Download presentation
Presentation is loading. Please wait.

1
Diabetes Medications Update
Eric L. Johnson, M.D. Assistant Medical Director Altru Diabetes Center Altru Health System Associate Professor Department of Community and Family Medicine University of North Dakota School of Medicine and Health Sciences Grand Forks, ND

2
Disclosures Off label use of some medications will be discussed

3
Objectives Assess knowledge of usual diabetes medications
Implement proper medication use per guideline management Improve knowledge of side effects and contraindications of diabetes medications

4
Diabetes Mellitus Type 1: Usually younger, insulin at diagnosis
Type 2: Usually older, often oral agents at diagnosis Type “1.5” (Latent Autoimmune), mixed features Gestational: Diabetes of Pregnancy
, mixed features. Gestational: Diabetes of Pregnancy.")
5
U.S. Prevalence of Diabetes 2010
Diagnosed: 26 million people—8.3% of population (90%+ have Type 2) Undiagnosed: 7 million people 79 million people have pre-diabetes CDC 2011
 Undiagnosed: 7 million people. 79 million people have pre-diabetes. CDC")
6
Diabetes Diagnosis Normal <100 <140 <5.7
Category FPG (mg/dL) h 75gOGTT A1C Normal < < <5.7 Prediabetes Diabetes >126** > >6.5 Or patients with classic hyperglycemic symptoms with plasma glucose >200 ** On 2 separate occasions Diagnostic criteria for diabetes have changed. Impaired fasting glucose (IFG) is a new term, defined as fasting plasma glucose between 110 and 125 mg/dL. Diabetes is diagnosed at a serum glucose level of >126 mg/dL on at least two occasions. For low risk individuals over the age of 45 years, the ADA recommends routine screening every 3 years with fasting glucose. OGTT are not recommended for screening. Diabetes Care 35:Supplement 1, 2012
 2h 75gOGTT A1C. Normal <100 <140 <5.7. Prediabetes Diabetes >126** >200 >6.5. Or patients with classic hyperglycemic symptoms with plasma glucose >200. ** On 2 separate occasions. Diagnostic criteria for diabetes have changed. Impaired fasting glucose (IFG) is a new term, defined as fasting plasma glucose between 110 and 125 mg/dL. Diabetes is diagnosed at a serum glucose level of >126 mg/dL on at least two occasions. For low risk individuals over the age of 45 years, the ADA recommends routine screening every 3 years with fasting glucose. OGTT are not recommended for screening. Diabetes Care 35:Supplement 1,")
7
Natural History of Type 2 Diabetes
Uncontrolled Hyperglycemia Obesity IFG* Diabetes 350 – Fasting Glucose Postmeal Glucose 300 – 250 – Glucose (mg/dL) 200 – 150 – 100 – 50 – 250 – Insulin Resistance 200 – Relative Function (%) 150 – 100 – -Cell Failure -cell Function 50 – 0 – -10 -5 5 10 15 20 25 30 Years of Diabetes *IFG=impaired fasting glucose. Copyright® 2000 International Diabetes Center, Minneapolis, USA. All rights reserved. Adapted with permission.
 200 – 150 – 100 – 50 – 250 – Insulin Resistance. 200 – Relative Function (%) 150 – 100 – -Cell Failure. -cell Function. 50 – 0 – Years of Diabetes. *IFG=impaired fasting glucose. Copyright® 2000 International Diabetes Center, Minneapolis, USA. All rights reserved. Adapted with permission.")
8
Decreased Incretin Effect
The Ominous Octet Islet b-cell Impaired Insulin Secretion Decreased Incretin Effect Increased Lipolysis Islet a-cell Increased Glucagon Secretion Insulin and appetite interact in the brain when neurotransmitters in the hypothalamus signal satiety in response to increased insulin. Adding brain and neurotransmitter dysfunction to the pathogenic picture of type 2 diabetes gives us the ominous octet. Increased Glucose Reabsorption Neurotransmitter Dysfunction Increased HGP Decreased Glucose Uptake DeFronzo Diabetes 2008 8

9
Goals of Glucose Management
Targets for glycemic (blood sugar) control in most non-pregnant adults ADA AACE A1c (%) <7* ≤6.5 Fasting (preprandial) plasma glucose mg/dL <110 mg/dL Postprandial (after meal) plasma glucose <180 mg/dL <140 mg/dL R36/p34/P1/L15 Both the ADA and the AACE recommend tight glucose control for persons with diabetes, although their definitions vary. Despite the findings of two large-scale trials, the DCCT and UKPDS, a universally agreed-upon set of glucose management goals has yet to be defined. While almost every diabetes management guideline includes the hallmark variables of A1c and fasting plasma glucose, there are slight variations in specific target values. The American Diabetes Association (ADA) currently recommends a target A1c of <7%, while the American Association of Clinical Endocrinologists (AACE) suggests aiming for a value of 6.5% or lower. The ADA proposes a target range for fasting plasma glucose levels between 90 and 130 mg/dL, while the AACE recommends levels below 110 mg/dL. Postprandial plasma glucose recommendations put forth by the two organizations are <180 and <140 mg/dL, respectively. In addition to these standard variables, there are other important aspects of diabetes management that deserve consideration. Other important issues identified in the two landmark trials, both medically and from a quality of life perspective, include reducing the frequency of hyperglycemic excursions, minimizing the risk of hypoglycemia, especially nocturnal, and minimizing weight gain. Addressing these issues could have an impact on patient motivation and/or treatment compliance, increasing the chance of attaining A1c and plasma glucose goals. References: American Diabetes Association. Standards of medical care in diabetes – Diabetes Care. 2006;29(suppl 1):S4-S42. Implementation Conference for ACE Outpatient Diabetes Mellitus Consensus Conference Recommendations: Position Statement at ImplementationPositionStatement.pdf. Accessed January 6, 2006. R5/pS10/T6 R2/p3/P2 *<6 for certain individuals American Diabetes Association. Diabetes Care. 2012;35(suppl 1) 2011 9
 control in most non-pregnant adults. ADA. AACE. A1c (%) <7* ≤6.5. Fasting (preprandial) plasma glucose mg/dL. <110 mg/dL. Postprandial (after meal) plasma glucose. <180 mg/dL. <140 mg/dL. R36/p34/P1/L15. Both the ADA and the AACE recommend tight glucose control for persons with diabetes, although their definitions vary. Despite the findings of two large-scale trials, the DCCT and UKPDS, a universally agreed-upon set of glucose management goals has yet to be defined. While almost every diabetes management guideline includes the hallmark variables of A1c and fasting plasma glucose, there are slight variations in specific target values. The American Diabetes Association (ADA) currently recommends a target A1c of <7%, while the American Association of Clinical Endocrinologists (AACE) suggests aiming for a value of 6.5% or lower. The ADA proposes a target range for fasting plasma glucose levels between 90 and 130 mg/dL, while the AACE recommends levels below 110 mg/dL. Postprandial plasma glucose recommendations put forth by the two organizations are <180 and <140 mg/dL, respectively. In addition to these standard variables, there are other important aspects of diabetes management that deserve consideration. Other important issues identified in the two landmark trials, both medically and from a quality of life perspective, include reducing the frequency of hyperglycemic excursions, minimizing the risk of hypoglycemia, especially nocturnal, and minimizing weight gain. Addressing these issues could have an impact on patient motivation and/or treatment compliance, increasing the chance of attaining A1c and plasma glucose goals. References: American Diabetes Association. Standards of medical care in diabetes – Diabetes Care. 2006;29(suppl 1):S4-S42. Implementation Conference for ACE Outpatient Diabetes Mellitus Consensus Conference Recommendations: Position Statement at ImplementationPositionStatement.pdf. Accessed January 6, R5/pS10/T6. R2/p3/P2. *<6 for certain individuals. American Diabetes Association. Diabetes Care. 2012;35(suppl 1)")
10
Goals of Glucose Management
More stringent (<6.5) appropriate: -No significant CVD -Short duration -Long life expectancy American Diabetes Association. Diabetes Care. 2012;35(suppl 1)
 appropriate: -No significant CVD. -Short duration. -Long life expectancy. American Diabetes Association. Diabetes Care. 2012;35(suppl 1)")
11
Goals of Glucose Management
Less stringent (<8) appropriate: History of severe hypoglycemia Limited life expectancy Advanced complications or comorbid conditions Longstanding difficult to control diabetes American Diabetes Association. Diabetes Care. 2012;35(suppl 1)
 appropriate: History of severe hypoglycemia. Limited life expectancy. Advanced complications or comorbid conditions. Longstanding difficult to control diabetes. American Diabetes Association. Diabetes Care. 2012;35(suppl 1)")
12
Goals of Glucose Management
Hypoglycemia must be considered “Many factors, including patient preferences, should be taken into account when developing a patient's individualized goals” American Diabetes Association. Diabetes Care. 2012;35(suppl 1)
")
13
A1C ~ “Average Glucose” A1C eAG % mg/dL mmol/L 6 126 7.0 6.5 140 7.8
Formula: 28.7 x A1C eAG American Diabetes Association

14
Diabetes Medications

15
Diabetes Medications Many new medications in last decade
Three main categories Oral agents (pills)- many different kinds old and new Insulin- newer, more modern insulins Newer, non-insulin injectable medications Choices allow individualization of treatment plan Different medications, different indications, different situations
- many different kinds old and new. Insulin- newer, more modern insulins. Newer, non-insulin injectable medications. Choices allow individualization of treatment plan. Different medications, different indications, different situations.")
16
Glucose-lowering Potential of Diabetes Therapies*
Treatment FPG ¯ HbA1C ¯ Sulfonylureas mg/dl 1-2% Metformin mg/dl 1-2% a-Glucosidase Inhibitors (Precose) mg/dl 0.5-1% Repaglinade (Prandin) 60mg/dl 1.7% Thiazolidinediones mg/dl 1-2% Gliptins (Januvia,Onglyza) targets ppd % *based on package insert data as monotherapy
 mg/dl 0.5-1% Repaglinade (Prandin) 60mg/dl 1.7% Thiazolidinediones mg/dl 1-2% Gliptins (Januvia,Onglyza) targets ppd % *based on package insert data as monotherapy.")
17
Glucose-lowering Potential of Injection Diabetes Therapies*
Treatment FPG ¯ HbA1C ¯ Exenatide (Byetta) targets ppd 1-1.5% Liraglutide (Victoza) targets ppd % Pramlintide (Symlin) targets ppd 1-2% Insulin Limited by % hypoglycemia *based on package insert data as monotherapy
 targets ppd 1-1.5% Liraglutide (Victoza) targets ppd 1-1.5% Pramlintide (Symlin) targets ppd 1-2% Insulin Limited by % hypoglycemia. *based on package insert data as monotherapy.")
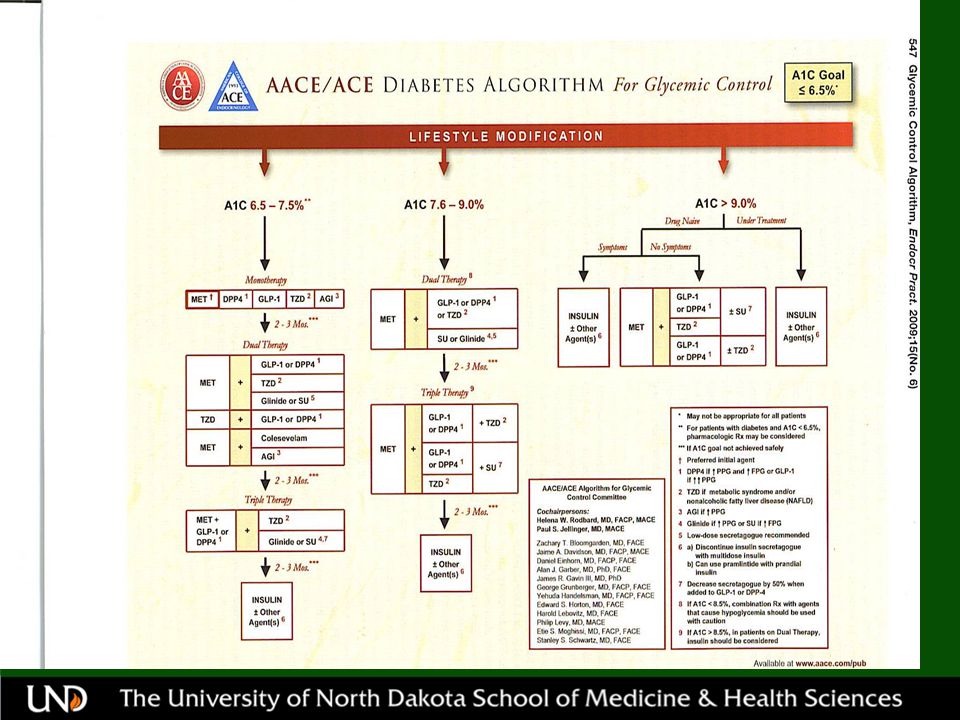
18
ADA/EASD consensus algorithm Type 2
Reinforce lifestyle interventions at every visit and check A1C every 3 months until A1C is <7% and then at least every 6 months. The interventions should be changed if A1C is ≥7%. Tier 1: Well-validated core therapies At diagnosis: Lifestyle and MET + basal insulin Lifestyle and MET + intensive insulin Lifestyle + MET Lifestyle and MET+ SUa Step 1 Step 2 Step 3 Tier 2: Less well-validated therapies/studies Lifestyle and MET + pioglitazone Lifestyle and MET + pioglitazone + SUa No hypgglycemia No edema/CHF Bone loss Lifestyle and MET + GLP-1 agonistb Lifestyle and MET + basal insulin No hypoglycemia No Weight loss Nausea/vomiting aSU other than glyburide or chlorpropamide. bInsufficient clinical use to be confident regarding safety. MET: metformin; SU: sulfonylurea. Nathan et al. Diabetes Care 2009;32(1):
:")
20
Key Points of Medication Selection in Type 2
Metformin at diagnosis unless a contraindication Second line agents- basal insulin or many other meds Advance therapy as disease progresses ADA/EASD will have a new guideline in 2012

21
Oral Diabetes Medications

22
Sulfonylureas Oldest oral medications
Stimulate pancreas to secret more insulin Effective, inexpensive Glyburide, Glipizide, Glimiperide

23
Caveats with Sulfonylureas
Hypoglycemia (particularly in elderly) Premature B-cell exhaustion? Caution in liver disease, renal disease Weight gain Rash Avoid if anaphylactic to sulfa
 Premature B-cell exhaustion Caution in liver disease, renal disease. Weight gain. Rash. Avoid if anaphylactic to sulfa.")
24
Metformin Improves insulin resistance
Reduced Hepatic Glucose production Effective, inexpensive Extremely low incidence of hypoglycemia Weight neutral or weight loss Positive effects on lipid profiles Long term use may result in better CVD outcomes Can be combined with virtually all other DM meds

25
Caveats with Metformin
Liver Disease Renal Disease GI upset Heavy Alcohol Use Intravascular Dye Studies (IVP, Angio,etc) CHF Not for persons over 80 Can result in B12 deficiency
 CHF. Not for persons over 80. Can result in B12 deficiency.")
26
Thiazolidinediones (TZD’s)
Pioglitazone (Actos) Rosiglitazone (Avandia) Improves insulin resistance Extremely low incidence of hypoglycemia The role of TZD’s is rapidly diminishing
 Rosiglitazone (Avandia) Improves insulin resistance. Extremely low incidence of hypoglycemia. The role of TZD’s is rapidly diminishing.")
27
Caveats with TZD’s CHF (or if hx/risk?)
Patients already dealing with edema Potential weight gain Renal disease-fluid overload Current TZD’s rare liver disease, not recommended in active liver disease Heart disease risk? (Rosiglitazone-restrictions) Bladder cancer? Pioglitazone (Actos)
 Bladder cancer Pioglitazone (Actos)")
28
Gliptins(DPP-IV) DPP-IV inhibitors Sitagliptin (Januvia)
Saxagliptin (Onglyza) Linagliptin (Tradjenta) Oral agents Weight neutral or weight loss Can use with Metformin, Sulfonylurea, TZD, or insulin (sitagliptin)
 Linagliptin (Tradjenta) Oral agents. Weight neutral or weight loss. Can use with Metformin, Sulfonylurea, TZD, or insulin (sitagliptin)")
29
Gliptins’ Caveats, Benefits
Hypoglycemia if used with sulfonyurea or insulin Nausea, rash Benefits: Few drug interactions; can be renally dosed

30
“Niche” Drugs Colesevelam (Welchol) - adjunct to lower A1c and LDL
Repaglinide (Prandin), Nateglinide (Starlix) - may replace SU if sulfa allergy - Prandin may be useful in CKD Acarbose (Precose), Miglitol (Glyset) - limited efficacy, GI intolerance, cost Bromocriptine (Cycloset) - limited efficacy? Mechanism uncertain Salsalate-older NSAID, may lower blood sugar, no indication yet
, Nateglinide (Starlix) - may replace SU if sulfa allergy - Prandin may be useful in CKD. Acarbose (Precose), Miglitol (Glyset) - limited efficacy, GI intolerance, cost. Bromocriptine (Cycloset) - limited efficacy Mechanism uncertain. Salsalate-older NSAID, may lower blood sugar, no indication yet.")
31
Non-Insulin Injectable Medications

32
Glucagon-like Peptide-1 (GLP-1)
Gut hormone Stimulates pancreas to secret insulin Suppresses glucagon action Many target organs Weight regulation

33
GLP-1 Medications Exenatide (Byetta) GLP-1 mimetic
Liraglutide (Victoza) GLP-1 analog Both available in pen injectors (easy) Modest weight loss Combined with other agents except DPP-IV inhibitors Exenatide approved for combo use with insulin
 GLP-1 analog. Both available in pen injectors (easy) Modest weight loss. Combined with other agents except DPP-IV inhibitors. Exenatide approved for combo use with insulin.")
34
GLP-1 Caveats Nausea, vomiting Pancreatitis
Medullary thyroid carcinoma in rodents (liraglutide) Hypoglycemia combined with sulfonylurea Caution in renal or hepatic impairment
 Hypoglycemia combined with sulfonylurea. Caution in renal or hepatic impairment.")
35
Pramlintide-Synthetic Amylin (Symlin)
Amylin secreted by normal pancreas along with insulin to regulate blood glucose Enhances Postprandial control. Used in Type 1 and Type 2 patients Used as adjunct to insulin Available in pen injector Possible significant hypoglycemia

36
Combination Drug Therapy
Consider early if failing monotherapy Generally additive or synergistic effects Triple or quadruple non-insulin drug therapy -limited benefit in many -safe for many Insulin is often a better,more potent choice

37
Prediabetes Lifestyle measures are treatment of choice to prevent progression to type 2 diabetes Many meds have some prediabetes data Metformin may be considered in those with prediabetes especially for: BMI >35 kg/m Age <60 years Women with prior GDM or PCOS ADA Diabetes Care. 2012;35(suppl 1)
")
38
Insulin Therapies

39
Intensifying Treatment
Beta-cell function declines as Type 2 diabetes progresses 100 Diagnosis Beta-cell decline exceeds 50% by time of diagnosis 75 Beta-cell function (%) IGT Insulin initiation 50 Postprandial Hyperglycemia 25 Type 2 Diabetes Beta-cell function is tied to glycemic control Type 2 diabetes is characterized by insulin resistance and the progressive loss of islet beta-cell function. Although the former is already established at diagnosis and changes little thereafter, beta-cell function continues to decline, leading to secondary failure of anti-hyperglycemic therapies. In the UKPDS, glycemic deterioration was associated with progressive loss of beta-cell function. Reference Lebovitz H. Insulin secretagogues: old and new. Diabetes Rev 1999;7: 12 8 4 4 8 12 Years from diagnosis Lebovitz H. Diabetes Rev 1999;7: 39
 IGT. Insulin initiation. 50. Postprandial Hyperglycemia. 25. Type 2 Diabetes. Beta-cell function is tied to glycemic control. Type 2 diabetes is characterized by insulin resistance and the progressive loss of islet beta-cell function. Although the former is already established at diagnosis and changes little thereafter, beta-cell function continues to decline, leading to secondary failure of anti-hyperglycemic therapies. In the UKPDS, glycemic deterioration was associated with progressive loss of beta-cell function. Reference. Lebovitz H. Insulin secretagogues: old and new. Diabetes Rev 1999;7: 12. 8. Years from diagnosis. Lebovitz H. Diabetes Rev 1999;7:")
40
Insulin Therapy All Type 1 patients at diagnosis
All type 2 patients will require insulin if they live long enough -7 to 10 years post diagnosis -A1C >9% -Function of many non-insulin meds based on presence of native insulin

41
Insulin Therapy Modern insulins safer and more predictable
Most insulin types come in pen injectors Pen injectors easy to use, to teach, less cumbersome than vials/syringes 41

42
Long-Acting Insulin Detemir (Levemir) Glargine (Lantus)
(Human NPH (N) ) Taken 1 or 2 times daily “Basal” insulin
 ) Taken 1 or 2 times daily. Basal insulin.")
43
Rapid Acting Insulin Aspart (Novolog) Lispro (Humalog)
Glulisine (Apidra) (Human Regular) Taken with meals and snacks “Bolus” insulin
 (Human Regular) Taken with meals and snacks. Bolus insulin.")
44
Insulin Time Action Curves
140 Rapid (Lispro,Glulisine, Aspart) 120 100 Short (Regular) 80 Intermediate (NPH) Insulin Effect 60 40 Long (Detemir,Glargine) 20 2 4 6 8 10 12 14 16 18 20 Hours adapted from R. Bergenstal, IDC
 Short (Regular) 80. Intermediate (NPH) Insulin Effect Long. (Detemir,Glargine) Hours. adapted from R. Bergenstal, IDC.")
45
Basal Insulin in Type 2 Diabetes
Glargine (Lantus), Detemir (Levemir) Good, potent add-on for improved A1C Second line agent for many patients A1C >9, diabetes longer than 5 to 7 years AACE: ? Weight benefit with Detemir Pen injectors easy
, Detemir (Levemir) Good, potent add-on for improved A1C. Second line agent for many patients. A1C >9, diabetes longer than 5 to 7 years. AACE: Weight benefit with Detemir. Pen injectors easy.")
46
Basal Insulin in Type 2 Diabetes
Some oral meds may be continued -metformin, maybe TZD, maybe SU, maybe gliptin (sitagliptin) Glargine (Lantus) or Detemir (Levemir) started at 10 units at HS Increase 3 units every 3 to 5 days until fasting blood sugars <110 (or <140) Most type 2 on units/day
 Glargine (Lantus) or Detemir (Levemir) started at 10 units at HS. Increase 3 units every 3 to 5 days until fasting blood sugars <110 (or <140) Most type 2 on units/day.")
47
Adding Bolus Insulin in Type 2 Diabetes
Lispro (Humalog) Aspart (Novolog) Glulisine (Apidra) Pen injectors Why is bolus insulin important in Type 2?
 Aspart (Novolog) Glulisine (Apidra) Pen injectors. Why is bolus insulin important in Type 2")
48
Fasting and Postprandial Glycemic Excursions as a Function of A1C
20 60 80 2 (7.3–8.4) 3 (8.5–9.2) 4 (9.3–10.2) 5 (>10.2) 1 (<7.3) 40 Contribution (%) A1C (%) Quintiles Postprandial hyperglycemia Fasting hyperglycemia Slide 17 The slide shows the relative contributions of postprandial and fasting hyperglycemia (%) to the overall diurnal hyperglycemia over quintiles of A1C1 These data were obtained from a study of 290 patients with type 2 diabetes conducted to determine the exact contributions of postprandial and fasting glucose increments to overall hyperglycemia1 The relative contribution of postprandial decreased progressively from the lowest to the highest quintile of A1C, while the relative contribution of fasting glucose increased gradually with increasing levels of A1C1 Therefore, the relative contribution of postprandial glucose excursions is predominant in fairly well-controlled patients, whereas the contribution of fasting hyperglycemia increases as diabetes worsens1 Reference Monnier L, Lapinski H, Colette C. Contributions of fasting and postprandial plasma glucose increments to the overall diurnal hyperglycemia of type 2 diabetic patients: variations with increasing levels of A1C. Diabetes Care. 2003;26: Monnier L et al. Diabetes Care. 2003;26:
 3. (8.5–9.2) 4. (9.3–10.2) 5. (>10.2) 1. (<7.3) 40. Contribution (%) A1C (%) Quintiles. Postprandial hyperglycemia. Fasting hyperglycemia. Slide 17. The slide shows the relative contributions of postprandial and fasting hyperglycemia (%) to the overall diurnal hyperglycemia over quintiles of A1C1. These data were obtained from a study of 290 patients with type 2 diabetes conducted to determine the exact contributions of postprandial and fasting glucose increments to overall hyperglycemia1. The relative contribution of postprandial decreased progressively from the lowest to the highest quintile of A1C, while the relative contribution of fasting glucose increased gradually with increasing levels of A1C1. Therefore, the relative contribution of postprandial glucose excursions is predominant in fairly well-controlled patients, whereas the contribution of fasting hyperglycemia increases as diabetes worsens1. Reference. Monnier L, Lapinski H, Colette C. Contributions of fasting and postprandial plasma glucose increments to the overall diurnal hyperglycemia of type 2 diabetic patients: variations with increasing levels of A1C. Diabetes Care. 2003;26: Monnier L et al. Diabetes Care. 2003;26:")
49
Adding Bolus Insulin in Type 2 Diabetes
1 injection basal/1 injection bolus good 2 injection program better than split basal 90/10 rule (90% basal, 10% bolus) Start with largest meal of the day Add other meal doses later (MDI-different formulas) Often stop TZD, always stop SU Easy with pens
 Start with largest meal of the day. Add other meal doses later (MDI-different formulas) Often stop TZD, always stop SU. Easy with pens.")
50
Other Insulins Premix 70/30, 75/25, 50/50
Combine R or rapid acting with NPH or an “NPH-like” component Certain applications may be appropriate Limitation: change 2 insulins at once U-500 Sometimes in severe insulin resistance

51
Severely Insulin Resistant
units total daily dose Obesity Lipodystrophies Donohue and Rabson–Mendenhall Syndrome Type a Insulin Resistance Syndrome and HAIR-AN Garg NEJM 2004 Semple et al Clin Endocrinol. 2010

52
Severely Insulin Resistant
Consider occult infections (UTI, abcess, sinus, etc) Consider other inflammatory conditions (periodontal disease, etc)
 Consider other inflammatory conditions (periodontal disease, etc)")
53
Severely Insulin Resistant
Options: U-500 Add Symlin Add GLP-1 (exenatide now FDA approved with insulin) Change/add “insulin sensitizing” agents Bariatric Surgery Sometimes pump- better absorption, maybe lower daily dose
 Change/add insulin sensitizing agents. Bariatric Surgery. Sometimes pump- better absorption, maybe lower daily dose.")
54
Medication Combinations
Sulfonylureas: Virtually any in type 2 Metformin: Virtually any in type 2 TZD: Virtually any in type 2 Gliptins (DPP-IV): metformin, TZD, insulin (sitagliptin),sulfonylureas Insulin: metformin, TZD, sulfonylurea, amylin, sitagliptin Amylin: only in insulin regimens Exenatide/Liraglutide: metformin, sulfonyureas, TZD
: metformin, TZD, insulin (sitagliptin),sulfonylureas. Insulin: metformin, TZD, sulfonylurea, amylin, sitagliptin. Amylin: only in insulin regimens. Exenatide/Liraglutide: metformin, sulfonyureas, TZD.")
55
Medication Indications
Type 1 Diabetes: Insulin, amylin (amylin only in combination with insulin) Type 2 Diabetes: All oral agents, exenatide, liraglutide, amylin, insulin (amylin only in combination with insulin) Prediabetes: Case by case as discussed
 Type 2 Diabetes: All oral agents, exenatide, liraglutide, amylin, insulin (amylin only in combination with insulin) Prediabetes: Case by case as discussed.")
56
Future Medications SGLT (sodium-glucose co-transporter) 1/2 inhibitors (i.e., Dapagliflozin) GPR (G-protein receptors) Ultralong acting insulins (i.e., degludec) Ultralong acting GLP-1 (i.e., bydureon) New P-PARS
 Ultralong acting GLP-1 (i.e., bydureon) New P-PARS.")
57
Typical Type 2 Timeline Metformin at diagnosis Add something else
Consider insulin if: -Duration >5 years -A1C>9

58
Summary Diabetes is common Understand Medications and Indications
Type 1 diabetes: Insulin regimen (pumps) Type 2 diabetes: Lots of choices, but nearly all will need insulin eventually
 Type 2 diabetes: Lots of choices, but nearly all will need insulin eventually.")
59
Acknowledgements Jim Brosseau, M.D., M.P.H. Altru Diabetes Center
William Zaks, M.D., Ph.D., Altru Diabetes Center Altru Diabetes Center Team Melissa Gardner, Department of Family and Community Medicine, UNDSMHS

60
Contact Info/Slide Decks/Media Facebook search “North Dakota Diabetes” on Facebook Phone cell Slide Decks (Diabetes, Tobacco, other) iTunes Podcasts (Diabetes) (Free downloads) or iTunes>> search UND Medcast ( WebMD Page: (under construction) Diabetes e-columns (archived):
 iTunes Podcasts (Diabetes) (Free downloads) or iTunes>> search UND Medcast ( WebMD Page: (under construction) Diabetes e-columns (archived):")
61
Case Studies

62
Case Study 54 y/o white male
Diagnosed with type 2 diabetes after 2 fasting blood sugars of 154 and 142 Also has high blood pressure and cholesterol disease (common in type 2)
")
63
Case Study Metformin 500 mg prescribed twice daily, titrated to 1000mg BID ASA 81 mg daily Lisinopril 10 mg daily Simvistatin 40 mg daily Fish Oil 1000mg BID

64
Case Study Referred to Diabetes Educator and Dietician
Recommend developing graduated exercise plan (exercise prescription) Six months after diagnosis, A1C = 6.8% (target <7%)
 Six months after diagnosis, A1C = 6.8% (target <7%)")
65
Case Study Three years later, patient’s A1C has risen to 8.4% (target <7%) Blood pressure and cholesterol effectively treated Now what?

66
Case Study Choices include Any of these are good choices
Adding a basal insulin once daily Adding any other oral agent Adding exenatide twice daily or liraglutide once daily Any of these are good choices Choice may be made on individual factors

67
Case Study Patient chose additional oral agent (sitagliptin), but others would be OK A1C: 6 months later = 7.4% (target <7%) 3 years later = 8.1% (target <7%) Now what?
 Now what")
68
Case Study Sitgliptin, metformin continued
Basal insulin started with titration Eventually added bolus insulin with largest meal (90/10 rule) Likely will add bolus with other meals over time
 Likely will add bolus with other meals over time.")
Similar presentations


 HbA1c – IFFC (mmol/mol) 6.042 6.548 7.053 7.559 8.064 9.075.>")




. Who needs screening for DM? Age >45 Obese – BMI >25 1 st degree relative with DM Racial groups: –African American –Hispanic American.>")


>")








