Download presentation
Presentation is loading. Please wait.

1
OPTIMISING ASSESSMENT OF REHABILITATION NEEDS
Virginia Pascall Consultant Occupational Physician

5
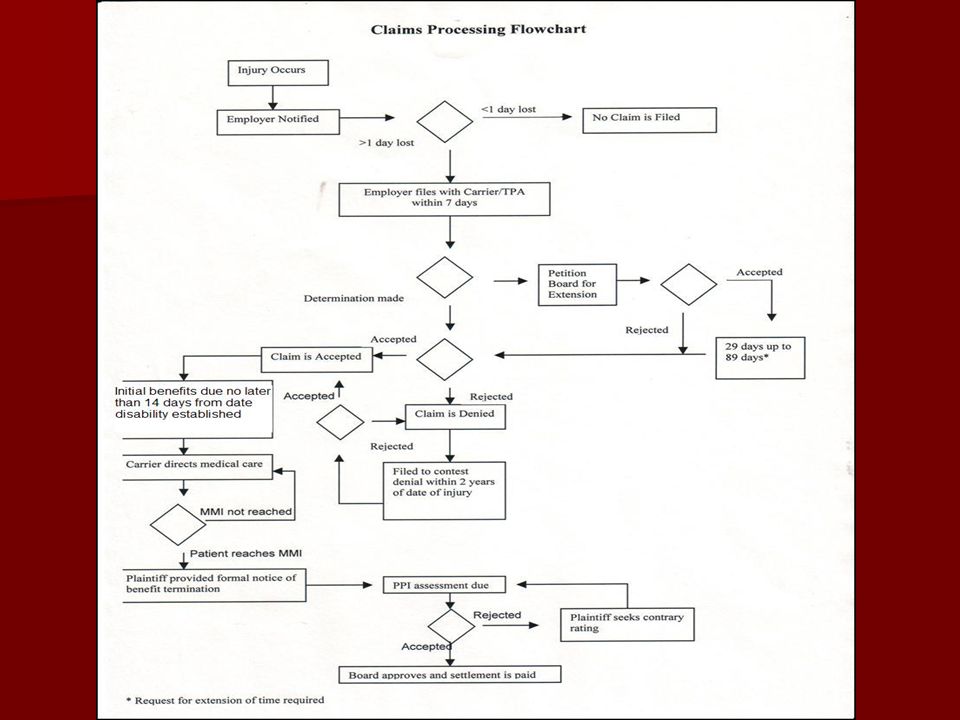
Your rehab. mental flow chart
Can the employee work at all? increase his/her hours at work? increase the range of duties or tasks they are given? resume normal work/hours at work?

6
What are your questions?
What is wrong with the employee (diagnosis)? Different or more treatment? Is it the work that is slowing their recovery? Is it the travel to work? Can I change anything about the work?
 Different or more treatment Is it the work that is slowing their recovery Is it the travel to work Can I change anything about the work")
7
The underlying questions
Anything about this employee’s complaints that are due to their: Underlying constitutional endogenous degenerative or pre-injury condition(s)? Their personality (including other agendas)?
 Their personality (including other agendas)")
8
The Treating Doctor His mental flow chart
My patient is injured I prescribe treatment I write WC certificate YOU do whatever is on certificate

9
The Next Visit I see my patient again I listen to my patient
I give new treatment or same treatment I write new WC certificate YOU do what is on certificate.

10
The ethos of medical practice
Do no harm Make people better If I can’t make them better, I feel I should try harder and at times, I can hand over the management to my patient because they often are happy to receive what they want, even if not recovered.

11
AT SOME STAGE My patient tells me that they are better
I write final certificate OR

12
My patient keeps telling me they are no better
I don’t know what to do, so I do nothing but write another WC certificate and REFER to A SPECIALIST My role has now become much more passive ….

13
TURN IT AROUND The best thing for recovery is for the patient to resume as NORMAL a life as possible – including working life. You do not need to be pain free to achieve that.

14
THE OBJECTIVE IS NOT FREEDOM FROM PAIN
IT IS TO LEAD A NORMAL LIFE PAIN CANNOT BE CENTRE STAGE FOR NORMAL LIFE –

15
PAIN cannot be the determining factor in what a person will or will not do …..
The sooner you can shift the emphasis in the employee’s mind and in the treating doctor’s mind from pain intolerance to capability the sooner you will have your employee working effectively

16
The ‘One’ Message Keep talking about capability Praise achievement
Look for small steps not big goals Show confidence in the employee’s ability to overcome pain avoidance Walk this talk with

17
The employee The supervisor Especially the doctor The rehabilitation provider (who should be doing it anyway but can become bogged down in the emotions of a visit to the doctor situation)
")
18
The Doctor’s Perspective
Always believes his patient Underlying fear that he might miss some crucial medical condition Does not want to disenfranchise his patient Doctors don’t want conflict

19
If you cannot persuade the doctor to increase hours/tasks/reduce restrictions
When might it occur? How could it occur? What needs to be done to make it happen?

20
The treating doctor and BARRIERS
The treating doctor may be the barrier Many do not have up to date knowledge of medical conditions and base their diagnosis, causation and treatment on old fashioned and often failed strategies. The employee may be very faithful/trusting of their treating doctor

21
Suggest a ‘second opinion’ – but watch out for the nexus between an old fashioned GP and an old fashioned specialist You will need to persuade regarding a specialist with the skills you want

22
The treating doctor may be oblivious to the underlying agenda
The patient/employee who is accustomed to the restricted hours and tasks The treating doctor may be oblivious to the underlying agenda BRING IT OUT INTO THE OPEN IN FRONT OF THEIR DOCTOR – CHALLENGE THE EMPLOYEE TO REJECT THIS SUPPOSITION

23
The employee who likes the day off each week to
Sleep in Have their treatment See doctors RECOVER

24
It may be the treating doctor’s belief that their patient is so exhausted with working whilst in pain that they need ‘a day off to recover’. THEY’RE MISSING THE POINT!

25
WE ALL WOULD LIKE A DAY OFF WORK (at full pay or even less than full pay) TO RECOVER FROM WORKING A COUPLE OF DAYS …. WE ARE ALL TIRED AND WE OFTEN ARE ACHING

26
Couple of Steps Reinforce the aim is to return to normal life
Propose the idea that if so tired after two days, that is not good in itself Propose that shorter hours per day should prevent such a level of fatigue/pain

27
Come up with a combination of hours for 5 days a week, but the TOTAL hours is the same as employee has been managing Doctors find the logic hard to reject and will usually give it a try

28
BUT MOST OF ALL, MAKE THEM FEEL CAPABLE
Don’t forget LOTS OF PRAISE MAKE THEM FEEL IMPORTANT BUT MOST OF ALL, MAKE THEM FEEL CAPABLE

29
Questions for the Independent Specialist
Diagnosis Got to know what the working diagnosis is for the specialist, because all the opinions and recommendations must be logical in relation to this .....

30
1. Diagnosis Why is the employee experiencing the symptoms?
Is there more than one condition (incl. the underlying etc etc)? What is the relationship between the condition and the employee’s work? Why are the symptoms recurring/not getting better?
 What is the relationship between the condition and the employee’s work Why are the symptoms recurring/not getting better")
31
2. Ability to work Can the employee do normal work/hours now or in the future – what is the expectation for recovery? What is their current capability if not normal hours/work? Anything about current tasks, equipment that is impeding recovery? Can anything be changed re. tasks, equipment?

32
3. Psychological Issues Is there a discrepancy between what the employee complains about and the medical condition/injury they have? Every medical condition and injury has a known set of symptoms and signs. Anything outside this should raise a flag of one colour or another.

33
Symptom Magnification Pain Behaviours
Ask about Symptom Magnification Pain Behaviours

34
THESE ARE NOT THE SAME AS SAYING THE PERSON IS MALINGERING OR CREATING A FACTITIOUS CONDITION

35
They are usually genuine
They are often fearful/anxious They often believe that pain means damage or injury or generally ‘Don’t do!’ They are often not aware that they are acting or thinking in a negative/abnormal/counter-productive way They often believe they are doing the right thing to recover – and some do not like to be challenged on this.

36
PAIN BEHAVIOUR Apparent that the person is in pain
Verbal and nonverbal – serve to communicate the fact that there is pain If you are getting the message that the person is in pain, most likely they are manifesting pain behaviours

37
Moaning, grimacing, crying, body postures, facial expressions, shifting posture, limping, not using a limb But also, history of medication each time in pain, ceasing activity to pursue a pain-related activity, not accepting medical advice – 2nd opinion, & 3rd, more tests

38
SYMPTOM MAGNIFICATION
Vague, inconsistent history Inappropriate health care utilisation Symptom complex inconsistent with condition Functional limitations inconsistent with condition Disability more than indicated by condition Abnormal pain inventories Reported pain level inconsistent with observations Reported functional limitations inconsistent with observations Pain behaviour demonstrated Non-physiologic findings on examination C Brigham, ACOEM, Advanced Topics, 1996

39
ASK Why Is It Present? What Can Be Done When Will It Stop?
For any outstanding pain behaviour or complaint ASK the DOCTOR - Why Is It Present? What Can Be Done When Will It Stop?

Similar presentations