Download presentation
Presentation is loading. Please wait.

1
הריונות מרובי עוברים MULTIPLE PREGNANCY
We shall refer to multiple pregnancy or multifetal preg as “twins preg” because it is the most frequent

2
When dealing with multifetal pregnancy you should be prepared for surprises

3
This amazing event atracted scientists for many years until now

4
multiple gestation General concerns:
Multiple gestations are HIGH RISK pregnancies. The major problems are: PRETERM BIRTH LOW BIRTH WEIGHT

5
Frequency MULTIFETAL PREGNANCY Twins: 2% of all deliveries-
12% of NND. Monozygotic 1/250 (1/3 of twins) Tiplets: 1/802 Quadriplet: 1/803
 Tiplets: 1/802. Quadriplet: 1/803.")
6
Epidemiology: In 1970’s multiple gestations 1% of births
In 1990’s multiple gestations > 2% due to: 75% - Assisted Reproductive Technologies (ART) 25% - older age childbearing
 25% - older age childbearing.")
7
Epidemiology: Up to 10% of natural conceptions begin as twins
Multiple gestation Epidemiology: Up to 10% of natural conceptions begin as twins By early 1st trim. transvaginal sonography. vanishing sac 5+5 wk (LMP) Bateman,1990; Boklage,1990
 Bateman,1990; Boklage,1990.")
8
Epidemiology: Multiple gestation "Natural" (1970’s) ART ( 1990's)
Twins :80 births : 55 to x 2 Triplets :6400 (1:802) : to x 6 Quadruplets 1:512,000 (1:803) x 10-20 balanced by fetal reduction 5+5 wk (LMP)
 1: 3323 to 1341 x 6. Quadruplets 1:512,000 (1:803) x balanced by fetal reduction. 5+5 wk (LMP)")
9
Definitions: Monozygotic Twins (Identical) Multiple gestation
Dizygotic Twins (Fraternal): 66% U.S. twins fertilization of 2 ova by 2 sperm Monozygotic Twins (Identical) 33% U.S twins division of 1 ovum fertilized by same sperm unlike sex: 33% of twin pairs
: 66% U.S. twins. fertilization of 2 ova by 2 sperm. Monozygotic Twins (Identical) 33% U.S twins. division of 1 ovum fertilized. by same sperm. unlike sex: 33% of twin pairs.")
10
Etiology MULTIFETAL PREGNANCY Causes of twining
(race, heredity, age, parity, fertility agents, IVF) Genesis of monozygotic twins Monoamniotic twins When searching for etiological factors only fraternal twins should be considered
 Genesis of monozygotic twins. Monoamniotic twins. When searching for etiological factors only fraternal twins should be considered.")
11
Risk factors for dizygotic twins:
Multiple gestation Risk factors for dizygotic twins: Age: older mothers Race: 1:20 in nigeria 1:80 whites 1:150 japanese Parity: higher Family history

12
Risk factors for dizygotic twins:
Multiple gestation Risk factors for dizygotic twins: ART results: 35% of twins 77% of higher order multiples Clomiphene citrate: 10-15% Gonadotropins: 20-40% IVF ~ number of embryos

13
Monozygotic twinning:
Multiple gestation Monozygotic twinning: random event ~ 1:250 pregnancies. not influenced by age, race increased with ovulation induction (?) sex ratio in pairs: female>male
 sex ratio in pairs: female>male.")
14
Definitions: Superfecundation - twins fertilized by different fathers
Multiple gestation Definitions: Superfecundation - twins fertilized by different fathers Superfetation - 2nd ovum fertilized at different month (in animals) Heterotopic Multiple Gestation - intrauterine pregnancy coexisting with extauterine one (IVF)
 Heterotopic Multiple Gestation - intrauterine. pregnancy coexisting with extauterine one (IVF)")
15
Definitions: Dichorionic: separate chorions
Multiple gestation Definitions: Dichorionic: separate chorions Diamniotic: separate amnions Monochorionic: common chorion Monoamniotic: common amnion Dizygotic Twins: always Di-Di Monozygotic Twins: Di-Di; Di-Mo; Mo-Mo

16
Chorionicity & amnionicity impact:
Multiple gestation Chorionicity & amnionicity impact: MZ Twins Frequency Mortality Di-Di % % Mo-Di % % Mo-Mo % %

17
Embryology of membranes
Multiple gestation Blastocyst implantation: day 6-7 (embryonic age) amniotic cavity exocoelomic cavity (primary yolk sac)
 amniotic. cavity. exocoelomic cavity. (primary yolk sac)")
18
Embryology of membranes
Multiple gestation Chorionic cavity: day 14 (embryonic age) secondary yolk sac chorionic cavity (exraembryonic coelom)
 secondary yolk sac. chorionic cavity. (exraembryonic coelom)")
19
Embryology of membranes
Multiple gestation Folding & amniotic cavity: day (embryonic age) cephalocaudal folding lateral folding
 cephalocaudal. folding. lateral folding.")
20
Embryology of membranes
Multiple gestation Embryology of membranes chorion chorionic cavity embryo Where is the amniotic membrane in this ultrasound image? yolk sac decidua capsularis amnion - ? 6+2 wk (LMP)
")
21
Embryology of membranes
Multiple gestation 6 wk (LMP) amnion 7 wk (LMP) 9 wk (LMP) 8 mm 21 mm
 amnion. 7 wk (LMP) 9 wk (LMP) 8 mm. 21 mm.")
22
Zigosity Multifetal pregnancy DC/DA MC/DA MC/MA Con- -joined 3%
Conception chorion amnion embryonic disc DC/DA MC/DA MC/MA Con- -joined Fraternal ~1/3 identical ~2/3 identical 3% 1/50000 Chorionicity depends on the timetable of events after conception Multifetal pregnancy

23
Monozygotic twinning:
Multiple gestation Monozygotic twinning: division <3 days: Di-Di division 4-8 days: Mo-Di division 9-13 days: Mo-Mo division >13 days: Conjoined twins

24
Monozygotic twinning:
implantation Monozygotic twinning: Multiple gestation Dichorionic – always diamniotic Monoamniotic – always monochorionic

27
The dividing membrane is thin but doubled (diamniotic)
")
28
What is the corionicity in the lt sac? DA!

29
Unlike sexes : DC – male chasing his co-twin

30
Two males practicing monosexual relationship

31
Diagnosis MULTIFETAL PREGNANCY History Physical examination X rays
Ultrasound Biochemical test

32
Diagnosis: Multiple gestation
Historically up to 2/3 not diagnosed until labor: poor dates late/poor prenatal care absence of ultrasound screening

33
Diagnosis: Clinical Hints: Multiple gestation
family history, late childbearing, black race ART: clomiphene citrate, gonadotropins, IVF Large for dates uterus: fundal height >3 cm Elevated MSAFP > 2 MOM More than one audible FHR (late finding)
")
34
Definitive diagnosis:
Multiple gestation Definitive diagnosis: Ultrasound Multiple gestations outcome is improved with screening all pregnancies at weeks.

36
Differential Diagnosis:
Multiple gestation Differential Diagnosis: Misdated pregnancy Polyhydramnios Uterine myomas Ovarian cyst Hydatiform mole What are the situations in the DD?

37
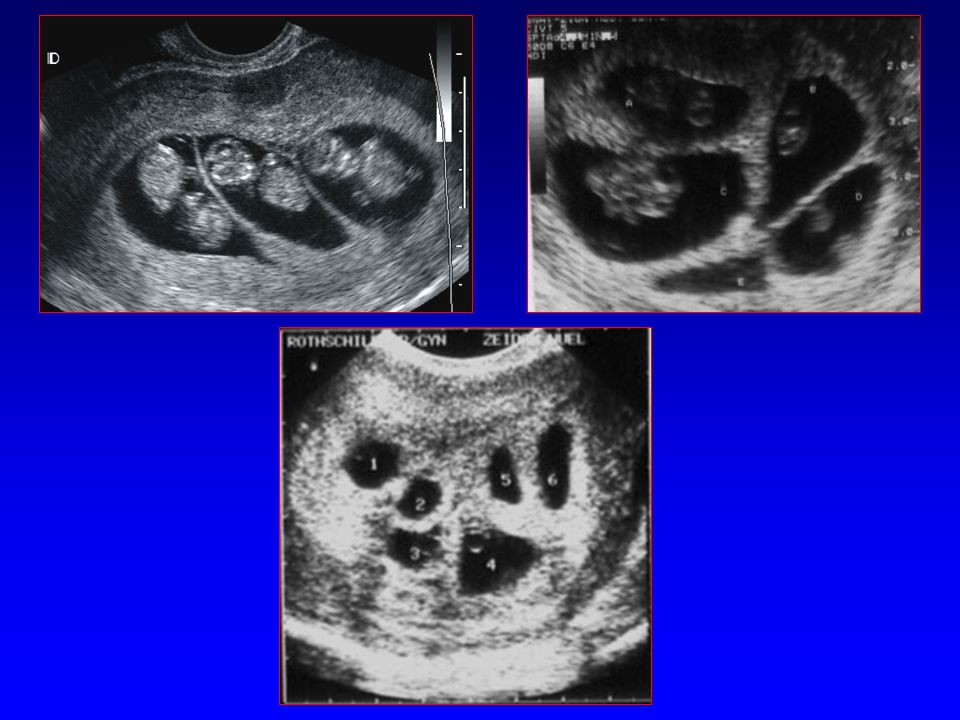
Di-Di Mo-Di Mo-Mo Determination of chorionicity & amnionicity:
Multiple gestation Determination of chorionicity & amnionicity: Early determination: 8-10 weeks is optimal Di-Di Mo-Di Mo-Mo

39
Determination of chorionicity & amnionicity:
Dichorionic-Diamniotic: late determination Unlike sex fetuses "Lambda" or “Y” sign Thick membrane (> 2mm) 3-4 layers Two separate placentas Multiple gestation Placentas may fuse (40%), but no vascular anastamosis occurs
 3-4 layers. Two separate placentas. Multiple gestation. Placentas may fuse (40%), but. no vascular anastamosis occurs.")
40
Interplacental vascular anastamosis > 20%
Multiple gestation Determination of chorionicity & amnionicity: Monochorionic-Diamniotic: late determination Same sex fetuses "T" sign Thin membrane: 2 layers Fused placenta Interplacental vascular anastamosis > 20%

41
Interplacental vascular anastamosis - almost always
Multiple gestation Determination of chorionicity & amnionicity: Monochorionic-Monoamnionic: late determination Same sex fetuses No membrane seen between fetuses Adequate fluid with free movement of both fetuses Single placenta Interplacental vascular anastamosis - almost always

42
Maternal adaptation: Multiple gestation
Weight gain ~ 15 kg (twin gestation) Plasma volume Cardiac output Systemic vascular resistance Venous engorgement
 Plasma volume. Cardiac output. Systemic vascular resistance. Venous engorgement.")
43
Maternal adaptation: Multiple gestation Tidal volume Residual volume
Ventilation Decreased GIT motility Renal plasma flow Uterine volume: 10 liters at term (x2 as singleton)
")
44
General management: Multiple gestation Nutrition
2700 kcal/day – twins 2400 kcal/day – singleton 2100 kcal/day – non pregnant Elementary Iron mg/day Folate 1 mg/day protein gr/day Reduce activity and increase rest (after 20 weeks)
")
46
Fetal reduction-needle in chest

48
General management : Clinic visits every 2 wks after 24 wks:
Multiple gestation General management : Clinic visits every 2 wks after 24 wks: Preterm labor Education Fetal movement counts daily after 32 weeks

49
Obstetric ultrasound: every 2-4 weeks
Multiple gestation Obstetric ultrasound: every 2-4 weeks Fetal growth assessment Biophysical profile Presentations Placental site Cervix length Doppler study singletons weight twins triplets Flattening of growth curve after 30 wks in twins (kg)
")
50
Non Stress Test: Multiple gestation Weekly after 34 weeks
More frequent and earlier if indicated Assess fetal well-being

51
Complications Multiple gestation
Unfortunately we are not living in a perfect world… and the rate of complication for twins is quite high

52
Complications: Multiple gestation Fetal: Abortion / vanishing twin
Inevitable abortion X 2 as in singleton 50 % of early 1st trim. twin sacs are finally deliver as twins 80 % of early 1st trim. alive twins are finally deliver as twins Congenital Anomalies: usual & unique

53
Complications: Fetal: Multiple gestation
Hydramnios / Oligohydramnios: TTTS Discordant growth Intrauterine growth retardation: IUGR ~ 70% of multiple gestations More than 50% of twins < 2500 gr at birth Intrauterine fetal death of one or more fetuses

54
Complications: Multiple gestation Maternal: Hyperemesis gravidarum
Anemia (40%) GDM Pregnancy induced hypertension: twins % triplets - 60%
 GDM. Pregnancy induced hypertension: twins - 40% triplets - 60%")
55
Complications: Maternal-fetal: Multiple gestation
Premature uterine contractions / labor twins: 10% of all preterm deliveries twins: 25% of prenatal deaths worse < 32 weeks and birth weight < 1500gr Premature rupture of membranes Antepartum hemorrhage: abruptio placenta placenta previa

56
Intrapartum hemorrhage
Multiple gestation Labor: Intrapartum hemorrhage abruptio placenta placenta previa uterine rupture Postpartum hemorrhage atonia uteri placental residia DIC birth canal trauma

57
Labor: Multiple gestation Malpresentation
Cord accident: prolapse, entanglement Prematurity associated morbidity and mortality Birth trauma (interlocking, breech extraction) Instrumental delivery Cesarean delivery
 Instrumental delivery. Cesarean delivery.")
58
Premature delivery: Average length of gestation to delivery :
Multiple gestation Premature delivery: Average length of gestation to delivery : No. fetuses weeks(LMP) ~33 ~29
 ~33. 4 ~29.")
59
Premature delivery: Twins: X 12 as singletons
Multiple gestation Premature delivery: Twins: X 12 as singletons > 50% of twins deliver < 37 weeks 91% of triplets deliver < 37 weeks

60
Premature delivery: Multiple gestation
Liberal policy of tocolysis may be justified The decision to administer tocolytics is influenced by: gestational age fetal well-being subtle cervical changes history of prior preterm delivery Prophylactic tocolysis in multiple gestations is not indicated

61
Premature delivery: Multiple gestation
Contraindications for tocolytic use: unexplained vaginal bleeding fetal distress chorioamnionitis advanced cervical dilation.

62
Premature delivery: Multiple gestation
Special considerations for tocolysis in multiple gestations: High intravascular volume and cardiac output. Careful fluid balance using beta-mimetics: increased risk for pulmonary edema Fetal status may preclude use: indomethacin with oligohydramnios

63
Vascular anastomoses between fetuses
Effects of anastomotic circulation Twin to twin transfusion Acardiac twin Multifetal pregnancy

64
A-V, A-A, V-V shunting between placental vessels
Multiple gestation Twin-to-twin transfusion syndrome (TTTS): A-V, A-A, V-V shunting between placental vessels of the monochorionic twins 10-20% of monochorionic: (Mo-Mo > Mo-Di) 80%-100% perinatal mortality if not treated (lethal in early, acute form)
: A-V, A-A, V-V shunting between placental vessels. of the monochorionic twins % of monochorionic: (Mo-Mo > Mo-Di) 80%-100% perinatal mortality if not treated. (lethal in early, acute form)")
65
Twin-to-twin transfusion syndrome (TTTS):
Multiple gestation Twin-to-twin transfusion syndrome (TTTS): Ultrasound: oligo/polyhydramnios - the first finding stuck twin: severe oligohydramnios fetus stucked close to the uterine wall discordancy: >20-25% weight difference >20mm abdominal circuference difference
: Ultrasound: oligo/polyhydramnios - the first finding. stuck twin: severe oligohydramnios. fetus stucked close to the uterine wall. discordancy: >20-25% weight difference. >20mm abdominal circuference difference.")
66
Twin-to-twin transfusion syndrome (TTTS): Donor twin:
Multiple gestation Twin-to-twin transfusion syndrome (TTTS): Donor twin: small & anemic poor renal perfusion small urinary bladder oligohydramnios
: Donor twin: small & anemic. poor renal perfusion. small urinary bladder. oligohydramnios.")
67
Twin-to-twin transfusion syndrome (TTTS):
Multiple gestation Twin-to-twin transfusion syndrome (TTTS): Recipient twin: large & polycythemic (>5 gm% Hb difference) large urinary bladder hypertrophic heart polyhydramnios CHF, hydrops & death from circulatory overload polyhydramnious can cause early labor
: Recipient twin: large & polycythemic (>5 gm% Hb difference) large urinary bladder. hypertrophic heart. polyhydramnios. CHF, hydrops & death from circulatory overload. polyhydramnious can cause early labor.")
68
Twin-twin transfusion syndrome
Prenatal Donor : anemia, oligohydramnios, IUGR, Recipient :polycytemia, polyhydramnios, macrosomia Postnatal Donor : swollen placenta, pale Recipient : red, congested, hypertrophy of placenta, injection studies:anastomoses. Multifetal pregnancy

69
Twin-to-twin transfusion: mechanism
Donor Recipient Chronic blood loss Chronic blood gain Hypovolemia Anemia Hypoxia IUGR Decreased renal flow Oligohydramnios Hypervolemia Polyhydramnios Polycytemia Embolization Hypertension Cardiac failure Placental shunt

70
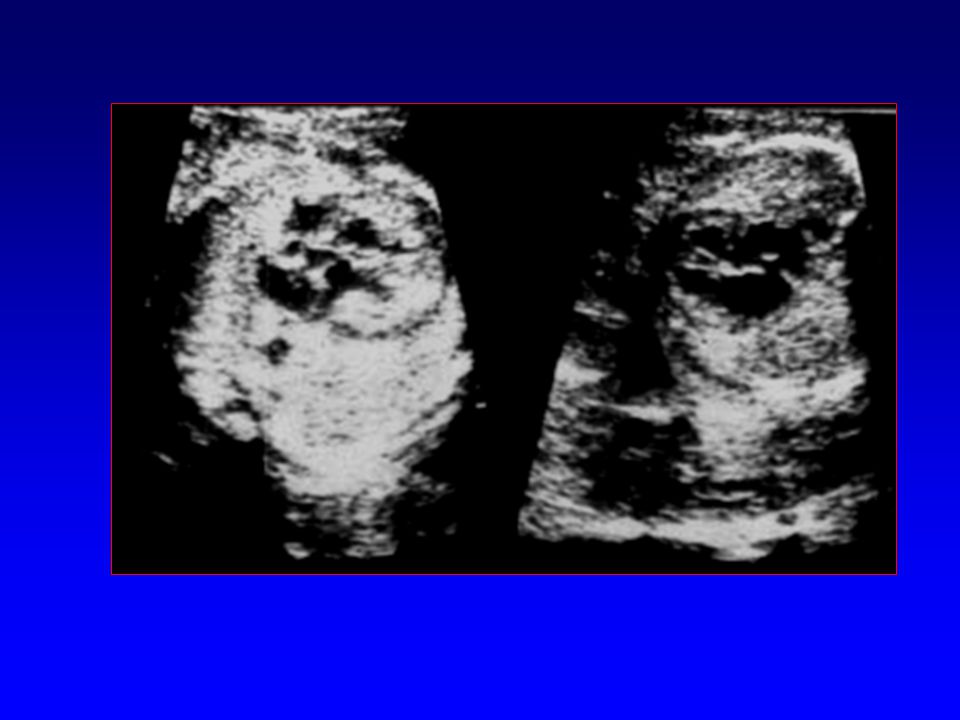
Twin transfusion with stuck twin
Donor twin with progressive oligohydramnios Stuck twin Recipient twin with progressive polyhydramnios

71
Twin transfusion with stuck twin
Donor twin with progressive oligohydramnios Stuck twin Recipient twin with progressive polyhydramnios

72
Twin transfusion with stuck twin
Donor twin with progressive oligohydramnios Stuck twin Recipient twin with progressive polyhydramnios

73
Twin transfusion with stuck twin
Donor twin with progressive oligohydramnios Stuck twin Recipient twin with progressive polyhydramnios

74
Twin transfusion with stuck twin
Donor twin with progressive oligohydramnios Stuck twin Recipient twin with progressive polyhydramnios

75
Twin transfusion with stuck twin
Donor twin with progressive oligohydramnios Stuck twin Recipient twin with progressive polyhydramnios

76
The “stuck twin”

77
The folding of the membrane
Early stages of the stuck twin phenomenon: folding of the membrane

80
Twin-to-twin transfusion syndrome (TTTS):
Multiple gestation Twin-to-twin transfusion syndrome (TTTS): Treatment: Bed rest improves intrauterine blood flow Laser coagulation of shunting vessels Aggressive serial amniocentesis Septostomy (?) If treated - survival up to the 80% To attain > 28 weeks seems to be critical
: Treatment: Bed rest improves intrauterine blood flow. Laser coagulation of shunting vessels. Aggressive serial amniocentesis. Septostomy ( ) If treated - survival up to the 80% To attain > 28 weeks seems to be critical.")
81
Discordant growth and IUGR:
Multiple gestation Discordant growth and IUGR: Discordance: 100% x ( weights / larger twin weight) Discordance of 20-25%: single IUGR fetus > 50% Discordance > 25%: X 6 risk of IUFD (compared to discordance < 25%)
 Discordance of 20-25%: single IUGR fetus > 50% Discordance > 25%: X 6 risk of IUFD (compared to discordance < 25%)")
82
Discordant growth and IUGR:
Multiple gestation Discordant growth and IUGR: At > 30% discordancy in weight: fetal death (the smaller): % congenital anomalies: % low Apgars < 7 at 5 min.: % periventricular leukomalacia: 17%
: 25% congenital anomalies: 38% low Apgars < 7 at 5 min.: 33% periventricular leukomalacia: 17%")
83
Discordant growth and IUGR:
Multiple gestation Discordant growth and IUGR: Ultrasound diagnostic criteria: >20mm abdominal circumferences difference >25% fetal weight difference

84
Discordant growth and IUGR:
Multiple gestation Discordant growth and IUGR: Management considerations: chorionicity: Di-Di virtually rules out TTTS gestational age: late IUGR suggests extrinsic causes weight percentiles: Both twins with normal percentiles - less concern

85
Discordant growth and IUGR:
Multiple gestation Discordant growth and IUGR: Management considerations: pattern of growth important: < 10th percentile or oligohidramnios or pathologic umbilical artery Doppler – close antepartum testing isolated discordance at <32 weeks and <2000 gr, does not support intervention in the absence of other signs of fetal jeopardy.

86
Single IUFD in 2nd and 3rd trimester:
Multiple gestation Single IUFD in 2nd and 3rd trimester: Unlike the demise in early pregnancy, significant problems may occur depending upon the gestational age and chorionicity Loss during the 2nd half of twin pregnancies: ~ 2-3% X 3 as often in monochorionic as dichorionic Fetus papyraceous - hylanized twin remnant

87
Single IUFD in 2nd and 3rd trimester:
Multiple gestation Single IUFD in 2nd and 3rd trimester: Overall morbidity and mortality approximates 45-50% IUFD of one fetus is associated with preterm delivery in the surviving fetus Associated with prematurity, fetal distress and PET Maternal coagulopathy (DIC)
")
88
Single IUFD in 2nd and 3rd trimester:
Multiple gestation Single IUFD in 2nd and 3rd trimester: Monochorionic IUFD: worst prognosis with placental anastomoses: death of one fetus causes severe hypotension in the surviving twin embolisation(?)/DIC and organ damage in the surviving twin: CNS: porencephaly, hydrocephalus, microcephalus limb reduction renal cortical necrosis intestinal atresia aplasia cutis
/DIC and organ damage in the surviving twin: CNS: porencephaly, hydrocephalus, microcephalus. limb reduction. renal cortical necrosis. intestinal atresia. aplasia cutis.")
89
Single IUFD in 2nd and 3rd trimester:
Multiple gestation Single IUFD in 2nd and 3rd trimester: Management depends upon: chorionicity cause of the demise gestational age Intensive fetal monitoring should be undertaken

90
Single IUFD in 2nd and 3rd trimester:
Multiple gestation Single IUFD in 2nd and 3rd trimester: Because of the potential for chronic damage, it is reasonable to deliver monochorionic gestations with lung maturity after 32 weeks Timing of delivery for dizygotic twins with a single demise should be individualized

91
Presentations: Multiple gestation First twin presents vertex: 74%
Both twins vertex: % First twin presents breech: 20% Both twins breech: % Other (transverse/oblique): 6%
: 6%")
92
Cesarean delivery: Multiple gestation Absolute indications:
monoamniotic twins conjoined twins first twin - not vertex triplets and higher order other Cesarian section indications: non progressive labor fetal distress placenta previa uterine scar: corporeal, >1 past CSLT’s absolute CPD, etc.

93
Cesarean delivery: Multiple gestation Relative indications:
Second twin - not vertex: Mother not willing to undergo breech delivery Fetus <1.5 kg (? 2 kg) one or both twins have non-reassuring fetal status fetal discordancy: the first twin is the smaller member single past low transverse cesarian delivery
 one or both twins have non-reassuring fetal status. fetal discordancy: the first twin is the smaller member. single past low transverse cesarian delivery.")
94
Vaginal delivery: (ACOG, 1998)
Multiple gestation Vaginal delivery: (ACOG, 1998) During labour - continuous cardiotocogram All patients should have a ready IV access Double set-up delivery room First twin - vertex vaginal delivery
 During labour - continuous cardiotocogram. All patients should have a ready IV access. Double set-up delivery room. First twin - vertex vaginal delivery.")
95
Vaginal delivery: (ACOG, 1998)
Multiple gestation Vaginal delivery: (ACOG, 1998) Second twin - vertex presentation: vertex vaginal delivery Second twin - non vertex presentation: internal podalic version and breech extraction external cephalic version: less successful expectant management
 Second twin - vertex presentation: vertex vaginal delivery. Second twin - non vertex presentation: internal podalic version and breech extraction. external cephalic version: less successful. expectant management.")
96
Vaginal delivery: (ACOG, 1998)
Multiple gestation Vaginal delivery: (ACOG, 1998) Second twin considerations: Delay > 20 min. may increase morbidity of the 2nd twin. Delays >15 min. are associated with a 6 fold increase in Cesarean section. Morbidity and mortality are minimized with continuous CTG of twin B and the ability for immediate Cesarean section.
 Second twin considerations: Delay > 20 min. may increase morbidity of the 2nd twin. Delays >15 min. are associated with a 6 fold increase in Cesarean section. Morbidity and mortality are minimized with continuous CTG of twin B and the ability for immediate Cesarean section.")
97
Vaginal delivery: (ACOG, 1998)
Multiple gestation Vaginal delivery: (ACOG, 1998) Second twin considerations: ~15% of vertex/nonvertex require a Caesarean section for the second twin: Failure of second twin delivery Second twin experiences fetal distress prepare for double set-up delivery placentas of multifetal pregnancies should be sent to pathology with each cord clearly labelled.
 Second twin considerations: ~15% of vertex/nonvertex require a Caesarean section for the second twin: Failure of second twin delivery. Second twin experiences fetal distress. prepare for double set-up delivery. placentas of multifetal pregnancies should be sent to pathology with each cord clearly labelled.")
98
Diagnosis of multiple gestation Gestational age assessment
Prenatal diagnosis: Diagnosis of multiple gestation Gestational age assessment Determination of Amnion/Chorion Status Survey for anomalies: NTT, Triple screen, TIFFA Invasive procedures: CVS, Amniocentesis TIFFA: Targeted Imaging For Fetal Anomalies

100
Problems with prenatal diagnosis: Increase in multiple gestations and
aneuploidy with older maternal age Increased background risk for anomalies Correct determination of zygosity Difficulties with interpretation of triple screen

101
Problems with prenatal diagnosis:
Multiple gestation Problems with prenatal diagnosis: Ability to sample all fetuses (CVS, AC) Increased loss of pregnancies before 28 weeks Increased loss rate with CVS and amniocentesis
 Increased loss of pregnancies before 28 weeks. Increased loss rate with CVS and amniocentesis.")
102
Congenital anomalies: Incidence in twins: x2 as in singletons
Multiple gestation Congenital anomalies: Incidence in twins: x2 as in singletons major malformations: 2.3% vs. 1% Monozygotic: x2 as in dizygotic chromosomal anomalies: each twin ~ singleton conjoined twins – higher incidence risk of Down syndrome in twins: 1:370 for women aged 33 (35 in singeltons)
")
103
Congenital anomalies:
Unique to monozygotic twins: conjoined twins acardiac twin (TRAP syndrome) fetus-in-fetu Multiple gestation
 fetus-in-fetu. Multiple gestation.")
104
Congenital anomalies:
Multiple gestation Congenital anomalies: Twinning process associated anomalies: anencephaly holoprosencephaly sirenomelia extrophy of cloaca renal agenesis anal atresia tracheoesophageal fistula situs inversus defects

105
NTD

106
Congenital anomalies:
Multiple gestation Congenital anomalies: Vascular disruption sequences secondary to one twin demise: porencephaly hydranencephaly hydrocephalus multicystic encephalomalacia microcephalus limb reduction renal cortical necrosis intestinal atresia aplasia cutis

107
Congenital anomalies:
Multiple gestation Congenital anomalies: Deformations due to crowding of fetuses: congenital dislocation of hip clubfoot

108
Twin to twin transfusion Mortality - up to 60%
Multiple gestation Monoamniotic twins: Cord entanglement Twin to twin transfusion Mortality - up to 60% Ultrasound surveillance and delivery ~34 weeks

110
cord entanglement

111
1st trim. spontaneous loss of one
Multiple gestation Vanishing twin: 1st trim. spontaneous loss of one or more with higher order multiples fetus 50 % - if only "sacs" are counted 20 % - if alive embryos counted Higher loss rate with advancing maternal age Excellent prognosis for remaining fetus(es)
")
112
Acardiac twin: Multiple gestation One of Mo-Mo twins grows despite of
the absence of cardiac activity / presence of heart. Occurs at 1 : 30,000-40,000 pregnancies or slightly less than 1% of monozygous twins. A normal ("pump") twin supplies perfusion to acardiac twin. "twin reverse arterial perfusion" (TRAP) Oxygenated blood to the acardiac fetus in the artery
 twin supplies perfusion. to acardiac twin. twin reverse arterial perfusion (TRAP) Oxygenated blood to the acardiac fetus in the artery.")
113
acardiac twin

114
Multiple gestation Acardiac twin: Hydramnios is a common finding (40%), with a strong association with PTD and CHF in the pump twin. Better prognosis if acardiac twin weight < 50% of the pump twin

115
Acardiac twin: Treatment: Multiple gestation
Conservative: digoxin and indomethacin Fetal surgery: endoscopic laser prior to 24 weeks and umbilical cord ligation thereafter Invasive techniques may be avoided if acardiac fetal mass very small or flow to acardiac decreasing or absent.

116
Conjoined twins: Multiple gestation Also called "Siamese" twins
Incomplete division of the embryonic disk at day after conception The incidence 1: ,000 births High rate of congenital anomalies

117
Classification by the area of joining:
Multiple gestation Conjoined twins: Classification by the area of joining: chest (thoracopagus) head (craniopagus) abdomen (omphalopagus) coccyx and sacrum (ischiopagus) body with two heads (dicephalus) one head with two bodies (dipygus)
 head (craniopagus) abdomen (omphalopagus) coccyx and sacrum (ischiopagus) body with two heads (dicephalus) one head with two bodies (dipygus)")
118
Conjoined twins Craniopagus Thoracopagus Ischiopagus
Multifetal pregnancy

120
presence of other anomalies
Multiple gestation Conjoined twins: Survival in conjoint twins depends upon: extent of attachment place of attachment presence of other anomalies

121
In this old sonographic image this fetus is going to score using the head of his brother twin

122
In conclusion: twins pregnancy is quite a project but the lovely results justify the efforts..

123
Multiple gestation Prof. S. Degani June 2007

Similar presentations













 MULTIPLE PARITY -Twins (two babies) -Monozygotic(Division of 1 ova fertilized.>")



 MULTIPLE PARITY -Twins (two babies) -Monozygotic(Division of 1 ova fertilized by the same sperm) -Dizygotic(Fertilization.>")










