Download presentation
Presentation is loading. Please wait.

2
speculum Examination

4
-name the position of patient -ues for what
-name of picture -name the position of patient -ues for what -How to do speculum Examination - is it most common 1- Cusco’s or bivalve speculum 2-women in the dorsal position 3-examine the cervix 4-Use a warm and well lubricated speculum. The labia minora must be adequately parted with the left hand. Insert the speculum upwards and backwards (direction of vagina) Advance into vagina fully. Directly visualize as you open the plates to expose the cervix. If cervix not seen: close plates, withdraw slightly, change direction and open again. 5- Cusco’s bivalve is more frequently used
 Advance into vagina fully. Directly visualize as you open the plates to expose the cervix. If cervix not seen: close plates, withdraw slightly, change direction and open again. 5- Cusco’s bivalve is more frequently used.")
6
-name the position of patient -ues for what
-name of picture -name the position of patient -ues for what 1-a sims speculum 2-left lateral position 3-used in pelvic organ prolapse. For examine posterior vaginal wall

8
Name the manuver Use for what 1-Bimanual Vaginal Examination
2- to palpat the the uterus and adenexia

9
Described the picture Adnexae:to assess
Mal ovaries are usually not palpable Any masses systic/solid and described approximate size Tenderness is assessed by direct digital pressure into the fornices and cervical

10
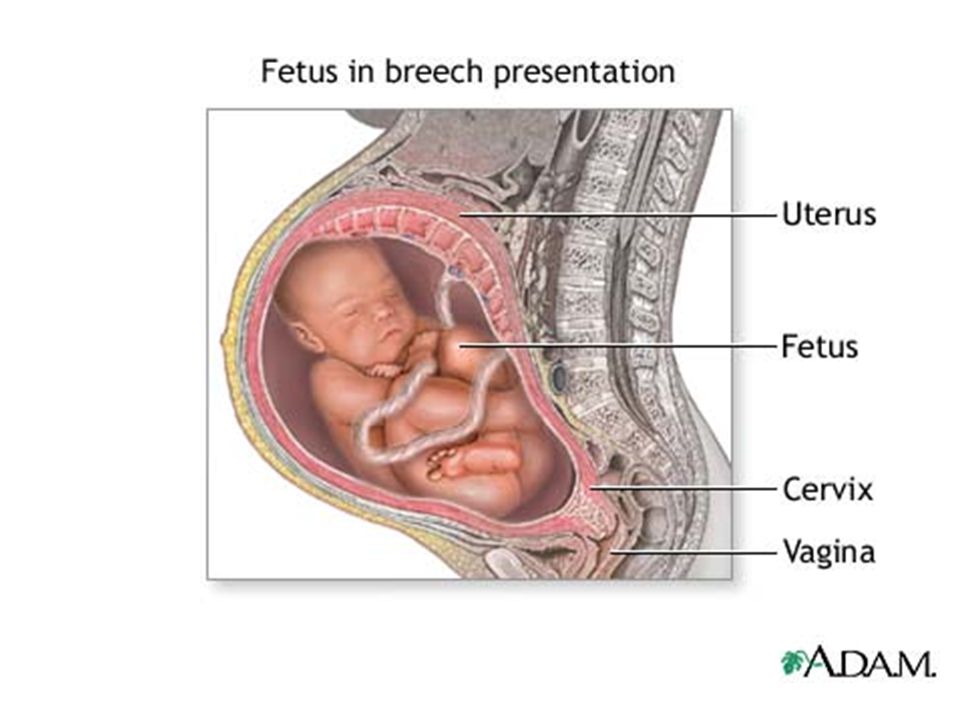
Obstetrical maneuvers. Fundal height
Using reference points. Using a tape

11
Obstetrical grips (Leopold’s maneuvers).
Fundal grip (First maneuver) What fetal part occupies the fundus if soft consistency/ indefinite outline broad & irregular breech If hard, smooth, well defined, rounded, bullottable head
 What fetal part occupies the fundus if soft consistency/ indefinite outline broad & irregular breech. If hard, smooth, well defined, rounded, bullottable head.")
12
Obstetrical grips (Leopold’s maneuvers).
Lateral grips (Second maneuvers). On which side is the fetal back ? Lie. Position. Where to auscultate for FHS.
. On which side is the fetal back Lie. Position. Where to auscultate for FHS.")
13
Obstetrical grips (Leopold’s maneuvers).
First pelvic grip - Pawlik’s grip (Third maneuver). What fetal part lies over the pelvic inlet?. Presentation.
. What fetal part lies over the pelvic inlet . Presentation.")
14
Obstetrical grips (Leopold’s maneuvers).
Second pelvic grip (Fourth maneuver) Engagement Attitude
 Engagement. Attitude.")
15
A and B. Children with Down syndrome, which is characterized by a flat,
broad face, oblique palpebral fissures, epicanthus, and furrowed lower lip. C. Another characteristic of Down syndrome is a broad hand with single transverse or simian crease.

16
Structural chromosome abnormalities
Patient with Prader-Willi syndrome resulting from a microdeletion on paternalchromosome 15. If the defect is inherited on the maternal chromosome, Angelmansyndrome occurs

17
Barr body (arrows) in the epidermal spinous cell layer
Nuclear appendage ("drumstick") identified by arrow in white blood cells
 identified by arrow in white blood cells.")
18
Hypothalamic-pituitary- gonadal axis
CNS +/- hypothalamus +/- neurons gonadotropin releasing hormone +/- + _ ant. pituitary +/- LH FSH (LH R) thecal cells androgens inhibin granulosa cells LH R هذي الصوره متكرره مرتين بالمحاضره يمكن يحط فراغات باماكن الهرمونات واحنا نعبيها أو يتنيذل ويقول اشرحي عمل الهرمونات The Hypothalamus Secretes GnRH, Which Causes the Anterior Pituitary Gland to Secrete LH and FSH: the pulsatile nature of GnRH release (lasting 5 to 25 minutes that occur every 1 to 2 hours) is essential to its function Estrogen in small amounts has a strong effect to inhibit the production of both LH and FSH. Also, when progesterone is available, the inhibitory effect of estrogen is multiplied, even though progesterone by itself has little effect. These feedback effects seem to operate mainly on the anterior pituitary gland directly, but they also operate to a lesser extent on the hypothalamus to decrease secretion of GnRH Hormone inhibin from the corpus luteum inhibits FSH and LH Secretion Hormone activin from the stimulates FSH Secretion FSH R progestins activin estrogens + Reproductive tract
 thecal cells. androgens. inhibin. granulosa cells. LH R. هذي الصوره متكرره مرتين بالمحاضره يمكن يحط فراغات باماكن الهرمونات واحنا نعبيها أو يتنيذل ويقول اشرحي عمل الهرمونات. The Hypothalamus Secretes GnRH, Which Causes the Anterior Pituitary Gland to Secrete LH and FSH: the pulsatile nature of GnRH release (lasting 5 to 25 minutes that occur every 1 to 2 hours) is essential to its function. Estrogen in small amounts has a strong effect to inhibit the production of both LH and FSH. Also, when progesterone is available, the inhibitory effect of estrogen is multiplied, even though progesterone by itself has little effect. These feedback effects seem to operate mainly on the anterior pituitary gland directly, but they also operate to a lesser extent on the hypothalamus to decrease secretion of GnRH. Hormone inhibin from the corpus luteum inhibits FSH and LH Secretion. Hormone activin from the stimulates FSH Secretion. FSH R. progestins. activin. estrogens. + Reproductive tract.")
19
when secretion throughout the sexual life of the female?
The increasing levels of estrogen secretion at puberty, the cyclical variation during the monthly sexual cycle, the further increase in estrogen secretion during the first few years of reproductive life, the progressive decrease in estrogen secretion toward the end of reproductive life, and, finally, almost no estrogen or progesterone secretion beyond menopause.

20
What are the

21
Growth in puberty Girls: 1-When start growth acceleration ?
2-When peak growth velocity occurs ?) 3-When menarche occurs? 1-Growth acceleration begins at the onset of puberty 2-Peak growth velocity occurs earlier (6-9 months after thelarche) 3-Menarche occurs after peak growth velocity
 3-When menarche occurs 1-Growth acceleration begins at the onset of puberty. 2-Peak growth velocity occurs earlier (6-9 months after thelarche) 3-Menarche occurs after peak growth velocity.")
22
Growth in puberty Boys: When Peak growth velocity occurs? Boys:
Peak growth velocity occurs relatively late in puberty

23
Define of this endometrial cycle? How much day each cycle take ?
proliferative phase: proliferation of the uterine endometrium; secretory phase: development of secretory changes in the endometrium; and desquamation of the endometrium, which is known as menstruation.. Define of this endometrial cycle? How much day each cycle take ?

24
Skin changes 1) identefy ? What is the cause ? -
1)Skin changes in pregnancy Pigmentation: chloasma gravidarum: Butterfly pigmentation of the face (mask of pregnancy) due to increased melanocyte stimulating hormone 2) Striae gravidarum : - stretch of the abdominal wall rupture of the subcutaneous elastic fibers pink lines in flanks - become white after labor
Skin changes in pregnancy Pigmentation: chloasma gravidarum: Butterfly pigmentation of the face (mask of pregnancy) due to increased melanocyte stimulating hormone. 2) Striae gravidarum : - stretch of the abdominal wall rupture of the subcutaneous elastic fibers. pink lines in flanks. - become white after labor.")
25
ماادري وش ممكن يكون عليه سؤال بس حطيته للذمة عشان يشمل كل الصور

26
للذمة

27
الصور الجاية السؤال عليهن
In what step of mechanism of labor ? What is the position ? الجواب بالملاحظات

28
Descent step - occiputo transverse position

29
Flextion step - occiputo transverse position

30
Internal rotation occipito- anterior position.

31
Delivery by Extension: As the fetal head reaches the maternal symphysis pubis it hitches under the bone. The pressure by the uterine contractions causes the neck of the baby to get extended

32
External Rotation: The shoulders rotate into an oblique or frankly anterio-posterior orientation with further descent. This encourages the fetal head to return to its transverse position. This is also known as Restitution .

33
External Rotation:نفس اللي قبل
The shoulders rotate into an oblique or frankly anterio-posterior orientation with further descent. This encourages the fetal head to return to its transverse position. This is also known as Restitution

34
Transverse – vertex – breech lie

35
What is the name of this technique? And what we use it for ?
Leopold’s Maneuvers It uses to palpate the fetus part , to estimate it position ,lie engagement

36
للذمة

37
What is the name ? What is it`s component ?
Partogram - It include : fetal heart rate Uterine contraction pulse, blood pressure, temp fluid intake, oxyotcin dilation of the cervix station of the presenting part, status of membranes, meconium, blood

38
للذمة

39
للذمة

41
WHICH BONES COMPOSE THE BONY PELVIS?
Iliopectineal line Left sacro-iliac joint Sacrospinous ligament Sacrotuberous ligament Symphysis pubis Sacral promontory 48 L4 Ischial spine Ischial tuberosity THE BONY PELVIS WHICH BONES COMPOSE THE BONY PELVIS? I ) 2 Innominate bones : a) Illium b) Ischium c) Pubis II) Sacrum III) Coccyx
 2 Innominate bones : a) Illium. b) Ischium. c) Pubis. II) Sacrum. III) Coccyx.")
42
False pelvis The false pelvis is bounded posteriorly by the lumbar vertebra and laterally by the iliac fossa. In front, the boundary is formed by the lower portion of the anterior abdominal wall.

43
43

44
After you activate your book, you will get
Pelvic inlet and its diameters. Printed from: Hacker & Moore's Essentials of Obstetrics and Gynecology 5e (on 05 January 2013) © 2013 Elsevier After you activate your book, you will get اتوقع يسأل عن اسماء conjugate and its length in cm WHAT IS THE OBSTETRIC CONJUGATE? The shortest APD between sacral promontory & symphysis pubis Can only be measured radiologically N ≥ 10 cm WHAT IS THE TRUE CONJUGATE? APD between promontory of the sacrum & superior margin of the symphysis pubis 11cm or diagonal conjugate – 1.5cm WHAT IS THE DIAGONAL CONJUGATE? Distance between sacral promontory & inferior margin of the symphysis pubis cm? Measured clinically
 © 2013 Elsevier. After you activate your book, you will get. اتوقع يسأل عن اسماء conjugate and its length in cm. WHAT IS THE OBSTETRIC CONJUGATE The shortest APD between sacral promontory & symphysis pubis. Can only be measured radiologically. N ≥ 10 cm. WHAT IS THE TRUE CONJUGATE APD between promontory of the sacrum & superior margin of the symphysis pubis 11cm. or diagonal conjugate – 1.5cm. WHAT IS THE DIAGONAL CONJUGATE Distance between sacral promontory & inferior margin of the symphysis pubis 12.5cm Measured clinically.")
45
After you activate your book, you will get
The four basic pelvic types. The dotted line indicates the transverse diameter of the inlet. Note that the widest diameter of the inlet is posteriorly situated in an android or anthropoid pelvis. The gynecoid pelvis illustrates the location of the sacrosciatic notch, present in all pelvic types. Printed from: Hacker & Moore's Essentials of Obstetrics and Gynecology 5e (on 05 January 2013) © 2013 Elsevier After you activate your book, you will get
 © 2013 Elsevier. After you activate your book, you will get.")
46
PELVIC SHAPE 1-GYNECOID Typical female pelvis found in 50% of women
Rounded—slightly oval inlet Straight pelvic sidewalls with roomy pelvic cavity Good sacral curve Ischial spines are not prominent Pubic arch is wide 46

47
PELVIC SHAPE 2-ANDROID Typical male pelvis found in 1/3 white women 1/6 non-white Pelvic brim is heart shaped Pelvis funnels from above downwards (convergent sidewalls) Narrow pubic arch Prominent spines 47
 Narrow pubic arch. Prominent spines. 47.")
48
PELVIC SHAPE 3-ANTHROPOID 25% white women & 50% nonwhite
Pelvic brim APD > TD Long & narrow pelvic canal with long sacrum Straight pelvic sidewalls 48

49
PELVIC SHAPE 4-PLATYPELLOID 3% of women
Pelvic brim TD >>>APD kidney shape Sacral promontory pushed forwards 49

50
FETAL SKULL SUTURES Frontal suture between 2 frontal bones
Sagittal suture between 2 parietal bones Coronal suture between parietal & frontal Lambdoid suture between parietal & occipital Temporal suture between inferior margin of the parietal & temporal

51
FETAL SKULL FONTANELLES
Anterior fontanelle : diamond shaped space between coronal & sagittal suture, ossifies at month Post font (lambda) : triangle shaped space between sagittal & lambdoid suture
 : triangle shaped space. between sagittal & lambdoid suture.")
52
Diameteres of the fetal skull
Biparietal diameter = 9.5cm Suboccto-bregmatic diameter = 9.5cm Occipito-frontal diameter = 11.5cm (occipito-posterior position) The suboccipito-frontal diameter= 10 cm (1st diameter passes through vulval orifice)
 The suboccipito-frontal diameter= 10 cm. (1st diameter passes through vulval orifice)")
53
Diameteres of the fetal skull
Mento-vertical diameter =13cm (Brow presentation) Submento-bregmatic diameter = 9.5cm (face presentation) Bis-acromial diameter =12cm (diameter of the shoulder) Bitrochanteric diameter =10cm (Diameter of the breech)
 Submento-bregmatic diameter = 9.5cm. (face presentation) Bis-acromial diameter =12cm. (diameter of the shoulder) Bitrochanteric diameter =10cm. (Diameter of the breech)")
64
Placenta Previa Bleeding results from small disruptions in the placental attachment during normal development and thinning of the lower uterine segment

66
Placental Abruption external hemorrhage concealed hemorrhage Total
Partial

67
Sequelae of Placental Abruption
Maternal Shock Consumptive Coagulopathy (DIC) Renal Failure Fetal Death Couvelaire Uterus
 Renal Failure. Fetal Death. Couvelaire Uterus.")
68
Vasa Previa Velamentous insertion of the umbilical cord

69
Vasa Previa Succenturiate (Accessory) lobe
 lobe")
70
Nitrazine Test

71
Positive Fern by Microscopic Exam

72
HL Shoulder Dystocia A review of the risks, physiology, management, and prevention of Shoulder Dystocia Next Slide

73
PATHOPHYSIOLOGY The anterior shoulder can then slide under the symphysis pubis for delivery. If the fetal shoulders remain in an anterior-posterior position during descent or descend simultaneously rather than sequentially into the pelvic inlet, then the anterior shoulder can become impacted behind the symphysis pubis and/or the posterior shoulder may be obstructed by the sacral promontory. Then you get the dreaded “Turtle Sign” of doom. Next Slide

74
Turtle Sign More about this in a bit Next Slide

75
Risk Factors for Shoulder Dystocia
Maternal Abnormal pelvic anatomy Gestational diabetes Post-dates pregnancy Previous shoulder dystocia Short stature Fetal Suspected macrosomia Male sex Labor related Assisted vaginal delivery (forceps or vacuum) Protracted active phase of first-stage labor Protracted second-stage labor Put mouse over chart to review pt’s information. Next Slide
 Protracted active phase of first-stage labor. Protracted second-stage labor. Put mouse over chart to review pt’s information. Next Slide.")
76
Vignette Since she is post-term and nothing good happens after 41 weeks…you decide to induce Jaquita. Labor has been fine, she has progressed like she should, and is now complete and ready to push. You gown up and are ready to catch this baby. The head begins to come out and…Oh crap…..Turtle Sign. Click HERE for a purely representative and graphical demonstration.

77
Turtle Sign Demonstration
Oh crap, Turtle Sign! Replay Demonstration Next Slide

78
HELPERR Mnemonic The HELPERR mnemonic is a clinical tool that offers a structured framework for coping with shoulder dystocia. These maneuvers are designed to do one of three things: Increase the functional size of the bony pelvis through flattening of the lumbar lordosis and cephalad rotation of the symphysis (i.e., the McRoberts maneuver) Decrease the bisacromial diameter, the breadth of the shoulders, of the fetus through application of suprapubic pressure. Change the relationship of the bisacromial diameter within the bony pelvis through internal rotation maneuvers. Next Slide
 Decrease the bisacromial diameter, the breadth of the shoulders, of the fetus through application of suprapubic pressure. Change the relationship of the bisacromial diameter within the bony pelvis through internal rotation maneuvers. Next Slide.")
79
HELPERR Mnemonic H Call for Help:
This refers to activating the pre-arranged protocol or requesting the appropriate personnel to respond with necessary equipment to the labor and delivery unit. Click HERE for Diagram. Next Slide

80
HELPERR Mnemonic H Call for Help:
This refers to activating the pre-arranged protocol or requesting the appropriate personnel to respond with necessary equipment to the labor and delivery unit. Click HERE for Diagram. Click Diagram to Dismiss it

81
HELPERR Mnemonic E Evaluate for episiotomy:
Episiotomy should be considered throughout the management of shoulder dystocia but is necessary only to make more room if rotation maneuvers are required. Shoulder dystocia is a bony impaction, so episiotomy alone will not release the shoulder. Because most cases of shoulder dystocia can be relieved with the McRoberts maneuver and suprapubic pressure, many women can be spared a surgical incision. Next Slide

82
HELPERR Mnemonic L Legs (the McRoberts maneuver):
This procedure involves flexing and abducting the maternal hips, positioning the maternal thighs up onto the maternal abdomen. This position flattens the sacral promontory and results in cephalad rotation of the pubic symphysis. Nurses and family members present at the delivery can provide assistance for this maneuver. Click HERE for McRobert’s Diagram. Next Slide

83
McRobert’s Maneuver Click Diagram to Dismiss it

84
HELPERR Mnemonic P Pressure (Suprapubic):
The hand of an assistant should be placed suprapubically over the fetal anterior shoulder, applying pressure in a cardiopulmonary resuscitation style with a downward and lateral motion on the posterior aspect of the fetal shoulder. This maneuver should be attempted while continuing downward traction. Click HERE for Diagram. Next Slide

85
Suprapubic Pressure Click Diagram to Dismiss it

86
HELPERR Mnemonic E Enter maneuvers (internal rotation):
These maneuvers attempt to manipulate the fetus to rotate the anterior shoulder into an oblique plane and under the maternal symphysis. Next Slide

87
"Enter" Maneuvers 1. 2. 3. 1. Rubin II At vaginal examination apply pressure as indicated. If shoulders move into the oblique diameter, attempt delivery. 2. Rubin II + Woods corkscrew maneuver If unsuccessful, add the Woods corkscrew maneuver and continue rotation in the same direction. Use both hands and apply pressure as indicated. If shoulders now move into the oblique, attempt delivery. If this is unsuccessful, continue rotation 180 degrees and deliver. 3. Reverse Woods corkscrew maneuver If the last maneuver is unsuccessful, change to reverse Woods corkscrew maneuver. Slide fingers down to back of posterior shoulder and attempt 180-degree rotation in the opposite direction. Next Slide

88
HELPERR Mnemonic R Remove the posterior arm:
Removing the posterior arm from the birth canal also shortens the bisacromial diameter, allowing the fetus to drop into the sacral hollow, freeing the impaction. The elbow then should be flexed and the forearm delivered in a sweeping motion over the fetal anterior chest wall. Grasping and pulling directly on the fetal arm may fracture the humerus. Click HERE for Diagram. Next Slide

89
Removing Posterior Arm
R Remove the posterior arm: Removing the posterior arm from the birth canal also shortens the bisacromial diameter, allowing the fetus to drop into the sacral hollow, freeing the impaction. The elbow then should be flexed and the forearm delivered in a sweeping motion over the fetal anterior chest wall. Grasping and pulling directly on the fetal arm may fracture the humerus. Click HERE for Diagram. Click Diagram to Dismiss it

90
HELPERR Mnemonic R Roll the patient:
The patient rolls from her existing position to the all-fours position. Often, the shoulder will dislodge during the act of turning, so that this movement alone may be sufficient to dislodge the impaction. In addition, once the position change is completed, gravitational forces may aid in the disimpaction of the fetal shoulders. Click HERE for Diagram. Next Slide

91
HELPERR Mnemonic R Roll the patient:
The patient rolls from her existing position to the all-fours position. Often, the shoulder will dislodge during the act of turning, so that this movement alone may be sufficient to dislodge the impaction. In addition, once the position change is completed, gravitational forces may aid in the disimpaction of the fetal shoulders. Click Diagram to Dismiss it

92
Complications of Shoulder Dystocia
Maternal Postpartum hemorrhage Rectovaginal fistula Symphyseal separation or diathesis, with or without transient femoral neuropathy Third- or fourth-degree episiotomy or tear Uterine rupture Fetal Brachial plexus palsy Clavicle fracture Fetal death Fetal hypoxia, with or without permanent neurologic damage Fracture of the humerus Next Slide

93
Prevention Evidence is lacking to support labor induction or elective cesarean delivery in women without diabetes who are at term when a fetus is suspected of having macrosomia. In two studies of 313 women without diabetes, induction for suspected fetal macrosomia did not lower the rates of shoulder dystocia or cesarean delivery, nor did it improve the rates of maternal or neonatal morbidity. While labor induction in women with gestational diabetes who require insulin may reduce the risk of macrosomia and shoulder dystocia, the risk of maternal or neonatal injury is not modified. Not enough evidence is available to routinely support elective delivery in this population. Next Slide

94
Prevention So, prophylactic cesarean delivery is not recommended as a means of preventing morbidity in pregnancies in which fetal macrosomia is suspected. Analytic decision models have estimated that 2,345 cesarean deliveries, at a cost of nearly $5 million annually, would be needed to prevent one permanent brachial plexus injury in a patient without diabetes who had a fetus suspected of weighing more than 4,000 g. Next Slide

95
Prevention One method of preliminary intervention for shoulder dystocia in a patient with risk factors involves implementing the "head and shoulder maneuver" to "deliver through" until the anterior shoulder is visible. This step is accomplished by continuing the momentum of the fetal head delivery until the shoulder is visible. After controlled delivery of the head, the physician proceeds with immediate delivery of the anterior shoulder without stopping to suction the oropharynx. Next Slide

Similar presentations