transfuse if hct < 20%
 increased > 2.5. Persistent decrease Increase FIO2/ pulsitile pressure/ propofol / transfuse if hct < 20%")
35
Preoperative Cerebral Oxygen Saturation and Clinical Outcomes in Cardiac Surgery
Anesthesiology:January Volume Issue 1 - pp 58-69

36
Cerebral Desaturation Algorithm
Increase FIO2 to 100% Assess head and cannula position If PaCO2 < 40 mmhg increase to > 40 mmhg Increase MAP > 60 mmhg If Hct < 20 % consider transfusion of PRBC Increase anesthetic depth

37
Case Presentation 57 yr old female for CABG/ Mitral valve annuloplasty
A-line/ large bore IV/ PA catheter/ TEE/ Cerebral Oximeter Induction of anesthesia- 100% oxygen, sevoflurane/ microgms fentanyl/ 1-4 mg midazolam/ 10 mg vecuronium

38
Anesthesia objectives for patients undergoing cardiopulmonary bypass
Analgesia Narcotic (fentanyl micrograms/kg) Amnesia (midazolam mg) Inhalation agents ( desflurane, sevoflurane, isoflurane) Muscle relaxation Long acting Nondepolarizing muscle relaxant pancuronium ( no longer available) Intermediate acting nondepolarizing muscle relaxant
 Amnesia (midazolam mg) Inhalation agents ( desflurane, sevoflurane, isoflurane) Muscle relaxation. Long acting Nondepolarizing muscle relaxant. pancuronium ( no longer available) Intermediate acting nondepolarizing muscle relaxant.")
39
Principles of Anesthetic: Major Determinants of Myocardial Oxygen Consumption
Heart rate Increases in heart rate increase contractility Increase oxygen consumption Decrease myocardial oxygen supply Contractility Wall tension Law of Laplace

40
Ischemic preconditioning
- Cath lab- PTCA- human observation of ischemic preconditioning 1st balloon inflation ST-segment elevation with chest pain 2nd balloon inflation- reduction in ST-segment with decreased chest pain A small period of sub-lethal ischemia prior to a prolong period of ischemia induces a complex series of reactions which reduces myocardial injury adenosine and bradykinin activate G-proteins in the myocyte pathways in turn activates complex cascade (open KATP channels, protein kinase C, (-) guanine nucleotide, ROS) - Tanaka K. Mechanisms of cardioprotection by volatile anesthesthics. Anesthesiology 2004, 100:707-21
 guanine nucleotide, ROS) - Tanaka K. Mechanisms of cardioprotection by volatile anesthesthics. Anesthesiology 2004, 100:")
41
Effects of sulfonylureas on Ischemic preconditioning

42
Ischemic Preconditioning

43
The Inhalational Anesthetics
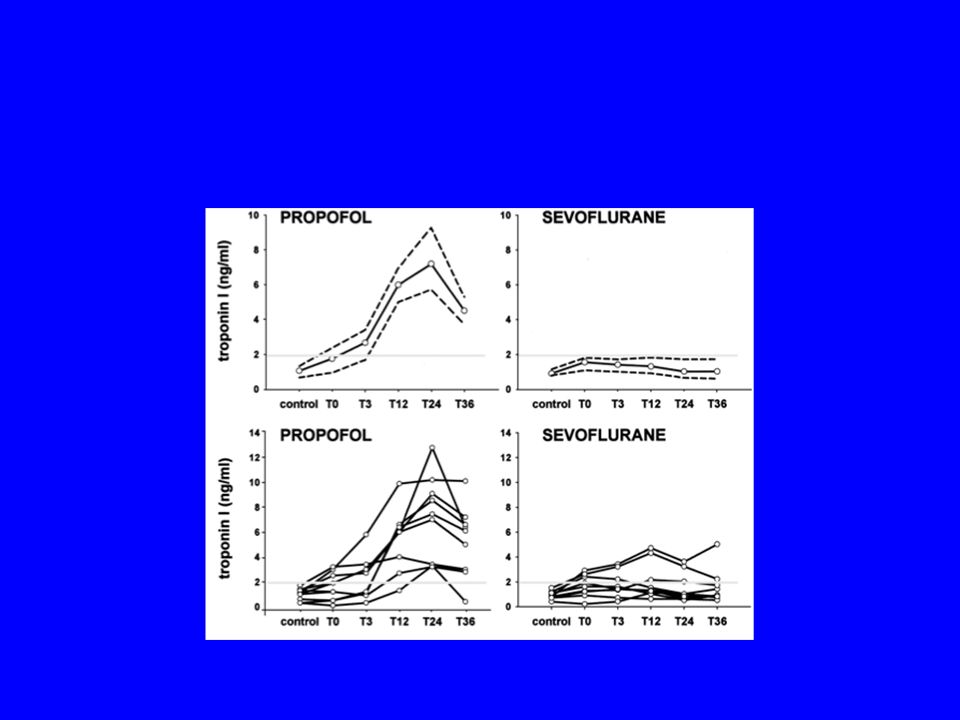
Sevoflurane Most data on sevoflurane Isoflurane Kersten JS. Isoflurane mimics ischemic preconditioning via activation of KATP channels. Anesthesiology 1997;87: Desflurane No study favor one volatile agent over another. Maintain volatile anesthetic throughout the procedure De Hert SG. Effects of propofol, desflurane, and sevoflurane On recovery of myocardial function after coronary surgery. Anesthesiology.2003;99:314-23

45
De Hert SG. Effects of propofol,, and sevoflurane On recovery of myocardial function after coronary surgery. Anesthesiology.2003;99:314-23

46
Myocardial damage prevented by volatile anesthetics Journal cardiothoracic and Vascular Anesthesia 2006

47
Glucose control for Cardiac Surgery
Maintain tight glucose control Blood sugars < 180 mg/dl If > bolus between 2-3 units regular (short acting) insulin CPB associated w/ increase in blood glucose
 insulin. CPB associated w/ increase in blood glucose.")
48
Blood glucose control in patients undergoing cardiac surgery
Elevated blood glucose levels in patients with myocardial infarctions have a 30% worse outcome Elevated blood glucose implicated in worsening the severity of stroke The society of thoracic surgeons guideline series: Blood glucose management during adult cardiac surgery 2009 Higher glucose levels during and after cardiac surgery independent predictor of mortality

49
Case Discussion 51 year old male for CABG. Severe 3 vessel disease. History of increased cholesterol Intraoperative sugars prior to CPB normal Sugars on CPB increase to 200 gm/dl Should the blood sugar be treated? What if the sugar was 145?

50
Deleterious effects of hyperglycemia
Increases myocardial infarction size in dogs Inhibits ischemic preconditioning Amplifies reperfusion injury Produces coronary endothelial dysfunction facilitating myocardial ischemia Inhibits neutrophils Positive effects of Insulin Decrease free fatty acids and decreases free radical formation

51
Fish – 200 patients undergoing coronary artery bypass grafting (2003)
Postop glucose > 250 mg/dl => 10 fold increase in complications Gandhi retrospective cardiac surgery- elevated blood glucose independent predictor of poor outcome (2005)
")
52
Intensive Insulin Therapy in Critically Ill Patients N Engl J Med 2001; 345:1359-1367 Van de Berghe
Prospective randomized to intensive treatment (bs- < 110 mg/dl) conservative treatment (bs mg/dl) Pt population 59% CABG, 27% Valve, 14% combined procedure 39% intensive hypo, 6% hypo The key point is Blood glucose control not occur intraoperatively, only on admission to the unit
 conservative treatment (bs mg/dl) Pt population 59% CABG, 27% Valve, 14% combined procedure. 39% intensive hypo, 6% hypo. The key point is Blood glucose control not occur intraoperatively, only on admission to the unit.")
53
Intensive Insulin Therapy in Critically Ill Patients N Engl J Med 2001; 345:1359-1367

54
CABG- n=3554 1987-1991 subcut insulin (n=942)
Continuous insulin infusion reduces mortality in patients with diabetes undergoing coronary artery bypass grafting. J thorac Card Surg 2003;125: Funary CABG- n=3554 subcut insulin (n=942) Continuous infusion 1991 to 1998 target sugar mg/dl sugar mg/dl 2001- sugar
 Continuous infusion to 1998 target sugar mg/dl sugar mg/dl sugar")
55
Funary J thoracic and Cardiovascular Surgery 2003
Overall mortality 388/ 3554 =2.8% Mortality in Sub Cut =4.5% 40/942 Mortality in Continuous infusion = 1.6% P<0.05 Conclusion: improved blood sugar control improve overall mortality ? Which blood glucose range

56
Furnary, A. P. et al.; J Thorac Cardiovasc Surg 2003;125:1007-1021
No Caption Found Furnary, A. P. et al.; J Thorac Cardiovasc Surg 2003;125: Copyright ©2003 The American Association for Thoracic Surgery

57
Randomized to tight control GIK solution Subcuntaneous Injections
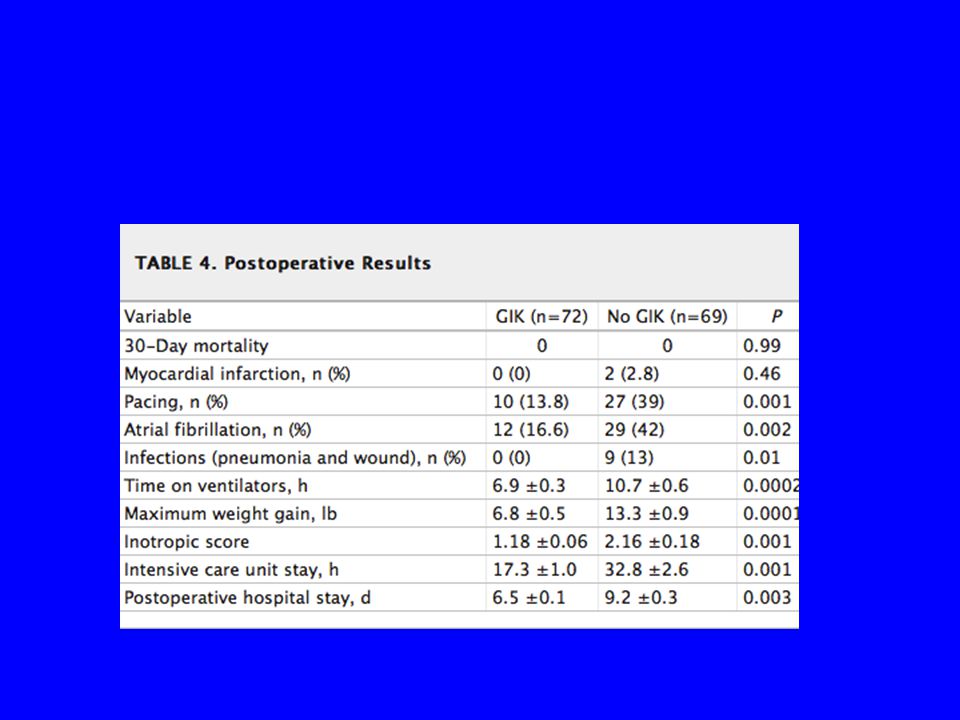
Tight Glycemic control in diabetic coronary artery bypass graft patients improves perioperative outcomes. Lazar Circulation 2004 N= 141 patients Randomized to tight control GIK solution Target blood glucose mg/dl Subcuntaneous Injections Blood glucose < 250 mg/dl GIK started before CPB, but discontinued on CPB- restart with Aortic unclamped Continued 12 hrs postop

59
Figure 4. Cardiac index. Figure 4. Cardiac index. Cardiac index remains higher in GIK-treated patients throughout perioperative period even after termination of GIK infusion at 18 hours. CPB indicates cardiopulmonary bypass. Lazar H L et al. Circulation 2004;109: Copyright © American Heart Association

60
Maintain intraop blood glucose 150<to <200 mg/dl
Poor intraoperative blood glucose control associated with a worsened hospital outcome after cardiac surgery in diabetic patients. Anesthesiology 2005 N= 200 Maintain intraop blood glucose 150<to <200 mg/dl Insulin infusion started intraop Postop maintain blood glucose < 140 mg/dl 71 patients had intraop insulin infusion 35 patients uncontrolled sugars

61
Poor intraoperative blood glucose control is associated with a worsened hospital outcome after cardiac surgery in diabetic patients. Ouattara Anesthesiology 2005;103:677-8

62
N= 3050 conventional N= 3012 intensive
Intensive versus convention glucose management in the critically ill. The Nice-sugar investigation. NEJM 2009 N= 6104 N= 3050 conventional N= 3012 intensive 206 of the intensive rx group had severe hypoglycemia 15 in the conventional group had severe hypoglycemia 27% intensive group died * 24.9% conventional group died *

63
Intensive glucose control Conventional glucose control
gm/dl Conventional glucose control < 180 gm/dl Non surgical population- different treatment protocol- high incidence Of hypoglycemia in intensive group

64
Conclusions Elevated blood glucose preop is associated with poor outcomes postop Intraoperative insulin infusions reduce mortality in the postoperative period (perhaps) During CPB insulin administration if Blood glucose > 140 Continue infusion in the postoperative period
 During CPB insulin administration if Blood glucose > 140. Continue infusion in the postoperative period.")
65
Blood Conservation in Cardiac Surgery
Case conference November 2, 2012

66
Case Presentation 76 year old male for CABG (1 bypass) and mitral valve repair. He has Aortic insufficiency ( mild to moderate). He appears frail. Pre op platelet count is 100K Undergoes 1 vessel bypass/ Mitral valve repair. After chest closure chest tube drainage at 300 for one hour. No thrombus in the chest tube Second Hour 200 cc of chest tube drainage
 and mitral valve repair. He has Aortic insufficiency ( mild to moderate). He appears frail. Pre op platelet count is 100K. Undergoes 1 vessel bypass/ Mitral valve repair. After chest closure chest tube drainage at 300 for one hour. No thrombus in the chest tube. Second Hour 200 cc of chest tube drainage.")
67
Case Transfused 5-7 units PRBC, 12 units FFP, 18 units Platelets, cryo, Recombinant Factor VII (90 ug/kg) Lowest intraoperative Hgb 6 gm/dl After 4 hours chest tube drainage decrease TEE no evidence of tamponade 2 days postoperative chest X-ray reveals ARDS Aggressive diuresis chest X-ray resolves

68
Does packed red blood cell transfusion affect patient outcome independently?
Does the number of packed red blood cells administered affect patient outcome? Does blood component therapy affect patient outcome?

69
ASA refresher course 2012

70
Background 30% of patients post cardiopulmonary bypass develop microvascular bleeding 10% of hospital transfusions are allocated to patients cardiac surgical patients 34%-50% of CABG patients are transfused However significant risk is associated with allogenic red blood transfusions

71
N= 10,289 isolated CABG patients 1995-2002
Transfusion in Coronary Artery Bypass Grafting is Associated with Reduced Long-Term Survival Ann Thorac Surg 2006;81: N= 10,289 isolated CABG patients 49% of patients received PRBC Est 5,041 transfused 9.8 % Platelets 2.8% FFP 0.5% Cryo 2,067 deaths

72
Koch. Transfusion and long-term survival. Ann Thorac Surg 2006;81;1650

73
Koch. Ann Thorac Surg 2006;81:1650-7

74
Conclusion Perioperative PRBC transfusion is associated with adverse long-term sequela in isolated CABG. Attention should be directed toward blood conservation methods and a more judicious use of PRBC. With increased units of PRBC there was an increase in patient mortality

75
Criticism Observational study Not randomized
No indication of transfusion trigger Blood transfusions could be the cause or just a marker of patients that were sicker and had a tendency to bleed Included in analysis greater than 2 PRBC

76
Northern New England Cardiac disease group
The Association of perioperative red blood cell transfusions and decreased long term survival after cardiac surgery. A&A Surgenor Northern New England Cardiac disease group 8 medical centers 9,079 CABG 2001 to 2004 36% of patients PRBC 1-2 units Risk factors for transfusion Increasing age Anemia Female (decreased BMI) Co-morbid disease
 Co-morbid disease.")
77
Figure 1. Adjusted survival by red blood cell use.
Surgenor S D et al. Anesth Analg 2009;108: ©2009 by Lippincott Williams & Wilkins

78
Conclusion “ For anesthesiologists and cardiac surgeons, transfusion of just 1 or 2 units is often viewed as minor and routine decision” That decision places patients at significant risk Exposure of 1 to 2 units of PRBCs was associated with a 16% increased hazard of decreased survival after cardiac surgery

79
Why? Shelf life of PRBC = 42 days 20-40% of PRBC > 28 days
Could prolonged storage time be associated with increased morbidity and mortality? In Cardiac patients increased risk of death, renal dysfunction ,respiratory dysfunction and ICU PRBC greater than 28 Days undergo conformational changes

80
Stored PRBC changes Post operative infectious process
Inhibition of immune system (non leukocyte washed) Damage of the microcirculation from transfused Packed RBCs that have abnormal morphology Long term inhibition of the recipients immune function Stimulation of the inflammatory response
 Damage of the microcirculation from transfused Packed RBCs that have abnormal morphology. Long term inhibition of the recipients immune function. Stimulation of the inflammatory response.")
81
Duration of Red-Cell Storage and Complications after Cardiac Surgery
Duration of Red-Cell Storage and Complications after Cardiac Surgery. N Engl J Med 2008; 358: Koch 2872 CABG 14 day PRBC from 3130 CABG >14 days (old blood) Mean storage for 14 day blood- 11 days Mean storage for old blood- 20 days
 Mean storage for 14 day blood- 11 days. Mean storage for old blood- 20 days.")
82
Duration of Red-Cell Storage and Complications after Cardiac Surgery
Duration of Red-Cell Storage and Complications after Cardiac Surgery. N Engl J Med 2008; 358: PRBCs stored greater than 14 days had increased risk of perioperative complications and reduced short term and long term survival Respiratory failure, septicemia, renal failure, and multisystem organ failure.

83
Duration of Red-Cell Storage and Complications after Cardiac Surgery
Duration of Red-Cell Storage and Complications after Cardiac Surgery. N Engl J Med 2008; 358:

84
Duration of Red-Cell Storage and Complications after Cardiac Surgery
Duration of Red-Cell Storage and Complications after Cardiac Surgery. N Engl J Med 2008; 358:

85
Greater in hospital mortality More likely develop renal failure
Duration of Red-Cell Storage and Complications after Cardiac Surgery. N Engl J Med 2008; 358: Greater in hospital mortality 2.8% vs 1.7% older vs newer More likely develop renal failure 2.7% vs 1.6 % older vs newer Septicemia 4.0% vs 2..8% older vs newer Multisystem organ failure 0.7% vs 0.2%

86
Reasons for increased morbidity and mortality
Conformational changes decreases PRBC viability Decreased deformability results in impairing microvascular flow Decrease 2-3 DPG - decrease oxygen delivery Increased adhessiveness and aggregabilty Decreased nitric oxide and accumulation of proinflammatory substances

89
Questions How can we reduce blood transfusions?
Blood conservation strategies Does component transfusion carry the same risk? Platelets Fresh frozen plasma Cryo

90
Coagulation and Cardiopulmonary Bypass

91
Case Presentation 50 year old male for redosternotomy along with revision aortic root replacement. He has severe aortic insufficiency Receives 300 units / kg of Heparin with targeted ACT > 400 Duration of Cardiopulmonary Bypass = 4hrs Off CPB 1:100 reversal of protamin ACT returns to baseline

92
Case Presentation No thrombus is formed and the patient demonstrates diffuse microvascular bleeding Receives empiric 4 units of FFP / 2 (6) packs of platelets- continues to bleed Receives cryoprecipitate Receives Recombinant Factor VII (45 ug/kg) Receives Prothrombin Concentrate (45 units/kg)
 packs of platelets- continues to bleed. Receives cryoprecipitate. Receives Recombinant Factor VII (45 ug/kg) Receives Prothrombin Concentrate (45 units/kg)")
93
Overview Coagulation Cascade
Classic Coagulation Cascade Current Depiction of In vivo clot formation Cardiopulmonary Bypass and effect on the Coagulation Cascade Anticoagulation for Cardiopulmonary bypass (measure of anticoagulation) Reversal of anticoagulation Measure of reversal of anticoagulation
 Reversal of anticoagulation. Measure of reversal of anticoagulation.")
94
Coagulation Cascade Classic coagulation Cascade
Intrinsic Pathway Extrinsic Pathway 2 phase Model of Coagulation Initiation Phase Propagation Phase

95
Waterfall / cascade model of Coagulation

96
Utility of Classic Cascade
Not an adequate representation of in vivo events Dovetail with coagulation tests: pro-thrombin time (PT, extrinsic) and activated partial thromboplastin time (aPTT intrinsic) Also helps explain factor deficiencies (hemophilia) and effect of anticoagulants (coumadin, heparin) with respect to coagulation tests
 and activated partial thromboplastin time (aPTT intrinsic) Also helps explain factor deficiencies (hemophilia) and effect of anticoagulants (coumadin, heparin) with respect to coagulation tests.")
97
Question Can you have a normal ACT with an abnormal PT and Normal PTT ? i.e. defect in extrinsic pathway Can you have a normal ACT with abnormal PTT and normal PT ? i.e. defect in intrinsic pathway

98
Waterfall / Coag Cascade
Intrinsic or contact pathway has no role in early events in clotting in vivo. The end result of the intrinsic and extrinsic pathways: prothrombin cleaved to thrombin => fibrinogen to fibrin. However thrombus formation is a much more dynamic process involving platelet activation and adhesion, interacting with coagulation factors,VonWillebrand factor, Ca++

99
Basics of Coagulation Platelets are bound to sites of injury, they serve both to localize and to accelerate the soluble coagulation process i.e. activate factors Thrombin generated during the initiation phase potently Activates Platelets

100
2 Phase Model of Coagulation

101
Initiation phase Platelets+Tissue Factor + VIIa+ = Extrinsic Xase=> Xa and IXa

102
Factor Va-Xa-Ca++(prothrombinase) + platelets=> small amounts of thrombin
 + platelets=> small amounts of thrombin")
103
IIa cleaves VIII + V + IX => intrinsic Xase=> 30 increase in thrombin generation

104
AS a result of the intrinsic Xase- Explosive thrombin generation results and produces enough fibrin to stabilize clot formation

105
Initiation Phase TF-VIIa (extrinsic Xase)=> Catalyzes X to Xa => which complexes on the platelet with factor Va small amounts of thrombin Thrombin then initiates the propagation phase which ends in explosive generation of thrombin and fibrin gel Most lab tests only address the initiation phase

106
Propagation Phase Thrombin generated in the initiation phase potently activates platelets along with cleaving factors VIIIa, and Va Prior to this Factor VIII complexed with VWF is released and activated to complex with factor IX forming an enzymatic complex (intrinsic Xase) which generates Xa 50 fold increase in thrombin production Factor XI further amplifies the reaction
 which generates Xa. 50 fold increase in thrombin production. Factor XI further amplifies the reaction.")
107
Clot Architecture Amplification of thrombin generation permits the formation of fibrin clot Clots vary in fibrin thickness Paradoxically thicker clots have more permeability between fibrin strands making them more susceptable to lysis Thin clots develop a more occlusive network

108
Clot Architecture High thrombin clots have tighter cross- linking and are more resistant to lysis Low thrombin clots have less cross linking and are susceptable to lysis High fibrin concentrations also more resistant to lysis Low fibrin concentrations more susceptable to lysis

109
Conclusion Disruption of the endothelium (EC) => TF initiates the coagulation system along with platelet activation/adhesion which forms a platelet plug and starts the process of clot End pathway prothrombin- thrombin (II) Fibrinogen- fibrin (I) Fibrin strands cross link to form clot
 => TF initiates the coagulation system along with platelet activation/adhesion which forms a platelet plug and starts the process of clot. End pathway prothrombin- thrombin (II) Fibrinogen- fibrin (I) Fibrin strands cross link to form clot.")
110
Review Initiation Phase Propagation Phase
Extrinsic Xase- TF- VII- plt=> Xa =>IXa- Va=> IIa Propagation Phase Intrinsic Xase- VIII-IX=> Xa=> Va=> Iia Prothrombinase Xa+Va=>explosive thrombin In order to form thrombus need platelets for activation of coagulation factors

111
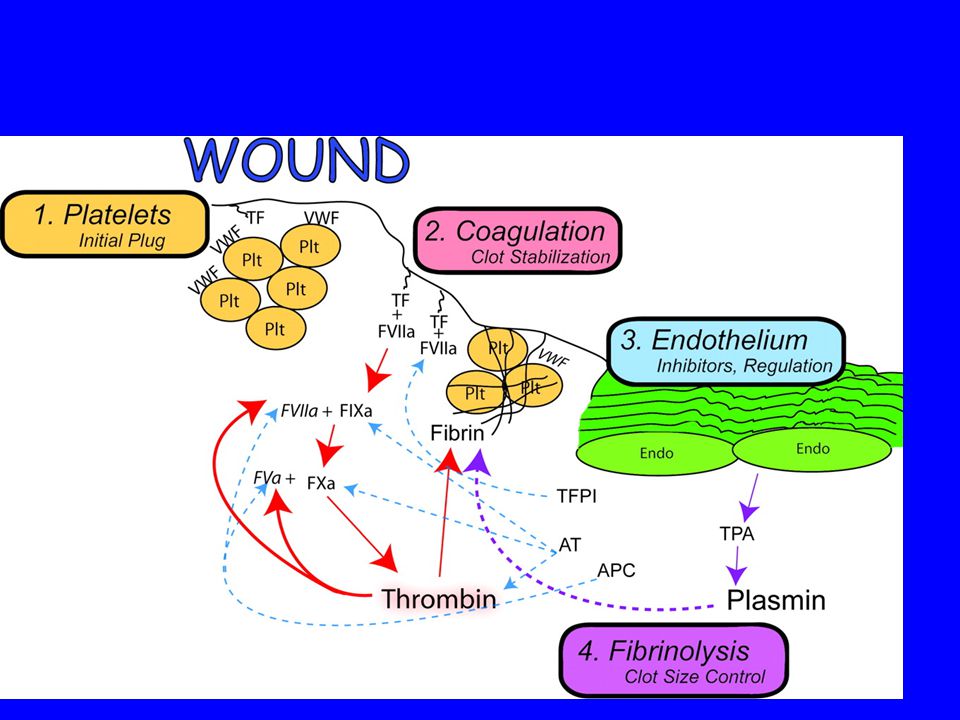
Normal hemostasis. 1, Initial plug formation begins with von Willebrand factor (VWF) binding to collagen in the wound and platelets (plt) adhering to VWF. 2, Coagulation is initiated by small amounts of active factor VII (FVIIa) in blood binding to the expo... Normal hemostasis. 1, Initial plug formation begins with von Willebrand factor (VWF) binding to collagen in the wound and platelets (plt) adhering to VWF. 2, Coagulation is initiated by small amounts of active factor VII (FVIIa) in blood binding to the exposed tissue factor (TF) in the wound, leading to activation of factor IX (FIXa) and factor X (FXa), which in turn initiates the conversion of prothrombin to thrombin. Thrombin creates a positive feedback loop by activating factors VIII (FVIIIa) and V (FVa), which increases FIXa and FXa's conversion of prothrombin to thrombin. This local burst of thrombin production at the wound site converts soluble fibrinogen into a fibrin mesh that stabilizes the initial plug. 3, Clot formation away from the site of injury is prevented by antithrombin (AT), which destroys thrombin and FXa, FIXa, and FXIa, activated protein C (APC), which destroys FVIIIa and FVa, and tissue factor pathway inhibitor (TFPI), which destroys TF-VIIa complexes. 4, Additionally, the endothelium (endo) secretes tissue plasminogen activator (tPA), which binds to fibrin and converts plasminogen to plasmin, which in turn lyses the fibrin. Once a stable clot is formed and the wounded tissue is no longer exposed, the regulatory proteins and fibrinolytic proteins prevent further thrombus formation. Sniecinski R M , Chandler W L Anesth Analg 2011;113: ©2011 by Lippincott Williams & Wilkins
 binding to collagen in the wound and platelets (plt) adhering to VWF. 2, Coagulation is initiated by small amounts of active factor VII (FVIIa) in blood binding to the exposed tissue factor (TF) in the wound, leading to activation of factor IX (FIXa) and factor X (FXa), which in turn initiates the conversion of prothrombin to thrombin. Thrombin creates a positive feedback loop by activating factors VIII (FVIIIa) and V (FVa), which increases FIXa and FXa s conversion of prothrombin to thrombin. This local burst of thrombin production at the wound site converts soluble fibrinogen into a fibrin mesh that stabilizes the initial plug. 3, Clot formation away from the site of injury is prevented by antithrombin (AT), which destroys thrombin and FXa, FIXa, and FXIa, activated protein C (APC), which destroys FVIIIa and FVa, and tissue factor pathway inhibitor (TFPI), which destroys TF-VIIa complexes. 4, Additionally, the endothelium (endo) secretes tissue plasminogen activator (tPA), which binds to fibrin and converts plasminogen to plasmin, which in turn lyses the fibrin. Once a stable clot is formed and the wounded tissue is no longer exposed, the regulatory proteins and fibrinolytic proteins prevent further thrombus formation. Sniecinski R M , Chandler W L Anesth Analg 2011;113: ©2011 by Lippincott Williams & Wilkins.")
112
Arterial Clot vs Venous Clot
Arterial thrombus formation relies heavily on acute platelet plugging Anticoagulants for arterial thrombus attack platelet function- ADP inhibitors/phosphatidylserine ( clopidorel, ticagrolar), GP IIa/IIIb inhibitors Venous thrombus formation relies heavily on thrombin generation (Coumadin, heparin pradaxa)
, GP IIa/IIIb inhibitors. Venous thrombus formation relies heavily on thrombin generation (Coumadin, heparin pradaxa)")
113
Platelets 3 A’s Activation and formation of platelet / platelet bonds
Adhesion to endothelium Aggregation

114
Platelets Platelets must activate and adhere to the injured vessel nearly instantaneously platelet–coagulation factor interactions culminate fibrin formation Most potent platelet activator?

115
Protease Activated Receptor-1 PAR-1

116
Platelets Platelet Activation
Shape change-Change in shape from Sphere to disc to finger like projections Exposure and activation of GPIb and GP IIb/IIIa permit binding of fibrinogen and platelet adhesion to the exposed vessel wall Dense granules (ADP, TA-2 and Serotonin) and alpha granules (growth factor, PF-4 and fibrinogen, VWF) migrate to center and then periphery
 and alpha granules (growth factor, PF-4 and fibrinogen, VWF) migrate to center and then periphery.")
117
Dense Granule Release ADP- potent stimulant to attract other platelets for aggregation Thromboxane-A2- platelet attraction and also vasoconstriction Serotonin- platelet attraction and vasoconstriction

119
Platelet Activation major goals
recruitment of additional platelets vasoconstriction of smaller arteries to slow bleeding (Thromboxane, serotonin) local release of ligands to stabilize platelet–platelet matrix localization and acceleration of platelet associated fibrin formation protection of clot from fibrinolysis
 local release of ligands to stabilize platelet–platelet matrix. localization and acceleration of platelet associated fibrin formation. protection of clot from fibrinolysis.")
120
Adhesion and Activation

121
Platelet Adhesion under shear stress

122
Platelet Adhesion VwF affinity to GPIba slows the platelet down and has the platelet change from sphere to disc. At same time platelet activated and GPIIb/IIIa changes and binds to VWF Platelet covers endothelium

123
Platelet Aggregation Release of alpha and dense granules contents
ADP, Ca++, serotonin, thromboxane A2 Recruits other platelet GPIIb/IIIa change and permit growth of platelet plug

124
Platelet Aggregation platelet–ligand–platelet matrix in which fibrinogen or vWf serves as the bridging ligand GPIIb/IIIa is the most abundant glycoprotein on the platelet surface activated platelets provide specific receptors for factors VII, VIII, Xa, IXa, and Va

125
Factor XIII Factor XIIIa stimulated by thrombin
bind to fibrin and stabilizes fibrin and cross links with fibrin to stabilize clot Binds antiplasmin to prevent clot lysis Clot less likely to be dissolve

126
Endogenous Anticoagulants
Directed at inhibiting Platelets Arterial circulation Directed at inhibiting thrombin Venous circulation

127
Endogenous anticoagulants Arterial
Endothelial Cell surface carries a net negative surface charge nitric oxide and prostacylin (PGI2) inhibit platelet clot (adhesion and aggregation) Healthy endothelial cells also synthesize ADPase (inhibits Platelet aggregation)
 inhibit platelet clot (adhesion and aggregation) Healthy endothelial cells also synthesize ADPase (inhibits Platelet aggregation)")
128
Endogenous Anticoagulants venous
Endothelial cells synthesize an endogenous heparin congener, heparan sulfate works via antithrombin III => X, IX, XI,II Activated protein C (APC) cleaves factors IXa and VIIIa, thereby down regulating thrombin formation (also anti inflammation) Tissue factor pathway inhibitor (TFPI) cleaves Tf-VII
 cleaves factors IXa and VIIIa, thereby down regulating thrombin formation (also anti inflammation) Tissue factor pathway inhibitor (TFPI) cleaves Tf-VII.")
129
Tissue Plasminogen Activator
Thrombin, and Xa stimulate release of t-PA Cleaves plasminogen to plasmin Release of fibrin split products (D-dimer) Effect of TPA blunted by plasminogen activator inhibitor Also Thrombin Activator Fibrinolysis Inhibitor (plasmin or thrombin for stimulus)
 Effect of TPA blunted by plasminogen activator inhibitor. Also Thrombin Activator Fibrinolysis Inhibitor (plasmin or thrombin for stimulus)")
130
Fibrinolysis

132
Summary Denuding the endothelium results in release of tissue factor which activates factor VII platelets and thrombin (initiation Phase or the extrinsic pathway) Denuding the endothelium results in cleaving serine protease and activation of platelets, XII which stimulates the intrinsic pathway Both pathways result in thrombin then cleaving fibrinogen to fibrin
 Denuding the endothelium results in cleaving serine protease and activation of platelets, XII which stimulates the intrinsic pathway. Both pathways result in thrombin then cleaving fibrinogen to fibrin.")
133
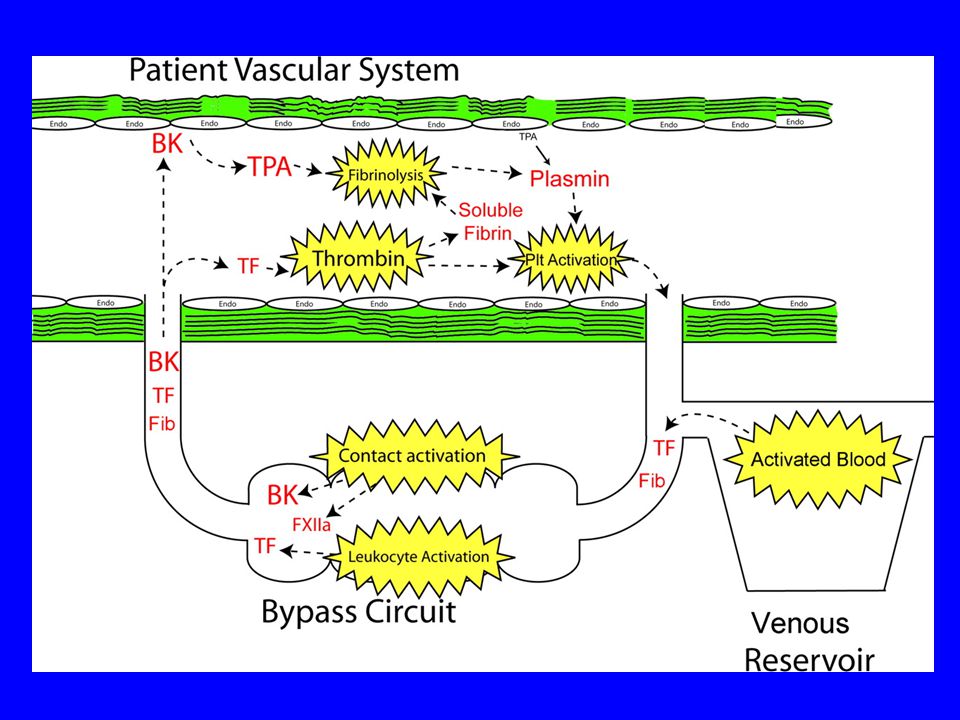
CPB: Upsetting the balance
Heparin Paralysis of the coagulation cascade by heparin Hemodilution Hypothermia Coagulation cascade Platelet defect Complement system Leukocyte Activation (inflammatory Response)
")
134
Heparin Variability on its effect from patient to patient (as measured by the Act) Stimulates ATIII (1,000 fold) Inhibits II, Xa, IX, XI Inhibits Platelets (direct, indirect) VWF effect on GP1b receptors No effect on GP IIb/IIIa Bound to protein and sequestered into the endothelial cells – mechanism of heparin rebound
 VWF effect on GP1b receptors. No effect on GP IIb/IIIa. Bound to protein and sequestered into the endothelial cells – mechanism of heparin rebound.")
135
Hemodilution Pump Prime- 1 to 2 L of crystalloid
Hematocrit decrease from 40 to 25% Coagulation factors decrease 60-70% Factors II, V, fall significantly and factor II correlate with post op bleeding With increased duration of CPB factors decrease further due to activation on CPB

136
Changes in Coag factors before and after bypass

137
Fall in thrombin potential and increased chest tube drainage

138
Hypothermia 100 decrease in temperature results in 50% inhibition of enzymatic activity 33-37 nonsignificant reduction in coagulation enzyme activity below 33 sig Temperature of 320C inhibits platelet activation and aggregation by thrombin Fibrinolysis not inhibited by <330 C

139
Activation of Coagulation Cascade
CPB induces contact activation Auto cleave Factor XII =>preKallikrein => Kinins ( bradykinin) Intrinsic coagulation cascade=> thrombin and fibrin and EC => TPA TF initiator of clottting (dominant source of clotting factor activation) Intense thrombin and fibrin generation over the first 5 min despite maximal heparinization (ACT > 480)
 Intrinsic coagulation cascade=> thrombin and fibrin and EC => TPA. TF initiator of clottting (dominant source of clotting factor activation) Intense thrombin and fibrin generation over the first 5 min despite maximal heparinization (ACT > 480)")
143
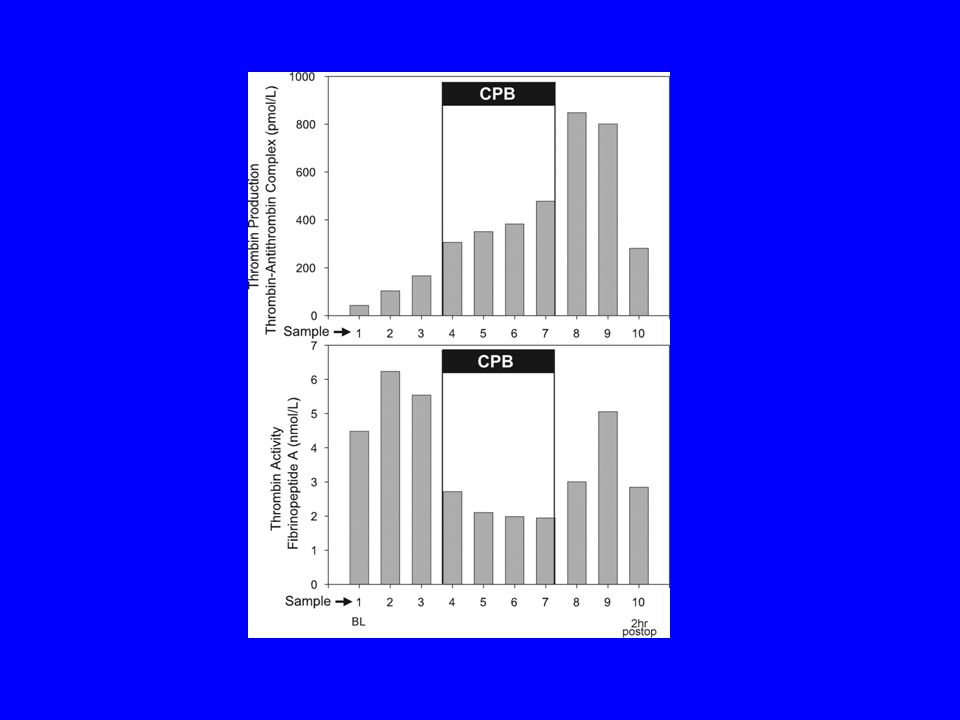
5 minutes of CPB thrombin and fibrin levels increase 20 fold
Soluble Thrombin/Fibrin not circulate in blood- thrombin/fibrin measured is non hemostatic Total fibrin reduced on bypass (heparin) After reperfusion increase in thrombin/ and fibrin increase
 After reperfusion increase in thrombin/ and fibrin increase.")
144
CPB Platelet dysfunction
CPB decreases plt count beyond amount attributed to hemodilution CPB-induced functional platelet defects may produce bleeding that requires platelet transfusion despite seemingly adequate platelet counts CPB activates platelets, (release of the contents of internal granules alpha and dense)
")
145
Post CPB Platelet dysfunction
Blunted response to stimulation (in vitro) Higher concentrations of thrombin, ADP, and collagen needed to activate and aggregate CPB activates plts- release of dense and alpha granules Platelets adhere to exposed endothelium, CPB circuit binding to fibrinogen Net result- Spent platelets or dysfunctional platelets
 Higher concentrations of thrombin, ADP, and collagen needed to activate and aggregate. CPB activates plts- release of dense and alpha granules. Platelets adhere to exposed endothelium, CPB circuit binding to fibrinogen. Net result- Spent platelets or dysfunctional platelets.")
146
Platelets Binding of Platelets to fibrin through the GPIIb/IIIa can tear the receptor through sheer forces Results in dysfunctional platelets Protease activated receptor (par-1) cleaved Use of Lysine or Kallekrien inhibitors preserve Par-1 and preserve GP1b receptors (decrease platelet activation)
 cleaved. Use of Lysine or Kallekrien inhibitors preserve Par-1 and preserve GP1b receptors (decrease platelet activation)")
147
Platelets Young platelets exhibit more robust response to activation
Older platelets less of a response CPB demonstrates older platelets Conclusion – set up post bypass platelet dysfunction

148
CPB Stimulates Fibrinolysis
Increase release of TPA with bypass due to EC cell (animal models) stimulation Stimulus for TPA release XII, HMWK, bradykinin, TF, thrombin increase in plasmin production with CPB Plasmin antiplatelet effects (platelet activation) Fibrin formation=> fibrin degradation (result of cpb)
 stimulation. Stimulus for TPA release XII, HMWK, bradykinin, TF, thrombin increase in plasmin production with CPB. Plasmin antiplatelet effects (platelet activation) Fibrin formation=> fibrin degradation (result of cpb)")
149
Plasmin also cause platelet GPIb, GP IIb/IIIa to internalize

150
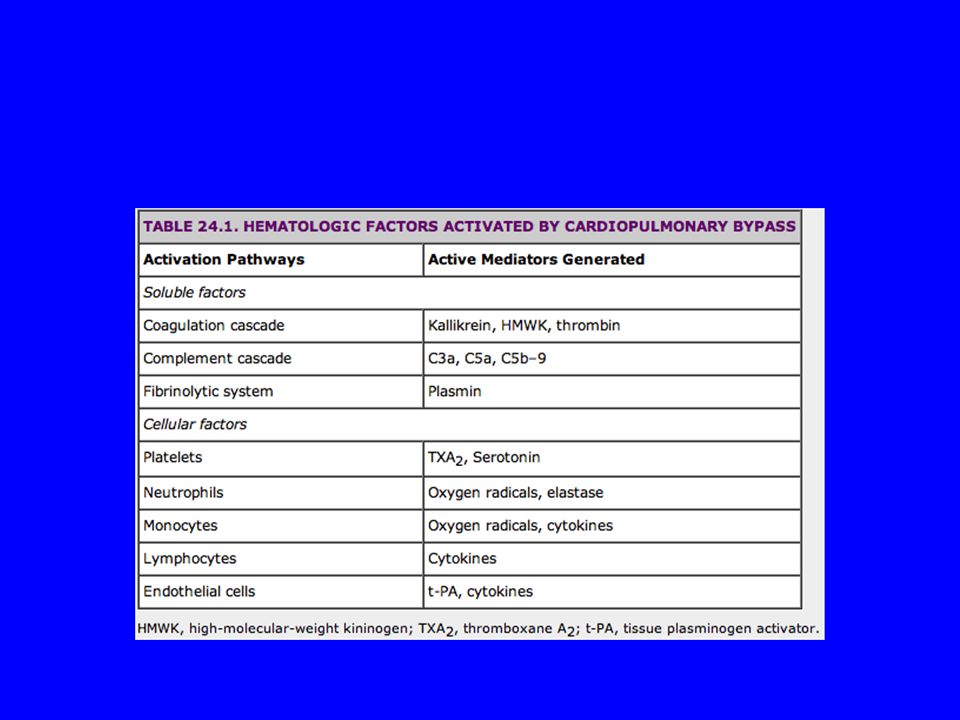
Complement Activation
Increase markers of complement activation associated with increased perioperative blood loss Administration of protamine induces complement surge Complement also stimulates inflammatory cascade, leukocytes, platelets, and ECs

151
Inflammatory Response
Leukocytes bind and are activated by the CPB tubing => TF Leukocytes and TF found in shed blood Decrease Protein C activation=> thrombin formation Inflammatory response procoagulant

153
CPB effect on Coagulation

154
Monitoring anticoagulation
J Parmet Team Leader Cardiac Anesthesiology Pennsylvania Hospital

155
Case Presentation 51 yr old male for coronary artery revascularization
h/o cocaine use and abuse h/o v fib arrest with successful resucitation Not cooled allowed to awake Neurologically intact, strange affect

156
Case presentation Smooth induction/ intubation/ invasive line placement During swan patient require supplemental muscle relaxation Continued high requirement for muscle relaxation Difficulties ventilating Carbon dioxide

157
Case Presentation Propofol infusion started/ continued increased muscle relaxation/ pt temperature not decreasing Heparinized with 300 units/ kg => ACT =380 Do you want to initiate Cardiopulmonary bypass?

158
Case Presentation Give another 10K heparin Want to initiate bypass?
Repeat ACT after cooling?

159
Case presentation Decided give 10K of heparin Repeat ACT 340 sec
What now? More Heparin? Thaw FFP? Cancel case? Get HIT work up? Measure antithrombin III levels?

160
Questions? What ACT for CPB? Where does this number come from?
Why do we use the ACT? Are there other options?

161
Monitoring Anticoagulation for CPB - Effects of heparin
Monitoring Anticoagulation for CPB - Effects of heparin? Or heparin levels ? PT- prothrombin time PTT- activated partial thromboplastin time

162
Prothrombin time TF added tests factors- VII, X, V, II, I
TF + Factor => robust response Vitamin K dependant factors (II,VII, IX , X) Variability in thromboplastin potency =>INR Excessive amounts of heparin will alter the prothrombin time
 Variability in thromboplastin potency =>INR. Excessive amounts of heparin will alter the prothrombin time.")
163
Partial Thromboplastin time
Thromboplastin + phospholipid (Cephalin kaolin) TF absent Intrinsic pathway Not as robust a response (takes longer for fibrin to form thrombus) Measure of Heparin effect- II, X, IX , XI
 TF absent. Intrinsic pathway. Not as robust a response (takes longer for fibrin to form thrombus) Measure of Heparin effect- II, X, IX , XI.")
164
One advantage to selecting the ACT to monitor anticoagulation during cardiac surgery is that other clotting time methods (e.g., activated partial throm- boplastin time, thrombin time) become either incoa- gulable (infinite) or highly variable at heparin concentrations below those usually required for safe CPB(10,13-15).
 become either incoa- gulable (infinite) or highly variable at heparin concentrations below those usually required for safe CPB(10,13-15).")
165
Thrombin Time Plasma + thrombin => fibrin (10 sec)
Factors which affect Heparin Fibrinogen Fibrinogen degradation products

166
Activated clotting time
Point of care test introduced by Casthely in 1966 1975 Bull – heparin monitoring protocol ACT for cpb* 2 cc of whole blood withdrawn from arterial circulation Mixed- with activator (celite or kaolin) in test tube with magnet Tube 370c and rotates Clot holds magnet away from detector => end of test ( nl- 80-? sec)
 in test tube with magnet. Tube 370c and rotates. Clot holds magnet away from detector => end of test ( nl- 80- sec)")
167
Activated clotting time
Celite More sensitive to heparin (higher ACT) More sensitive to hypothermia (higher ACT) Aprotinin artificially prolongs ACT Kaolin More resistant to heparin Not prolonged by aprotinin Binds aprotinin
 More sensitive to hypothermia (higher ACT) Aprotinin artificially prolongs ACT. Kaolin. More resistant to heparin. Not prolonged by aprotinin. Binds aprotinin.")
168
Anticoagulation Protocols for Cardiopulmonary Bypass
How much Heparin should we give for CPB? How do we know to give more heparin CPB ? Should we measure heparin effect or serum concentration?

169
Factors affecting the Activated Clotting Time
Heparin Hypothermia Hemodilution Thrombocytopenia <20,000 Severe Platelet inhibitors > 50% GP IIb/IIIa inhibitors alone no, with yes Protamine Gross protamine excess

170
Bull. Heparin therapy during extracorporeal circulation
Bull. Heparin therapy during extracorporeal circulation J Thor Card Surg

171
Bull 1975 J thorac Card Surg Looked at 6 heparin dosing protocols
Measured ACT’s Found a 3 fold patient variation with heparin dosing Found in 4 of the dosing protocols ACTS non therapeutic (<300) Defined therapeutic range 300< TR<600
 Defined therapeutic range 300< TR<600.")
172
Bull J thorac Card surg Suggested ACT > 480 before initiating CPB Provide safety margin over an Act of 300 sec “ it appears many practitioners assume a needed ACT > 480 for cpb and that number represents minimum safe level ( not scientifically validated)”
")
173
Case Presentation 48 yr old obese male for CABG Weight = 122 kg
Calculated heparin dose= 36.6 K units heparin ACT= 380 What to do?

174
Case Given 15 K of heparin Repeat ACT = 410
Vein not ready patient temperature 35.3 Repeat ACT= 340 What to do? How much heparin is to much? Should we accept an ACT below 400 s?

175
Gravlee G. Variability of the activated clotting time
Gravlee G. Variability of the activated clotting time. Anesth Analg 1988:, 46 pts undergoing CPB Duplicate act Baseline, 5 min post hep, 5 min post prot Beef lung heparin- 300 unit/kg Protamine administered by protamine titration test

176
Variability Activated clotting time
Gravlee and Rogers Anesth & analg 1988

177
Variability of ACT. A&A 1988

178
Variability of ACT. A&A 1988

179
ACT variability Once prolonged beyond 300 seconds, one should not expect ACT to produce pinpoint accuracy in determining heparin or prota- mine doses. Maintaining ACT values over 400 seconds during CPB probably constitutes safe anticoagulation.

180
Metz and Keats. Low activated coagulation time during cpb does not increase bleeding. J thorac & Cardiovasc surg 1990 193 patients Heparin single dose 300 units /kg (porcine) Random ACT measurement, and heparin levels Measured clot in CPB circuit chest tube drainage Protamine reversal 1.5 mg/100 units of heparin
 Random ACT measurement, and heparin levels. Measured clot in CPB circuit chest tube drainage. Protamine reversal 1.5 mg/100 units of heparin.")
181
Metz. J thorac Cardiovasc surg 1990

182
Metz Annal Thorac Surg

183
Metz. 1990 Ave pump time = 59 min 51 patients Act < 400 , 4 <300
Patients with low ACT values not bleed more than those with higher values Heparin level decreased markedly during CPB (2-4 u/ml) did not correlate with ACT Conclusion: No need to measure ACT for 1 hour of CPB
 did not correlate with ACT. Conclusion: No need to measure ACT for 1 hour of CPB.")
184
J thoracic Cardio 1990 Gravlee- found maintaining higher CPB heparin concentrations better suppressed plasma coagulation but predisposed to increased postoperative blood loss Measure fibrinopeptide a

185
Studies Gravlee. Variability of the activated coagulation time. A&A
Metz. . Low activated coagulation time during cpb does not increase bleeding. J thorac & Cardiovasc surg 1990 Gravlee. Heparin Management protocol for CPB influences heparin rebound but not bleeding.Anesthesiology 1992

186
Studies Increased accuracy and precision of heparin and protamine dosing reduces blood loss and transfusion patients undergoing primary cardiac operations. Jobes 1995 Heparin and protamine titration do not improve hemostasis in cardiac surgical patients Can Journal 1998 Shore lesserson

187
Studies The Impact of heparin concentration and activated clotting time monitoring on blood conservation. Despotis J thorac Surgery 1995

188
Gravlee. Heparin Management protocol for CPB influences heparin rebound but not bleeding. Anesthesiology 1992 63 patients Randomized- 200 units/kg bovine heparin, additional heparin to achieve ACT > 400 sec (Group A) N=30 Or 400 units/kg to maintain heparin level of > 4 units/ml (group H) N=33 Both groups same protamine neutralization protocol
 N=30. Or 400 units/kg to maintain heparin level of > 4 units/ml (group H) N=33. Both groups same protamine neutralization protocol.")
189
Heparin dose group H 57,000 (prot 256)
Heparin Management protocols for cardiopulmonary bypass influences heparin rebound but not bleeding Heparin dose group A 28,000 Prot 193 Heparin dose group H 57,000 (prot 256) 8 and 24 post no difference in chest tube drainage Group H > incidence in hep rebound, rx aggressive Antithrombin III levels lower in group H Small dose vs large dose no diff in blood loss or transfusion
 8 and 24 post no difference in chest tube drainage. Group H > incidence in hep rebound, rx aggressive. Antithrombin III levels lower in group H. Small dose vs large dose no diff in blood loss or transfusion.")
190
Gravlee. Heparin protocols
Solid line= Group A Dotted line= Group H

191
Test group(22)- heparin dose = 3(480-ACT)/ (HRT-ACT) X EBV
Increased accuracy and precision of heparin and protamine dosing reduces blood loss and transfusion in patients undergoing primary cardiac operations. Jobes 1995 N= 52 Control group (24)- heparin 300 units/kg (porcine)- protamine 1 mg/100 units of heparin (pump heparin not included) Test group(22)- heparin dose = 3(480-ACT)/ (HRT-ACT) X EBV Protamine 0.02(ACT status-ACTbase)/ (ACTstatus-PRT) X EBV
- heparin 300 units/kg (porcine)- protamine 1 mg/100 units of heparin (pump heparin not included) Test group(22)- heparin dose = 3(480-ACT)/ (HRT-ACT) X EBV. Protamine 0.02(ACT status-ACTbase)/ (ACTstatus-PRT) X EBV.")
192
Jobes. J thoracic Ccardiovasc 1995

193
Jobes. 1995

194
Heparin and protamine titration do not improve hemostasis in cardiac surgical patients Can Journal 1998 Shore Lesserson 4 groups-

195
Results

196
Results

197
Why the difference? Initial heparin dose by Jobes not reported
Transfusion triggers by Jobes not reported nor standardized by protocol Different protamine management strategies between the 2 groups No mention of the duration of cardiopulmonry bypass

198
Hepcon ACT= protamine titration method
The Impact of heparin concentration and activated clotting time monitoring on blood conservation. Despotis J thoracic Surgery 1995 N= 254 Control= heparin (porcine) 250 units/kg additional 5k to achieve ACT > 480s. Protamine 0.8 mg/100 units heparin Hepcon ACT= protamine titration method Additional heparin if ACT< 480s Protamine dose based on heparin concentration
 250 units/kg additional 5k to achieve ACT > 480s. Protamine 0.8 mg/100 units heparin. Hepcon ACT= protamine titration method. Additional heparin if ACT< 480s. Protamine dose based on heparin concentration.")
199
Despotis et al

200
Despotis et al

201
ACT and Heparin concentrations

202
Despotis Results

203
Conclusions Patient variability exists with respect to ACT response when given heparin Empiric 300 units per kg appears as common practice in cardiac operating rooms Achieving ACT >400 sec for CPB is acceptable

204
Conclusions Studies investigating heparin concentration vary in conclusions Differences in methodology as well as duration of CPB remain important Lack of standardization for transfusion of PRBC and of blood products may also contribute to different conclusions reached

205
Conclusions A discordance exists between ACT measure and serum heparin concentrations This discordance may contribute microvascular bleeding 2ndary to using to high a protamine reversal This discordance is exacerbating as the duration of CPB increases

206
References Anticoagulation Monitoring during cardiac surgery. Anesthesiology : Gravlee. Cardiopulmonary bypass principles and practice. Anticogulation for cardiopulmonary bypass Heparin sensitivity and Resistance: Management during cardiopulmonary bypass. Anesth Analg 2013:116:

207
Heparin Pharmacology Polysaccharide contained in mast cells
Acid, negative charge Unfractionated (beef lung vs porcine mucosa) low molecular weight high molecular weight (1k-50K da) High molecular weight attraction for anti thrombin III-thrombin complex- heparin cofactor II Low molecular weight (< 6K) heparin bind preferentially factor X no effect on anti thrombin III
 low molecular weight. high molecular weight (1k-50K da) High molecular weight attraction for anti thrombin III-thrombin complex- heparin cofactor II. Low molecular weight (< 6K) heparin bind preferentially factor X no effect on anti thrombin III.")
208
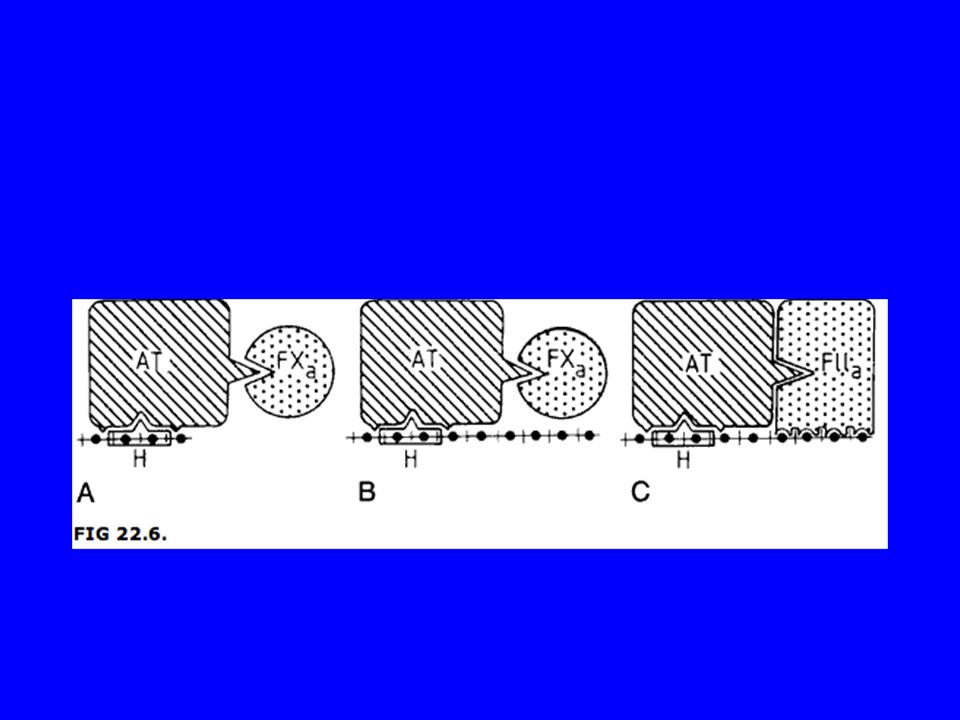
Thrombin inhibition -simultaneous binding of heparin antithrombin III and thrombin
Must contain critical pentasaccharide sequence/ length 18oligosaccharide

210
Other affects of Heparin on coagulation
Heparin may induce fibrinolysis => activate tissue plasminogen activator also releases TFPI Heparin affects platelet function Suppresses alpha granule release Increase platelet factor - 4 release Gp IIb / IIIa Gp Ib/ IIa

211
Heparin Only 1 in 3 heparins have critical sequence to bind to the antithrombin III complex Heparin also produces release of tissue factor pathway inhibitor and affects the extrinsic coagulation system (high dose) Possible initiation of the fibrinolytic pathway
 Possible initiation of the fibrinolytic pathway.")
212
Heparin dosing Bolus 2 mg/ kg heparin ( Bull )- heparin response test 150 units / kg – 400 units / kg u/kg for heparin bound circuit u/kg with additional bolus u/kg Measure an ACT if > 300 s , if > 400 s, if > 480s
- heparin response test 150 units / kg – 400 units / kg u/kg for heparin bound circuit u/kg with additional bolus u/kg Measure an ACT if > 300 s , if > 400 s, if > 480s")
213
Heparin Pharmicokinetics
Elimination half life varies with heparin dose (50 % eliminated by renal excretion) 100 units => 60 min 400 units => 150 min Substantial variability in heparin anticoagulant responsiveness- wide range of heparin dose response (patient specific)
 100 units => 60 min. 400 units => 150 min. Substantial variability in heparin anticoagulant responsiveness- wide range of heparin dose response (patient specific)")
214
Heparin Resistance Despite adequate dosing of heparin the ACT does not increase to the prescribed institutional value to initiate (safely) cardiopulmonary bypass The presumptive mechanism is Antithrombin III deficiency (possible VIII) Acquired liver disease, malnutrition, nephrotic syndrome, and heparin infusions Decrease antithrombin III levels
 cardiopulmonary bypass. The presumptive mechanism is Antithrombin III deficiency (possible VIII) Acquired liver disease, malnutrition, nephrotic syndrome, and heparin infusions. Decrease antithrombin III levels.")
215
Heparin resistance The incidence of heparin resistance is higher in patients with low anti-thrombin III levels. ? Supplementation with AT III fails to increase the ACT to target levels in all patients (some other mechanism) Heparin anti III complex cleared by the reticuloendothelial system Nicholson=> no diference in AT III levels
 Heparin anti III complex cleared by the reticuloendothelial system. Nicholson=> no diference in AT III levels.")
216
Heparin responsiveness is measured by ACT and just may be decreased in patients receiving preop heparin infusions Heparin resistance may be demonstrated by a decrease responsiveness in the ACT

217
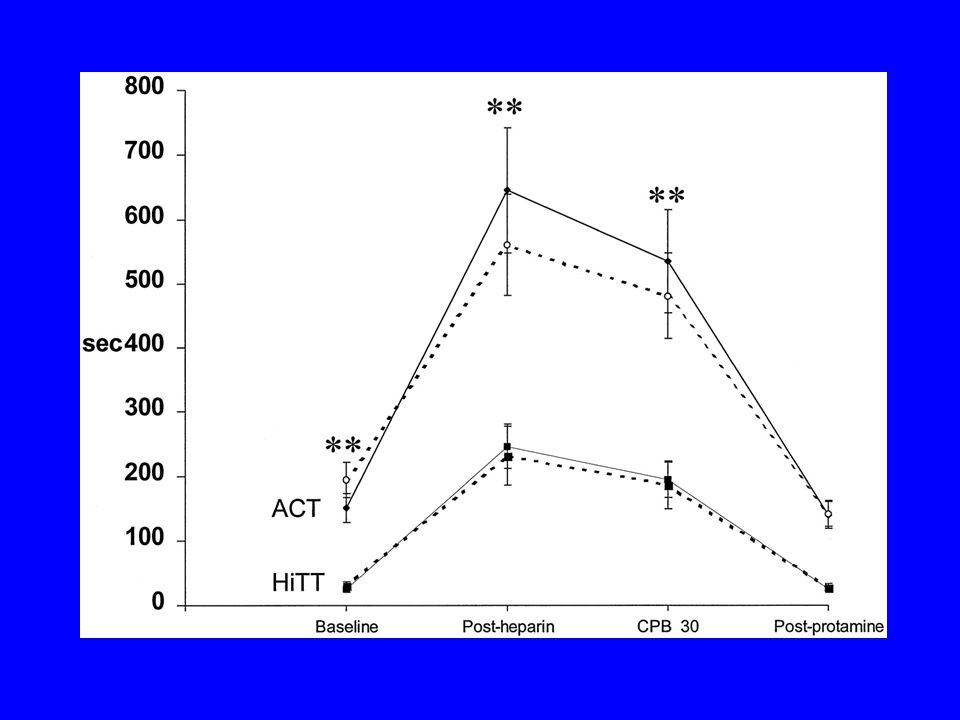
Anticoagulation in patients undergoing cardiac surgery on heparin infusions. Anesth Analg 2000
Patients receiving heparin H (n= 33) vs patients not receiving heparin REF (n=32) Measured ACT and high dose thrombin time ACT values increased less in the H group HiTT values did not differ between groups Thrombin/antithrombin III complex and fibrin monomer not differ
 vs patients not receiving heparin REF (n=32) Measured ACT and high dose thrombin time. ACT values increased less in the H group. HiTT values did not differ between groups. Thrombin/antithrombin III complex and fibrin monomer not differ.")
219
Heparin Resistance > 600 units /kg with ACT no increase > 400 sec. Case reports as large as 1200 units/kg Larger doses associated with increased heparin rebound RX- More heparin FFP Antithrombin III concentrate Accept lower ACT

220
Use of FFP Using FFP to prolong the ACT is based upon case reports
2 units of FFP increase AT III levels to 500 iu Aviden demonstrated 2 units FFP not increase heparin responsiveness in majority of patients

221
Anti thrombin III concentrate
No study demonstrate a reduction in bleeding Anti thrombin III concentrate increases the ACT in heparin resistant patients 500 iu-1000 iu

222
Scenarios

223
Conclusions HMW vs LMW anti thrombin III complexes Factor X vs II
Dosing affects elimination half life Hep resistance rxed with FFP no scientific basis Hep resistance rxed with antithrombin III concentrate expensive but effective Accepting lower target ACT may be most effective

224
Heparin Neutralization
Protamine Pharmacology Assessing Reversal of Anticoagulation Protamine reactions Protamine allergy Who at risk for protamine allergy Site of Administration

225
Protamine Pharmacology

226
Blood conservation strategy
Increase preoperative hemoglobin Implement Acute normovolumic hemodilution Reduce pump prime (mini CPB circuits) Administer Antifibrinolytics Lysine analogues- Amicar or Tranexamic Acid Discontinue preop P2Y12 inhibitors Plavix, effexor
 Administer Antifibrinolytics. Lysine analogues- Amicar or Tranexamic Acid. Discontinue preop P2Y12 inhibitors. Plavix, effexor.")
227
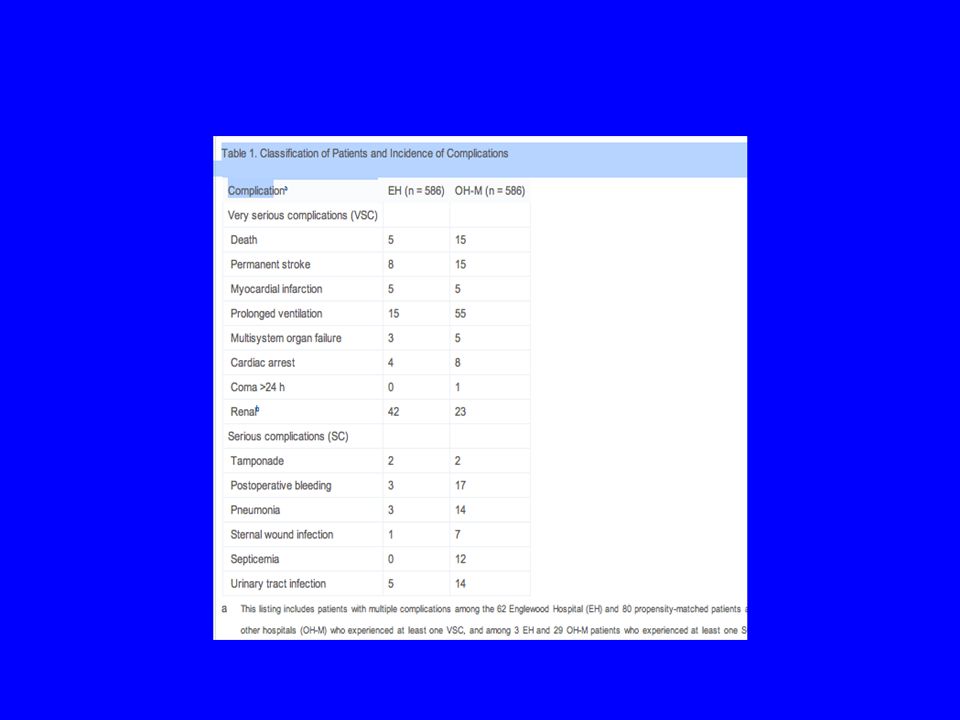
The impact of blood conservation of cardiac surgery: Is it safe and effective. Ann Thorac surg 2010;90:451-9 Englewood Hospital Blood conservation program Permissive anemia Hgb < 6g/dl Acute normovolemic hemodilution Sug technique antifibrinolytics New jersey department heath and senior services registry (32,000 CABG patients)
")
228
586 Englewood Hospital (EH) CABG
586 Other hospital (OH) case matched 10% of EH vs 46% OH received blood transfusion 5 EH vs 15 OH deaths p= .03 Complications ( Stroke, Myocardial infarction, multisystem organ failure, prolonged ventilation,
 case matched. 10% of EH vs 46% OH received blood transfusion. 5 EH vs 15 OH deaths p= .03. Complications ( Stroke, Myocardial infarction, multisystem organ failure, prolonged ventilation,")
230
Conclusion Permissive anemia can be tolerated for cardiac surgical procedures Blood conservation program reduces the incidence of Red blood cell transfusion By reducing Red blood cell transfusion reduce patient mortality and morbidity

231
Blood Conservation Acute normovolemic hemodilution Antifibrinolytics
Retrograde Autologous Priming Decrease prime in CPB mini- circuit Reduced diameter of CPB tubing

232
Acute normovolemic hemodilution
From large bore central catheter remove cc whole blood Can use a-line Remove prior to heparinization Replace volume 1:1 with colloid (5 % salt pure albumin) Reinfuse after CPB, after protamine administration
 Reinfuse after CPB, after protamine administration.")
233
Perioperative blood transfusion and blood conservation in cardiac surgery: The Society of thoracic surgeons and the society of cardiovascular anesthesiologists practice guideline series “Acute normovolemic hemodilution is not unreasonable for blood conservation but its usefulness is not well established.”

234
Acute Normovolemic Hemodilution
Contraindications Hemoglobin < 12 gm / dl or hematocrit < 36% Ejection fraction < 30% Creatinine > 2 mg/dl

235
Acute normovolemic Hemodilution
From large bore central catheter remove cc whole blood Can use a-line Remove prior to heparinization Replace volume 1:1 with colloid (25 % salt pure albumin) Reinfuse after CPB, after protamine administration
 Reinfuse after CPB, after protamine administration.")
236
Perioperative blood transfusion and blood conservation in cardiac surgery: The Society of thoracic surgeons and the society of cardiovascular anesthesiologists practice guideline series “Acute normovolemic hemodilution is not unreasonable for blood conservation but its usefulness is not well established.”

237
Administration of Anti-fibrinolytic
Synthetic lysine analogues - Amino-caproic acid Bolus, 150 mg/kg Infusion, 10 mg/kg/hr Continue 4-6 hours post CPB Aprotinin administration associated with increased perioperative mortality

238
Perioperative blood transfusion and blood conservation in cardiac surgery: The Society of thoracic surgeons and the society of cardiovascular anesthesiologists practice guideline series Lysine analogues limit total blood loss and the number of patients who require blood transfusion after cardiac procedures. These agents are slightly less potent blood-sparing drugs compared with aprotinin but may have a more favorable safety profile

239
Acute normovolemic Hemodilution
Contraindications Hemoglobin < 12 gm / dl or hematocrit < 36% Ejection fraction < 30% Creatinine > 2 mg/dl

240
Heparin Administration
300 units /kg of bovine heparin After IMA dissection 400 units/ kg if on heparin infusion Targeted Activated clotting time > 400 sec Activated clotting times > 480 sec may be associated with less postoperative bleeding

241
Cardiopulmonary Bypass
Maintain muscle relaxation Maintain volatile agent 1 MAC volatile agent Maintain mean arterial pressure MAP > 60 mmHg Maintain amnesia Maintain ACT > 400 seconds if using aprotinin need ACT > 480 seconds

242
Cardiopulmonary bypass
Single clamp technique Decrease incidence neuro injury Distal anastomosis Proximal anastomosis Cardioplegia q 15 min Assess electrical activity Open IMA decrease MAP Minimize reperfusion injury

243
Cardiopulmonary bypass
Maintain tight blood glucose control (< 180) Maintain hemoglobin < 6-7 gms/ dl Maintain hematocrit > 18 % * some recommend Hct > 22% * use cerebral oximetry guide treatment Attempt to avoid transfusion
 Maintain hemoglobin < 6-7 gms/ dl Maintain hematocrit > 18 % * some recommend Hct > 22% * use cerebral oximetry guide treatment Attempt to avoid transfusion")
244
Separation from bypass
Resume full mechanical ventilation Reinflate lungs place on ventilator Achieve target heart rate 90 bpm Atropine, isoproterenol, Beta-dose epi Epicardial pacing ( AOO, DOO, DDD) Achieve target temperature Bladder > 340 C, Esophageal > 370 C When leave OR target temp > 350 C Maintain hemoglobin > 7 gm/dl Reinfuse whole blood removed after protamine Maintain K+ > 4 but < 5.5
 Achieve target temperature. Bladder > 340 C, Esophageal > 370 C. When leave OR target temp > 350 C. Maintain hemoglobin > 7 gm/dl. Reinfuse whole blood removed after protamine. Maintain K+ > 4 but < 5.5.")
245
Emergence Bypass Determine cardiac function
Calculate cardiac index Transesophageal echocardiogram Administer Vasoactive agents If Cardiac Index < 2.0 or echo demonstrates poor ventricular function Reversal of Heparin Protamine Sulfate 250 mg Act return to baseline Protamine not benign 4 types reactions

246
Post bypass Maintain fast track protocol Maintain cardiac function
Target extubation 4- 8 hours after emergence from CPB Maintain cardiac function Continue inotropes Maintain muscle relaxation Readminister vecuronium Redose amnestic and analgesic Begin propofol (expensive, maintain volatile anesthetic) administer midaz or fentanyl
 administer midaz or fentanyl.")
247
Problems post bypass Bleeding Poor cardiac function
Long bypass Previous clopidorel thrombin inhibitors, GP IIbIIIa inhibitors other anticoagulants Poor cardiac function Epinephrine, milrinone, norepinephrine, vasopressin, intra-aortic balloon pump, ventricular assist device Poor respiratory function

248
Affects of Inhalation agent of ischemic myocardium
Ischemic preconditioning Cath lab- inflate balloon for 5 min prior to PTCA Result reduction in myocardial damage “ ischemic preconditioning” Inhalation agents exhibit myocardial protection Activate same pathways as ischemic preconditioning

249
Poor intraoperative blood glucose control is associated with a worsened hospital outcome after cardiac surgery in diabetic patients. Ouattara Anesthesiology 2005;103:677-8

250
Which inhalation agents?
Sevoflurane Isoflurane Desflurane

251
Coagulation Factors Bradykinin levels increase 10 fold with CPB
Elevated bradykinins induce secretion of TPA 5 fold increase in TPA levels increase in plasmin generation with CPB Fibrin consumption occurs during cpb

252
Contact activation XII, XI, bradykinin, HMWK and prekallikrein- rapidly degraded by kinins XII auto-cleaves itself when in contact with the CPB circuit XII activates Kalllikreins which feedbacks and cleaves XII Binds to the circuit

253
Platelet Cascade

254
Platelets

255
Two Phase Model

256
Glucose levels- 150- 200- then 125-175 then 100-150
Continuous insulin infusion reduces mortality in patients with diabetes undergoing coronary artery bypass Anthony P. Furnary, MDa,d, Guangqiang Gao, MDa, Gary L. Grunkemeier, PhDb, YingXing Wu, MDb, Kathryn J. Zerr, MBAb, Stephen O. Bookin, MDc, H. Storm Floten, MDa,d, Albert Starr, MDa,d Staged trial 1st- subcutaneous administration of insulin- 2nd stage insulin infusion Glucose levels then then

257
CPB upsets Coagulation balance
CPB circuit is foreign surface Activates coagulation cascade and inflammatory response (leukocytes host attacks) Platelet activation and coat the CPB circuit First pass decreases antithrombin III levels Paralysis of the coagulation cascade by heparin - hemodilution Hypothermia Stimulus of coagulation and pro-inflammatory mediators
 Platelet activation and coat the CPB circuit. First pass decreases antithrombin III levels. Paralysis of the coagulation cascade by heparin - hemodilution. Hypothermia. Stimulus of coagulation and pro-inflammatory mediators.")
258
Heparin Heparin binds to circulating antithrombin and causes a conformational change that accelerates its binding to and inactivation of three critical coagulation factors: Thrombin, Xa, and IXa Heparin also has both direct and indirect antiplatelet effects heparin binds to vWf at a site critical for binding to platelet GPIb

259
End result Prothrombin => thrombin Fibrinogen cleaved to fibrin
Basic structure of clot

Similar presentations