Download presentation
Presentation is loading. Please wait.

2
Managing poor responders in IVF
Bye : DR Seyed Mehdi Ahmadi GYN & Gynecologist

4
Definition of ovarian poor responder:
The definition of poor responders has varied throughout the medical literature . Three or fewer oocytes or follicles . Estradiol (E2) level below 500 pg/ml. Fewer than five oocytes retrieved in high gonadotropin dose cycles (at least 450 inter national IU of FSH with a peak E2 below 1000 pg/ml . Most literature on poor responders has utilized at least 450 IU of FSH, yet several studies in the 1990s confirmed no added benefit to gonadotropin dosing above 450 IU of hMG or FSH.
 level below 500 pg/ml. Fewer than five oocytes retrieved in high gonadotropin dose cycles (at least 450 inter national IU of FSH with a peak E2 below 1000 pg/ml . Most literature on poor responders has utilized at least 450 IU of FSH, yet several studies in the 1990s confirmed no added benefit to gonadotropin dosing above 450 IU of hMG or FSH.")
5
POR definition(ESHRE)
At least two of the following three features must be present: Advanced maternal age (≥ 40 years) or any other risk factor for POR. A previous POR (≤3 oocytes with a conventional stimulation protocol) An abnormal ovarian reserve test (i.e. AFC = 5–7 follicles or AMH=0.5–1.1 ng/ml) ) POR definition(ESHRE)
 or any other risk factor for POR. A previous POR (≤3 oocytes with a conventional stimulation protocol) An abnormal ovarian reserve test (i.e. AFC = 5–7 follicles or. AMH=0.5–1.1 ng/ml) ) POR definition(ESHRE)")
6
Poor responders – how to diagnose
D2 FSH AFC AMH FOLLICLES E2 HMG OOCYTES

7
Diagnosis: Basal (day 3) FSH level
day 10 FSH level of the clomiphene citrate (CC) challenge test. Serum basal FSH Estradiol levels anti-Müllerian hormone Sonographic assessment of ovarian reserve including (ovarian volume & antral follicle count) Color Doppler of ovarian However, the most accurate predictor of a poor response cycle is a history of poor response to gonadotropins.
 challenge test. Serum basal FSH. Estradiol levels. anti-Müllerian hormone. Sonographic assessment of ovarian reserve including (ovarian volume & antral follicle count) Color Doppler of ovarian. However, the most accurate predictor of a poor response cycle is a history of poor response to gonadotropins.")
8
Poor responders – BOLOGNA criteria from ESHRE
ADVANCED AGE>40/OTHER RISK FACTORS FOR POR ABNORMAL ORT PREVIOUS POR

9
Poor responders – how to sight them?
AMH Costly test Not widely available Cycle independent Better predictive value Current role - controversial AFC Simple test Good inter- & intra- observer reproducibility Before starting stimulation Better correlation with retrieval number Current role – widely practised AMH Costly test Not widely available Cycle independent Better predictive value Current role - controversial FSH Most commonly used Easily available D2 or D3 higher values –predictive False positive rate 5% SCREENING TEST! hormones Dynamic tests ultrasound ultrasound

10
Poor responders – how to manage them?
Mini dose protocol Conventional Agonists protocol - Dampening of ovarian response to gonadotropin stimulation Modify Stimulation Protocol Adjuvant therapy “Stop” protocol Short/ Ultra-short/Flare protocol Micro dose flare protocol

11
Poor responders – how to manage them?
Antagonist protocol -decreases stimulation duration -fewer cancellations -lesser Gonadotropins Modify Stimulation Protocol

12
Poor responders – how to manage them?
Growth Hormone Estradiol Adjuvant therapy Androgens COC pill Soft Protocols r- LH L-arginine, steroids, aspirin

13
Poor responders – how to manage them?
Potentiates effect of FSH Previous poor responders have proven benefit Costly Not widely available No consensus on dose / route Growth Hormone Case – Control design 128 – 81 2U s/c Growth Hormone More M-II oocytes, higher E2 levels, pregnancy rates

14
Poor responders – how to manage them?
Essential prohormone in follicular steroidogenesis Improves the ovarian micromilieu Micronised DHES – 25mg TID X 4months Improves pregnancy rates and reduces miscarriage rates Androgens DHES

15
Poor responders – how to manage them?
LH plays a role in follicular development From D8, IU Beneficial in a subset of a. age >35, b. previous POR c. Antagonist cycles Improves pregnancy rates r- LH

16
Treatment (Is There an Ideal Protocol?)
There is no really efficient treatment that could solve the problem of poor ovarian response and the current question is still which is the ideal protocol for patients defined as “poor responders”?

17
Gonadotropins : It is confirmed that the increase of FSH starting dose , does not result in higher pregnancy rates . It is found no differences between the starting dose of 300UI, 450UI, and 600 UI of gonadotropins in terms of retrieved oocytes, number of embryos obtained and pregnancy rates. Maximal dosing, currently set at 450 IU of FSH, should be started as early in the cycle as possible. The dose may then be reduced once adequate response has been established.

18
HMG versus recombinant FSH
Recombinant FSH (rFSH) was introduced in the mid-1990s, and was initially touted to improve stimulation and pregnancy rates when compared with the already available equivalent dose of hMG. More recent trials have suggested that hMG may have advantages for poor responders undergoing IVF, although the data are limited . Mixed protocols of rFSH and hMG have become popular to provide both a high FSH dose as well as some LH activity.
 was introduced in the mid-1990s, and was initially touted to improve stimulation and pregnancy rates when compared with the already available equivalent dose of hMG. More recent trials have suggested that hMG may have advantages for poor responders undergoing IVF, although the data are limited . Mixed protocols of rFSH and hMG have become popular to provide both a high FSH dose as well as some LH activity.")
19
The role of LH in stimulation protocols for poor responders
LH stimulation is available as both a recombinant LH (rLH) and in the standard urinary hMG, which contains a 1:1 ratio of FSH and LH activity. Additional LH activity during stimulation for IVF can be obtained with low doses of urinary or recombinant hCG. LH activity has been postulated to be beneficial during early follicular recruitment by increasing FSH receptors, as well as maintaining follicular development during later follicular maturation by maintaining steroid precursors.
 and in the standard urinary hMG, which contains a 1:1 ratio of FSH and LH activity. Additional LH activity during stimulation for IVF can be obtained with low doses of urinary or recombinant hCG. LH activity has been postulated to be beneficial during early follicular recruitment by increasing FSH receptors, as well as maintaining follicular development during later follicular maturation by maintaining steroid precursors.")
20
Articles have looked at the role of LH, both recombinant as well as mixed protocols with hMG .
One reviewer has suggested that hMG, due to its LH activity, slightly increases the pregnancy rates in IVF when compared with rFSH alone. Most reviews and meta- analyses of the role of LH, however, have been unable to confirm any benefit or detriment of LH to IVF pregnancy or LBRs.

21
The role of adding LH to rFSH stimulation in IVF is even less well studied in poor responders.
With the introduction of GnRH antagonists for poor responders, it has become clear that antagonists blunt the rise in E2 during rFSH- stimulated cycles. This decreased rise in E2 can be overcome with either hMG or rLH.however, no advantage in IVF outcome has been established. some authors have found a benefit to LH addition in stimulation protocols in older patients.

22
GnRH Analogues : in poor ovarian reserve the options could be :
To decrease the length of suppression by decreasing the duration of GnRH agonist use (short and ultrashort, mini- and microdose flareup regimens) .
 .")
23
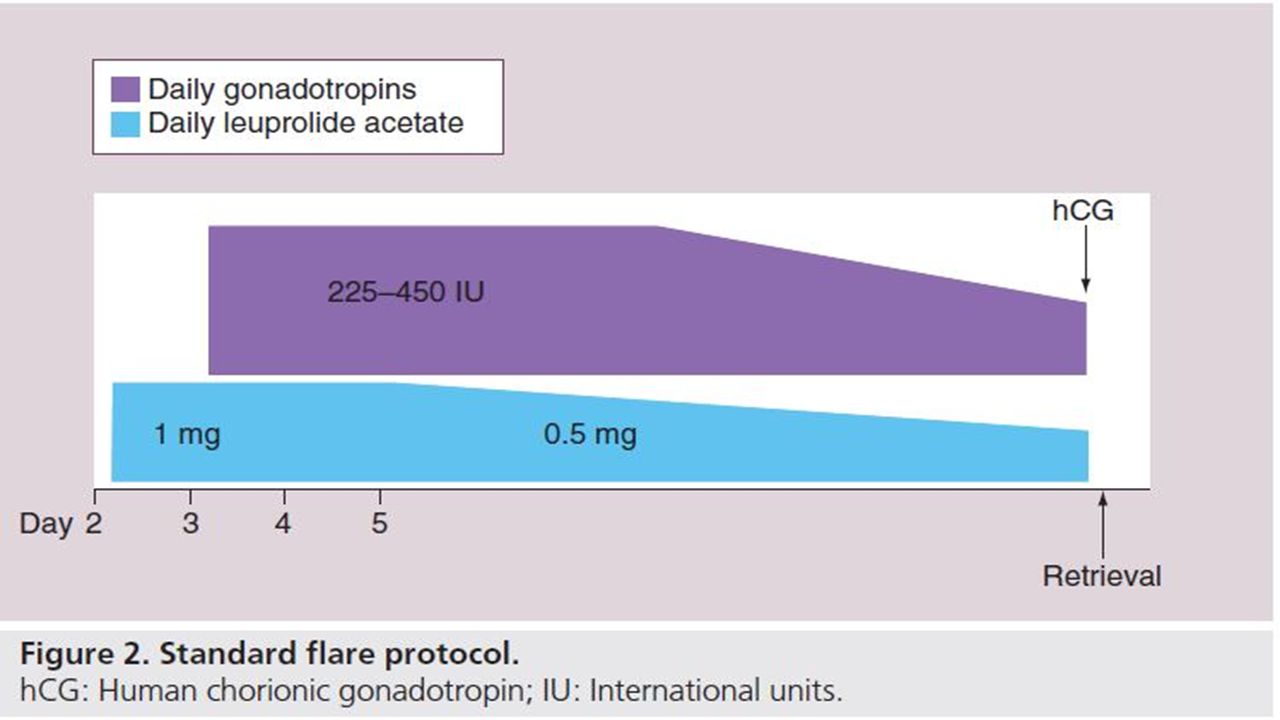
1.GnRH agonist microdose flare protocols :
It has been shown that a single dose of 25–50 µg of GnRH agonist given on cycle day 2 can increase both FSH and LH levels. The protocols utilizing minimal doses of GnRH agonists such as 20–50 µg twice daily (b.i.d.) for 2 days at the beginning of the cycle (microdose flare protocols) are usually combined with OCP pretreatment in the cycle prior to COH to prevent corpus luteum rescue .
 for 2 days at the beginning of the cycle (microdose flare protocols) are usually combined with OCP pretreatment in the cycle prior to COH to prevent corpus luteum rescue .")
24
In retrospective studies:
the use of microdose protocols in poor responders has shown improved cycle outcome with regards to the number of retrieved oocytes, percentage of patients undergoing embryo transfer, cancellation rates and pregnancy rates, when compared with traditional long GnRH agonist protocols.

25
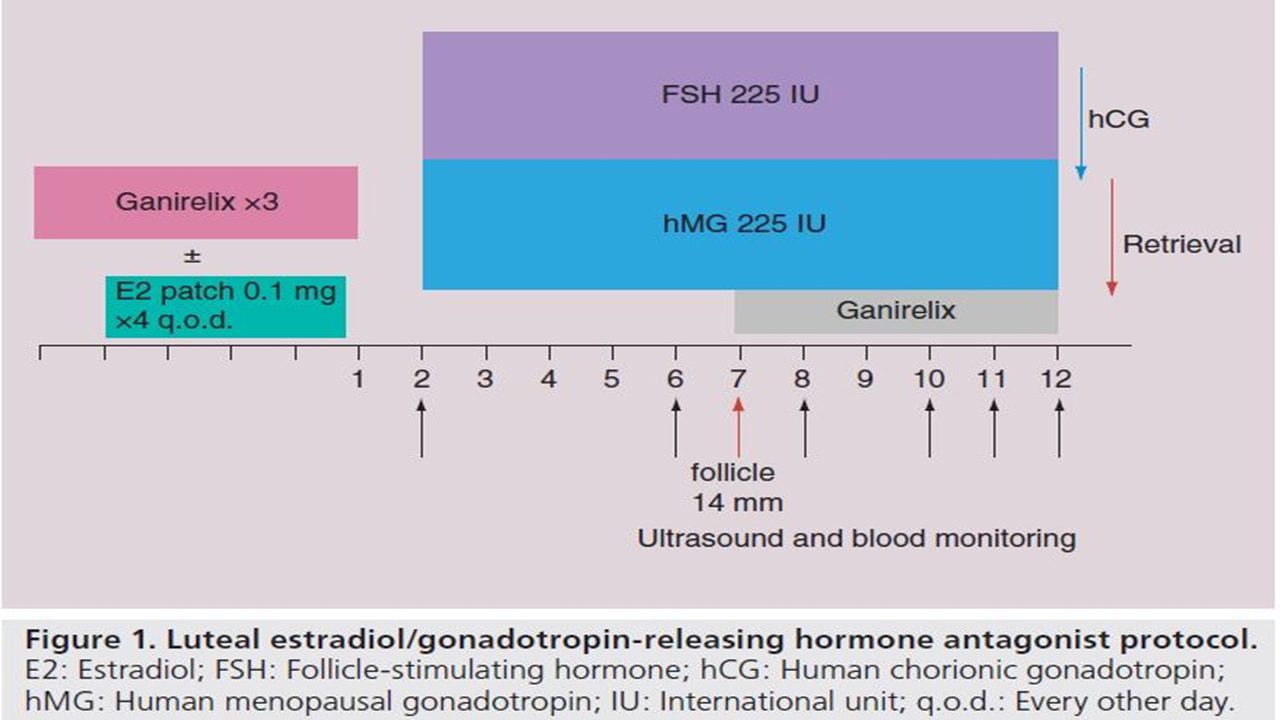
2.GNRH antagonist: Advantages of the use of GnRH antagonist + gonadotropins are : Improvement of patient’s compliance. Decreased number of days of stimulation and of the amount of gonadotropin administered. Reduction of ovarian hyperstimulation syndrome (OHSS). GnRH antagonists are not administered during the stage of follicular recruitment and thus suppression of endogenous gonadotropins secretion is not present at that time . Most protocols commence GnRH antagonists when the mean diameter of the lead follicle reaches 14 mm and continue daily until human chorionic gonadotropin (hCG) administration.
. GnRH antagonists are not administered during the stage of follicular recruitment and thus suppression of endogenous gonadotropins secretion is not present at that time . Most protocols commence GnRH antagonists when the mean diameter of the lead follicle reaches 14 mm and continue daily until human chorionic gonadotropin (hCG) administration.")
26
suitable protocol for poor responders:
GnRH antagonists + gonadotropins Reason : GNRH antagonists in the mid-late follicular phase during ovarian stimulation prevent the premature LH surge while not causing suppression in the early follicular phase, obtaining more natural follicular recruitment without any inhibitory effect possibly induced by the GnRH agonist.

27
As a general : Employ flare protocols when using OCPs and
Antagonist protocols when not pretreating with OCPs.

29
Clomiphene flare protocols
A flare of endogenous gonadotropins can be also achieved with early CC administration. In these cycles, endogenous LH surge can be blocked with GnRH antagonists . CC flare was shown to: Reduce cancellation rates Increase the number of oocytes retrieved Result in a higher implantation rate Higher pregnancy rates in poor responders.

30
Concerns about The use of a CC flare : Endometrial suppression
CC is commonly and successfully used both in minimal stimulation protocols and for its flare effect in high-dose protocols in poor responders who are undergoing freeze-all cycles. Its potential for negative endometrial effects during a fresh transfer cycle necessitates further study.

31
Letrozole flare protocols
Letrozole is a highly selective aromatase inhibitor that has been used in assisted reproductive technology. Mechanism: Blocking estrogen synthesis and decreasing its circulating levels →effect on the pituitary →increasing release of endogenous gonadotropins.

32
In COH protocols : letrozole doses of 2.5–5.0 mg daily on day 3–7 of stimulation cycle + menotropins + GnRH antagonist. Addition of letrozole in poor response cycles can decrease the total dose of FSH used when compared with a long GnRH agonist protocol + having an advantage in antagonist cycles in poor responders.

33
Dosing intervals for poor responders
It has become common to offer b.i.d. dosing of hMG or FSH in poor responders. When using mixed protocols of hMG from vials and rFSH from a pen, the authors often recommend twice-daily injections . Despite no documented benefit from b.i.d. dosing, it continues to be popular, especially for mixed protocols in poor responders.

34
Minimal stimulation Many studies have suggested that for poor responders, natural cycle IVF or IVF with minimal stimulation produces similar pregnancy rates as with full-dose gonadotropins . A significant problem with natural cycle IVF is the high cancelation rate; however, use of GnRH antagonists in the late follicular phase has shown promising results .

35
In two studies including poor responders, similar pregnancy rates were found following minimal stimulation IVF when compared with full-dose gonadotropins with IVF, despite a lower number of oocytes retrieved and embryos transferred. To decrease the rate of cycle cancelation and premature LH surge, one study included supplementation with : GnRH antagonists and hMG Administered 0.25 mg of GnRH antagonists and 75 IU rFSH daily until ovulation induction.

36
Natural, clomiphene or letrozole only IVF
One randomized trial showed that poor responders treated with natural cycles + ICSI had higher implantation rates but similar clinical pregnancy rates per cycle and per transfer as patients treated with full-dose gonadotropins . CC stimulation alone was far more successful than natural-cycle IVF. Letrozole has also been looked at as an adjuvant in minimal stimulation cycles employing a low dose of gonadotropins.

37
Laboratory options in poor response cycles ICSI for low oocyte yield
Poor responders typically produce fewer than five oocytes per retrieval. In couples with poor ovarian response and fertilization failure, ICSI could have a potential advantage over IVF.( Higher fertilization rate ). If either the oocytes appear immature, or the mature-appearing oocyte is immature after stripping, employing standard IVF for the remaining oocytes. An oocyte is considered immature when it is surrounded by corona radiata with a less dense cumulus oophorus.
. If either the oocytes appear immature, or the mature-appearing oocyte is immature after stripping, employing standard IVF for the remaining oocytes. An oocyte is considered immature when it is surrounded by corona radiata with a less dense cumulus oophorus.")
38
Preimplantation genetic screening for poor responders ( PGD )
Couples are at an increased risk of developing chromosomally abnormal embryos after unexplained repeated IVF failures or advanced maternal age . Therefore, preimplantation genetic screening (PGS) utilizing FISH has been studied for patients with : advanced maternal age repeated miscarriage repeated implantation failure severe male factor infertility
 utilizing FISH has been studied for patients with : advanced maternal age. repeated miscarriage. repeated implantation failure. severe male factor infertility.")
39
Clinical trials utilizing FISH technology decreased the LBRs in women of advanced reproductive age and poor responders, either due to damage to the embryos or inaccuracy of the testing. Newer methods such as comparative genomic hybridization (CGH) have been introduced with the ability to analyze the entire genome.
 have been introduced with the ability to analyze the entire genome.")
40
Ideal day of transfer In poor responders where fewer oocytes and embryos are available for transfers, transferring embryos at an earlier cleavage stage appears to be beneficial. As a general rule, once the number of viable embryos is equal to the number planned to be transferred, further delay of transfer is likely to be more harmful than beneficial. The clinical pregnancy rates per oocyte retrieval and per embryo transfer were significantly higher in the day 2 embryo transfer group compared with day 3.

41
Number of embryos for transfer
Indication for increasing the number of embryos to transfer: advanced reproductive age poor ovarian reserve poor response ASRM guidline: in women aged less than 35 years→→→ up to two embryos in women aged less than 38 years→→→ up to three embryos in women aged less than 41 years→→→ up to four embryos Even in poor responders.

42
Donor oocytes Recommend oocyte donation IVF only for:
poor responders with multiple failed IVF cycles those with a very poor prognosis prior to IVF. Very poor prognosis group includes : all patients over 43 years of age any patient with an FSH over 15 mIU/ml an undetectable AMH.

43
Number of newer procedures in ART that have a role in the management of poor responders:
In vitro maturation (IVM) Cryopreservation of oocytes Embryos from multiple retrieval cycles Cryopreservation of donor oocytes (egg banking )
 Cryopreservation of oocytes. Embryos from multiple retrieval cycles. Cryopreservation of donor oocytes (egg banking )")
44
IVM IVM of human oocytes is a new procedure.
Oocytes are retrieved at 8–12-mm size after either priming with a few days of FSH injections followed by hCG, or during a natural cycle followed by a hCG injection. The immature retrieved oocytes are then matured in vitro in special media.

45
While IVM has been proposed for patients with :
Polycystic ovary syndrome at high risk of OHSS Cancer patients who may not undergo standard stimulation A few case reports have described success using IVM in poor responders. There are limited data on the use of IVM for poor responders, it may aid in cases that otherwise would have been cancelled. The accumulation of oocytes from several ovarian stimulation cycles or freeze all cycles , creates a similar situation as in normal responders.

46
Oocyte banking: The use of cryo-banked oocytes in an ovum donation program may be a realistic option in the future, significantly increasing the efficiency of the donor process. The process of synchronizing the recipient with the donor has some drawbacks, including waiting lists and coordinating recipient schedule to the timing of the donor.

47
Alternative Approaches

48
1.DHEA TO IMPROVE OVARIAN FUNCTION
Increase antral follicles Increase no of mieotically active oocytes Decrease follicular atresia Increase ovarian steroidogenesis DHEA

49
2.Pre conditions the ovary for ovulation induction
DHEA supplementation for production of estrogen in the ovaries Improves follicular dynamics- enhances aromatase activity required for improved E2 levels Better ovarian function in women with increased resistance to OI – increase no of oocytes and embryos favoring clinical pregnancies

50
ACTION OF DHEAS IMPROVES REDUCES OVARIAN APOPTOSIS RESERVE DHEA
PROHORMONE IMPROVES REDUCES OVARIAN APOPTOSIS RESERVE IMPROVES AUGMENTS OVARIAN IGF ENVIRONMENT DHEA

51
1)Dehydroepiandrosterone (DHEA)
The mechanism by which DHEA supplementation may increase oocyte yield in poor responders is unknown. 1- Animal models support the theory that androgens might facilitate the response of the growing follicles to FSH. 2-In humans, this may result in higher AFC in patients with higher ovarian androgen levels such as in patients with polycystic ovary syndrome. It can also be responsible for the exaggerated ovarian response to exogenous gonadotropins in COH.

52
3-Other theories include an increase of IGF-1 during gonadotropin stimulation, and improved follicular steroidogenesis . 4- In some studies, higher baseline testosterone levels were found to be associated with a higher number of oocytes retrieved and improved IVF outcomes . Older patients have been shown to have diminished levels of DHEAs and may benefit from achieving normal serum levels . 5-It has also been postulated that DHEA supplementation reduces follicular apoptosis, thereby increasing the pool of primordial follicles.

53
2)Simple cyst drainage prior to stimulation protocols :
One of the most significant side effects of pituitary down regulation with GnRH agonists in COH protocols is ovarian cyst formation. The incidence of these cysts ranges from 8 to 53% . Formation of follicular cysts may be related to the endogenous gonadotropin flare in response to mid-luteal GnRH agonists. The impact of these ovarian cysts on IVF outcomes remains controversial.

54
There is evidence of poor IVF performance in patients who form ovarian cysts in response to GnRH agonists in both poor responders and normal responders. The worst outcomes were found with: Hormonally inactive cysts greater than 15 mm . While follicular cyst formation prior to IVF is probably a poor prognosticator, further studies are required to determine whether to proceed, wait or drain the cyst prior to the cycle.

55
3)Addition of Estradiol in the Luteal Phase
Addition of estradiol in the luteal phase ± GnRH antagonist →→→Decreases the risk of cycle cancellation & Increases the chance of clinical pregnancy in poor responder REASON: luteal estradiol priming could improve synchronization of the pool of follicles available to controlled ovarian stimulation.

57
4)Addition of Growth Hormone:
MECHANISM: modulating the action of FSH on granulosa cells by upregulating the local synthesis of insulin-like growth factor-I (IGF-I). Addition of GH significantly increased the probability of live birth in poor responders.
. Addition of GH significantly increased the probability of live birth in poor responders.")
58
5)Addition of Aspirin: MECHANISM:
Increased intraovarian vascularity→→improving delivery of gonadotropic or other growth factors required for folliculogenesis. On the other hand, impaired ovarian blood flow could contribute to poor ovarian response. Although some papers have reported some beneficial effects of aspirin from the day of embryo transfer others have failed to confirm these findings.

59
On the basis of updated evidence: A low dose of aspirin has no substantial positive effect on the likelihood of pregnancy and it should not be routinely recommended for women undergoing IVF.

60
The benefits & risk of precycle oral contraceptive pill or antagonist suppression combined with estrogen priming BENEFITS: OCP pretreatment in IVF protocols establishes: an estrogenic environment increases sex hormone-binding globulin levels decreasing follicular androgen levels →→→ may delay apoptosis.

61
The progestin component of the OCP :
suppresses luteinizing hormone (LH) and may synchronize follicular development leading to a more evenly sized follicular response. OCP pretreatment in GnRH agonist flare cycles can prevent an early rise in progesterone by eliminating the corpus luteum. It is also believed that OCPs cause less pituitary downregulation when compared with GnRH agonists used in a long protocol.
 and may synchronize follicular development. leading to a more evenly sized follicular response. OCP pretreatment in GnRH agonist flare cycles can prevent an early rise in progesterone by eliminating the corpus luteum. It is also believed that OCPs cause less pituitary downregulation when compared with GnRH agonists used in a long protocol.")
62
RISKS: OCPs significantly prolong stimulation and increase the dose of gonadotropins . Pituitary suppression with OCPs may blunt a GnRH agonist or letrozole flare response in follicular phase.

64
Double stimulation Combination of two stimulations in one menstrual cycle. Targeted for antral follicles in the follicular phase and luteal phase. Two chances of OPU in a single menstrual cycle Achieve more oocytes and viable embryos FET as a primary strategy(from March my clinic only do FET)
")
65
Antral follicles Many antral follicules in the periovulation time.
Sometimes more antral follicles in the luteal phase than the early follicular phase. For poor responders, it is good opportunity to retrieve oocytes.

66
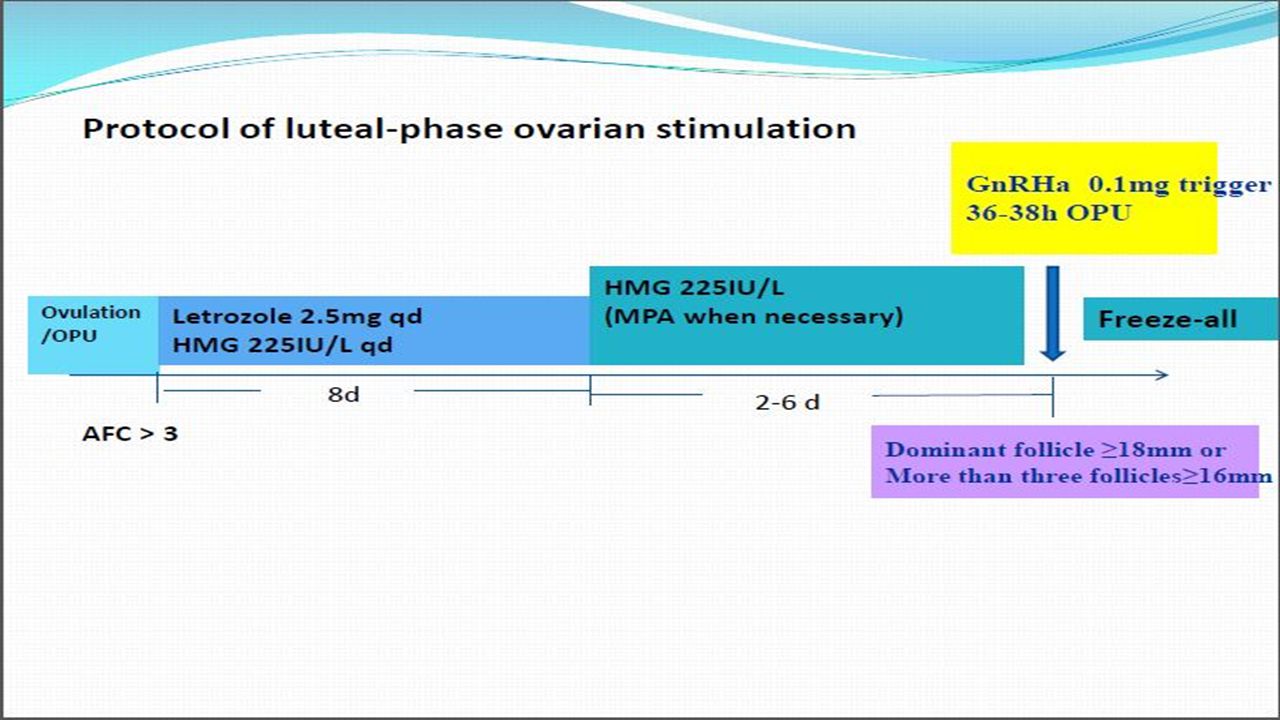
luteal-phase ovarian stimulation
• Targeted for the antral follicles after ovulation or OPU. • Higher progesterone milieu during ovarian stimulation • Protocol: letrozole and HMG

68
• Our data show that luteal-phase ovarian stimulation is feasible for producing potential oocytes/embryos, with potential pregnancy outcomes in subsequent FETs • Advantages: No spontaneous LH surge • lower OHSS incidence

69
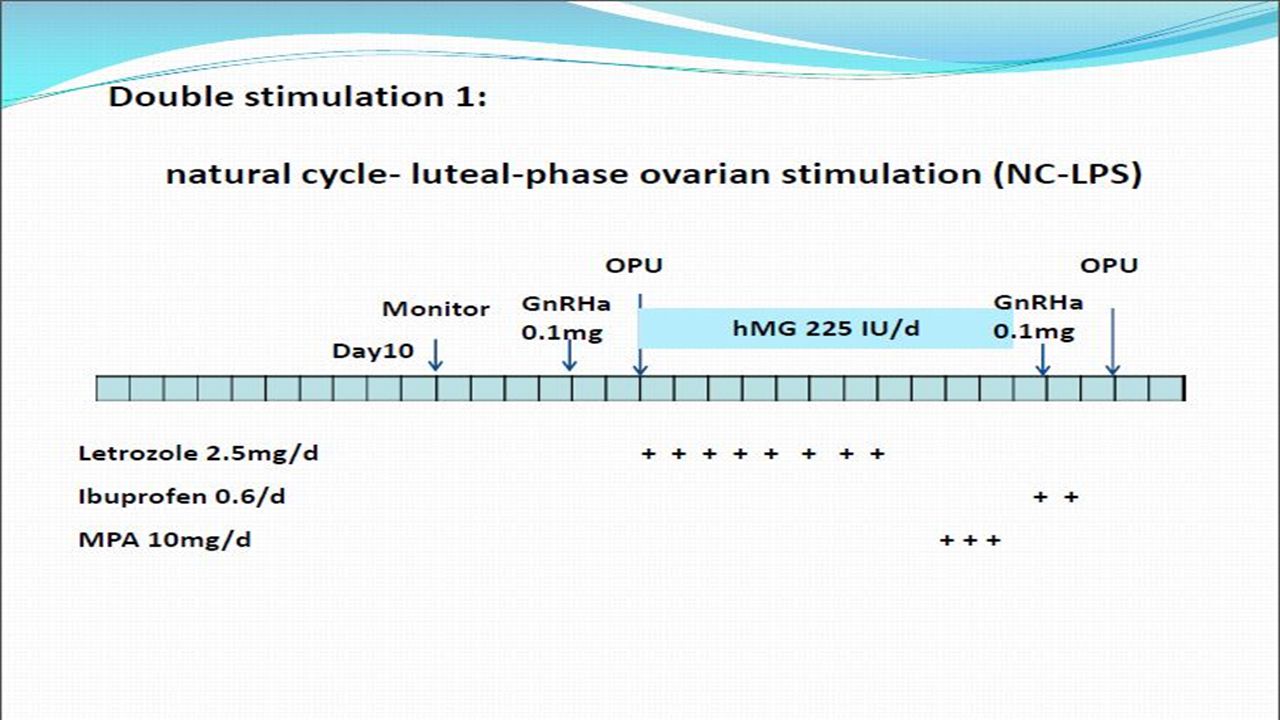
How to do double stimulation in poor responders?
Protocol Natural cycle -luteal-phase ovarian stimulation Mild stimulation-luteal-phase ovarian stimulation

73
Double stimulation in poor responders
• Double stimulation is a promising approach both for patients with poor responders, especially for the cases that repeatedly did not have retrieved or viable embryos using conventional IVF regimens, and for cancer patients needing emergency fertility preservation. • Advantages – More oocytes retrieval – Reduced cancel rate – More flexible stimulation protocol

76
Evidence-based management of poor ovarian response in IVF
Stratis Kolibianakis MD MSc PhD

77
Management of poor responders
Treatment of poor responders has been attempted with various methods in retrospective, prospective, studies using comparative and non-comparative designs Most studies are underpowered and single and thus useful conclusions are difficult to be drawn There is a need for an evidenced based approach in the problem of treatment of poor responders

78
Search strategy: MEDLINE (1966 to November 2009) EMBASE (1988 to November 2009) Cochrane Central Register of Controlled Trials (Cochrane Library Issue 1, 2009) Keywords :(“poor” OR “low” OR “slow” OR “inadequate” OR “suboptimal”) AND (“response” OR “responder” OR “ovarian reserve”) No language limitations Hand-searching
 Keywords :( poor OR low OR slow OR inadequate OR suboptimal ) AND ( response OR responder OR ovarian reserve ) No language limitations. Hand-searching.")
79
Data extraction Demographic type of study number of patients included definition of poor ovarian response Methodological randomization method allocation concealment Procedural type of intervention examined type and protocol of ovarian stimulation Outcome data clinical or ongoing pregnancy rate live birth

80
Inclusion criteria: Prospective parallel two -arm
Randomized controlled trial Full manuscript Exclusion criteria: Quasi-randomization methods (sequential numbers, date of birth, allocation by week day) Participation of patients more than once in studies
 Participation of patients more than once in studies.")
81
Definition of poor ovarian response:
Variable Retrospective vs. Prospective

82
Addition of : Growth hormone (GH) or GH-releasing factor (GHRF) Pyridostigmine Transdermal testosterone Aspirin L-arginine Aromatase inhibitors Modifications of the long GnRH-a protocol Short versus long GnRH agonist protocol

83
GnRH antagonist protocol versus:
GnRH –a protocols No pituitary suppression Natural cycle Modifications of ovarian stimulation Intracytoplasmic sperm injection (ICSI) Kyrou et al, Fertil Steril, 2009 FS
 Kyrou et al, Fertil Steril, 2009 FS.")
84
Background GH enhances GHRF enhances :
gonadotrophin effects on granulosa cells (Lanzone et al., 1992) GHRF enhances : gonadotrophin-induced steroidogenesis cyclic adenosine monophosphate formation (cAMP) (Doldi et al., 1996)
 GHRF enhances : gonadotrophin-induced steroidogenesis. cyclic adenosine monophosphate formation (cAMP) (Doldi et al., 1996)")
85
RD: 17 % Growth hormone for poor responders GH Addition and live birth
(CI 95% to 0.30) Kolibianakis et al 2009 HRU
 Kolibianakis et al 2009 HRU.")
86
Single study (Howles et al., 1999) Addition of GHRF vs. No addition
GHRF Addition: Single study (Howles et al., 1999) Addition of GHRF vs. No addition Live birth rate: 5.2% vs. 4.0% Rate difference: 1.2% (95% CI: -5.3 to +8.1)
 Addition of GHRF vs. No addition. Live birth rate: 5.2% vs. 4.0% Rate difference: 1.2% (95% CI: -5.3 to +8.1)")
87
Conclusions GH Addition: Beneficial effect on the probability of live birth GHRF Addition: No beneficial effect

88
Background Acetylcholinesterase inhibitor
Increase GH secretion by enhancing the action of acetylcholine (Delitala et al., 1988)
")
89
Relevant study: Kim et al ., 1999
N: 70 patients Protocol: GnRH agonist protocol and gonadotrophins Definition of poor response : < 3 oocytes retrieved and/or a minimum requirement of 50 ampoules of gonadotrophins in a previous failed IVF attempt Outcome: ongoing pregnancy / delivery rate

90
Addition of pyridostigmine vs. no addition:
Ongoing pregnancy/delivery rate: 8.6% vs. 22.9% Rate difference : -14.3% (95% CI:-31.4 to +3.2)
")
91
Addition of pyridostigmine
Conclusion: Addition of pyridostigmine does not appear to improve the ongoing pregnancy / delivery rate in poor responders undergoing IVF

92
beneficial effect on the number of small antral follicles
Background Identification of androgens receptors by immunochemistry in the human ovary (Suzuki et al., 1994) Androgens play a critical role on follicular growth (Ryan et al.,1968) Convertion of androgens into estrogens by the aromatase activity of the granulosa cells (Harlow et al., 1988; Shaw et al., 1989) Rationale: beneficial effect on the number of small antral follicles improve ovarian sensitivity to FSH
 Androgens play a critical role on follicular growth (Ryan et al.,1968) Convertion of androgens into estrogens by the aromatase activity of the granulosa cells (Harlow et al., 1988; Shaw et al., 1989) Rationale: beneficial effect on the number of small antral follicles. improve ovarian sensitivity to FSH.")
93
Relevant study: Massin et al.,2006
N: 53 patients Protocol: GnRH-a/recombinant FSH (rFSH) Definition of poor response :E2 <1200 pg/ml on the day of HCG administration, < 5 follicles retrieved, in a previous IVF cycle Outcome : Delivery rate
 Definition of poor response :E2 <1200 pg/ml on the day of HCG administration, < 5 follicles retrieved, in a previous IVF cycle. Outcome : Delivery rate.")
94
Addition of transdermal testosterone vs. placebo
Delivery rate: 8.3% vs. 4% Rate difference: 4.3% (95% CI:-12.3 to +22.2) Massin et al.,2006
 Massin et al.,2006.")
95
Testosterone addition in poor responders treated by IVF
Conclusion: Testosterone addition in poor responders treated by IVF does not appear to result in an increased probability of pregnancy Massin et al.,2006

96
Background: Beneficial effect of the addition of low-dose aspirin in:
- patients with low uterine blood flow undergoing thawed ET (Wada et al., 1994) -oocytes donation recipients with a thin endometrium (Weckstein et al.,1997) Rationale: impaired ovarian blood flow (Battaglia et al ., 2000)
 -oocytes donation recipients with a thin endometrium. (Weckstein et al.,1997) Rationale: impaired ovarian blood flow (Battaglia et al ., 2000)")
97
Relevant study: Lok et al., 2004
N: 60 patients Protocol: GnRH-a/HMG Definition of poor response : recruitment of fewer than 3 mature follicles (≥17mm) in previous IVF attempt or presence of repeated high basal levels of FSH (>10IU/L) Outcome : clinical pregnancy rate
 in previous IVF attempt or presence of repeated high basal levels of FSH (>10IU/L) Outcome : clinical pregnancy rate.")
98
Addition of Aspirin vs. placebo
Clinical pregnancy rate: 3.33% vs. 6.77% Rate difference: -3.33% (95% CI: to )
")
99
A beneficial effect of low-dose aspirin
Conclusion A beneficial effect of low-dose aspirin in poor responders undergoing IVF is not currently supported

100
Background Increased vascularization appears to play a critical role in the selection, growth and maturation of follicles in both natural and IVF cycles (Weiner et al.,1993) Nitric oxide (NO), a product of L-arginine, is an intra and intercellular modulator in many biologic processes, including ovarian physiology NO participates in periovulatory vasodilatatory modulation of the ovarian blood flow in the rat (Ben-Shlomo, 1994)
 Nitric oxide (NO), a product of L-arginine, is an intra and intercellular modulator in many biologic processes, including ovarian physiology. NO participates in periovulatory vasodilatatory modulation of the ovarian blood flow in the rat (Ben-Shlomo, 1994)")
101
Background NO play a role in follicular maturation and ovulation. (Anteby et al., 1996) L-arginine is involved in the formation of NO either by a calcium dependent or a cytokine-inducible NO synthatase (Moncada et al., 1991)
")
102
Relevant study: Battaglia et al.,1999 N: 34 patients
Protocol: flare-up GnRH-a/pFSH Definition of poor response : at least one previous cycle cancellation due to E2<1100 pmol/l and/or < 3 follicles recruited by day 8 in a previous IVF cycle Outcome : cumulus-oocyte complexes (COCs), pregnancy rate
, pregnancy rate.")
103
Addition of L-arginine vs. placebo COCs: 4.1 ± 1.9 vs. 1.6 ± 0.5
Battaglia et al.,1999 Addition of L-arginine vs. placebo COCs: 4.1 ± 1.9 vs. 1.6 ± 0.5 WMD: 2.5 (95% CI: 1.53 to 3.47) Pregnancy rate : 17.6% vs. 0% Rate difference: 17.6% (95% CI: -4.1 to +41.0)
 Pregnancy rate : 17.6% vs. 0% Rate difference: 17.6% (95% CI: -4.1 to +41.0)")
104
Addition of L-arginine: no beneficial effect
Battaglia et al.,1999 Conclusion Addition of L-arginine: no beneficial effect

105
Background: The selective inhibition of aromatase: - prevents the overall production of estrogens and their negative feedback on the hypothalamus- hypophysis axis -results in an increased pituitary production of FSH (Simpson et al .,2000) -may increase the production of follicular androgens, which might improve follicular sensitivity or stimulate IGF- 1 (Giudice et al., 1992; Palter et al., 2001
 -may increase the production of follicular androgens, which might improve follicular sensitivity or stimulate IGF- 1. (Giudice et al., 1992; Palter et al.,")
106
renders AI an attractive option for poor responders
-induces ovulation in anovulatory PCOS women (Mitwally and Casper, 2000) -increases ovarian sensitivity to gonadotrophins renders AI an attractive option for poor responders (Mitwally and Casper, 2002)
 -increases ovarian sensitivity to gonadotrophins. renders AI an attractive option for poor responders. (Mitwally and Casper, 2002)")
107
Relevant study: Goswami et al .,2004
N:38 patients Protocol: long GnRH-a/rFSH protocol Definition of poor response : Poor ovarian response was defined as one to three failed IVF attempts, in which less than two dominant follicles developed Outcome : pregnancy rate

108
Goswami et al .,2004 Addition of aromatase inhibitors vs.placebo
Pregnancy rate/ cycle: 23.1% vs. 24.0% Rate difference: -0.9% ( 95% CI to +29.0)
")
109
does not appear to improve clinical pregnancy rate
Goswami et al .,2004 Conclusion Letrozole addition does not appear to improve clinical pregnancy rate in poor responders undergoing IVF

110
Background: Different dosages of GnRH agonist
Different protocols for GnRH agonist administration have been used to enhance pregnancy rates in patients with poor ovarian response.

111
Relevant study: N: 63 patients
Dirnfeld et al.,1999 N: 63 patients Protocol: standard long luteal protocol versus a stop agonist long protocol. In the stop agonist protocol administration of GnRH-a was initiated in the midluteal phase and was stopped upon adequate down- regulation. Relevant study: Garcia-Velasco et al.,2000 N: 70 patients Protocol: “stop” versus “non-stop” protocol i) non-stop protocol: GnRH-a long protocol/high doses of FSH+HMG or (ii) stop protocol: GnRH-a initiated in midluteal phase of the previous cycle and was stopped with the onset of menses, FSH+HMG doses similar to the non stop protocol
 non-stop protocol: GnRH-a long protocol/high doses of FSH+HMG or (ii) stop protocol: GnRH-a initiated in midluteal phase of the previous cycle and was stopped with the onset of menses, FSH+HMG doses similar to the non stop protocol.")
112
Dirnfeld et al.,1999 Definition of poor response :
Garcia-Velasco et al.,2000 Definition of poor response : ≤ 4 mature oocytes retrieved in at least one previous IVF cycle and/or a previous low response to COH, as evidenced by a peak E2 level of<2.000 pmol/L Outcome : ongoing pregnancy rate Definition of poor response : development of less than three follicles ≥18mm in diameter in a previous IVF attempt and presence of basal FSH concentration <12IU/ml Outcome : pregnancy rate

113
Ongoing pregnancy rate : 5.0% vs. 2.6%
-Dirnfeld et al.,1999 Stop agonist protocol vs. standard long protocol Ongoing pregnancy rate : 5.0% vs. 2.6% Rate difference: 2.4% ( 95% CI ) -Garcia-Velasco et al.,2000 Non- stop vs. stop protocol Pregnancy rate : 13.9% vs. 17.6% Rate difference: 3.7% ( 95% CI to +13.7)
 -Garcia-Velasco et al.,2000. Non- stop vs. stop protocol. Pregnancy rate : 13.9% vs. 17.6% Rate difference: 3.7% ( 95% CI to +13.7)")
114
The modifications of the long agonist protocol described
Dirnfeld et al.,1999 Garcia-Velasco et al.,2000 Conclusion The modifications of the long agonist protocol described do not appear to enhance the probability of pregnancy over the conventional long protocol

115
Background: Suppression of premature LH surge: Short protocol:
promotes follicular growth by taking advantage of the flare- up effect of GnRH-agonist on pituitary gonadotrophin release Long protocol: results in a more coordinated follicular growth.

116
Relevant study: Weissman et al .,2003
N:60 patients Protocol: Short protocol: a high dose of GnRH-a for 4 days, followed by standard GnRH-a dose Long protocol: a standard GnRH-a dose was used until pituitary down- regulation, following by halving the GnRH-a dose Definition of poor response : presence of fewer than 5 oocytes retrieved or three or fewer follicles of 16mm or larger developed on the day of cycle cancellation, or serum E2 level < 500pg/ml on the day of HCG administration Outcome :clinical pregnancy rate

117
Weissman et al .,2003 Mini-dose long protocol vs. modified short protocol Clinical pregnancy rate/ started cycle: 22,6% vs 3,4% p=0.053 Rate difference: +19.2% ( 95% CI: to +38.6)
")
118
The two protocols appear to yield the same results
Weissman et al .,2003 Conclusion The two protocols appear to yield the same results in poor responders undergoing IVF

119
Background: GnRH antagonist prevent the suppression of endogenous gonadotrophin secretion at the stage of follicular recruitment (Craft et al., 1999; Tarlatzis et al., 2003).
.")
120
GnRH-antagonists in poor responders
Griesinger et al 2006 Relevant studies:8 Total N: 575 patients Protocols: 2 studies→ long agonist protocol 6 studies → flare-up protocol Definition of poor response: In the majority of studies →“inappropriate ovarian response” during a previous stimulated cycle. Only in two studies→ age of the patients and the basal FSH concentrations used as criteria Outcome: clinical pregnancy rate, COCs

121
Clinical pregnancy rate
GnRH-antagonists in poor responders Griesinger et al 2006 . Agonist vs.antagonist Clinical pregnancy rate OR=1.28 (95% CI: )
")
122
GnRH-antagonists in poor responders
Griesinger et al 2006 Long agonist group vs. GnRH-ant group COCs SDF (95 % CI: )
")
123
GnRH-antagonists in poor responders
Griesinger et al 2006 Conclusion No difference in pregnancy rates appears to exist between GnRH agonists and antagonists in poor responder patients

124
Relevant study: Akman et al.,2000
N: 40 patients Protocol: GnRH-ant/FSH+HMG vs FSH+HMG Quasi-randomization Definition of poor response : at least two previous IVF attempts with low response due to the one of the following reasons: baseline FSH concentrations >15mIU/ml, E2 on the day of HCG < 500pg/ml, or fewer than four oocytes retrieved Outcome : ongoing pregnancy rate

125
GnRH antagonist group vs. control group
Akman et al.,2000 GnRH antagonist group vs. control group Clinical pregnancy rate: 20.0% vs. 6.2%

126
The addition of GnRH antagonists to ovarian stimulation
Conclusion The addition of GnRH antagonists to ovarian stimulation does not appear to offer any benefit in poor responder patients undergoing IVF

127
Background: Short agonist vs. natural cycle
the use of natural cycle IVF in poor responder patients as alternative to COH and oocyte donation: →less invasive → less costly

128
Short agonist vs. natural cycle
Relevant study: Morgia et al .,2004 N: 129 patients Protocol: natural cycle versus a short agonist protocol Definition of poor response : retrieval of three or fewer oocytes in a previous attempt or cancellation of the cycle because of no follicular development Outcome : pregnancy rate

129
Short agonist vs. natural cycle
Morgia et al .,2004 Natural cycle vs. short agonist Pregnancy rate: 6.1% vs. 6.9%, respectively Rate difference: 0.8% (95% CI: -8.2 to +6.2)
")
130
Short agonist vs. natural cycle
Morgia et al .,2004 Conclusion No beneficial effect of natural cycle compared to short agonist protocol in poor responders

131
High vs standard dose of FSH
High vs decremental dose of FSH

132
Relevant study: Cedrin-Durnerin et al., 2000 N: 96 patients
Protocol: high fixed dose of gonadotropins versus a decremental dose in a short mini-dose GnRH-a protocol Definition of poor response : retrieval of fewer of five oocytes in a previous IVF cycle or elevated baseline FSH or E2 levels on cycle day 3 Outcome : pregnancy rate Relevant study: Klinkert et al .,2005 N: 52 patients Protocol: higher starting dose of gonadotrophins during a long GnRH –a protocol Definition of poor response : the presence of fewer than four oocytes retrieved or fewer than three follicles developed on the day of cycle cancellation Outcome :ongoing pregnancy rate cedrin durnerin not retrospective klinkert AFC definition

133
Cedrin-Durnerin et al., 2000 Decremental group vs.high fixed dose group Pregnancy rate: 6.25% vs. 8.33% Rate difference: 2.08 (95% CI: to +9.64) Klinkert et al .,2005 Standard dose of FSH vs. double dose Ongoing pregnancy rate: 7.69% vs. 3.85% Rate difference: 3.84 ( 95% CI: to )
 Klinkert et al .,2005. Standard dose of FSH vs. double dose. Ongoing pregnancy rate: 7.69% vs. 3.85% Rate difference: 3.84 ( 95% CI: to )")
134
A high fixed-dose gonadotrophin regimen
Cedrin-Durnerin et al., 2000 Klinkert et al .,2005 Conclusion A high fixed-dose gonadotrophin regimen does not improve the pregnancy rate in poor responder patients

135
Initiation of FSH during the luteal phase
Background: B) The antral follicles are present in late follicular phase of the ovarian cycle and initiation of their further development occurs under the action of the premenstrual FSH rise (Gougeon et al, 1996) Rationale: Earlier administration of FSH might ↑ the number of recruited follicles by opening the recruitment window in the late luteal phase of the preceding cycle
 The antral follicles are present in late follicular phase of the ovarian cycle and initiation of their further development occurs under the action of the premenstrual FSH rise. (Gougeon et al, 1996) Rationale: Earlier administration of FSH might ↑ the number of recruited follicles by opening the recruitment window in the late luteal phase of the preceding cycle.")
136
Relevant study: Rombauts et al., 1998
N:40 patients Protocol: initiating FSH during the luteal phase Definition of poor response : retrieval of three to six oocytes in the last FSH stimulated IVF or GIFT cycle. Outcome : COCs

137
Luteal initiation of FSH vs. follicular initiation of FSH
Rombauts et al., 1998 Luteal initiation of FSH vs. follicular initiation of FSH Number of oocytes retrieved/cycle : median: 4.5, range: vs. median: 6, range: 1-10 no data on pregnancy rate

138
The administration of FSH in the luteal phase
Rombauts et al., 1998 Conclusion The administration of FSH in the luteal phase has no beneficial effect on the total number of oocytes retrieved in poor responder patients

139
Background Available evidence is not able to demonstrate
whether ICSI is more efficacious than conventional IVF in poor responder patients (Van Steirteghem 1993)
")
140
Relevant study: Moreno et al.,1998
N: 104 patients Protocol: long GnRH-a protocol/HMG+FSH. Fertization method: ICSI or IVF Definition of poor response: retrieval of six or fewer oocytes in a previous cycle. Outcome : pregnancy rate

141
Rate difference: -3.8% ( 95% CI -18.9 to +11. 4)
Moreno et al.,1998 IVF vs. ICSI Pregnancy rate : 17.3% vs. 21.1% Rate difference: -3.8% ( 95% CI to )
")
142
are not dependent on the fertilization method in poor responders,
Moreno et al.,1998 Conclusion Pregnancy rates are not dependent on the fertilization method in poor responders, however more studies are necessary

143
The management of poor responders still represents a challenge for the clinician, which is further complicated by the variations in the definition of poor ovarian response With the exception of GH co-administration, none of the examined approaches appears to be beneficial Due to the low incidence of poor ovarian response, evaluation of the interventions proposed is usually performed in single, underpowered studies, which might not allow the detection of the true effect of an intervention

Similar presentations


















 Is It Safe? Mustafa Uğur Zekai Tahir Burak Women’s Health Education and Research Hospital, Ankara, Turkey.>")







