Download presentation
Presentation is loading. Please wait.

1
Stanford Hospital and Clinics John Morton, MD, MPH, FACS
Beyond SCIP Stanford Hospital and Clinics John Morton, MD, MPH, FACS

2
Surgical Safety A serious public health issue
Globally, 234 million operations/yr With a mortality rate of % and 3- 16% complications rate: 1 million deaths 7 million disabling complications

3
SF Chronicle

4
Update: FY 2010 SCIP CORE MEASURES

5
Surgical care improvement project
SCIP is one of four categories of Core Measures The Surgical Care Improvement Project (SCIP) is a national quality partnership of organizations interested in improving surgical care by significantly reducing surgical complications. Each of the SCIP target areas are advised by a technical expert panel and supported by evidence-based research.
 is a national quality partnership of organizations interested in improving surgical care by significantly reducing surgical complications. Each of the SCIP target areas are advised by a technical expert panel and supported by evidence-based research.")
6
FY2010 SCIP CORE measures SCIP INF 1: Patient receives prophylactic antibiotic within minutes prior to surgical incision. SCIP INF 2: Patient receives prophylactic antibiotics consistent with current recommendations identified in published guidelines. SCIP INF 3: Prophylactic antibiotics are discontinued within hours of surgery end time (48 hours for cardiac surgery). SCIP INF 4: Glucose control in cardiac surgery patients. SCIP INF 6: Surgery patients with appropriate hair removal.
. SCIP INF 4: Glucose control in cardiac surgery patients. SCIP INF 6: Surgery patients with appropriate hair removal.")
7
FY2010 SCIP CORE measures SCIP CARD 2: Beta Blocker therapy prior to Admission who Received a Beta Blocker During the Perioperative Period SCIP VTE 1: Surgery patients with recommended VTE prophylaxis SCIP VTE 2: Surgery patients who received appropriate VTE prophylaxis within 24 hours prior to surgery to 24 hours after surgery, 48 hours for CABG and other cardiac surgery. SCIP-INF-9: Urinary Catheter Removed on Postoperative Day (POD 1) or by midnight on Postoperative Day 2 (POD 2). SCIP-Inf-10 Surgery Patients with Perioperative Temperature Management. NEW NEW
 or by midnight on Postoperative Day 2 (POD 2). SCIP-Inf-10 Surgery Patients with Perioperative Temperature Management. NEW. NEW.")
8
SCIP Infection Measure - 9
Measure: Indwelling Urinary Catheter Removed on POD 1 or by midnight on POD 2 Science-based rationale: Studies have shown that the longer indwelling urinary catheters remain in patients the greater risk of UTI. Inclusion criteria: Indwelling catheters: Foley catheter 3-Way catheter, Coude catheter, Council tip catheter Intermittent catheters: “in and out” catheterization, Texas catheter, “prn” catheterization for residual urine, self-catheterization, straight catheterization, “spot” catheterization Exclusion criteria: External catheter Exceptions to removing catheter: Urological, GYN, Perineal procedures Planned return to OR Suprapubic catheter

9
Potential Exclusion Criterion
Urological, gynecological or perineal procedure performed ICU bed and documentation of receiving diuretics Other surgical procedures that occurred within 3 days (4 days for CABG) prior to or after the procedure of interest Physician documented infection prior to surgical procedure Length of stay < two days postoperatively Suprapubic catheter or had intermittent catheterization preoperatively No catheter in place postoperatively Physician documentation of a reason for not removing the urinary catheter postoperatively Example: “Foley retained to monitor accurate input and output”
 prior to or after the procedure of interest. Physician documented infection prior to surgical procedure. Length of stay < two days postoperatively. Suprapubic catheter or had intermittent catheterization preoperatively. No catheter in place postoperatively. Physician documentation of a reason for not removing the urinary catheter postoperatively Example: Foley retained to monitor accurate input and output")
10
SCIP Infection Measure - 9
Documentation that the catheter was removed on POD 1 or POD 2 with Anesthesia End Date being POD 0 (POD 2 ends at midnight on the second post-op day) Role of Surgeons: Documentation of the reason why urinary catheter needs to stay in longer than midnight on POD 2. An order to just “continue catheter” will not suffice. Example: The patient required ICU care AND receiving diuretics”. Role of RNs: Check physicians’ orders to discontinue catheter and then discontinue catheter asap and document removal.
 Role of Surgeons: Documentation of the reason why urinary catheter needs to stay in longer than midnight on POD 2. An order to just continue catheter will not suffice. Example: The patient required ICU care AND receiving diuretics . Role of RNs: Check physicians’ orders to discontinue catheter and then. discontinue catheter asap and document removal.")
11
SCIP Infection Measure - 10
Measure: Surgery Patients with Perioperative Temperature Management Science-based rationale: Studies have shown that hypothermia has been associated with adverse outcomes, including impaired wound healing, adverse cardiac events, altered drug metabolism, increased infection and coagulopathies. Documentation of at least one body temperature greater than or equal to 36° C within the 30 minutes immediately prior to or 15 minutes immediately after Anesthesia End Time (i.e. time associated with the anesthesia providers “signoff” after principal procedure).
.")
12
SCIP Infection Measure - 10
Anesthesiologists: Temperature must be 36 degrees or higher by end of surgery, unless “Intentional Hypothermia” is documented in medical record. Document core temperature on anesthesia record 30 minutes before patient is transferred. Physicians/CRNAs need to document “intentional” hypothermia during perioperative period. PACU and ICU RNs: Obtain and document temperature within first 15 minutes after patient arrives in unit.

13
Potential Exclusion Criterion
Patients whose length of anesthesia was less than 60 minutes Patients who did not have general or neuraxial anesthesia Patients who received Intentional Hypothermia for the procedure performed.

14
Focus on outstanding surgical care Remove urinary catheters by POD 2
SCIP Measure effective NOW Surgeons: Document reason catheter needs to stay in longer Example: “Foley retained to monitor accurate urine output” Exceptions to removing catheter: Urological, GYN, and Perineal procedures Planned return to OR In ICU and receiving diuretic on POD1 or POD2 RNs: Check MD orders for the DC Catheter order Ask MD to document any exceptions Document! Document!

15
Focus on outstanding surgical care
Perioperative Temperature Management SCIP Measure effective NOW Anesthesiologists: Temperature must be 36º C /96.8ºF degrees or higher at handoff to PACU/ICU RNs, unless Intentional Hypothermia is documented Document End of Anesthesia time & final temperature Document use of Bair Hugger PACU and ICU RNs: Temp must be taken and documented within 15 minutes of handoff by Anesthesiologist Document! Document!

16
Surgical Care Improvement Project (SCIP)
SHC Goal: Increase compliance for the following measures to 90%: SCIP Inf 1—Antibiotic received with one hour prior to incision SCIP Inf 2—Antibiotic selection SCIP Inf 3—Antibiotic discontinued within 24 hours after surgery time SCIP VTE 1—Surgery patients with recommended VTE prophylaxis ordered SCIP VTE 2—Surgery patients who received appropriate VTE prophylaxis within 24 hours prior to surgery to 24 hours after surgery

18
COLLABORATION

19
How did we get here? 1 YEAR MORTALITY RATE 4.6%

20
Accreditation in Bariatric Surgery
CMS National Coverage Determination February, 2006 CMS will approve and reimburse procedures at a program accredited by one of the two programs: ▪ ASBS/ Surgical Review Corporation. American College of Surgeons – Bariatric Surgery Centers

21
37% 24% 21% 21%

22
7000 cases ? mortalities 2

23
NSQIP- SSI Observed Rate: 6.96% Expected Rate: 5.14% O/E Ratio: 1.35
Status: Needs Improvement * Includes General and Vascular Surgery Cases

24
Semiannual Report, July 2009
American College of Surgeons National Surgical Quality Improvement Program Semiannual Report, July 2009 Dates of Surgery: January 1, 2008 – December 31, 2008 Stanford Hospital and Clinics

25
A Means For Improvement
Stanford Cedars Sinai Mayo Clinic University of MN Saint Francis OSF North Shore – LIJ Cleveland Clinic Northwestern American College of Surgeons Targeted Solutions Tool Share solutions with 16,000 accredited institutions Targeted Solutions Tool™ (TST) encapsulates the work of the Joint Commission Center for Transforming Healthcare -TST is an application that guides health care organizations through a step-by-step process to accurately measure their organization’s actual performance, identify their barriers to excellent performance, and direct them to proven solutions that are customized to address their particular barriers. TST provides a step-by-step process to measure performance, identify barriers to excellent performance, and implement proven solutions TST provides accredited hospitals the foundation and framework of an improvement method that, if implemented well, will improve an organization's compliance Complimentary data-driven tool provides validated and customized solutions to address an organization's particular barriers to excellent performance Self paced and confidential, the TST offers instantaneous data analysis
 encapsulates the work of the Joint Commission Center for Transforming Healthcare. -TST is an application that guides health care organizations through a step-by-step process to accurately measure their organization’s actual performance, identify their barriers to excellent performance, and direct them to proven solutions that are customized to address their particular barriers. TST provides a step-by-step process to measure performance, identify barriers to excellent performance, and implement proven solutions. TST provides accredited hospitals the foundation and framework of an improvement method that, if implemented well, will improve an organization s compliance. Complimentary data-driven tool provides validated and customized solutions to address an organization s particular barriers to excellent performance. Self paced and confidential, the TST offers instantaneous data analysis.")
26
Looked for a procedure/outcome that:
Joint Commission Center for Transforming Healthcare - American College of Surgeons Surgical Site Infection Project Looked for a procedure/outcome that: Is common across different types of hospitals Complications have significant, adverse clinical impact High variability in performance across hospitals Ideal Candidate = SSI in colorectal surgery

27
Joint Commission Center for Transforming Healthcare - American College of Surgeons Surgical Site Infection Project Participating Hospitals Cedars-Sinai, Cleveland Clinic, Mayo Clinic, Northwestern North Shore Long Island Jewish, OSF Saint Francis, Stanford In August 2010, CTH launched its fourth project in collaboration with ACS on SSI NSQIP data on outcomes of surgery are widely regarded as highly reliable, with exemplary risk-adjusted outcomes

28
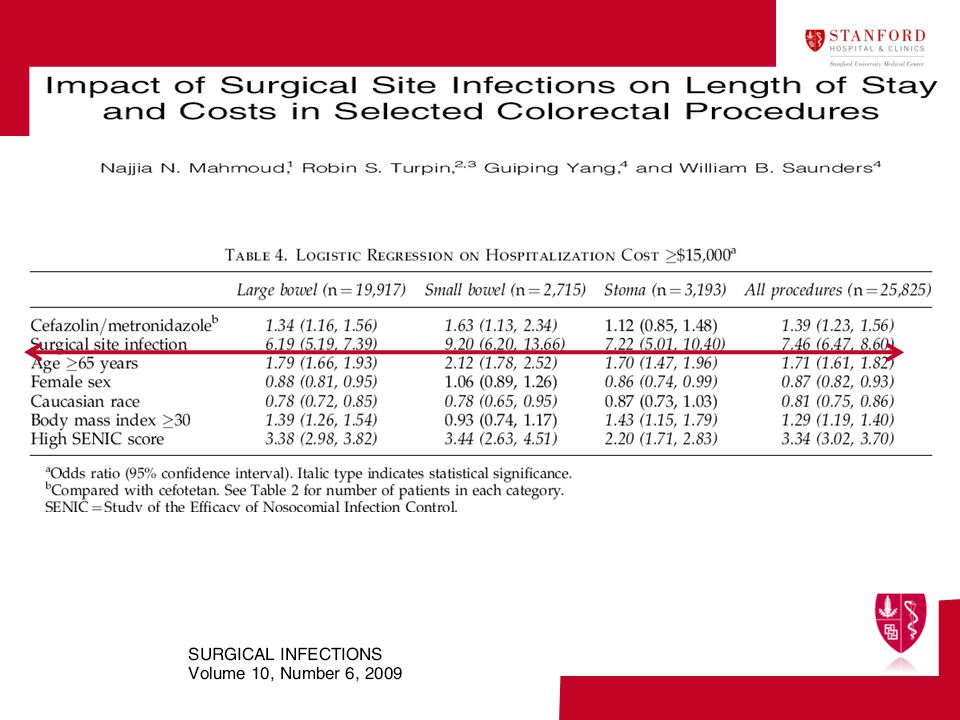
Impact of SSI Year 2008: SSIs generate an average of $28,211 in extra costs per case and comprise 38% of all morbidities. (ACS NSQIP, Business case, 2008) SSI’s add an additional 7-9 excess hospital days per case. (Infection Control Today, 2002)
 SSI’s add an additional 7-9 excess hospital days per case. (Infection Control Today, 2002)")
30
NSQIP Impact Mortality 33% Reduction Morbidity 50% Reduction
Khuri, Ann Surg, 2002

31
NSQIP Colorectal SSI Reduction ? NONE 15% REDUCTION INCREASE NONE

32
Complex Change

33
ICU Catheter Infections 2001-2009
It Doesn’t Work…. 63% Reduction ICU Catheter Infections

34
Motivation Needed?

35
Change Management

36
New Rules Dialogue is almost always a signpost on the road to quality improvement Quality is not a personal virtue; it is an performance expectation that is accountable and rewarded. If you knock one down, you got to put up another one CAN NOT KEEP DOING THE SAME

37
Three trials of 1443 Participants compared bar soap with chlorhexidine; when combined there was no difference in the risk of SSIs (RR 1.02, 95% CI 0.57 to 1.84). Three trials of 1192 patients compared bathing with chlorhexidine with no washing, one large study found a statistically significant difference in favour of bathing with chlorhexidine (RR 0.36, 95%CI 0.17 to 0.79). ITS SOAP!!!!
. Three trials of 1192 patients compared bathing with chlorhexidine with no washing, one large study found a statistically significant difference in favour of bathing with chlorhexidine (RR 0.36, 95%CI 0.17 to 0.79). ITS SOAP!!!!")
38
COLECTOMY IS A COST AND DEFECT MULTIPLIER

39
Pareto Curve

41
BMI: Modifiable? 2009 Colorectal Cases (All NSQIP Hospitals) Class I obesity ( ): % Class II obesity ( ): % Class III obesity (40): % ______________________________________________________________________________ 40% of Total Population with BMI > 30 13.23% of Total Population with Cancer 1/3 of our patients could benefit from pre-op surgical weight loss
: 10.19% Class III obesity (40): 8.00% ______________________________________________________________________________. 40% of Total Population with BMI > % of Total Population with Cancer. 1/3 of our patients could benefit from pre-op surgical weight loss.")
45
Science of SSI ( The development of an SSI is a multifactorial and not dependent on perioperative antibiotic administration alone. Prophylactic Antibiotics Wound Oxygen Tension (↑O2 = ↓SSI risk) Normothermia Mild hypothermia, 1-2°C, increases wound infection rate. (Kurz, NEJM, 1996) Glucose Control (↑Hyperglycemia = ↑SSI risk)
 Normothermia. Mild hypothermia, 1-2°C, increases wound infection rate. (Kurz, NEJM, 1996) Glucose Control (↑Hyperglycemia = ↑SSI risk)")
46
What can be the following step?
Further multivariate analysis of SSI risk factors Diabetes* Poor nutritional status* Medications* Body habitus Age Emergent surgery Post discharge follow up and care

47
What can be the following step?
Identify pathogen Pattern recognition OR traffic Redosing

48
Surgical Site Infection Prevention Strategies
Standardized OR Preps Preps w/highest efficacy (Chloraprep / Duraprep) Surgery Chlorhexidine Guidelines Outpatient Clinics: Provide patient with (4%) CHG EZ scrub sponges for Baths/Showers for pre-op skin prep night before surgery Pre Operative Units: If patient does not use (4%) CHG scrub RN to provide (2%) CHG wipes for use day of surgery Inpatient Units Nurses: Provide pre-operative antimicrobial skin prep using (2%) CHG Cloths night before or morning of surgery
 Surgery Chlorhexidine Guidelines. Outpatient Clinics: Provide patient with (4%) CHG EZ scrub sponges for Baths/Showers for pre-op skin prep night before surgery. Pre Operative Units: If patient does not use (4%) CHG scrub RN to provide (2%) CHG wipes for use day of surgery. Inpatient Units Nurses: Provide pre-operative antimicrobial skin prep using (2%) CHG Cloths night before or morning of surgery.")
49
Phase II (May – November 2010)
Service Specific Drill Down Review current practice for alignment with evidence based practice Antibiotic Re-dosing on OR Complex cases & cases longer than 4 hours; define re-dosing timeframe Cath Lab / ACS Cases “Small test of Change” pilot for EPS (Pace Maker and ICD cases ) Develop measurement and reporting mechanisms Adherence to dispensing of CHG shower/bath prior to surgery Boarding Pass for compliance with CHG shower/bath prior to surgery Post Operative Incision Care Guidelines Service specific “Surgical Wound Guidelines” Joint Commission Center for Transforming Healthcare American College of Surgeons NSQIP Project
 Develop measurement and reporting mechanisms. Adherence to dispensing of CHG shower/bath prior to surgery. Boarding Pass for compliance with CHG shower/bath prior to surgery. Post Operative Incision Care Guidelines. Service specific Surgical Wound Guidelines Joint Commission Center for Transforming Healthcare. American College of Surgeons NSQIP Project.")
Similar presentations





: What the Direct Caregiver Should Know>")

>")
>")

 Mark Wong, Pharm.D., BCPS 1,2,3 ; George Melnik, Pharm.D., BCPS, 1,2 South.>")






 Key Facts Three year demo (2003-2006); extended for three additional years through Oct. 2009 225 hospitals.>")





