Download presentation
Presentation is loading. Please wait.

1
Principles of Chest X-Ray Interpretation
Dr Rod Taylor Consultant Respiratory Physician

2
Different from us….

3
Only Two Choices Hmmn! There are far too many white bits!
That’s funny - this one’s got too many black bits!

5
= important radiological
Chest X-ray P = important radiological principle

6
Vertebral spines equidistant
The Normal CXR Vertebral spines equidistant Horizontal fissure Left hilum Cardiophrenic angle Descending aorta Right diaphragm Costophrenic angle

7
It’s All Relative… 1 P Stupid humans…

8
P Why Does It Show Up? Because there is something
of a different radiological density next to it. Four main densities: P

9
Étienne de Silhouette The silhouette sign If a structure shows up,
there must be adjacent to it something of a different radiological density. If a structure does not show up, there must be adjacent to it something of a similar Controller-General of Finances during the Seven Years War (1754 – 63)
")
10
Silhouetted Hills This one doesn’t This hill shows up

11
Rotation PA

12
The Lobes Front Back

13
Lateral View (Right) Upper Lobe Middle Lobe Lower Lobe Heart Oblique
fissure Upper Lobe Apical segment of lower lobe Middle Lobe Lower Lobe Horizontal fissure Heart Vertebral bodies appear to darken

14
Lateral View (Left) Upper Lobe Lingula Lower Lobe Heart No fissure
(normally) Upper Lobe Oblique fissure Lingula Lower Lobe Heart
 Upper. Lobe. Oblique. fissure. Lingula. Lower. Lobe. Heart.")
15
Naming of Segments Apical Medial Anterior Posterior Lateral

16
Don’t Forget…. The bones Gas under the diaphragm
Has this patient had a chest x-ray? Oh, good, then I can start! Gas under the diaphragm

17
P It’s All Relative… 2 Look for collateral evidence Normal CXR Too
White? Too Black? Normal CXR P Look for collateral evidence

18
P What Do You See? The most obvious abnormality is
likely to be the primary event. Other, more subtle, changes are likely to be secondary to this. P

20
The Man in the Street Dryclough Lane
Er, there’s a white bit on the right… at the top… um… which comes… ooh, about halfway down… with a sharp, um, line, at the bottom…

21
Right Upper Lobe Consolidation

22
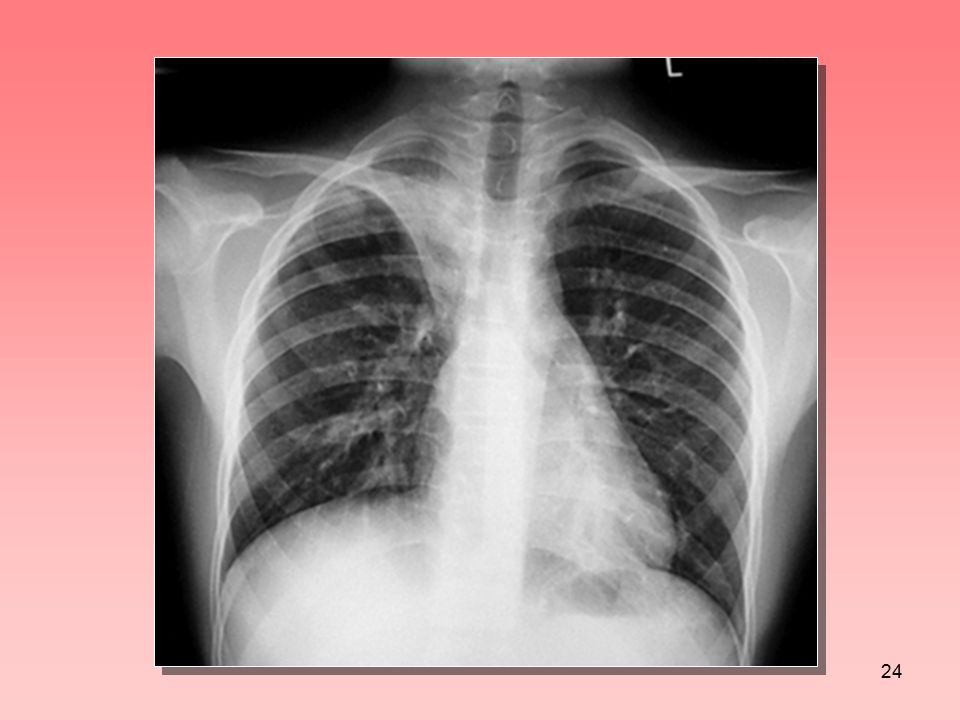
The ‘Pair of Scissors Sign’
If you could cut along a line seen on a CXR with a pair of scissors - think of a pleural boundary or fissure.

23
Interlobar Effusion

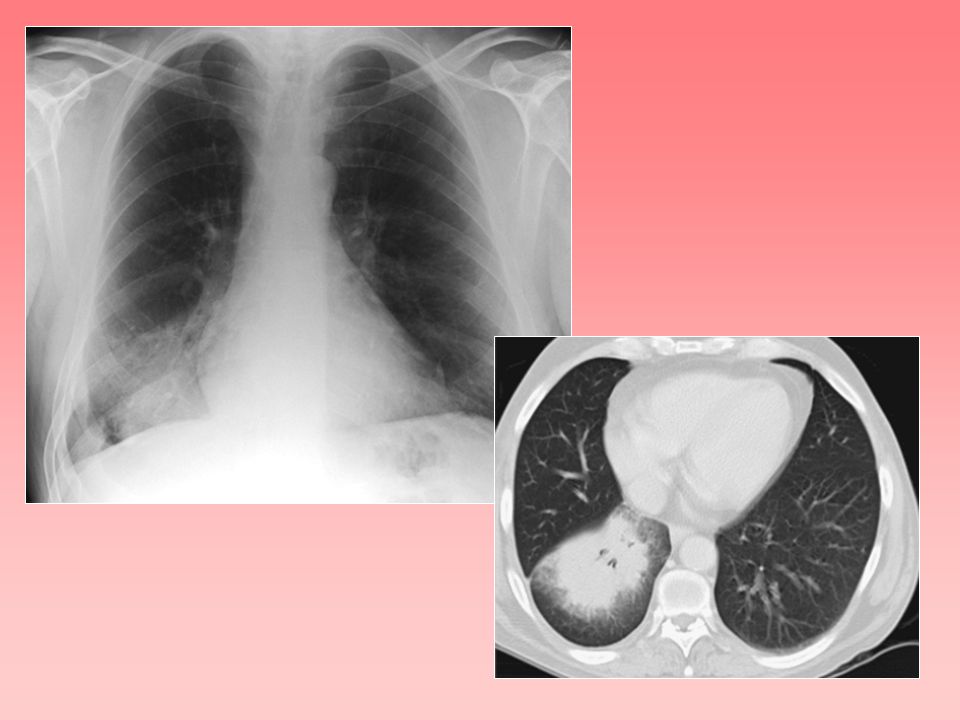
25
Right Upper Lobe Collapse
Horizontal fissure is pulled up, producing a sharply-defined RUZ opacity. Trachea is pulled to the right. Right hilum is pulled upwards. Right hemidiaphragm may be pulled up.

26
Fissure extends medial to hilum
Vertebrae get whiter Diaphragm indistinct Diaphragm disappears

27
Right Lower Lobe

28
Right Lower Lobe Collapse

29
Horizontal fissure Oblique fissure

32
Horizontal fissure

33
Middle Lobe Collapse

36
Right M & LL Collapse Oblique fissure Horizontal fissure

38
Displaced oblique fissure
Overinflated lower lobe Tongue of collapsed upper lobe Elevated left diaphragm

39
Left Upper Lobe Collapse
Overinflated left lower lobe

40
Collapse Consolidation

41
What is it?

43
“Radiological Homeostasis”
If a structure is displaced on a CXR, then something else will happen to compensate for that displacement. Example: collapse of one lobe overinflation of another P

44
If a Structure is Displaced
Pulled out of place Look for collateral evidence Pushed out of place

45
Left heart border indistinct

46
Left heart border visible
Oblique fissure Left heart border visible Diaphragm indistinct

47
Descending aorta indistinct
Triangular opacity Diaphragm indistinct

48
Collapsed Left Lower Lobe
Descending aorta Diaphragm visible

50
Left Lower Lobe Collapse

51
Collapsed left lower lobe
Collapsed right lower lobe

52
Left main bronchus ends
abruptly

53
Total Lung Collapse

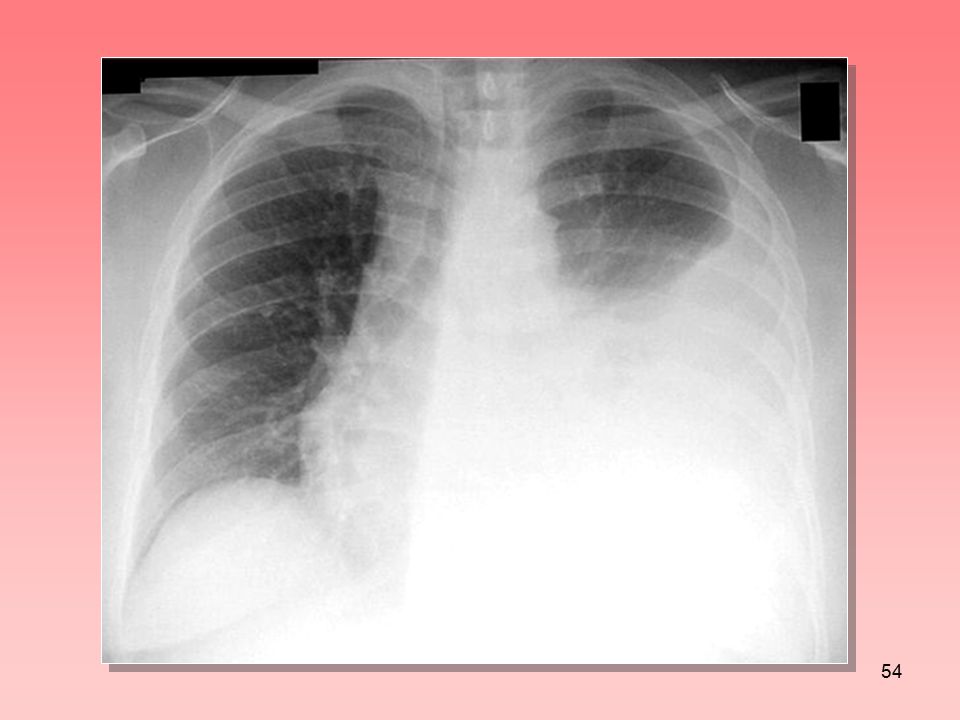
55
Pleural Effusion Davis, Gardner & Qvist 1963, BMJ

56
Basic Principles

57
INTERLUDE

58
Bronchial Tree

59
Bronchial Tree RUL LUL ML Upper division Lingula Basal lower Basal
Apical lower Apical lower

60
Anaesthetist’s Eye View
Lingula Middle lobe Basal lower Basal lower L trachea R Right upper Left upper division Apical lower Apical lower

61
Use Your Imagination!

62
Aspiration and Gravity

63
Apical Segment Apical segment Anterior Posterior Apical segment

64
P Air Bronchogram Two requirements: 1. The bronchus must contain air.
Contrast bronchogram Air bronchogram Two requirements: 1. The bronchus must contain air. 2. The surrounding lung must not. P

65
Resolution Nodules Fibrosis Ground glass

66
Ground Glass Shadowing
Can still see the vessels and airways

67
Consolidation Obscures the vessels and airways Consolidation
Ground glass shadowing

68
Pixels and Voxels Pixel Voxel
![]()
69
Volume Averaging When a pixel contains more than
one type of tissue, it shows the average density of the voxel. 1. One big object, only partially within the voxel 2. Lots of small objects, all within the voxel
![]()
70
Partial Voluming

71
Partial Voluming Aortic arch

72
Partial Voluming (1)
")
73
Partial Voluming

74
Partial Voluming (2) Ground glass shadowing
 Ground glass shadowing")
75
Individual ingredients
Volume-averaged mixture Individual ingredients

76
Ground Glass ‘Micro-fibrosis’
Normal Bronchiectatic

77
Traction Bronchiectasis
Dilated bronchus Fibrosis

78
Pulmonary Fibrosis

79
Plugging and thickening
Tree in Bud Sign Plugging and thickening of bronchioles

80
Basic Principles

81
If only everything was as simple as interpreting chest x-rays…
(Sigh) If only everything was as simple as interpreting chest x-rays…
 If only everything was as simple as interpreting chest x-rays…")
Similar presentations











 –Partial.>")





>")







