Download presentation
Presentation is loading. Please wait.

1
Adult Substance Abuse Provider Training
Presented by Carl Chrisman LMHP, Teresa Campbell LMHP and Beth Stratton LMHP, LADC

2
Training Objectives Review the Magellan clinical process for admission requests using ASAM guidelines. Review and use the new concurrent request form.

3
Training Assumptions: All clients have had a comprehensive ASAM substance abuse evaluation prior to admission. All providers use the ASAM PPC to determine service needs and level of care.

4
Set Up: Training Call This is an admission call to STR (III.5)
The provider has the comprehensive biopsychosocial ASAM assessment in front of them. The Magellan care manager goes through all the necessary information to make an ASAM level of care determination.

5
Role Play [telephone ring here]
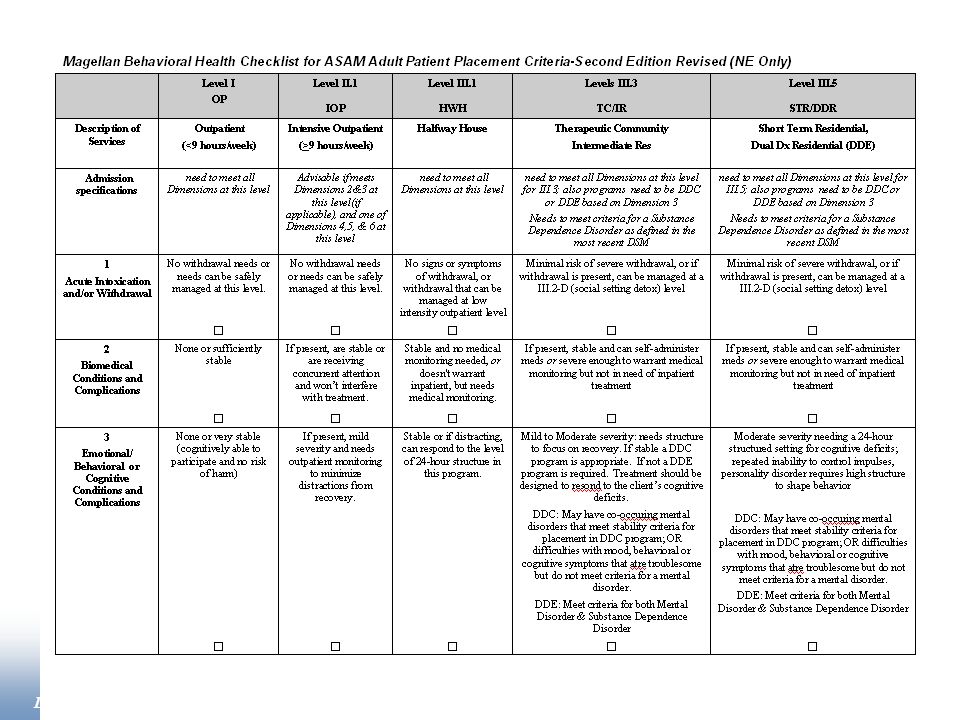
Criteria are from the NE Yellow Book Levels of Care and Placement Criteria adapted by permission of the publisher from Mee-Lee D, Shulman G, Fishman M, Gastfriend D & Harris JG, eds. (2001). ASAM Patient Placement Criteria for the Treatment of Substance-Related Disorders, Second Edition-Revised (ASAM PPC-2R), Chevy Chase, MD; American Society of Addiction Medicine. Copyright All rights reserved.
![Role Play [telephone ring here]](http://slideplayer.com/slide/4059081/13/images/5/Role+Play+%5Btelephone+ring+here%5D.jpg "Criteria are from the NE Yellow Book. Levels of Care and Placement Criteria adapted by permission of the publisher from Mee-Lee D, Shulman G, Fishman M, Gastfriend D & Harris JG, eds. (2001). ASAM Patient Placement Criteria for the Treatment of Substance-Related Disorders, Second Edition-Revised (ASAM PPC-2R), Chevy Chase, MD; American Society of Addiction Medicine. Copyright All rights reserved.")
6
Discussion What dimensions are met for STR? Why not IOP?
What do the dimensions say for IOP or for STR? When is a dual diagnosis enhanced (DDE) program needed for mental health/substance abuse treatment? Review II.1 and III.3
 program needed for mental health/substance abuse treatment Review II.1 and III.3.")
7
Review III.5 STR Criteria
Dimension 1: Acute Intoxication &/or Withdrawal Potential: At minimal risk of withdrawal, at Levels III.3 or III.5. If withdrawal is present, it meets Level III.2-D criteria. Dimension 2: Biomedical Conditions & Complications: None or stable, or receiving concurrent medical monitoring. Dimension 3: Emotional, Behavioral or Cognitive Conditions & Complications: Demonstrates repeated inability to control impulses or a personality disorder requires structure to shape behavior. Other functional deficits require a 24-hour setting to teach coping skills. A Dual Diagnosis Enhanced setting is required for SPMI Severely and Persistently Mentally Ill patients. Moderate. Dimension 4: Readiness to Change: Has marked difficulty with, or opposition to tx, with dangerous consequences; or there is high severity in this dimension but not in others. The client, therefore, needs a Level I motivational enhancement program. Dimension 5: Relapse, Cont. Use or Cont. Problem Potential: Has no recognition of the skills needed to prevent continued use, with imminently dangerous consequences. Dimension 6: Recovery Environment: Environment is dangerous and client lacks skills to cope outside of a highly structured 24-hour setting.

8
Review Level II.1 IOP Criteria
Dimension 1: Acute Intoxication &/or Withdrawal Potential: Minimal risk of severe withdrawal. Dimension 2: Biomedical Conditions & Complications: None or not a distraction from treatment. Such problems are manageable at Level II.1. Dimension 3: Emotional, Behavioral or Cognitive conditions & Complications: Mild severity, w/potential to distract from recovery; needs monitoring. Dimension 4: Readiness to change: Has variable engagement in treatment, ambivalence, or lack of awareness of the substance use or mental health problem, and requires a structured program several times a week to promote progress through the stages of change. Dimension 5: Relapse, Cont. Use or Cont. Problem Potential: Intensification of addiction or mental health symptoms indicate a high likelihood of relapse or continued use or continued problems without close monitoring and support several times a week. Dimension 6: Recovery Environment: Recovery environment is not supportive but, with structure and support, the client can cope.

9
Admission Call Revisited

10
The Admission Call DISCLAIMER AND CALL RECORDED
DEMOS: LOC and Service Requested; Estimated Length of Stay (based upon estimated time it will take to meet goals PRESENTING PROB and Why Now:: Why are we admitting now versus last week or last month. Why Now explanations may become treatment plan goals. D3 - MSE:: Determine if the client is at base line or is having acute symptoms in order to recommend the right service. Trauma history is included here. SI/HO

11
D2 MEDICAL CONCERNS:: Be sure to have information from the most recent health screen or physical regarding withdrawal if applicable. D 2 & 3 CURRENT MEDICATION:: Do we know if the client is compliant with psychotropic medication? Is medical support available to do medication management. D 5 & 6 FAMILY/COMMUNITY SUPPORT:: Natural supports section. Strengths to build on. TX HISTORY/PREVIOUS SOLUTIONS:: Do we know of service combinations that were successful in the past ? Where there extended periods where the client was not hospitalized? Can we identify any conditions which supported this? D6 LEGAL HISTORY:: Legal charges, court orders, etc.

12
D 5 & 6 CASE MANAGEMENT/OP PROVIDER:: Does the client have OP providers, are they coordinated?
D 2 PCP:: Does the client have a primary care physician? If not, can they be referred to a physical health provider? TX PLAN:: The dimensions with the highest rating must be addressed in the treatment plan. D 5 & 6 DC PLAN:: Initial d/c plan, ideas regarding supports that will be necessary when service goals are met.

13
D 3 & D4 - PERSONAL STRENGTHS:: Include level of motivation, achievements, interests, hobbies, skills, etc. D3 - FUNCTIONAL IMPAIRMENTS:: Related to use. DDE SPMI Criteria. D(ALL) RISK SUBSTANCE ABUSE:: Assess risk level for all six dimensions to determine. The dimensions with the highest ratings determine the immediate service needs and placement decision. D1,2,3, 6 DIAGNOSIS:: Axis I – V.
 RISK SUBSTANCE ABUSE:: Assess risk level for all six dimensions to determine. The dimensions with the highest ratings determine the immediate service needs and placement decision. D1,2,3, 6 DIAGNOSIS:: Axis I – V.")
14
ASAM Overview

15
All Six Assessment Dimensions are Managed and Monitored A Biopsychosocial Approach to Assessment and Treatment 1. Acute Intoxication and/or Withdrawal Potential 2. Biomedical Conditions and Complications 3. Emotional, Behavioral or Cognitive Conditions and Complications 4. Readiness to Change 5. Relapse/Continued Use, Continued Problem Potential 6. Recovery Environment

16
Dimension 1 Acute Intoxication and/or Withdrawal Potential
Assessment considerations Risk level Use history Current signs of withdrawal Supports

17
Dimension 2 Biomedical Conditions & Complications
Assessment considerations -Current physical illnesses -Chronic health conditions -Can client self manage -What supports are medically necessary

18
Dimension 3 Emotional, Behavioral or Cognitive Conditions & Complications
Assessment considerations -Current Psychiatric illness -Chronic Conditions -Part of the addictive disorder -Mental Health specific treatment -Activities of daily living -Treatment Barrier Treatment Goals

19
Dimension 4 Readiness to Change
Assessment Considerations -Resistance -Degree of readiness -Motivational Enhancement Approach (Treatment Goal) -Clinician Interpretation
 -Clinician Interpretation.")
20
Stages of change Precontemplation Contemplation Preparation Action
Relapse Maintenance

21
Therapist’s Motivational Tasks (Treatment Goals)
Pre-contemplation ----Raise doubt — increase the client’s perception of risks and problems with current behavior. Contemplation ----Tip the balance — evoke reasons to change, risks of not changing; strengthen the client’s self-efficacy for change of current behavior. Preparation ---Help the client to determine the best course of action to take in seeking change Action ---Help the client to take steps toward change Maintenance---Help the client to identify and use strategies to prevent relapse Relapse---Help the client to renew the processes of contemplation, determination, and action, without becoming stuck or demoralized because of relapse

22
Dimension 5 Relapse, Continued Use or Continued Problem Potential
Assessment Considerations -Mental health issues -History (Relapse does not equal higher level of care) -Sequence of factors of relapse -Coping skills, severity of other problems, own awareness, impulse control
 -Sequence of factors of relapse. -Coping skills, severity of other problems, own awareness, impulse control.")
23
Dimension 6 Recovery/Living Environment
Assessment Considerations -Support members use -Sober support -Community supports to aid sobriety -Other complications (child care, transportation, housing, etc)
")
24
Each Dimension is Rated
Low / Moderate / High Severity

25
Level of Functioning/Severity
Low Minimal current difficulty or impairment. Absent, minimal or mild signs and symptoms. Acute or chronic problems mostly stabilized or soon able to be stabilized and functioning restored with minimal difficulty. No immediate service(s) or low intensity of services needed for this Dimension. Treatment strategies usually able to be delivered in outpatient setting.
 or low intensity of services. needed for this Dimension. Treatment strategies usually. able to be delivered in outpatient setting.")
26
Level of Functioning/Severity
Moderate Moderate difficulty or impairment. Moderate to serious signs and symptoms. Difficulty coping or understanding, but able to function with clinical and other support services and assistance. Moderate intensity of service(s), skills training, or supports needed for this Dimension. Treatment strategies may require intensive levels of outpatient care.
, skills training, or. supports needed for this Dimension. Treatment strategies. may require intensive levels of outpatient care.")
27
Level of Functioning/Severity
High Severe difficulty or impairment. Serious, gross or persistent signs and symptoms. Very poor ability to tolerate & cope with problems. High intensity of service(s), skills training, or supports needed. More immediate, urgent services may require inpatient or residential settings, or closely monitored case management/support services at frequency greater than daily.
, skills training, or. supports needed. More immediate, urgent services may. require inpatient or residential settings, or closely monitored. case management/support services at frequency greater. than daily.")
28
Concurrent Review Form (Treatment Plan)
Use for IOP/HWH/IR/TC/STR/DDR Levels II.1/III.3/III.5 FAX or Mail Two Weeks Prior to End Date

30
Using the Form Check the specific Treatment box
Treatment Requested is the same as the box checked ASAM Level End date SS# and Medicaid # Anticipated D/C date Service Location For Each Dimension describe Strengths, Goal, Progress, Changes

31
Treatment Planning Motivation level/stage of change & treatment plan goals/activities need to be congruent (Discovery vs. Recovery) Dimensions of high risk are areas of focus; tie your treatment plan to your ASAM dimensions and areas of identified risk… SMART-SPECIFIC; MEASURABLE; ATTAINABLE; RELEVANT; TIME LIMITED KEEP IT SIMPLE INDIVIDUALIZED, group therapy is an expectation, doesn’t go on the treatment plan

32
Address Treatment Progress
Have the risk factors previously identified decreased; have the behaviors previously identified decreased in frequency, severity? Has the client developed new tools/ strategies to address those risk factors? What are the barriers & risk factors that still exist, & what are the strengths, resources & protective factors that the family & client possess, what skills have they developed? What interventions are you incorporating to motivate client/family; how are you utilizing the strengths of the client & family system to move the client toward the next level of motivation, and toward a safe enough level to move to a lower level of care?

33
Crosswalk to Medicaid & Behavioral Health Levels of Care

36
ASAM Dimension Questions
Appendix A

37
ASAM Dimension Questions
Acute Intoxication and/or Withdrawal Potential What substances is client using? How much? How often? How recently? How long? Method of use? Any signs of Intoxication or withdrawal now? Vitals? If so, what are they? What is BAL? Has UA been obtained? What are results? What meds has the client been given for withdrawal? History of withdrawal? Biomedical conditions and complications Does the client have any medical problems? (Is she pregnant?) What is the client’s weight/height? Has this changed recently? What medications is the client on for these medical problems?
 What is the client’s weight/height Has this changed recently What medications is the client on for these medical problems")
38
ASAM Dimension Questions
Emotional, Behavioral, or Cognitive Conditions/Complications What mental health diagnoses besides substance abuse does the client have? Does the client exhibit any mental health symptoms? Does the client have any cognitive impairments? Orientation? Memory? Concentration? What is the client’s mental health history? Any suicide attempts? Any hospitalizations for MI? Any placements? Who is the client’s psychiatrist/therapist? Is the client on or has he/she been on any psychotropic meds? What are they? Family history of MI?

39
ASAM Dimension Questions
Readiness to Change Has the client had prior treatment for substance abuse? When? Where? What level? What was the outcome? What was his/her longest period of sobriety? What did he/she do to stay sober? What is the client’s perception of his/her problem? Does he/she recognize that he/she has a substance abuse problem? What is his/her motivation? Is he/she willing to change? Why now? Why have they come for help at this specific time? What happened that made them seek treatment at this time? Relapse, Continued Use or Continued Problem Potential Does the client have cravings currently? If client had a period of sobriety, what led to client’s relapse? MI? If client hasn’t used for a week, how did they do it and why do they need residential? What resources does the client have to avoid using?

40
ASAM Dimension Questions
Recovery/Living Environment Whom does the client live with? Does anyone in the house use substances? Does the client have a SO? Does he or she use? Any family history of substance abuse? Who? Are they using or in recovery? Any family support for recovery? Does the client have any children? If so, ages and where are they living. Are there any family issues that may impact recovery? What legal charges? When did they occur? Does the client have a court appearance coming up. Is he/she on probation? Is DHS involved? Name of PO/DHS and phone numbers? Will PO/DHS be involved in client’s treatment? What level of education does the client have? Any problems in school? Is the client employed? What is client’s work history? Work potential?

41
References Behavioral Health and Medicaid Managed Care guidelines “Yellow Book” : Behavioral Health and Medicaid Managed Care draft guidelines: ASAM website: Carl Chrisman Magellan Supervisor:

42
The End Questions?

Similar presentations

















>")


