Download presentation
Presentation is loading. Please wait.

1
Basic Fetal Monitoring
Southwest Washington Perinatal Education Consortium Intro self. Then ASK: How many of you have already been reading monitor strips in L&D? How many have been doing it for more than 2 or 3 months? How many are just starting to learn this month? This lecture is for all of you. Kathleen Murray, CNM, MN, RN

2
Objectives Identify the components of a fetal heart rate pattern: baseline, variability, accelerations, decelerations, periodic, and non-periodic changes Discuss maternal and fetal physiology and how it influences fetal heart rate patterns Differentiate criteria for reassuring and non-reassuring fetal heart rate patterns Today is fetal monitoring For some of you this class will feel like a helpful introduction, and you’ll be better prepared for the all-day fetal monitoring class you’re attending here (next class day, day 4). For those of you who have already been reading monitor strips for a while, this class will feel too easy and slow for you. I invite you to use the class to fill in any gaps in what you were taught, and to see if you’ve been doing it right!
. For those of you who have already been reading monitor strips for a while, this class will feel too easy and slow for you. I invite you to use the class to fill in any gaps in what you were taught, and to see if you’ve been doing it right!")
3
Fetal Heart Rate Monitoring Techniques
Auscultation Fetoscope Auscultation was the first method developed for listening to fetal heart, discussed more than 100 years ago, not used much in practice until the last 50 years. Still valuable for ongoing assessment during low-risk labors, and is used in out-of-hospital labors (home birth). Fetoscope, show demo if have one….developed in early 1900’s by Dr Hillis and Dr. DeLee (have you heard that name?). Is stethoscope with trumpet to amplify sound from abdomen, and uses bone conduction. Do any of you work on a unit that has one? If you ever work and the power goes out (big natural disaster, etc) you could use this. Sound is QUIET, like the muffled sound of a watch ticking.
. Fetoscope, show demo if have one….developed in early 1900’s by Dr Hillis and Dr. DeLee (have you heard that name ). Is stethoscope with trumpet to amplify sound from abdomen, and uses bone conduction. Do any of you work on a unit that has one If you ever work and the power goes out (big natural disaster, etc) you could use this. Sound is QUIET, like the muffled sound of a watch ticking.")
4
Auscultation Fetoscope Low tech Need quiet room

5
Auscultation Doppler Motion detector Portable
Some models are made for underwater use (in tub) Doppler small, portable, like a miniature monitor but only produces sound, no printout. Some of them calculate the average FHR for you and display it so you don’t have to count. Must be aimed at baby’s heart to get FHR. Some are made to immerse in water (pt in shower or tub). Do you know where the dopplers are kept on your unit? They cost about $500, so are often kept locked up, or mounted on IV pole so they don’t get stolen.
 Doppler small, portable, like a miniature monitor but only produces sound, no printout. Some of them calculate the average FHR for you and display it so you don’t have to count. Must be aimed at baby’s heart to get FHR. Some are made to immerse in water (pt in shower or tub). Do you know where the dopplers are kept on your unit They cost about $500, so are often kept locked up, or mounted on IV pole so they don’t get stolen.")
7
Doppler Doppler used throughout pregnancy and labor

8
Auscultation Benefits
Detects baseline FHR rhythm and dysrhythmias Hear changes in fetal heart rate Differentiates maternal from fetal heart rate What can the nurse do using auscultation? Count a baseline, just like when you take someone’s pulse; you hear abnormal rhythm’s better with doppler than with a monitor; You can hear increases, and decreases in the rate (we don’t chart them as accels and decels because we can’t measure them like a monitor does). Dopplers are a good way to find and be sure you are hearing baby, not mom. (move on to next slide without elaborating here).
. Dopplers are a good way to find and be sure you are hearing baby, not mom. (move on to next slide without elaborating here).")
9
Auscultation Limitations
Not continuous No printout or computer record Can’t demonstrate variability Requires some 1:1 nurse-time May be limited by position of mother Can hear good accels, but can’t chart whether variability is 0-5 bpm, or 6-25, etc. Would need to document audible “increases”, and lack of decreases, etc. Is a 1:1 skill, requires the nurse to attend only to this task for minutes at a time to assess FHR. Labor intensive in a way, although much appreciated by patient who doesn’t want to lie in a bed!

10
Fetal Heart Rate Monitoring Techniques
Electronic Fetal Monitoring External Internal EFM is standard, applied first. Involves 2 leads applied to maternal abdomen with 2 belts. Change to Internal lead for heart rate as needed. Now, Let’s focus on interpreting what we see on the monitor strip. (note, if they ask about Fetal Pulse Oximetry found to be unhelpful in changing outcome for neonate, removed from market in 2005 although was still being studied in centers in 2006.

11
Fetal Monitoring Strip
Point out features (FHR, UC pattern). Will come back and discuss variability, decels, what Ucs should look like, later. Some hospitals use paper, some record only on hard drive of computer, some use both. What do your hospitals use to record FHR strips? Strips have consecutive numbers to help match them up, identify with label or write with pen on each section. USA standard is to run paper speed at 3cm per minute, so that each dark line is one minute, each little section or box in between is 10 seconds. Paper is heat sensitive, marks are burnt on with hot needle, not ink. Paper hard to write on sometimes, but good place to jot down events for charting into notes later.
. Will come back and discuss variability, decels, what Ucs should look like, later. Some hospitals use paper, some record only on hard drive of computer, some use both. What do your hospitals use to record FHR strips Strips have consecutive numbers to help match them up, identify with label or write with pen on each section. USA standard is to run paper speed at 3cm per minute, so that each dark line is one minute, each little section or box in between is 10 seconds. Paper is heat sensitive, marks are burnt on with hot needle, not ink. Paper hard to write on sometimes, but good place to jot down events for charting into notes later.")
12
What’s the Purpose of Fetal Monitoring??? ASK them for their ideas?

13
Purpose of Electronic Fetal Monitoring
Identify reassuring signs of fetal well-being Screen for non-reassuring signs of a fetus who is at risk (Read slide) And, how are we doing? Rates of cerebral palsy, the usual source of lawsuits for birth injuries, have not gone down due to EFM. Partly because we found that CP is often caused during pregnancy, not during labor. EFM purpose was to screen for asphyxia and prevent neonatal morbidity or death, and to predict newborn condition. Monitoring has been studied along the way, rather than before being used, and the goals have changed. Usual policy at hospitals is 20 minute minimum EFM strip on admission to L&D. Then periodic or continuous after that. What would that depend on? Low vs. High risk status, patient request, MD or CNM orders, your hospital’s policy on monitoring. If patient refuses EFM, document that and need to offer doppler or fetoscope assessment. Will be 1:1 nursing care thru labor.
 And, how are we doing Rates of cerebral palsy, the usual source of lawsuits for birth injuries, have not gone down due to EFM. Partly because we found that CP is often caused during pregnancy, not during labor. EFM purpose was to screen for asphyxia and prevent neonatal morbidity or death, and to predict newborn condition. Monitoring has been studied along the way, rather than before being used, and the goals have changed. Usual policy at hospitals is 20 minute minimum EFM strip on admission to L&D. Then periodic or continuous after that. What would that depend on Low vs. High risk status, patient request, MD or CNM orders, your hospital’s policy on monitoring. If patient refuses EFM, document that and need to offer doppler or fetoscope assessment. Will be 1:1 nursing care thru labor.")
14
Benefits of External Fetal Monitoring (EFM)
Noninvasive Paper document Demonstrates variability Less labor intensive Paper readout helpful….85% of us are visual learners. It really helps to SEE the FHR. You will become aware of this when you try to describe a strip over the phone to the doctor or midwife, (about their patient). Often you end up faxing the strip, or having them come look at it! Paper document provides permanent record, but you should chart assuming your medical records dept will lose the strip, because more than 10% of strips go missing.
. Often you end up faxing the strip, or having them come look at it! Paper document provides permanent record, but you should chart assuming your medical records dept will lose the strip, because more than 10% of strips go missing.")
15
Limitations of EFM Restricts patient movement
Measures cardiac motion, is not ECG Doubling or half-count of FHR possible Might pick up maternal HR instead Learn to do EFM in various patient positions. Almost any position the mother can assume will allow for monitoring. We often place women in semi-fowler’s for our convenience, which causes what??? OP presentations! Since EFM uses ultrasound, works as motion detector, not like ECG…can’t always pick up dysrhythmias. Need to aim transducer directly at fetal chest or back. If computer can’t make sense out of a very slow or rapid HR, it may double or halve it…..if FHR is really 210, for instance , monitor might count as 105. (More about the fetal-demise- scenario in a later slide)
")
16
Internal Fetal Monitoring
Spiral electrode (FSE) provides direct ECG Measures interval between R waves Produces very accurate picture of FHR Hand out samples of FSE to handle
 provides direct ECG. Measures interval between R waves. Produces very accurate picture of FHR. Hand out samples of FSE to handle.")
17
Benefits of Internal Monitoring (Using FSE)
Accurate measure of FHR and variability May detect dysrhythmias Can allow for more patient movement Ask: what does FSE stand for? Fetal scalp electrode. Can see and hear abnormal fetal heart rhythms better. Mom, especially if very large woman, able to change positions often without losing the ‘aim’ at fetal heart.

18
Limitations of FSE Membranes must be ruptured to use Risk of infection
If fetus has died, may pick up maternal heart rate accidentally Once you rupture mom’s bag of waters, you :commit her to staying in hospital, you commit her to labor, you introduce risk of cord prolapse, and you introduce a real risk of infection to baby and mom thru uterus. If baby has died, the mother’s electrical charge (which is picked up by the wires in the electrode for ECG) will carry right thru the baby’s body. This is because the baby’s heart beat is not there to over-ride the signal from the mother. So, if you place a monitor (external, or internal) on a woman, you should verify fetal life first….thru use of comparison of maternal pulse with monitor reading, or feeling abdomen for fetal movement (or ultrasound).
 will carry right thru the baby’s body. This is because the baby’s heart beat is not there to over-ride the signal from the mother. So, if you place a monitor (external, or internal) on a woman, you should verify fetal life first….thru use of comparison of maternal pulse with monitor reading, or feeling abdomen for fetal movement (or ultrasound).")
19
Uterine Activity Monitoring
External: tocotransducer Detects frequency and length, not strength Requires palpation to assess strength of contractions The activity , or lack of it, of the uterus is important in evaluating labor/preterm labor/the ability of baby to tolerate stress/ etc. We always consider what the uterus is doing as part of the picture when considering the fetal heart pattern. Toco transducer has a button sticking out of it, placed firmly against mother’s fundus, when the uterus tightens, the button is pushed in, and this is translated onto strip , looks like a mountain. If belt too loose, or mom too heavy, or toco not placed well, Ucs can look weaker than they really are. AND if belt tight, can make little Ucs look very impressive.

20
Uterine Monitoring Note the normal-looking UC first
Then baseline rises and next few UC’s seem high (false) External UC monitor does not accurately show strength
 External UC monitor does not accurately show strength.")
21
External Uterine Monitoring
BENEFITS Noninvasive Provides documentation of UC frequency and duration LIMITATIONS Does not measure strength of contraction, nor resting tone of uterus Difficult to use in maternal obesity, in some positions

22
Monitoring With Internal Uterine Pressure Catheter (IUPC)
Accurate measure of uterine pressure Contraction strength, and resting tone Measured in mmHg Accurate timing of FHR changes in relation to UC’s If Available, PASS OUT samples of IUPC leads for nurses to handle at this point. Direct measure of uterine pressure from within, where the baby also feels the pressure, gives a sense of the forces of labor working in mother’s body and on baby’s body. Measured and compared against atmospheric pressure. Next ASK: when might you use IUPC on a patient? In what cases?

23
IUPC INDICATIONS External reading not adequate Labor dystocia
Fetal distress Amnioinfusion for cord compression RISKS Infection Uterine perforation Placental injury Extraovular placement If can’t assess contractions because external toco can’t pick up UC’s can be dangerous, especially if you are running pitocin. If labor stalled, IUPC helps you to know if is stalled because UC’s are painful but weak….can save a patient from Csection. Fetal distress might indicate the UC’s are stronger than you thought, and IUPC can accurately show what’s going on with the uterus. Amnioinfusion involves giving warm IV fluids thru hollow part of lead into uterine cavity to relieve pressure on cord. Used with oligohydramnios, etc (especially post-term). Used to be used to thin out meconium, not indicated for this, does not help prevent the baby from aspirating mec. It’s pretty hard to perforate a uterus with the lead because it bends, you’d have to mistakenly insert the rigid sleeve into the uterus. Extraovular means the lead slides under the membranes against the uterus, instead of into the amniotic sac to float next to the baby. If the lead goes under the placenta, it could cause an abruption. Placing IUPCs is often done by nurses, and you would want to have regular L&D experience for a while first, then be formally taught how to insert IUPC’s, so you will do it safely.
. Used to be used to thin out meconium, not indicated for this, does not help prevent the baby from aspirating mec. It’s pretty hard to perforate a uterus with the lead because it bends, you’d have to mistakenly insert the rigid sleeve into the uterus. Extraovular means the lead slides under the membranes against the uterus, instead of into the amniotic sac to float next to the baby. If the lead goes under the placenta, it could cause an abruption. Placing IUPCs is often done by nurses, and you would want to have regular L&D experience for a while first, then be formally taught how to insert IUPC’s, so you will do it safely.")
24
IUPC placement Point out picture on left showing lead tip floating in amniotic fluid, with great looking strip below. Then picture on the right with extraovular placement between uterus and sac, and abnormal reading on strip.

25
Are You Worried? ASK: How many of you are worried about being about to do: fetal monitoring? ASK for show of hands? Most nurses worry about this at first. Monitoring sounds complex/hard/risky/difficult to do, doesn’t it? Look at it this way. It’s a lot like learning to drive a car. Do you remember how nervous you were (or your parents were) when you were just starting to drive? There were a lot of safety rules to learn and remember, and you needed a lot of practice, you might have enjoyed the new skill but might have been worrried you were going to get killed, or hurt someone else if you made a mistake. But after some practice, the complex task of driving a car becomes second nature and now you do it daily with out even thinking much about it. Right? Well, learning to monitor mom’s and babies is a lot like that. It is very important to do it right, so no one gets hurt. But you will do it all day every day, and pretty soon you will have so much practice it will seem easy. You will get to the point you can monitor the baby, start an IV, coach the mom, answer dad’s questions, all at the same time!! Let’s take a 5 minute stretch break and we will talk about How To Read the Strips.
 when you were just starting to drive There were a lot of safety rules to learn and remember, and you needed a lot of practice, you might have enjoyed the new skill but might have been worrried you were going to get killed, or hurt someone else if you made a mistake. But after some practice, the complex task of driving a car becomes second nature and now you do it daily with out even thinking much about it. Right Well, learning to monitor mom’s and babies is a lot like that. It is very important to do it right, so no one gets hurt. But you will do it all day every day, and pretty soon you will have so much practice it will seem easy. You will get to the point you can monitor the baby, start an IV, coach the mom, answer dad’s questions, all at the same time!! Let’s take a 5 minute stretch break and we will talk about How To Read the Strips.")
26
Consecutive ID numbers see 91246 above
Date and time Label or write patient name every piece of strip, most facilities don’t want you to tear pieces off if can avoid… Vertical lines every 10 seconds, in US standard is to run at 3cm per minute Darker lines are every minute Horizontal lines are every 10 bpm for FHR and every 10 mmHg for UC’s

27
Up close view of same strip
Vertical lines every 10 seconds, in US standard is to run at 3cm per minute Darker lines are every minute Horizontal lines are every 10 bpm for FHR and every 10 mmHg for UC’s

28
Fetal Heart Rate Monitoring
Baseline, rounded up to nearest 5 bpm Variability Accels and Decels Periodic changes (with UC’s) Non-periodic changes (spontaneous) Briefly run thru this, will go into more detail next
 Non-periodic changes (spontaneous) Briefly run thru this, will go into more detail next.")
29
Fetal Heart Rate Monitoring
Baseline Normal: bpm Tachycardia : >160 bpm for >10 minutes Bradycardia: <110 bpm for >10 minutes Round to nearest 5. So, if FHR ranges between 140 and 150, you chart it as 145 bpm. Need at least 2 minute segment, in a 10 minute window, and not using portions containing accels or decels.

30
Strip shows baseline where? 130 to 140, I’d chart it as 135.
Variability present, point out beat to beat, small changes, as well as larger accels. No more detail than that at this time needed, will cover later.

31
Variability Characteristic of FHR baseline
Smoothness, or roughness of the line Very important characteristic of FHR, must be present for reassuring strip You want CHAOS in this rate….constant interaction between well-oxygenated brain and heart constantly responding to stresses and changing the rate to compensate. You’ve heard the term flat-line? Sounds bad, right? It is…you don’t want it in your baby. You CAN NOT have a good-looking strip without variability present. It is possible to have variability and still have a baby in trouble, although that is not common. But, generally, whenever variability is lost, unless to something like giving mom pain med, it is a sign of trouble for baby.

32
See previous slide. Point out differences between normal and diminished variability. Mention clear plastic tool some nurses use to ‘measure’ variability and accels. To decide if a pattern looks like random variability or mild decels, sometimes it is helpful to turn the strip upside down, with UC pattern on top and FHR on bottom, and look at it that way. Pattern becomes clearer if subtle decels. Also, to detect baseline change over the hours, take a long folded strip, hold it folded in your hand, look at edge….you can see the line of baseline FHR along the numerous folds of paper over the hours and easy to see if baseline rising.

33
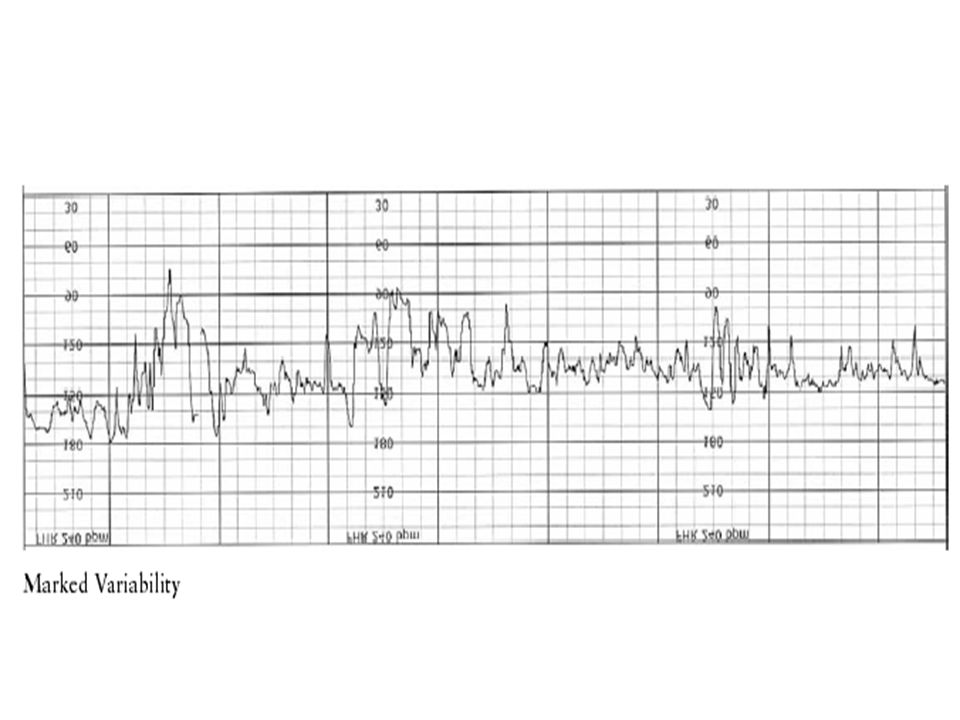
Variability Assessed in between UC’s and periodic changes
Absent: undetectable Minimal: 1-5 bpm amplitude Moderate: 6-25 bpm (normal) Marked: >25 bpm (also called saltatory) Might go back one slide and look at variability again and decide if normal amplitude.
 Marked: >25 bpm (also called saltatory) Might go back one slide and look at variability again and decide if normal amplitude.")
35
Causes of Decreased Variability
Non hypoxic causes Fetal sleep (20 min) Medications Tachycardia (such as from maternal fever) Fetal anomaly dysrhythmia Hypoxic causes Uteroplacental insufficiency Cord compression Mat. Hypotension Tachysystole Abruption Tachycardia Can a patient walk in the door of L&D with a flat strip? Yes….can be fetal hypoxia, mom maybe just had a cigarette, or needs IV hydration, or baby might be in sleep cycle. But, don’t wait an HOUR for things to look better….if you don’t see improvement within 10 minutes of intervening, you should be calling MD/CNM. You don’t know how long the baby has been this way, and things could get worse quickly.
 Medications. Tachycardia (such as from maternal fever) Fetal anomaly. dysrhythmia. Hypoxic causes. Uteroplacental insufficiency. Cord compression. Mat. Hypotension. Tachysystole. Abruption. Tachycardia. Can a patient walk in the door of L&D with a flat strip Yes….can be fetal hypoxia, mom maybe just had a cigarette, or needs IV hydration, or baby might be in sleep cycle. But, don’t wait an HOUR for things to look better….if you don’t see improvement within 10 minutes of intervening, you should be calling MD/CNM. You don’t know how long the baby has been this way, and things could get worse quickly.")
36
Interventions Determine cause Position change IV fluids
Oxygen 10 liters snug face mask Stop or turn down pitocin Place internal FSE Notify MD/CNM without delay Determine cause: if fetal sleep cycle, will be short lived. If caused by meds like fentanyl or other pain Rx, should have seen rapid change right after med took effect, and no decels or other concerning changes in FHR. Position change. Often this changes the picture. Look at mom…is she on her back!!?? IV fluids for rapid infusion if hypotension, bolus can also slow down UC’s a bit if that’s the problem. Go slower if patient has PIH etc. or fluid restrictions. And remember, IV fluids don’t carry oxygen! Notify provider unless you know benign cause like fetal sleep. Some providers deliver patients with loss of variability without waiting for decels to develop.

37
What is this?? Looks like normal to a new nurse sometimes, but is very dangerous pattern.

38
Sinusoidal Pattern Not to be confused with variability!!
Regular, sine-like wave pattern with amplitude of 5-15 bpm above and below baseline Ominous in most cases, requires prompt intervention, usually immediate C-section Usually caused by severe fetal anemia, can be from hypoxia, or briefly from narcotic dose You might go months or years before you see sinusoidal pattern, but it’s important to recognize it when it is there And take action to see that baby is rescued promptly. (back up one slide and show the pattern again) You wouldn’t start an induction, for instance, you’d get ready for a C-section.
 You wouldn’t start an induction, for instance, you’d get ready for a C-section.")
40
Causes of Increased Variability
Uteroplacental insufficiency or Cord Compression or Fetal Activity and A compensatory response to a mild hypoxic event Can be from harmful things like a bad placenta, or baby laying on cord, or from good things like a baby doing pilates or judo in the womb.

41
Interventions Determine cause Position change Assess fetal response
This pattern bears watching….may turn into decels next when baby has harder time compensating.

42
Accelerations Caused by sympathetic nervous system response to fetal movement or stimuli, normal and reassuring, rules out acidosis But, periodic accels, with UC’s are mild cord compression Stimuli that can create an accel are: Touching mom’s abdomen, voices or music, scalp stimulation Periodic accels with UC show baby trying to compensate for decreased O2 flow by increasing HR to get thru it. Can’t do this for long, decels will happen next if you don’t change something.

43
Bottom right strip shows spontaneous accels, occuring with fetal movement most likely. Wonderful strip. Upper left strip shows accels happening with UC, part of baby’s method of compensating for mild hypoxia. Probably cord compression, drop in fetal blood pressure from decreased blood reaching fetal heart, so baby increases heart rate, just like you or I would if our BP dropped. Note that with 2nd UC on strip, the initial accel is followed by a variable-looking decel.

44
Criteria for Accelerations
<32 weeks gestation, stays 10 beats above baseline for at least 10 seconds For > 32 weeks, acceleration stays 15 beats above baseline for at least 15 seconds

45
Base line 135, so they start measuring the accel on top at point where accel goes above baseline, and stop when it returns to base (although to me it looks like it only comes down to 140 there, so I don’t quite agree) 2nd example more clear, same 135 baseline

47
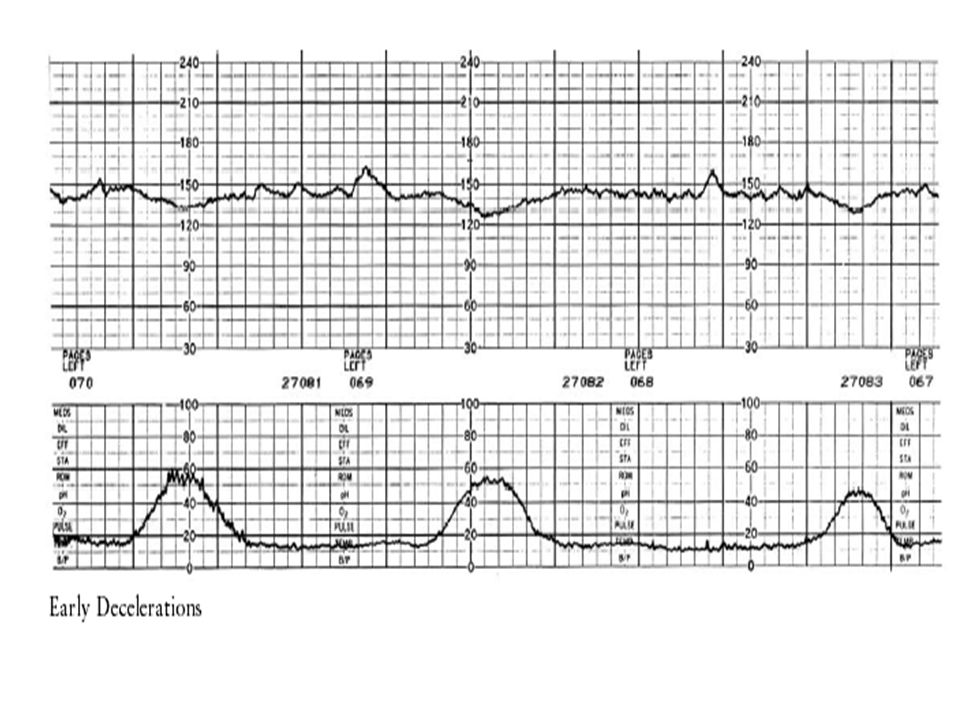
Early Decelerations Caused by pressure on fetal head, vagal response
Uniform, mirrors contraction Gradual onset, reaches nadir >30 sec. Reaches nadir at peak of UC, returns to baseline by the end of UC Benign Pressure on cranium from descent of head, intracranial pressure stimulates vagus nerve during UC when pressure peaks. Make sure decels are early, not LATE! Can change maternal position if OP position. If patient has Epidural, CHECK HER. Sometimes early decels tell you your mom went to 10 cm and baby coming down quickly!

49
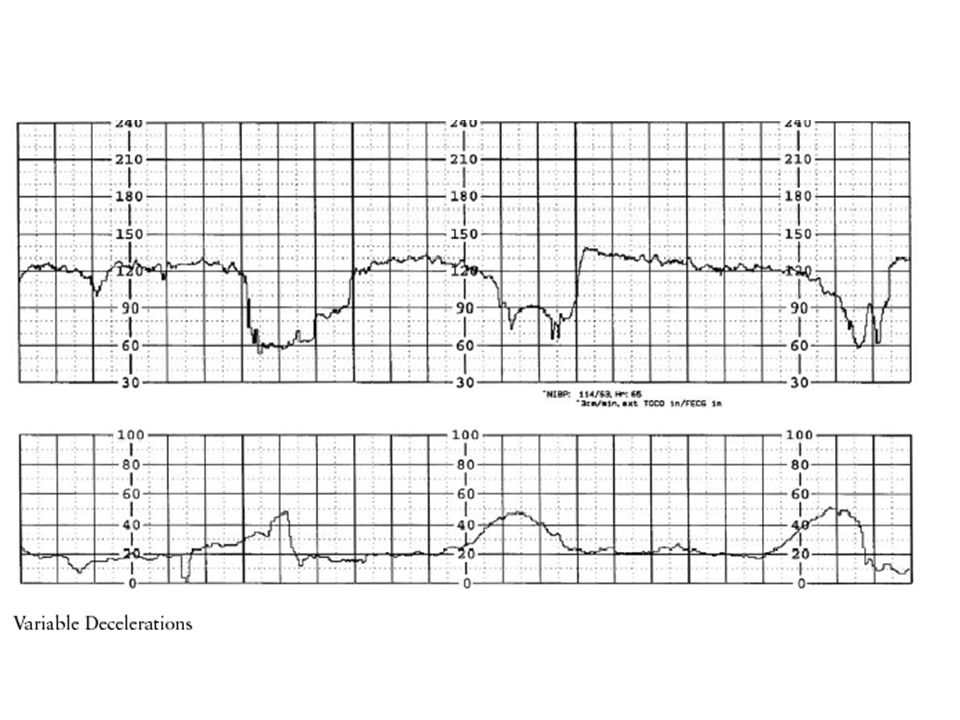
Variable Decelerations
Caused by cord compression, baroceptor response quickly slows FHR to compensate Abrupt onset, reaches nadir < 30 sec. Decel. Of >15 bpm lasting > 15 sec., and return to baseline < 2 minutes Usually occurs during contraction, cord pressed on by baby, or pulled tight around neck/ankle/arm or all 3. Baroreceptors in blood vessels sense stress and abruptly decrease HR so baby can use available O2 more slowly. As UC lets up pressure, HR bounds quickly back up. Some variables occur without UC’s, usually from fetal movement, or baby grabs cord and squeezes.

50
Example of 3 dips in FHR. Do they count as variable decelerations?
# 1 decels more than 15 bpm below baseline (130), but only lasts 10 seconds. So, no. #2 same thing. #3, however, decels more than 15 bpm, and lasts 15 seconds from beginning to recovery so yes.
, but only lasts 10 seconds. So, no. #2 same thing. #3, however, decels more than 15 bpm, and lasts 15 seconds from beginning to recovery so yes.")
51
Causes of Variable Decelerations
Intrauterine Nuchal cord, or body entanglement Oligohydramnios Rupture of membranes Short cord or true knot Occult prolapse of cord Maternal conditions Positioning Second stage labor with descent Monoamniotic multiple gestation

53
Variable Decel. Characteristics
Shape, depth, and duration vary (not uniform), can be V, W, U shaped Timing may vary Watch for fetal compromise increasing baseline loss of variability slow return to baseline Watch, make sure baby still tolerates the decels well. If can’t compensate, will lose the other reassuring features.
, can be V, W, U shaped. Timing may vary. Watch for fetal compromise. increasing baseline. loss of variability. slow return to baseline. Watch, make sure baby still tolerates the decels well. If can’t compensate, will lose the other reassuring features.")
54
Interventions Vag. Exam rule out prolapse Position change IV fluids
Oxygen 10 l/mask Turn pit off or down Assess fetal response Call MD/CNM Same list as with late decels, except added vag exam, and If ordered, start amnioinfusion Your goal is to relieve the cord. Might need to try multiple things. Amnioinfusion is warm IV fluid thru IUPC into amniotic sac around baby to relieve pressure on cord, often works within minutes if low fluid volume is the cause. Need order from MD or CNM to do it.

55
Late Decelerations Caused by uteroplacental insufficiency
Fetus runs low on oxygen during a UC Maternal, placental, or fetal cause of inadequate oxygen to fetal heart Often indicates metabolic acidosis Needs urgent response Lates are never reassuring, always require a response, and are sometimes a fast ticket to a C-’Section

57
Late Decel. Characteristics
Always associated with a UC, with delay in timing Gradual decrease from baseline to nadir >30 seconds Nadir occurs after peak of UC Depth of decel usually only 5-30 bpm Late is caused by a UC, if you see what looks like a late decel on your strip , and no UC, you might not be picking up contractions on your monitor, palpate and adjust your lead and look for UC’s (and, ask the patient!). Ask her about “tightening” of her belly…she may be having painless UC’s that she hasn’t complained about, but they might be strong enough to decompensate the baby. Decels often recover just after the end of the UC. The late timing of the nadir is the key. If it’s hard to see whether you have a late or not, try turning your strip upside down with FHR on bottom and Ucs on top…often becomes clearer when viewed this way. Another way to describe repetitive late decels is they look like birds in flight, in a row, with wingtips touching. And the one wing to the right of each bird often looks lower than the other, because recovery from the decel is often slower than onset See example.
. Ask her about tightening of her belly…she may be having painless UC’s that she hasn’t complained about, but they might be strong enough to decompensate the baby. Decels often recover just after the end of the UC. The late timing of the nadir is the key. If it’s hard to see whether you have a late or not, try turning your strip upside down with FHR on bottom and Ucs on top…often becomes clearer when viewed this way. Another way to describe repetitive late decels is they look like birds in flight, in a row, with wingtips touching. And the one wing to the right of each bird often looks lower than the other, because recovery from the decel is often slower than onset. See example.")
58
Interventions Lateral position, (usually left works best)
Increase IV fluids Oxygen 10 l/mask Stop pitocin Call MD/CNM Determine cause, and correct if possible Assess fetal response Prepare for possible delivery Your goal is to improve oxygen transfer to the fetus. ASK: why turn mom to her left side? Why bolus IV? Because increased in fluid volume sometimes slows UC pattern down briefly. Oxygen by tight face mask. Pitocin is either causing, or worsening the condition that is responsible for the lates, so don’t just turn it down!!!. Be clear on phone the type of decel. Depth is not important. A late decel of 5-10 bpm means the same thing as a deeper late decel.

59
Prolonged deceleration
Deceleration of >15bpm, lasting more than 2 minutes, less than 10 minutes Measured from onset until return to baseline Often is long, exaggerated variable Cause often: cord compression, or tachysystole, or maternal hypotension The majority of long decels like this are cord events (root cause is same as variable, just a more serious event.

60
Let’s count how long this decel lasts
Let’s count how long this decel lasts. Assuming the first 30 seconds we see of the strip is true baseline, we get what? bpm. Then, decel starts, reaches nadir at 2 minutes 30 seconds. Returns to baseline abruptly 20 seconds later. The abrupt recovery strongly suggests a cord event…baby leaned on, pulled on cord, or the force of the UC might have made too much stretch on cord if nuchal and baby is starting to descend. You chart the decel as 2min50 seconds, with nadir of 60’s. Note the overshoot at recovery, as baby’s adrenaline finally got a chance to stimulate the HR. Probably the mom moved (or was moved by the nurse), or the baby moved, and relieved pressure on the cord. Mild decel a minute later, and increased baseline of This baby is stressed, and needs recovery time at this point. Consider turning pitocin off or down to help baby resuscitate. And of couse, who have you notified about the prolonged decel?? Answer is doctor/cnm.
, or the baby moved, and relieved pressure on the cord. Mild decel a minute later, and increased baseline of 140. This baby is stressed, and needs recovery time at this point. Consider turning pitocin off or down to help baby resuscitate. And of couse, who have you notified about the prolonged decel Answer is doctor/cnm.")
61
Hint: Same List As for lates
Interventions Without Looking at Your Notes, Tell Me What You’d Do for a Prolonged Decel? Hint: Same List As for lates

62
Interventions Lateral position Increase IV fluids Oxygen 10 l/mask
Stop pitocin Call MD/CNM Determine cause, and correct Assess fetal response Prepare for possible delivery, moving into O.R. by 3rd minute if not resolving Your goal is to improve uteroplacental blood flow, perfusion of oxygen thru cord Call MD or midwife, usually by 2 minutes into the decel. No need to wait more minutes to decide to call.

63
Uterine Contractions What do you need to know about a patient’s contractions? ASK for ideas.

64
Contraction Monitoring
Interval “how far apart are they?” Duration “how long do they last?” Resting tone: how does the uterus feel between contractions Intensity “how hard are they?” mild moderate strong Measure Ucs from beginning of one, to start of next one. Might need to palpate if tracing not clear. Measure in units of 10 seconds. Resting tone is either soft, or rigid, by palpation. (or else in mmHg by IUPC). Intensity is mild, feels on palpation like your lips Moderate, feels like the end of your nose Strong feels like your forehead.
. Intensity is mild, feels on palpation like your lips. Moderate, feels like the end of your nose. Strong feels like your forehead.")
65
Point out the Ucs on this strip and how to document them.
Normal Ucs are q 2-3 minutes in active labor, lasting seconds, relaxed uterus in between. With IUPC, want peaks for progress, and resting tone 15-20mmHg.

66
Electronic Fetal Monitoring
Strip Interpretation

67
Systematic Review of strip
Baseline Normal is ___________ Variability Expressed as _________ Accelerations Present, or absent Decelerations Present, or absent 3 major types: ________________ Contraction pattern To evaluate a strip, use these steps. Normal baseline Variability is : absent, minimal, normal, marked. Decels are: early, variable, and lates.

68
Begin…. By looking at what is reassuring on the strip
Then, note any concerning features

69
What would you chart about this strip?
Is it reassuring? Why? Normal baseline, not changed from earlier as far as we know, variability moderate (normal) presence of spontaneous, non-periodic accels, which rules out acidosis absence of decels would need to palpate to say whether pt is having UC’s or not
 presence of spontaneous, non-periodic accels, which rules out acidosis. absence of decels. would need to palpate to say whether pt is having UC’s or not.")
70
How would you describe this strip?
Abnormal baseline of 205. Tachycardia. Minimal variability. Severe variable decels Abrupt decel in less than 30 seconds, abrupt recovery to baseline Nadir in 70’s The shape and rapid changes in the decel tell us these are variables, not lates or early’s, even though we don’t have a UC tracing to compare to. What do you think the fetal oxygen reserve is at this point? Such a high heart rate, deep decels…. This baby probably needs urgent delivery.

71
Documentation Critical job for you, your hospital, the patient
Chart as if the hard copy of your strip will get lost later…10% or more of all strips do Clear, concise language Institution-specific Standards of care Your charting should be able to basically re-create the major features of the monitor strip. Even if your hospital uses computer drive storage of the data, we all know what can happen with computers. Your words should be specific, detailed, consistent…..your charting should paint a picture of the strip.

72
Documentation on the strip
Label/write patient name, date etc. Events, actions, nursing interventions Calls to MD, CNM, nursery, etc. What not to write on strip Label each piece of strip if torn off to chart. Write down what??? Medications, VS, vag exam results, when ROM occurs, position changes, change to internal or external leads, Epidural events, care such as IV start, Oxygen placed. Phone calls to providers, etc. Never put on strip something like “Dr S grumpy and refused to leave office now”, however, do put in your nursing notes that you called Dr S, what info you covered during phone call, whether you specifically asked Dr to come now, exactly what the response to you was, and your actions to go up chain-of-command if indicated.

73
Auscultation documentation
Rate Rhythm (regular, irregular) Increases in rate (audible accels) Decreases (audible decels, and the timing)
 Increases in rate (audible accels) Decreases (audible decels, and the timing)")
74
FHR Documentation Intervals
Auscultation or EFM Low risk patient: Active labor every 30 minutes 2nd stage every 15 minutes High risk patient Active labor every 15 minutes 2nd stage every 5 minutes This means, if you are using doppler on low risk patient, you need to listen thru and after a UC, to rule out lates and variables, and listen for presence of accels, and stable baseline. If using EFM, you need to confirm that it is picking up heart rate well, and need to stop and look at strip and evaluate it that often. For high risk patients, usually doppler not considered adequate, and continuous monitoring is standard. So, you might not have perfect readout during all pushes with external, but need to be able to confidently evaluate all aspects of FHR for a period of time every 5 minutes.

75
If Confusing Pattern Complex patterns, combination of 2 types of decelerations sometimes exist Focus on: baseline stable or not, variability and accels, whether decels are periodic or not, timing related to UC’s, abruptness of change from baseline Sometimes helps to draw decel in your chart notes For example, and IUGR baby, who also has a true knot in his cord. IUGR, with poor placental function, will contribute to what kind of decel? Late. If the baby starts to descend and pulls on his cord, tightening the knot, what kind of decel does that produce? Variable. So, you could see an abrupt variable decel, with a delayed slow return to baseline (late component). Even if the variables are not very deep, the late component of the decel signals that the baby might be unable to tolerate the contractions.
. Even if the variables are not very deep, the late component of the decel signals that the baby might be unable to tolerate the contractions.")
76
Documenting Uterine Activity
What four characteristics do you note? ____________________ Interval Intensity Duration Resting tone

77
An example of a strip. What would you chart for this strip?

78
Example of Charting 2100-FHR baseline 130, accels to 160 present, no decels. UC’s q 2.5 minutes x seconds, palpate moderate, resting tone soft K Jones, RN

79
Non-reassuring FHR Patterns
Document the following: Pattern Nursing intervention Evaluation of response Notification of MD or CNM

80
What would you chart about this strip?
Tachycardia Baseline high , 170 Minimal variability No accels No decels Ucs q 2-3 minutes If this is IUPC the resting tone is too high, and the peaks of Ucs so low she is not going to dilate well with these UC’s. Needs delivery.

81
Example of Charting 2120- FHR 170, minimal variability, no accels, no decels. UC’s q minutes x seconds, peaks 40-50mmHg, resting tone 25. Positioned Left-lateral, O2 on 10 l per tight mask, pitocin turned off, IV rate increased. No change in FHR pattern. Phoned Dr James with report of non-reassuring strip and asked him to come now to evaluate. He stated he is on his way. Explained to patient and husband. K Jones, RN The variability in the final 3 minutes on example strip is essentially absent. (Back up and show previous slide if needed)_ Ucs are not too close, but they’re lasting too long. IUPC show’s abnormal resting tone, baby and uterus are not getting recovery time.
_. Ucs are not too close, but they’re lasting too long. IUPC show’s abnormal resting tone, baby and uterus are not getting recovery time.")
82
Conclusion Methods of fetal monitoring
Components of FHR, and uterine activity Causes of various changes Nursing interventions Systematic review of strip Documentation Discussed ways to monitor baby and mom, why we do it, benefits and risks of various methods. Components, such as accels, decels. ASK: what is one of the single most important components that tells you if your strip is probably reassuring? One of the first things to be lost when baby hypoxic? Variability!! You will become more skilled and comfortable with monitoring as you practice it. You will find helpful texts, websites, classes, and computer programs that will help you become expert over time. Some of these sources are listed in the reference page. Ask the charge nurses on your unit for sources within your facility, as well.

83
References Abcdefm:electronic fetal monitoring , Curran, Carol, and Torgersen, Keiko, Colley Avenue Copies & Graphics, Virginia Beach, VA, 2006, pp.31,158-9, 167,169,170,178-9. Fetal Heart Monitoring Principles & Practices 4th ed., Lyndon, Audrey et al editors, AWHONN, Kendall/Hunt, Dubuque, Iowa, 2003. NCC Monograph, Vol 2, No. 1, 2006, National Certification Corporation, pages 6-11.

Similar presentations






 Part 2 – Electronic Fetal Monitoring*>")














 Electronic Fetal Monitoring – use of instruments.>")

