Download presentation
Presentation is loading. Please wait.

1
Whole system working in Cheshire and Merseyside Melanie Sirotkin –Centre Director, PHE Fiona Johnstone –Director of Public Health, Policy & Performance, Wirral Council and Chair of Champs

2
Nine local authorities covering a population of 2.4 million people

3
Cheshire and Merseyside System
Cheshire & Merseyside Public Health England Centre Voluntary & Independent Sector Health & Wellbeing Board 2 x NHS England Area Teams 12 x CCGs 9 Local Authorities – supported by CHAMPs Network

4
What’s it like out there? – Wider determinants
Deprivation – 5/9 authorities in the most deprived quintile. Child poverty and older people in deprivation is worse than the England average. Unemployment - higher than England average in 6/9 authorities (2011/12). Income - average weekly pay is lower than the England average in 8/9 authorities. Index of Deprivation, 2010, %, Cheshire & Merseyside (comparing to England average)
. Income - average weekly pay is lower than the England average in 8/9 authorities. Index of Deprivation, 2010, %, Cheshire & Merseyside (comparing to England average)")
5
What’s it like out there? (PHOF)*
Life expectancy in both males and females is lower in most (8/9) local authorities. Higher preventable mortality (liver disease, CVD, cancer) Similar or better – health check offer but poorer health check take up. Rates of low birth weight better than or similar to. Lower breast feeding rates. Teenage conceptions lower or similar in 6/9 authorities. Excess weight in year olds worse than or similar to (most authorities). Similar levels of physical activity. Similar or less smoking in routine and manual groups. Successful completion of drug treatment (opiate and non opiates –similar or better) Good coverage MMR, HPV and flu (at risk). Higher rates of injuries due to falls. Emergency re-admissions within 30days of discharge from hospital is worse than England average *Compared to England average
 local authorities. Higher preventable mortality (liver disease, CVD, cancer) Similar or better – health check offer but poorer health check take up. Rates of low birth weight better than or similar to. Lower breast feeding rates. Teenage conceptions lower or similar in 6/9 authorities. Excess weight in year olds worse than or similar to (most authorities). Similar levels of physical activity. Similar or less smoking in routine and manual groups. Successful completion of drug treatment (opiate and non opiates –similar or better) Good coverage MMR, HPV and flu (at risk). Higher rates of injuries due to falls. Emergency re-admissions within 30days of discharge from hospital is worse than England average. *Compared to England average.")
6
Health & Care Indicators
Health and care indicators, 2011, %, Cheshire & Merseyside (comparing to England average)
")
7
What’s it like out there – North West mental health and wellbeing survey - key findings
All nine local authority areas within Cheshire and Merseyside (C&M) participated in the 2012/13 North West survey. The WEMWBS scores varied in significance for the 9 local authorities with 2 showing an improvement between 2012/13 and 2009. Overall 15.3% of respondents had ‘low’ mental wellbeing, 64.1% had ‘moderate’ and 20.6% had ‘high’ mental wellbeing. This varied widely across the nine local areas. The mean life satisfaction score for Cheshire and Merseyside was significantly higher than the North West mean. Source: North West Mental Health and Wellbeing Survey 2012/13
 participated in the 2012/13 North West survey. The WEMWBS scores varied in significance for the 9 local authorities with 2 showing an improvement between 2012/13 and Overall 15.3% of respondents had ‘low’ mental wellbeing, 64.1% had ‘moderate’ and 20.6% had ‘high’ mental wellbeing. This varied widely across the nine local areas. The mean life satisfaction score for Cheshire and Merseyside was significantly higher than the North West mean. Source: North West Mental Health and Wellbeing Survey 2012/13.")
8
What’s it like out there?
Strong traditions of music, arts, culture and sport rich heritage – castles, parks, historic building Vibrant voluntary sector – Change up consortium in Greater Merseyside working with 18 organisations and investing in voluntary, community and faith groups

9
Top 5 priorities from the Local Health and Wellbeing Board Strategies
Mental Wellbeing Children Alcohol Older people Sustainable places

10
Champs public health collaborative service
Led by the 9 Cheshire and Merseyside local authority Directors of Public Health, facilitated by a support team. Owned and delivered by our local public health teams. Generates efficiencies and improves service quality and outcomes. It does this across four key areas: Improving commissioning Advising the NHS Protecting health Leading public health

11
Key successes Mental health Behaviour change Sector led improvement
Asset based approaches Mental health champions Suicide prevention Behaviour change PHE mental wellbeing pilot Breastmilk It’s Amazing campaign Pharmacies campaigns Sector led improvement Health Checks review National Child Measurement Programme review Sexual Health review

12
Healthy places An innovative large scale change programme. A fresh approach to working with our commercial, public and 3rd sector partners. Our aim is to support communities to create their own healthy places to live. Ultimately, it’s about prevention and reducing reliance on services.

13
Shaping healthy places
CW&C – the journey so far Caryn Cox – Director of Public Health Cheshire West and Chester Council

14
The background Wholesale changes to healthy system
Public health moved into the local authority Planners unsure of how to engage with ‘health’ Raft of guidance and evidence already out there Public health - no understanding of where health fitted into existing planning processes

15
Getting started and the baseline
Established links with planners – strategic/spatial and development control Public health hosted and facilitated a meeting CCGs x 2 CSU – Cheshire and Merseyside Local authority planners NHS England NHS PropCo Public Health England Commissioned health planners to audit existing processes and recent planning applications to understand baseline “Better Health Outcomes Through Spatial Planning”

16
The journey continues Local development framework consultation – significant PH submission and all key stakeholders also submitted Agreement to develop a Supplementary Planning Document (SPD) as part of the Local Plan on Health and Wellbeing Preparing evidence for the Community Infrastructure Levy (CIL) All significant planning applications pass through Public Health Active member of SPAHG (Spatial Planning and Health Group) and strong links with WHO at UWE Housing links – local authority and RSLs Healthy Places – new key area for ChaMPS
 as part of the Local Plan on Health and Wellbeing. Preparing evidence for the Community Infrastructure Levy (CIL) All significant planning applications pass through Public Health. Active member of SPAHG (Spatial Planning and Health Group) and strong links with WHO at UWE. Housing links – local authority and RSLs. Healthy Places – new key area for ChaMPS.")
18
Cheshire & Merseyside PHE (North West KIT)
Key Assets for Recovery Tom Hennell Friday 4th April 2014

21
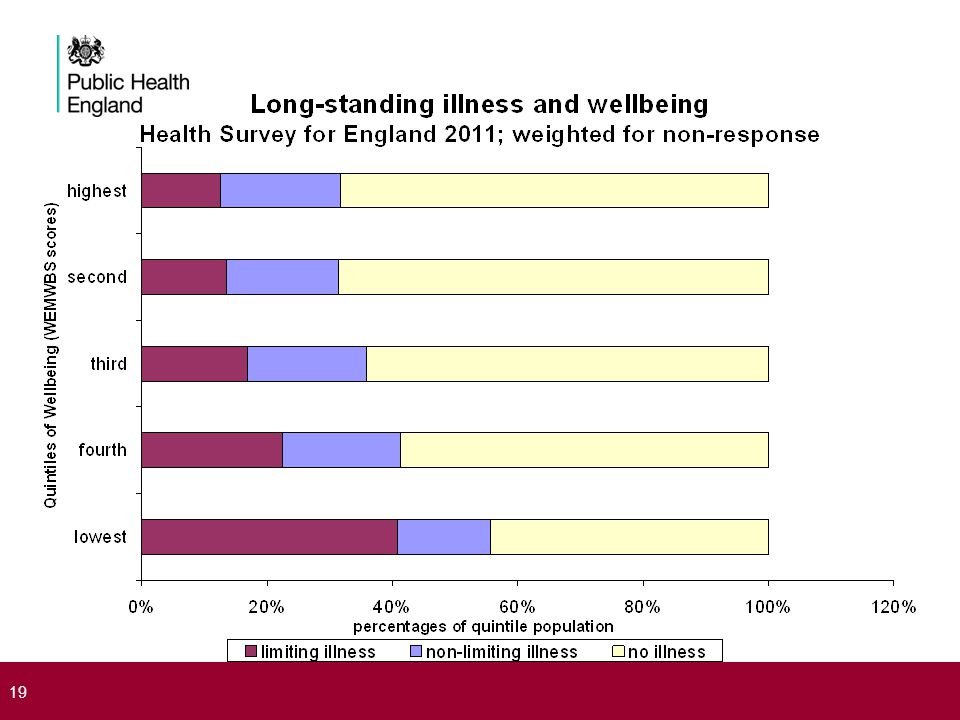
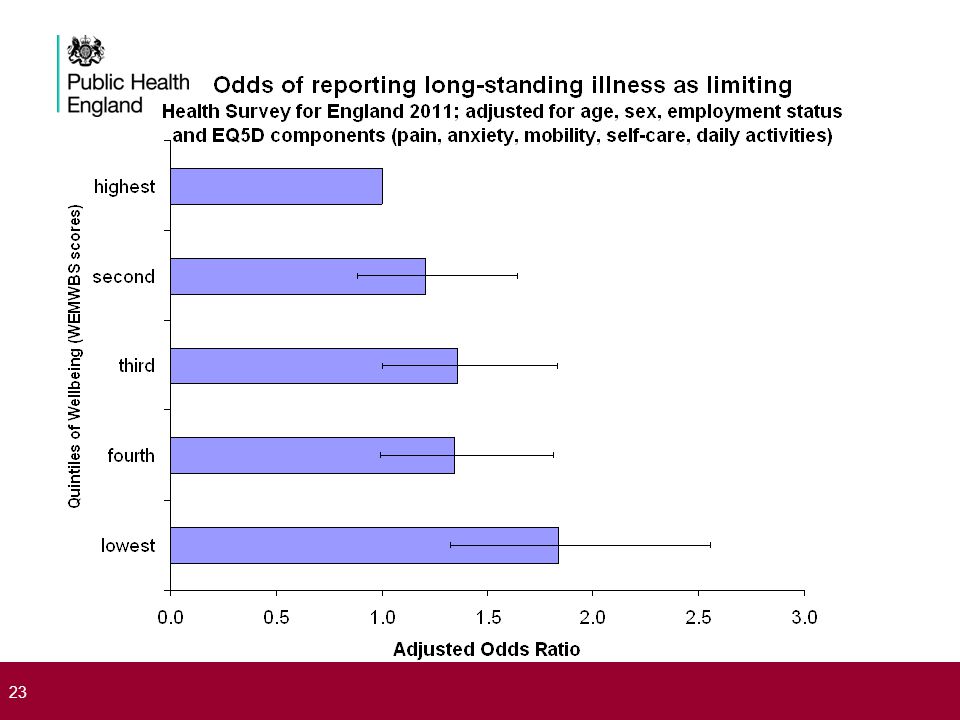
Observations on long-standing illnesses from population surveys
Long-standing conditions characteristically progress from being ‘limiting’ to being ‘non-limiting’. The proportion of persons reporting a long-standing condition, and experiencing it as non-limiting/limiting, is an indicator or recovery/non-recovery. Higher levels of positive wellbeing are associated with lower levels of limiting long-standing illness; through increased capability at ‘getting ill better’.

24
Two agendas for Public Health
‘Getting ill less’: interventions aimed at reducing incidence of illness, through reducing exposure to avoidable health risks. ‘Getting ill better’: Interventions aimed at earlier recognition of illness, and reducing inhibitions against becoming ill. Interventions aimed at reducing duration and recurrence of illness, through improving access to recovery assets; and reducing inhibitions against recovery.

26
Proposed ‘characteristics of recovery’
derived from reported experience of recovering persons; together with analyses of self-reported limiting long-term illness in Health Survey for England and British Household Panel Survey. (see Bartley et al. JECH 2004; 58, ) Recovery is: Universal; everyone is potentially able to recover, given access to recovery assets, and non-exposure to inhibitions, Non-clinical; recovery is to be distinguished from discharge from clinical treatment or long-term condition management, Transformational; recovery is conditional on acquiring the capability to change social context, such that the condition does not recur, Communicable; recovery is best achieved when co-produced within a community of recovering persons, supporting practitioners and reciprocal social partners. Presentation title - edit in Header and Footer
 Recovery is: Universal; everyone is potentially able to recover, given access to recovery assets, and non-exposure to inhibitions, Non-clinical; recovery is to be distinguished from discharge from clinical treatment or long-term condition management, Transformational; recovery is conditional on acquiring the capability to change social context, such that the condition does not recur, Communicable; recovery is best achieved when co-produced within a community of recovering persons, supporting practitioners and reciprocal social partners. Presentation title - edit in Header and Footer.")
27
Jobs, Homes, Friends Employment and Job Security
Being able to retain employed status while recovering; together with flexibility and capability for adjusting employment conditions to support recovery and reduce risk of recurrence. Housing and Financial Security Having access to secure and sufficient housing to support recovery; allied to assurance of sufficient financial resource (especially including access to benefit income) for housing to be sustainable without creating or exacerbating problems of debt. Wider Social Engagement and Shared Recreation Specifically, having access to mutual support from other recovering persons – as in ‘recovery communities’; but more widely in regular, non-work, engagement with friends and local neighbours outside of the immediate household, offering trust and being trusted.
 for housing to be sustainable without creating or exacerbating problems of debt. Wider Social Engagement and Shared Recreation. Specifically, having access to mutual support from other recovering persons – as in ‘recovery communities’; but more widely in regular, non-work, engagement with friends and local neighbours outside of the immediate household, offering trust and being trusted.")
28
Supporting local decision-making - the i-hit tool - Clare Perkins and Matt Hennessey Knowledge and Intelligence Team (North West)
")
29
i-hit Originally developed by the former North West Public Health Observatory, with Liverpool John Moores University, to support Salford PCT/LA and their partners in understanding where to invest to achieve maximum gain in life expectancy Salford wanted to develop a model that would predict the effect on life expectancy of improving key determinants of health, through investment in effective public health interventions. To better understand the ‘causes of causes’ and to identify priorities for multi-agency investment i-hit models statistical associations between indicators in the health profiles, using Bayesian mathematical methods and conditional independence algorithms, and quantifies the scale of change needed across all the health indicators to achieve ambitions for life expectancy The tool demonstrates that to achieve sustained health improvement, effort is needed across the spectrum of determinants of health Engaging with Health and Wellbeing Boards and Wider Partners; the i-hit tool

30
Engaging with Health and Wellbeing Boards and Wider Partners; the i-hit tool

32
Scenario: What is the scale of change needed to improve life expectancy for men by 2 years?
Engaging with Health and Wellbeing Boards and Wider Partners; the i-hit tool

33
Scenario: What is the scale of change observed if we reduced adult smoking in Salford to the national average? Note the effect on child poverty and wider social determinants Engaging with Health and Wellbeing Boards and Wider Partners; the i-hit tool

34
Scenario: What is the scale of change observed if GCSE attainment equalled the current national average? Note that life expectancy (males) would increase by over 4% and unemployment would be down by nearly 60% Engaging with Health and Wellbeing Boards and Wider Partners; the i-hit tool

35
Next steps for i-hit Stage 1 (in progress)
Refresh with recent data from Public Health Outcomes Framework and produce new map Increase map interactivity Scale up the tool for piloting across North West Local Authorities and Health and Wellbeing Boards Stage 2 Model impact for different geographies Develop functionality to be able to: ‘fix’ indicators in the tool model changes in multiple indicators ‘on the fly’ Engaging with Health and Wellbeing Boards and Wider Partners; the i-hit tool

36
Impact of i-hit in Salford
The tool was used in Salford to develop a long list of priorities and to consider the scale of the challenge It increased the Board’s focus on social determinants of health which became one of the key priorities It strengthened wider stakeholder engagement in considering inter- relationships of factors e.g. smoking and child poverty, violent crime and life expectancy Shaped the scale of challenge – creating more realistic scaled challenges for the first three years of the strategy alongside aspiration for long term goals Engaging with Health and Wellbeing Boards and Wider Partners; the i-hit tool

37
Local first Forthcoming National tools to support the local systems:
National conversation on Health inequalities Health and Wellbeing Framework for England and menu of interventions Alcohol licencing support pack Forthcoming NoE/Centre tools to support the local system: PHOF summary tool Health Equity North Horizon scanning for emerging issues Child health resource pack Working with NHS England to identify local data requirements

38
Dr Janet Atherton Director of Public Health
Wellbeing Sefton Dr Janet Atherton Director of Public Health

39
Sefton’s Award Winning Arts on Prescription Programme for adults with mild to moderate depression, stress or anxiety

40
Creativity flourishes in Sefton
Seed- ‘Arts & Health pilot’ in 2005 Roots- ‘Invest to Save’ three year funding Shoots- Weekly workshops in four locations NHS Sefton/Council joint funding Fruits- Creative Alternatives as a jewel of The Atkinson Centre- ‘Sefton’s Centre for Wellbeing through Culture &Creativity’

41
Rooted & growing in Sefton
Labyrinths Mazes Heritage walks Exhibitions Creativity with vulnerable groups Go with the Flow Volunteering

42
The Impact? The Data Case Study: Joanne’s Story Wellbeing
78% improvement in mental wellbeing SWEMWEBS measure 3.5 point shift from low to medium wellbeing Lifestyle improvements Physical activity 66% Diet 36% Increased social activity 68% Smoking cessation 29% Alcohol reduction 32% Reduced medication 32% GP visits reduced 34% Social Return on Investment £6.95 for every £1 invested £6.95 for every £1 of expenditure I have struggled with anxiety since I was fourteen but never found effective help. For me Creative Alternatives was a final attempt. At Creative Alternatives no one judged me, problems were shared and I have formed some special friendships. I have done many things through the programme which I never would have thought possible – they have encouraged me out of my comfort zone. Creative Alternatives has really increased my confidence in travelling to different places. Since leaving the programme I have been doing voluntary work. This was a big achievement for me as I had not worked for nine years as a result of anxiety. I loved seeing what a difference I could make to other people. I have halved my medication and now feel more in control of my anxiety, it doesn’t stop me from doing things as much as it used to, now I am living my life instead of just existing.

43
Sefton results: 5 point improvement on a 35 point scale from 20 to 25
Moving from low wellbeing to moderate wellbeing 43

44
Promote Prevent Recover
SEAS- Sefton Emotional Achievement Service delivered in Sefton schools Wellbeing Sefton- a collaborative of social prescribing providers targeting adults with low wellbeing Recovery College- an approach by Mersey Care enhancing the talents, skills and resources of service users to support their own recovery

45
Community Wellbeing Building community resilience Community asset development in 3 localities: ‘Fair Deal’ five ways to wellbeing kit utilised for community engagement Integrated Wellness Service- a holistic approach to individual and community wellbeing Green infrastructure for wellbeing Healthy Streets

46
Champs Mental Wellbeing Programme
Commissioning for mental wellbeing outcomes Brief Intervention Integrated Wellness Services Social Prescribing Leadership & Workforce Development Public awareness- PHE marketing Five Ways PH role in reducing burden of mental illness Mitigating the impact of welfare reform 46 46

47
Steps to flourishing Vision & drive Opportunities seized Creativity
Partnerships Evidence Influence ££ ?

48
Public Health Approach to addressing Domestic Abuse in Knowsley
Matthew Ashton Director of Public Health Knowsley MBC

49
Overview Background Process Key findings Political scrutiny
Scrutiny Recommendations Key messages

50
Background Domestic abuse is a significant public health issue, having a major impact upon those directly affected and their families. Locally, it had been raised as a issue at the Safeguarding Children’s Board and through the wider Knowsley Partnership. Previous needs assessments (and consequently services) developed from a Community Safety perspective. Need for new needs assessment from health perspective
 developed from a Community Safety perspective. Need for new needs assessment from health perspective.")
51
In Knowsley 1 in 3 females smoke
1 In 3 females suffer from domestic abuse 1 in 8 females have Cardiovascular Disease (CVD) – Heart disease and strokes 1 in 9 females drink alcohol at increasing & high risk levels 1 in 15 females have coronary heart disease (CHD) (source: Life style survey 2012) (source: Crime Survey for England & Wales 2012) - modelled estimates (source: Life style survey 2012) – modelled estimates 1 in 61 people have Cancer (source: QOF April 11 – March 12)
 – Heart disease and strokes. 1 in 9 females drink alcohol at increasing & high risk levels. 1 in 15 females have coronary heart disease (CHD) (source: Life style survey 2012) (source: Crime Survey for England & Wales 2012) - modelled estimates. (source: Life style survey 2012) RID= – modelled estimates. 1 in 61 people have Cancer. (source: QOF April 11 – March 12)")
52
Population impact? Domestic abuse incidents (N =3409)
Domestic abuse crimes (N = 489) Sanction detentions (N = 318) Court cases (N = 288) Successful convictions (N = 204)
 Sanction detentions (N = 318) Court cases (N = 288) Successful convictions (N = 204)")
53
Aims of Needs Assessment
The aims of the needs assessment were; To assess the levels of domestic abuse, and health and wellbeing needs of those affected in Knowsley To identify the causes and drivers of domestic abuse To explore the links between domestic abuse and other risk taking behaviours To investigate the extent to which current service provision is addressing the needs

54
Process Conduct Literature / evidence review
Data intelligence collation and analysis (incl. service mapping and intelligence) Stakeholder engagement Scrutiny review
 Stakeholder engagement. Scrutiny review.")
55
Overview of trend Domestic abuse Offences/crimes
Knowsley Domestic Abuse Service Referrals Housing issues / homelessness presentations Incidents (police) A & E - Home Assaults National Survey prevalence
 A & E - Home Assaults. National Survey prevalence.")
56
Financial Impact in Knowsley
£56m human and emotional £11m housing, civil, legal employment and other costs. £3.8m physical and mental health care costs. £2.4m criminal justice costs. £452,000 social care costs. Calculated using estimates from (Järvinen et al, 2008) for domestic violence. Total annual cost to Knowsley economy estimated as £73 million.
 for domestic violence. Total annual cost to Knowsley economy estimated as £73 million.")
57
Health and Wellbeing Needs – Victims and their children
Children and Young people Short term Physical health (minor – severe) Sexual health Eating disorders / self harm Fear and safety concerns (safety primary concern) Short and long term Mental health and wellbeing (depression, suicide, self harm, confidence, self esteem) Substance misuse (particularly alcohol) Housing Employment & Poverty Difficulties with relationships (intimacy, trust) Isolation Mental health and wellbeing Behavioural and emotional problems Links with substance misuse Child Maltreatment and Child abuse – identifying and dealing with it Education / housing Unsettled childhoods Long term impacts affecting life chances Links with crime, gangs and violence.
 Sexual health. Eating disorders / self harm. Fear and safety concerns (safety primary concern) Short and long term. Mental health and wellbeing (depression, suicide, self harm, confidence, self esteem) Substance misuse (particularly alcohol) Housing. Employment & Poverty. Difficulties with relationships (intimacy, trust) Isolation. Mental health and wellbeing. Behavioural and emotional problems. Links with substance misuse. Child Maltreatment and Child abuse – identifying and dealing with it. Education / housing. Unsettled childhoods. Long term impacts affecting life chances. Links with crime, gangs and violence.")
58
Political Scrutiny Scrutiny review by elected members on the draft needs assessment to; Inform, sense check and develop recommendations Three evidence sessions, involving expert witnesses, plus visits to MARAC and NICE stakeholder session

59
Identified needs / issues
Data / intelligence issues Strategic approach – systems Primary prevention Support for victims Support for affected children Dealing with perpetrator needs

60
Scrutiny recommendations
That the strategic approach to domestic abuse be reviewed That data and intelligence issues in relation to domestic abuse be resolved Seek all opportunities to break the cycle of domestic abuse through a greater focus on prevention That support for victim survivors is reviewed That support for affected children is reviewed That the way perpetrators are dealt with is reviewed

61
Key messages Domestic Abuse is a significant public health issue in Knowsley Applying a public health approach to the needs assessment important Involving members through scrutiny of draft needs assessment was integral to raising profile, gaining ownership and development of recommendations. It raised issues for local authority and health commissioners, wider public sector and providers about referral processes and support services Addressing mental health problems, alcohol issues and healthy relationships potentially could significantly impact on domestic abuse levels. Current focus on dealing with consequences rather than prevention

62
Communication Strategy
Methods Posters Postcards Beermats Bus / Taxis Media Releases Facebook Twitter Community Messaging One Stop Shops GP Practices

63
Questions?

64
Recommendation 1 That the strategic approach to domestic abuse be reviewed by: Considering the strategic governance arrangements for domestic abuse; The council and its partners considering joint commissioning arrangements for domestic abuse specific services to enable a more flexible use of resources; Services focussing on addressing the behaviour of perpetrators as well as resolving the needs of the victim survivor; and, Standards/expectations being developed in the response times to resolve domestic abuse incidents completely.

65
Recommendation 2 That data and intelligence issues in relation to domestic abuse be resolved through: Undertaking further work to improve the recording of domestic abuse across partner agencies and exploring other sources of insight (particularly for teenage intimate partner violence and child on parent abuse); and, Exploring opportunities for the streamlining of referral forms from various agencies to ensure a consistent approach and improving referral processes particularly from the Vulnerable Persons Unit (VPU).
; and, Exploring opportunities for the streamlining of referral forms from various agencies to ensure a consistent approach and improving referral processes particularly from the Vulnerable Persons Unit (VPU).")
66
Recommendation 3 Seek all opportunities to break the cycle of domestic abuse through a greater focus on prevention by: Developing a systematic approach to the primary prevention of domestic abuse; Considering the inclusion of evidence based programmes on violence and domestic abuse within the school curriculum and ensuring that their effectiveness is assessed; Investigating further the content of parenting programmes and exploring the introduction of a specific module on domestic abuse; and, Developing work with Her Majesty’s Prison Service that explores the use of more domestic abuse programmes/modules on programmes for prisoners where domestic abuse isn’t necessarily their trigger offence.

67
Recommendation 4 That support for victim survivors is reviewed by:
Considering the threshold level and pathways for low-medium risk victim survivors; and, Delivering training on domestic abuse awareness and how to support those affected to all front line responders including the police.

68
Recommendation 5 That support for affected children is reviewed by:
Evaluating the effectiveness of programmes to identify and support the needs of children affected by domestic abuse and show they make a difference; Reviewing the support for children affected by domestic abuse that fall below the threshold for wellbeing support and identify whether their needs are being adequately addressed; Collecting insight from children and young people on the impact of domestic abuse and using this information to inform commissioning decisions; and Testing the feasibility of rolling out Operation Encompass across Merseyside, through police colleagues given that some of Knowsley’s school age children may attend schools across local authority boundaries.

69
Recommendation 6 That the way perpetrators are dealt with is reviewed by: Assessing the long term effectiveness of existing perpetrator programmes; Exploring the reasons why there are disproportionately higher levels of cracked and ineffective domestic abuse trials in Knowsley; Exploring the greater use of sanctions for perpetrators who do not attend or complete community perpetrator programmes; Considering the use of civil action against perpetrators of domestic abuse where criminal convictions are not possible; and, Considering the broader use of Integrated Offender Management (IOM) for domestic abuse offenders to allow for a more intensive intervention to reduce the risk of reoffending and the risk of harm.
 for domestic abuse offenders to allow for a more intensive intervention to reduce the risk of reoffending and the risk of harm.")
70
Asset based alcohol and drug recovery

71
Strategy “For too many people currently on a substitute prescription, what should be the first step on the journey to recovery risks ending there. This must change.” “The voluntary and community groups, charities and social enterprises sector will be encouraged and supported to get involved.” “We will encourage local areas to promote a whole family approach to the delivery of recovery services.” Asset based alcohol and drug recovery

72
Solutions Expert group chaired by Professor John Strang
‘For many people, treatment is an important part of their recovery journey. It is a component of a broader recovery-orientated system of health and social care and support that harnesses the full range of individual, social and community assets.’ Asset based alcohol and drug recovery

73
Positive Social networks
Strategy change Deficit Focused Crime Overdose BBV Illicit heroin use Asset Focused Positive Social networks Mutual Aid Well-being Employment Housing Community Engagement ‘Voluntarily sustained control over substance use which maximises health and wellbeing and participation in the rights, roles and responsibilities of society.’ UKDPC Asset based alcohol and drug recovery

74
Individual assets - Recovery capital
Be active Connect ‘The breadth and depth of internal and external resources that can be drawn upon to initiate and sustain recovery’ Granfield and Cloud Give Take Notice Keep learning Asset based alcohol and drug recovery

75
Measuring Assets National Drug Treatment Monitoring System now measures recovery activity including access to support with housing, ETE, family support, parenting, mutual aid Asset based alcohol and drug recovery

76
Communities taking the lead
Asset based alcohol and drug recovery

77
Facilitating Access to Mutual Aid
Asset based alcohol and drug recovery

78
Public Services (Social Value) Act
The authority must consider— (a)how what is proposed to be procured might improve the economic, social and environmental well-being of the relevant area, and (b)how, in conducting the process of procurement, it might act with a view to securing that improvement. Potential lever to ensure that local recovery communities are at the heart of the commissioning of any future treatment/recovery systems and to ensure that the development of local recovery focused assets is a contracted outcome. Social Value vs Best Value or Social Value as Best Value Asset based alcohol and drug recovery
how what is proposed to be procured might improve the economic, social and environmental well-being of the relevant area, and (b)how, in conducting the process of procurement, it might act with a view to securing that improvement. Potential lever to ensure that local recovery communities are at the heart of the commissioning of any future treatment/recovery systems and to ensure that the development of local recovery focused assets is a contracted outcome. Social Value vs Best Value or Social Value as Best Value Asset based alcohol and drug recovery.")
79
Paul Duffy – Health Improvement Manager (Alcohol and Drugs) Paul
Paul Duffy – Health Improvement Manager (Alcohol and Drugs) Asset based alcohol and drug recovery
 Asset based alcohol and drug recovery.")
Similar presentations










 in Berkshire Community Partnership Forum February 2014 Sally Murray Head of Children’s Commissioning.>")













