Download presentation
Presentation is loading. Please wait.

1
Sleep Apnea and Cardiovascular Disease
Mohammed Fakhry AbdulMohsen, MD, FACC Associate Professor and Consultant Internist/Cardiologist University of Dammam and King Fahd Hospital of the University.

2
Sleep Apnea and Cardiovascular Disease
Sleep-related breathing disorders are highly prevalent in patients with established cardiovascular disease. Obstructive Sleep Apnea (OSA) affects adult Americans and is present in large number of patients with HTN and other CVD such as CAD, Stroke and AF. Central Sleep Apnea (CSA) occurs mainly in patients with Heart Failure (HF)
 affects adult Americans and is present in large number of patients with HTN and other CVD such as CAD, Stroke and AF. Central Sleep Apnea (CSA) occurs mainly in patients with Heart Failure (HF)")
3
Sleep Apnea and Cardiovascular Disease
Objectives: To describe the types and prevalence of SA and its relevance to individuals who are at risk for or already have established CVD. To help develop the platform from which with the collaboration with specialist in sleep medicine and related disciplines, such consensus may develop.

4
Sleep Apnea and Cardiovascular Disease

5
Sleep Apnea and Cardiovascular Disease
1. Airway narrowing/obstruction 2. Decreased air flow 3. Increased effort 4. Oxygen saturation swings and hypoxia 5. Increased BP and HR 6. Disrupted sleep

6
Sleep Apnea and Cardiovascular Disease

7
Sleep Apnea and Cardiovascular Disease

8
Sleep Apnea and Cardiovascular Disease

9
Sleep Apnea and Cardiovascular Disease
Table 1. Definitions of Terms (5) Apnea: Cessation of airflow for 10 s Hypopnea: A reduction in but not complete cessation of airflow to 50% of normal, usually in association with a reduction in oxyhemoglobin saturation AHI: The frequency of apneas and hypopneas per hour of sleep; a measure of the severity of sleep apnea OSA and hypopnea: Apnea or hypopnea resulting from complete or partial collapse, respectively, of the pharynx during sleep
 Apnea: Cessation of airflow for 10 s. Hypopnea: A reduction in but not complete cessation of airflow to 50% of normal, usually in association with a reduction in oxyhemoglobin saturation. AHI: The frequency of apneas and hypopneas per hour of sleep; a measure of. the severity of sleep apnea. OSA and hypopnea: Apnea or hypopnea resulting from complete or partial collapse, respectively, of the pharynx during sleep.")
10
Sleep Apnea and Cardiovascular Disease
Table 1. Definitions of Terms (5) CSA and hypopnea: Apnea or hypopnea resulting from complete or partial withdrawal of central respiratory drive to the muscles of respiration during sleep Oxygen desaturation: Reduction in oxyhemoglobin saturation, usually as a result of an apnea or hypopnea Sleep apnea syndrome: At least 10 to 15 apneas and hypopneas per hour of sleep associated with symptoms of sleep apnea, including loud snoring, restless sleep, nocturnal dyspnea, headaches in the morning, and excessive daytime sleepiness
 CSA and hypopnea: Apnea or hypopnea resulting from complete or partial withdrawal of. central respiratory drive to the muscles of respiration during. sleep. Oxygen desaturation: Reduction in oxyhemoglobin saturation, usually as a result of an apnea or. hypopnea. Sleep apnea syndrome: At least 10 to 15 apneas and hypopneas per hour of sleep associated with. symptoms of sleep apnea, including loud snoring, restless sleep, nocturnal. dyspnea, headaches in the morning, and excessive daytime sleepiness.")
11
Sleep Apnea and Cardiovascular Disease
Table 1. (Cont’d) Polysomnography: Multichannel electrophysiological recording of electroencephalographic, electrooculographic, electromyographic, ECG, and respiratory activity to detect disturbance of breathing during sleep NREM sleep: Non–rapid eye movement or quiet sleep REM sleep: Rapid eye movement or active sleep; associated with skeletal muscle atonia, rapid movements of the eyes, and dreaming Arousal: Transient awakening from sleep lasting 10 s
 Polysomnography: Multichannel electrophysiological recording of. electroencephalographic, electrooculographic, electromyographic, ECG, and respiratory activity to detect disturbance of breathing. during sleep. NREM sleep: Non–rapid eye movement or quiet sleep. REM sleep: Rapid eye movement or active sleep; associated with skeletal. muscle atonia, rapid movements of the eyes, and dreaming. Arousal: Transient awakening from sleep lasting 10 s.")
12
Sleep Apnea and Cardiovascular Disease
Table 2: Obstructive Sleep Apnea Signs, symptoms, and risk factors: - Disruptive snoring - Witnessed apnea or gasping - Obesity and/or enlarged neck size - Hypersomnolence - Other signs and symptoms include male gender, crowded-appearing pharyngeal airway, HTN, morning headache, sexual dysfunction, behavioral changes (especially in children)
")
13
Sleep Apnea and Cardiovascular Disease
Screening and diagnostic tests - Questionnaires - Holter monitoring - Overnight oximetry - Home-based/ambulatory unattended polysomnography - In-hospital attended overnight polysomnography. Treatment options: - Positional therapy - Weight loss - Avoidance of alcohol and sedatives - Positive airway pressure - Oral appliances

14
Sleep Apnea and Cardiovascular Disease
Table 3: Central Sleep Apnea (CSA) Signs, symptoms, and risk factors: Congestive heart failure Paroxysmal nocturnal dyspnea Witnessed apnea Fatigue/hypersomnolence Other signs and symptoms include male gender, older age, mitral regurgitation, atrial fibrillation, Cheyne Stokes Respiration (CSR) while awake, hyperventilation with hypocapnia
 Signs, symptoms, and risk factors: Congestive heart failure. Paroxysmal nocturnal dyspnea. Witnessed apnea Fatigue/hypersomnolence. Other signs and symptoms include male gender, older age, mitral regurgitation, atrial fibrillation, Cheyne Stokes Respiration (CSR) while awake, hyperventilation with hypocapnia.")
15
Central Sleep Apnea In HF
Figure 2. Schematic outlining possible mechanisms underlying development of CSA and the possible feedback from CSA resulting in exacerbation of heart failure.

16
Sleep Apnea and Cardiovascular Disease
Table 3: Central Sleep Apnea (CSA): Screening and diagnostic tests: Overnight oximetry Ambulatory (unattended) polysomnography In-hospital (attended) polysomnography Treatment options: Optimize treatment of heart failure Positive airway pressure Supplemental oxygen
: Screening and diagnostic tests: Overnight oximetry. Ambulatory (unattended) polysomnography. In-hospital (attended) polysomnography. Treatment options: Optimize treatment of heart failure. Positive airway pressure. Supplemental oxygen.")
17
Sleep Apnea and Cardiovascular Disease
OSA and Cardiovascular disease: There is a clear association between OSA and cardiovascular disease Higher incidence of adverse cardiovascular events in untreated patients with OSA Postgrad Med J 2008; 84:15-22 SLEEP 2007;30(3): CHEST 2008; 133: Proc Am Thorac Soc 2008; 5:
: CHEST 2008; 133: Proc Am Thorac Soc 2008; 5:")
18
Sleep Apnea and Cardiovascular Disease
Postgrad Med J 2008; 84:15-22

19
OSA is an independent risk for
hypertension

20
OSA and Hypertension:

21
OSA and Hypertension, Why does it happen?
OSA can lead to hypoxia (low oxygen levels), repetitive changes in oxygen saturations, and large swings in intrathoracic pressures These changes are detected by receptors in the brain and in the periphery (carotid bodies) Stimulate a sympathetic response (“fight or flight response”, “stress” response) increased heart rate and blood pressure Postgrad Med J 2008; 84:15-22
, repetitive changes in oxygen saturations, and large swings in intrathoracic pressures. These changes are detected by receptors in the brain and in the periphery (carotid bodies) Stimulate a sympathetic response ( fight or flight response , stress response) increased heart rate and blood pressure. Postgrad Med J 2008; 84:")
22
OSA and Hypertension Why does it happen?
Repeated stimulation increased sympathetic tone during the day High blood pressure Studies have showed: Increased tonic chemoreflex drive Abnormalities in HR and BP variabilities during normal awake hours in patients with OSA Postgrad Med J 2008; 84:15-22

23
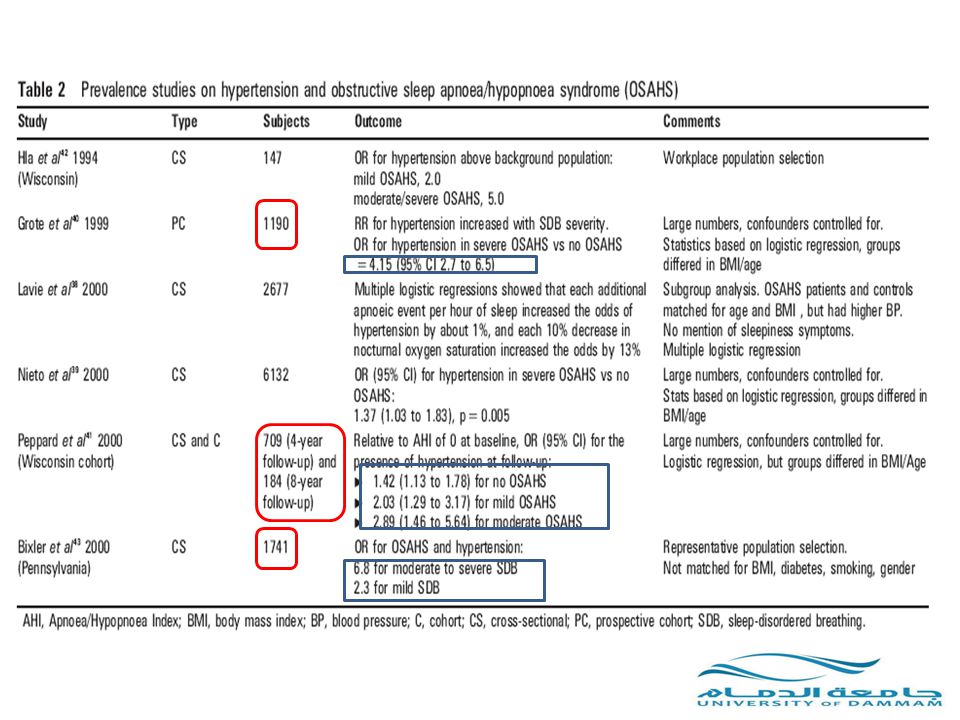
OSA and Hypertension Some Numbers
Wisconsin prospective sleep cohort (2000) 709 patients with OSA Risk of developing HTN over 4 years: Minimal OSA: 1.42 x normal Mild-moderate: 2.03 x normal Moderate-severe: 2.89 x normal After adjusting for other risk factors
 709 patients with OSA. Risk of developing HTN over 4 years: Minimal OSA: 1.42 x normal. Mild-moderate: 2.03 x normal. Moderate-severe: 2.89 x normal. After adjusting for other risk factors.")
24
OSA and Hypertension Some Numbers
~40% of people with OSA have HTN while awake 40-80% of people with non-controlled HTN have OSA

26
OSA and Hypertension How to treat it?
Effective CPAP therapy can reduce BP One study showed a fall in systolic BP by 10 mmHg after 4 weeks of CPAP Improvement in blood pressure correlated with improvement in sleepiness

27
OSA and Coronary Artery Disease

28
OSA and Heart Attacks People with sleep disordered breathing (SDB) have a high prevalence of coronary heart disease (CHD) People with CHD have a high prevalence of SDB

29
OSA and Heart Attacks: Why does it Happen?
Multiple nightly stresses on the heart: Repetitive fluctuations in oxygen levels Increased blood pressure surges High sympathetic nervous system tone

30
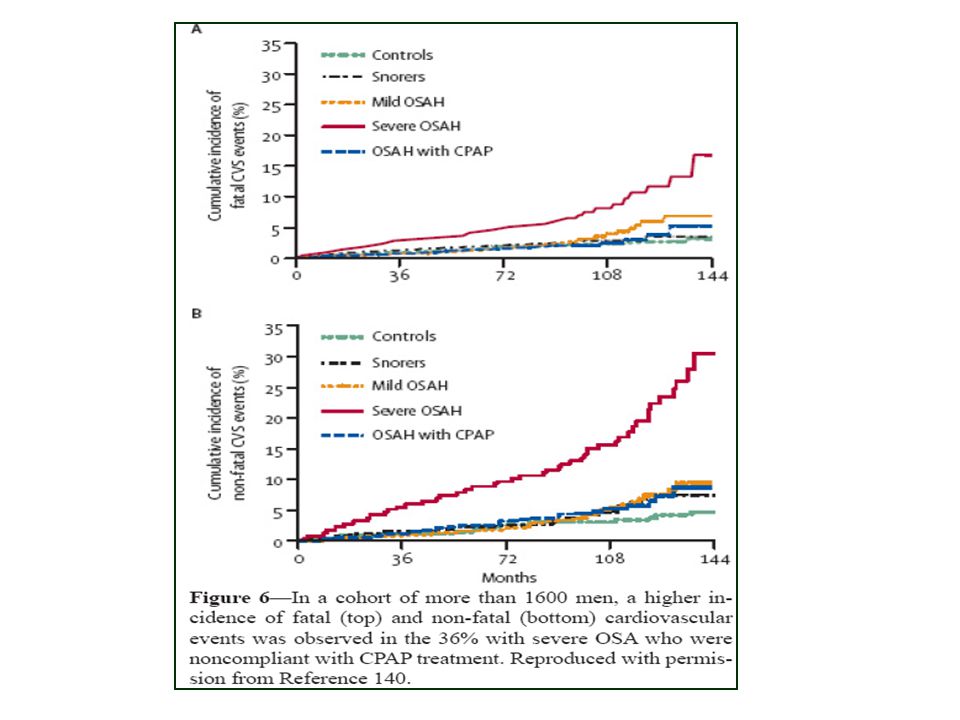
OSA and Heart Attacks Marin et al. 2005
10 year follow-up study looking at CV events and OSA (including heart attacks and strokes) Included 264 healthy men, 377 snorers, 403 untreated mild-mod OSA, 235 untreated severe OSA and 372 treated with CPAP
 Included 264 healthy men, 377 snorers, 403 untreated mild-mod OSA, 235 untreated severe OSA and 372 treated with CPAP.")
32
OSA and Heart Attacks Gami et al. looked at 112 patients who underwent a sleep study Followed them for 5 years Sudden death from cardiac causes (between midnight and 6 am) occurred in 46% of pts with OSA vs 16% of general population
 occurred in 46% of pts with OSA vs 16% of general population.")
33
OSA and Heart Failure

34
OSA and Heart Failure CSA is the SDB most commonly associated with HF. Javaheri 2006→ 49% with CHF have SDB (37% CSA, 12% OSA) Heart Failure is 2.38 x more common in “mild-moderate OSA” than in “no OSA” Postgrad Med J 2008; 84:15-22

35
OSA and Heart Failure: Why does it happen?
Hypertension Left ventricular diastolic dysfunction Atrial fibrillation CHEST 2008; 133:793–804

36
OSA and Heart Failure: Effect of treatment
2 randomized studies of CPAP for OSA in CHF, showed some improvement in EF over 1-3 months Effect of CPAP treatment on mortality/morbidity from heart failure is unknown CHEST 2008; 133:793–804

37
Sleep Apnea and Cardiovascular Disease

38
OSA and Cardiac Arrhythmias

39
OSA and Cardiac Arrhythmias
Abnormal heart rhythms have been associated with OSA 1983 Guilleminault et al.: 400 pts with OSA 48% had cardiac arrhythmias at night 2% sustained VT, 11% sinus arrest, 8% AV block, 19% PVC Postgrad Med J 2008; 84:15-22

40
OSA and Cardiac Arrhythmias; Atrial Fibrillation:
Four times increased risk of AF in pts with OSA (AHI>30) (Sleep Heart Health Study 2006) Onset of >75% of persistent A fib episodes in pts with OSA occur at night (8pm-8am) A fib recurrence after cardioversion twice as high in untreated OSA Observational review over 17 yrs suggests that nocturnal hypoxemia influences the onset of A fib Postgrad Med J 2008; 84:15-22 Proc Am Thorac Soc 2008; 5:
 (Sleep Heart Health Study 2006) Onset of >75% of persistent A fib episodes in pts with OSA occur at night (8pm-8am) A fib recurrence after cardioversion twice as high in untreated OSA. Observational review over 17 yrs suggests that nocturnal hypoxemia influences the onset of A fib. Postgrad Med J 2008; 84: Proc Am Thorac Soc 2008; 5:")
41
OSA and Cardiac Arrhythmias; Ventricular Arrhythmias:
Reported in pts with OSA Causative role not proven NEJM 2005, a study observed higher incidence of sudden death during night hours (12am-6am) in pts with OSA, suggesting but not proving a causative effect Proc Am Thorac Soc 2008; 5:
 in pts with OSA, suggesting but not proving a causative effect. Proc Am Thorac Soc 2008; 5:")
42
Sleep Apnea and Cardiovascular Disease

43
OSA and Strokes

44
OSA and Strokes OSA is a risk factor for stroke
2 prospective cohort studies following 1022 and 1651 pts found a higher incidence of stroke in OSA SLEEP, Vol. 30, No. 3, 2007

45
OSA and Strokes: Why does it happen?
Increased CRP (inflammation) and atherogenesis Increased thrombotic risks (clotting of blood) Increased blood pressure Hypoxia Theoretically PFO? SLEEP, Vol. 30, No. 3, 2007
 and atherogenesis. Increased thrombotic risks (clotting of blood) Increased blood pressure. Hypoxia. Theoretically PFO SLEEP, Vol. 30, No. 3,")
46
OSA and Strokes; Treatment effect:
No randomized controlled trials Observational studies are controversial on whether treatment of OSA would prevent strokes or not SLEEP, Vol. 30, No. 3, 2007

47
SLEEP, Vol. 30, No. 3, 2007

48
Sleep Apnea and Cardiovascular Disease
SLEEP, Vol. 30, No. 3, 2007

49
Thank you!

Similar presentations




 286-7455 Fax: (703) 286-7462.>")


 Necessary for Physical and Mental Health $50 Billion / Year in Lost Productivity Occupies 1/3 of our Lives.>")











