Download presentation
Presentation is loading. Please wait.

1
Thromboembolic complications in IBD
Athos Bousvaros MD, MPH Associate Director, IBD Center

2
With gratitude Naamah Zitomersky Cameron Trenor Menno Verhave
Thrombosis and IBD: A call for improved awareness and prevention. IBD Journal :458

3
Overview Pathophysiology Risks of venous thromboembolism Risk factors
Relative Absolute Risk factors Workup of thromboembolic event Prophylaxis Treatment

4
Arterial vs. venous thromboembolism
Clot in an artery (carotid, coronary, SMA) Rare in younger patients (under 40 years) Preventable with antiplatelet drugs (ASA) Venous Clot in venous system Deep venous thrombosis (usually in leg or arm) Preventable with anticoagulation (heparin, coumadin)
 Rare in younger patients (under 40 years) Preventable with antiplatelet drugs (ASA) Venous. Clot in venous system. Deep venous thrombosis (usually in leg or arm) Preventable with anticoagulation (heparin, coumadin)")
5
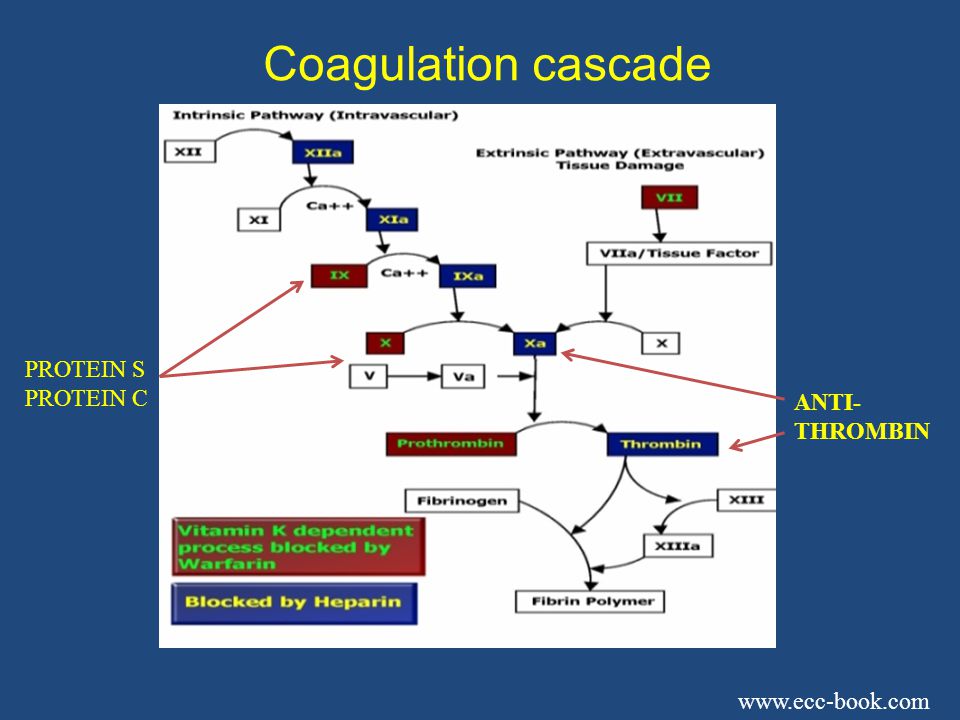
Coagulation cascade PROTEIN S PROTEIN C ANTI- THROMBIN
7
Risk factors in the general population
Hereditary thrombophilias Factor V Leiden mutation 5% of Caucasians, 2% Hispanics, 1% African Americans Prothrombin gene mutation (G20210A) 2% of Caucasians Protein C, Protein S, Antithrombin 3 deficiencies Environmental causes Smoking, oral contraceptives Surgery, immobility
 2% of Caucasians. Protein C, Protein S, Antithrombin 3 deficiencies. Environmental causes. Smoking, oral contraceptives. Surgery, immobility.")
8
Why are IBD patients especially at risk?
Inflammation and disease activity Increased fibrinogen Increased D-dimer Increased factors V, VIII, IX Prothrombotic antibodies (antiphospholipid) Endothelial damage Increased homocysteine Prothrombotic medications thalidomide
 Endothelial damage. Increased homocysteine. Prothrombotic medications. thalidomide.")
9
Inflammation is the Most Common Risk Factor; DVT without a Risk Factor is Rare in Children
No Risk Factor Infl Lupus Anticoag Infec CVL NEJM 2004;351: 9

10
Venous thromboembolism (VTE) in inflammatory bowel disease
Relative risk is high Six fold greater hazard ratio in < 20 years old* Mainly in patients with flares** Absolute risk is low 2811 IBD patients recruited over 2.5 yrs*** 116 (4%) of patients developed de novo VTE Mean age 42 years Risk of recurrence high if anticoagulation stopped *Kappelman et al; Gut 2011 Nylund et al; JPGN 2013 ** Grainge et al, Lancet 2010 *** Novacek, Gastro 2010
 of patients developed de novo VTE. Mean age 42 years. Risk of recurrence high if anticoagulation stopped. *Kappelman et al; Gut Nylund et al; JPGN ** Grainge et al, Lancet *** Novacek, Gastro")
11
What complications occur with increased frequency in adults?
Meta analysis of over 200,000 patients – increased risk of venous, but not arterial events. Deep venous thrombosis RR 2.4 Pulmonary embolism RR 2.5 Ischemic heart disease RR 1.3 Mesenteric ischemia RR 3.4 Fumery et al, J. Crohn’s Colitis 2013

12
IBD Clot rates – Boston Children’s
All kids IBD kids VTE risk 1/10,000/y ~3x higher VTE in Inpatients 0.58% (58/10,000) 1.5% (8/532) (1.7% incl. arterial) CVL CHB* 3.8% (4/104) *3.82 symptomatic events per 1000 catheter days Zitomersky et al, JPGN 2013; 57:343-7
 1.5% (8/532) (1.7% incl. arterial) CVL. CHB* 3.8% (4/104) *3.82 symptomatic events per 1000 catheter days. Zitomersky et al, JPGN 2013; 57:")
13
A major source of morbidity
IVC clot needing filter in severe UC

14
Is heparin prophylaxis indicated?
Not in outpatients, unless another reason “Prophylaxis would be needed for 312 person-years of IBD flares to prevent one person developing venous thromboembolism” – G. Nguyen, Lancet Yes in inpatients Included in AGA physician performance measure set, but only 35% of gastroenterologists use it.* “…heparin has an important role in prophylaxis against thromboembolism in patients admitted to hospital with severe colitis” – Kornbluth and Sachar, ACG Guideline 2010 *Tinsley, J. Clin Gastroenterol 2013

15
Prophylactic Anticoagulation for High Risk Colitis patients
No personal or strong family history of bleeding Pre-pubertal or < 40kg Enoxaparin 0.5 mg/kg BID Post-pubertal or > 40kg Enoxaparin 40 mg daily Continue anticoagulation until either: Discharge Resolution of colitis, or Baseline mobility, if post-op

16
The “ouch” factor

17
Colitis: New diagnosis or Admission
Review family history for thrombosis AND bleeding Address dehydration Address immobility (PT consultation, plan for ambulation) Alternatives to combined oral contraception Counsel about smoking, inactivity, long travel Consider factor VIII D-dimer lupus anticoagulant anti-cardiolipin and anti-2 glycoprotein 1 antibodies
 Alternatives to combined oral contraception. Counsel about smoking, inactivity, long travel. Consider. factor VIII. D-dimer. lupus anticoagulant. anti-cardiolipin and anti-2 glycoprotein 1 antibodies.")
18
Proposed High Risk Definition
Personal history thrombosis, 1st degree family history, Known thrombophilia,# OCPs, Smoking > 1ppd, BMI > 35 OR PICC/Broviac/Port-a-Cath (especially if ASD) thalidomide Inpatient colitis OR Major surgery High Risk *awareness if elevated factor VIII, D-dimer, isolated APLA #Known thrombophilia = factor V Leiden, prothrombin gene mutation, low protein C/S or antithrombin function, persistent APLA >40 for >12 weeks
 thalidomide. Inpatient colitis. OR. Major surgery. High Risk. *awareness if elevated factor VIII, D-dimer, isolated APLA. #Known thrombophilia = factor V Leiden, prothrombin gene. mutation, low protein C/S or antithrombin function, persistent APLA >40 for >12 weeks.")
19
Evaluation of DVT High index of suspicion Labs Imaging
Headache, vomiting Extremity swelling Labs D-dimer excellent negative predictive value Imaging Ultrasound of extremity and femoral veins MR or MR venography preferred for CNS Spiral CT for pulmonary embolism Cardiac echocardiogram for patent foramen

20
Therapy of clots (adult and pediatric)
Unfractionated heparin 75 U/kg bolus 18 U/kg/hour Goal anti-Xa level, U/ml Low molecular weight heparin (enoxaparin) 1mg/kg sc bid Goal anti-Xa level U/ml Warfarin for long term management? Colectomy may be life-saving Timing of colectomy is tricky
 1mg/kg sc bid. Goal anti-Xa level U/ml. Warfarin for long term management Colectomy may be life-saving. Timing of colectomy is tricky.")
21
Additional therapy Catheter directed thrombolysis
Inferior vena cava filter Protect against pulmonary emboli Surgical thrombectomy When thrombolysis contraindicated Is a large clot complicating severe colitis an indication for colectomy? What is optimal timing for the colectomy? Control colitis medically, treat clot, then operate

22
Is heparin safe in IBD? Severe bleeding on anticoagulation is rare
Treatment Prophylaxis All adults 2% 3% All kids 4.3% (trauma) CHB 2.5% (4/162) 4.1% HR (2/49) ??? CHB IBD 11.1% (1/9)
 CHB. 2.5% (4/162) 4.1% HR (2/49) CHB IBD. 11.1% (1/9)")
23
Conclusions All patients with IBD are probably at an increased risk of clots during disease flares Absolute risk is low The highest risk group appears to be inpatients with severe colitis Inflammation Immobility Prophylaxis with LMWH is indicated in patients hospitalized for severe colitis or post-op Enoxaparin, 40 mg SQ daily in adults

Similar presentations












>")

 IPC/GCS or, UFH 5000 SQ q 12 hrs or, Enoxaparin 40mg SQ daily IPC/GCS or, UFH 5000.>")




