Download presentation
Presentation is loading. Please wait.

1
Tuberculosis and HIV Management of Co-Infected Patients
Michael Lauzardo, MD MSc Director, Southeastern National Tuberculosis Center Chief, Division of Infectious Diseases and Global Medicine University of Florida

2
Disclosures of Financial Relationships
This speaker has no significant financial relationships with commercial entities to disclose. This speaker will not discuss any off-label use or investigational product during the program. This slide set has been peer-reviewed to ensure that there are no conflicts of interest represented in the presentation.

3
Epidemiology

4
TB epidemiology GLOBAL USA Infected cases 1.7 billion (33% population)
10-15 million (4% population) Case incidence 8-10 million/year 11,182 in 2010 Case prevalence 40-50 million 20,000 Deaths 1.9 million/year ~1,000 /year HIV Co-infection 1.1 million new cases/year >40% of all TB cases in Africa are HIV co-infected ~700 cases 6%
 Case incidence million/year. 11,182 in Case prevalence million. 20,000. Deaths. 1.9 million/year. ~1,000 /year. HIV Co-infection. 1.1 million new cases/year. >40% of all TB cases in Africa are HIV co-infected. ~700 cases. 6%")
5
Estimated Tuberculosis Incidence (WHO)
")
6
Epidemiology of HIV: Global

7
Epidemiology of HIV: United States
There are more than 1.1 million people living with HIV in the United States, and approximately 56,000 new HIV infections annually. Risk behavior data show that 47% of men who have sex with men engaged in unprotected anal intercourse in the past year, and 33% of injection drug users had shared syringes. One third (32%) of people diagnosed with HIV in 2008 were diagnosed with AIDS within 12 months, indicating missed opportunities for care and prevention. J Acquir Immune Defic Syndr Dec;55 Suppl 2:S64-8.
 of people diagnosed with HIV in 2008 were diagnosed with AIDS within 12 months, indicating missed opportunities for care and prevention. J Acquir Immune Defic Syndr Dec;55 Suppl 2:S64-8.")
8
Estimated prevalence of HIV co-Infection among New TB cases
0–4 5–19 20–49 50 and higher No estimate The situation is the same when we compare the HIV prevalence among TB patients and people who injecting drugs. In countries where there is high HIV prevalence among TB patients, the HIV prevalence among people who inject drugs is either high or unknown or with no reports.

9
Stop TB Department

10
Stop TB Department

11
Reported TB Cases* United States, 1982–2009
No. of Cases Year *Updated as of July 1, 2010.

12
Reporting of HIV Test Results in Persons with TB by Age Group United States, 1993–2009*
% with Test Results *Updated as of July 1, 2010. Note: Includes TB patients with positive, negative, or indeterminate HIV test results. Persons from California reported with AIDS only through 2004. (HIV test results are not reported from California)
")
13
Estimated HIV Coinfection in Persons Reported with TB, United States, 1993–2009*
*Updated as of July 1, 2010. Note: Minimum estimates based on reported HIV-positive status among all TB cases in the age group.

14
Trends in TB Cases in Foreign-born Persons, United States, 1989–2009*
No. of Cases Percentage *Updated as of July 1, 2010.

15
Clinical Presentation of HIV/TB

16
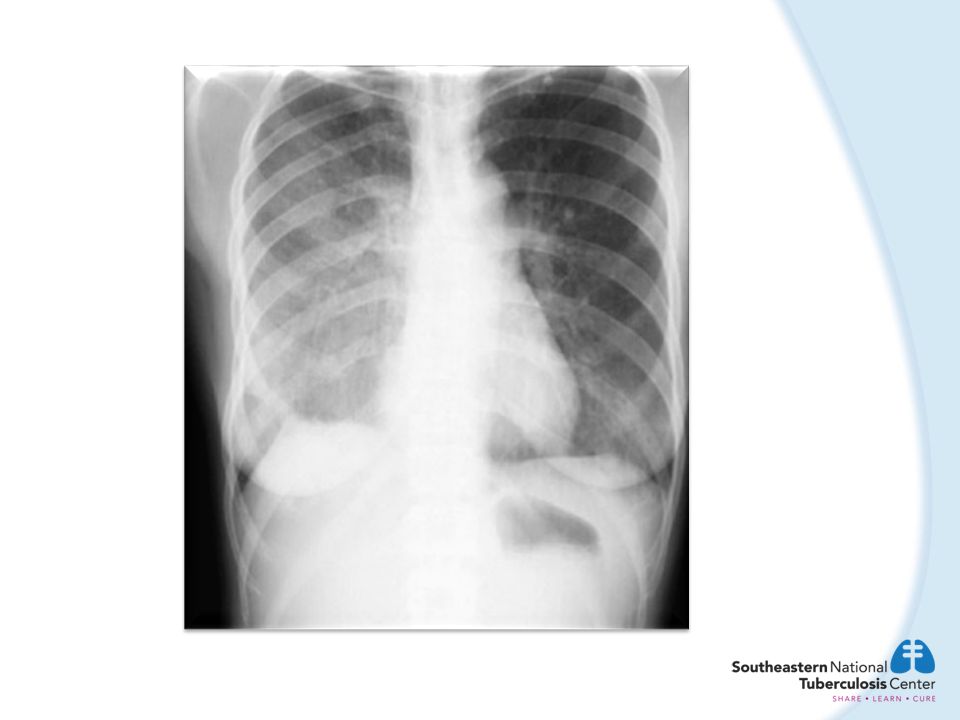
Case 1 The patient is a 28-year-old woman from the former Soviet Union who has just been diagnosed with HIV. She was exposed to TB presumably two years ago by her boyfriend who is from Ukraine She is on no medications at present. She is asymptomatic Her physical exam is unremarkable and a PPD is placed that is negative A chest x-ray is done

17
HIV positive patient with MTB positive sputum.
3/05

18
The radiologist reads the film and comments on the right paratracheal adenopathy and states that lymphoma is likely given that the patient has HIV infection. A reasonable next step is: Refer the patient to heme-onc for further evaluation. Order a PET scan. Obtain sputum for AFB times 3 through the health department. Consider empiric treatment for active TB by DOT. Answers C and D are correct.

19
Clinical Presentation
Persons with LTBI are, by definition, asymptomatic. Among HIV-infected persons, the presentation of active TB disease is influenced by the degree of immuno- deficiency. In addition, early after initiating ART in severely immunosuppressed patients, previously unrecognized subclinical TB can be unmasked by reconstitution of the immune system.

20
Clinical Presentation
In HIV-infected patients without pronounced immunodeficiency (e.g., CD4+ count >350 cells/µl), TB clinically resembles TB among HIV-uninfected persons. The majority of patients have disease limited to the lungs, and have typical chest radiographic manifestations. However, extrapulmonary disease is more common in HIV-infected persons than in HIV-uninfected persons, regardless of CD4+ counts.
, TB clinically resembles TB among HIV-uninfected persons. The majority of patients have disease limited to the lungs, and have typical chest radiographic manifestations. However, extrapulmonary disease is more common in HIV-infected persons than in HIV-uninfected persons, regardless of CD4+ counts.")
22
Clinical Presentation: More advanced Immunosuppression
In advanced HIV disease, the chest radiographic findings of pulmonary TB are markedly different. Lower lobe, middle lobe, interstitial, and miliary infiltrates are common and cavitation is less common. Marked mediastinal lymphadenopathy also can be found. Even with normal chest radiographs, patients with HIV infection and pulmonary TB might have acid fast bacilli (AFB)-positive sputum smear and culture results.
-positive sputum smear and culture results.")
26
Clinical Presentation: Advanced Immunosuppression
With increasing degrees of immunodeficiency, extrapulmonary TB (e.g., lymphadenitis, pleuritis, pericarditis, and meningitis), with or without pulmonary involvement, is more common, and found in the majority of TB patients with CD4+ counts <200 cells/µl. Among such patients, TB can be a severe systemic disease with high fevers, rapid progression, and sepsis syndrome.
, with or without pulmonary involvement, is more common, and found in the majority of TB patients with CD4+ counts <200 cells/µl. Among such patients, TB can be a severe systemic disease with high fevers, rapid progression, and sepsis syndrome.")
27
HIV/TB and Pulmonary Disease
Although HIV-infected persons with TB may have the classic symptoms of TB many patients have few symptoms. In addition, many HIV-infected patients with TB—particularly patients with advanced HIV disease and low CD4+ T lymphocyte counts—have atypical chest radiograph findings. HIV-infected patients with TB are less likely to have cavitary pulmonary disease than are HIV-uninfected patients with TB, and up to 22% of HIV-infected persons with pulmonary TB have normal chest radiograph findings. Sterling et al 2010

28
Extrapulmonary Disease in HIV/TB
Forty percent to 80% of HIV-infected persons with TB have extrapulmonary disease, compared with 10%–20% of HIV-uninfected persons. The risk of extrapulmonary TB increases with lower CD4+ T lymphocyte count. The most common forms of extrapulmonary disease are lymphatic and pleural, but almost any site can be involved, including the bone and/or joint (particularly the thoracic spine), soft tissue (eg, psoas muscle, which may be associated with spinal disease), central nervous system, and pericardium
, soft tissue (eg, psoas muscle, which may be associated with spinal disease), central nervous system, and pericardium.")
30
Diagnosis of LTBI

31
Patient is 34 year old man with a 2 year history of HIV
Patient is 34 year old man with a 2 year history of HIV. His last CD4 count was 325 and his viral load is 127,320. He is asymptomatic and reports that he has not been compliant with his anti-retroviral regimen. He has the following chest x-ray:

33
He has a documented history of a positive PPD after an exposure 4 years ago, but he did not take his treatment for LTBI at that time. His repeat PPD is negative one week ago. The best next step would be: Once active TB is adequately ruled out, treat for LTBI and consider DOT if that is at all possible. Perform an IGRA, T-SPOT or Quantiferon GIT, to confirm the history of a positive PPD before committing to a regimen of LTBI therapy. Start on therapy for active TB disease until you have the results of three sputum studies. Repeat PPD since that was what was used previously and he responded to it previously. None of the above.

34
Prevention of TB: Treatment of LTBI
Isoniazid (INH) preventive therapy (IPT) reduces risk of TB in HIV+ people by 62% in PPD+ By 36% overall Evidence of survival benefit in children and in adults in cohort studies Benefit of IPT may wane after 1-2 years in high prevalence settings
 preventive therapy (IPT) reduces risk of TB in HIV+ people. by 62% in PPD+ By 36% overall. Evidence of survival benefit in children and in adults in cohort studies. Benefit of IPT may wane after 1-2 years in high prevalence settings.")
35
Efficacy of IPT in HIV+ Adults: Risk of TB
11 randomised trials with 8,130 HIV+ participants overall reduction in TB = 36%, reduction PPD+ = 62% Woldehanna and Volmink, Cochrane Review 2006

36
Treatment of Latent TB in HIV+ Patients and Survival in Brazil
Pinho, AIDS 2001

37
Prevention of TB: Treatment of LTBI
Treatment options for LTBI include INH daily or twice weekly for 9 months. Results from a randomized clinical trial comparing INH daily therapy for 9 months with 12 doses of once- weekly INH-rifapentine are pending. Because of an increased risk for fatal and severe hepatotoxicity, a 2-month regimen of daily RIF and PZA is not recommended for LTBI treatment regardless of HIV status.

38
Prevention of TB: Treatment of LTBI
Alternatives for persons who cannot take INH or who have been exposed to a known INH-resistant patient include either RIF or rifabutin alone for 4 months. Decisions to use a regimen containing either RIF or rifabutin should be made after considering potential drug interactions. No evidence suggests that LTBI treatment should be continued beyond the recommended duration in persons with HIV infection. Therefore, LTBI treatment should be discontinued after completing the appropriate number of doses.

39
Case 2 Get a repeat chest x-ray.
A 35-year-old man from Honduras is newly HIV-positive. His CD4 count is 105 cells/μl and his viral load is 245,000. He has lost weight but has responded well recently to treatment for PCP. You place a PPD and it is 0 mm. He has no known exposure for TB and a workup for active TB, including a CT scan and bronchoscopy, was negative last month. For follow-up, you: Get a repeat chest x-ray. Repeat the PPD and do a QuantiFERON test. Repeat the PPD or an IGRA once the CD4 count is above 200 cells/μl. After the extensive work-up no other TB evaluation is necessary at this time. Answers A and B are correct.

40
Diagnosis: Diagnosis of Latent TB Infection (LTBI)
All persons should be tested for LTBI at the time of HIV diagnosis regardless of their TB risk category. Persons with negative tests for LTBI, advanced HIV infection (CD4+ count <200 cells/µl), and without indications for initiating empiric LTBI treatment should be re-tested for LTBI once they start ART and attain a CD4+ count >200 cells/µl. In general, annual testing for LTBI is recommended for HIV- infected persons who are or remain in a "high-risk" category for exposure to active TB. HIV-infected persons with LTBI should have chest x-ray and clinical evaluation to rule out active TB.
, and without indications for initiating empiric LTBI treatment should be re-tested for LTBI once they start ART and attain a CD4+ count >200 cells/µl. In general, annual testing for LTBI is recommended for HIV- infected persons who are or remain in a high-risk category for exposure to active TB. HIV-infected persons with LTBI should have chest x-ray and clinical evaluation to rule out active TB.")
41
Diagnosis of LTBI: Tuberculin Skin Testing
The tuberculin skin test (TST), placed by the Mantoux method, is considered positive in HIV-infected persons if induration of >5 mm is demonstrated hours after the intradermal placement of 0.1 mL purified protein derivative (PPD).
, placed by the Mantoux method, is considered positive in HIV-infected persons if induration of >5 mm is demonstrated hours after the intradermal placement of 0.1 mL purified protein derivative (PPD).")
42
Diagnosing LTBI with IGRA: Practical Points in HIV-infected Patients
For both the TST and IGRAs, however, HIV-related immunosuppression might be associated with false- negative result. The frequency of false-negative and indeterminate IGRA results increases with advancing immunodeficiency. Results from comparative studies of TST and IGRAs in HIV-infected patients indicate that concordance between the tests is not complete.

43
Treatment of LTBI: Current Recommendations
Drug Dose Duration INH 300 MG Daily 9 Months RIF 600 MG Daily 4 Months RIF/PZA 600MG/ 15-30 MG/KG Daily 2 Months No Longer Recommended RBN RPT/INH 900mg Once weekly 12 Weeks(12 doses total)
")
44
Case 3 45-year-old man with HIV for 7 years with a CD4 count of 250 and a viral load of 1000. No recent OI and other than his HIV and mild hypertension he has been healthy. He has no symptoms of TB. He drives to work daily with co-worker who was recently diagnosed with active pulmonary TB. As part of the contact investigation a PPD was placed 12 weeks after the last exposure and it was read at the health department as 0 mm. Because of concerns over the PPD result a QuantiFERON test was ordered and that test was negative as well

46
Case 3 After a thorough history and physical, the next appropriate step would be: Start INH at 300 mg daily for 9 months if there are no contraindications for therapy. Follow-up as clinically indicated because there is no evidence of LTBI at this time. Repeat chest x-ray and clinical exam in 3 months because of the increased risk of TB. Repeat testing for LTBI when the CD4 count is above 350 and viral load undetectable. Answers B and C are correct.

47
Treatment of Active TB in HIV Co-infected Patients

49
TB/HIV Treatment: Basic Principles
The treatment of TB in patients with HIV infection should be the same as that for patients with TB who do not have HIV infection. Standard first-line therapy for TB with a 4-drug intensive treatment phase of 2 months, followed by 4 months of treatment with a 2-drug regimen, is highly effective in patients with HIV infection-related TB. Early reports of treatment outcomes in patients with HIV/TB showed that early outcomes were generally very good, but long-term outcomes were poor because of HIV infection-related mortality.

50
Recommendations for the Treatment of HIV Infection-Related Tuberculosis.
Sterling T R et al. Clin Infect Dis. 2010;50:S223-S230 © 2010 by the Infectious Diseases Society of America

51
TB/HIV: When should ARVs be started in newly diagnosed TB and HIV?
Among HIV-infected persons who receive a diagnosis of TB and do not receive HAART, the mortality rate is high (as high as 91% among persons with AIDS). Initiation of HAART is associated with improved survival among all HIV infected persons, including those with TB. Three randomized, controlled trials (SAPiT, STRIDE, and CAMELIA) demonstrate that, for co-infected patients with advanced immunosuppression, the survival benefit of starting ARV within the first 2 weeks of TB therapy outweighs the risk for immune reconstitution inflammatory syndrome (IRIS) and other adverse events.
. Initiation of HAART is associated with improved survival among all HIV infected persons, including those with TB. Three randomized, controlled trials (SAPiT, STRIDE, and CAMELIA) demonstrate that, for co-infected patients with advanced immunosuppression, the survival benefit of starting ARV within the first 2 weeks of TB therapy outweighs the risk for immune reconstitution inflammatory syndrome (IRIS) and other adverse events.")
52
TB/HIV: When should ARVs be started in newly diagnosed TB and HIV?
In the CAMELIA trial, 661 patients with new, smear-positive TB and a median CD4 count of 25 cells/mm3 were randomized to begin ARV either 2 weeks or 8 weeks after the start of TB therapy. More than 70% of the patients had baseline CD4 counts 50 cells/mm3. Median interval from TB treatment initiation to ART initiation was 14 days and 56 days, respectively.

53
CAMELIA Study During a median follow-up of 25 months, the earlier-ART group had a significantly lower mortality rate than the later-ART group (18% vs. 27%). IRIS risk was once again higher in the earlier-ART group. Six deaths were attributed to IRIS. Conclusion: Starting ARV is reduces mortality even after the increased risk of complications and deaths related to IRIS. Patients with CD4 counts below 50 cells/mm3 need to be monitored more closely for the development of IRIS
. IRIS risk was once again higher in the earlier-ART group. Six deaths were attributed to IRIS. Conclusion: Starting ARV is reduces mortality even after the increased risk of complications and deaths related to IRIS. Patients with CD4 counts below 50 cells/mm3 need to be monitored more closely for the development of IRIS.")
54
TB/HIV: Drug Interactions
The primary drug-drug interactions of concern are those between rifamycins and HIV-1 protease inhibitors, nonnucleoside reverse transcriptase inhibitors, integrase inhibitors, and CCR5 inhibitors. Protease Inhibitors: Rifampin significantly decreases protease inhibitor levels and, therefore, should generally not be given in combination with this drug class. NNRTI: Rifampin can be given with efavirenz or nevirapine, but there is increasing evidence that virological outcomes are better with efavirenz than with nevirapine. Integrase Inhibitors: Rifampin decreases raltegravir concentrations by 40%–61%; thus, this combination should generally not be given; rifabutin does not effect raltegravir levels. CCR5 Inhibitors: Rifampin decreases maraviroc levels by 78%.

55
Management of Interactions among Drugs Used to Treat Tuberculosis (TB) and HIV Infection.
Sterling T R et al. Clin Infect Dis. 2010;50:S223-S230 © 2010 by the Infectious Diseases Society of America

56
TB/HIV Treatment: Risk of Recurrence
The primary risk factor for TB recurrence among HIV-infected patients with TB appears to be low CD4+ T lymphocyte count, with the risk highest among persons with a CD4+ T lymphocyte count <100 cells/mm3. Low CD4+ T lymphocyte count appears to be a stronger risk factor than the factors that are associated with relapse in HIV-seronegative persons: cavitary pulmonary disease, positive sputum culture result after 2 months of treatment, bilateral pulmonary disease, low body weight, and white race.

57
Treatment of TB Disease
Considering the variability of yield from smear microscopy and nucleic acid amplification tests (NAA tests), empiric treatment should be initiated and continued in HIV-infected persons in whom TB is suspected until all diagnostic work-up is complete. When active TB is diagnosed or suspected, a multi- drug anti-TB treatment regimen should be started immediately. This approach promotes rapid killing of tubercle bacilli, prevents the emergence of drug resistance, and decreases the period of contagion.
, empiric treatment should be initiated and continued in HIV-infected persons in whom TB is suspected until all diagnostic work-up is complete. When active TB is diagnosed or suspected, a multi- drug anti-TB treatment regimen should be started immediately. This approach promotes rapid killing of tubercle bacilli, prevents the emergence of drug resistance, and decreases the period of contagion.")
58
Treatment of TB Disease
Recommendations for anti-TB treatment regimens in HIV-infected are the same as for those without HIV infection. Treatment of drug-susceptible TB disease should include a 6-month regimen with an initial phase of INH, rifampin (RIF) or rifabutin, pyrazinamide (PZA), and ethambutol (EMB) administered for 2 months, followed by INH and RIF (or rifabutin) for 4 additional months. When drug-susceptibility testing confirms the absence of resistance to INH, RIF, and PZA, EMB may be discontinued before 2 months of treatment have been completed.
 or rifabutin, pyrazinamide (PZA), and ethambutol (EMB) administered for 2 months, followed by INH and RIF (or rifabutin) for 4 additional months. When drug-susceptibility testing confirms the absence of resistance to INH, RIF, and PZA, EMB may be discontinued before 2 months of treatment have been completed.")
59
Multi-Drug Resistant (MDR) TB
Defined as resistance to isoniazid and rifampin Created by poorly managed TB programs Non-adherence to therapy Poor quality drugs or supply Leads to bad outcomes Longer treatment (go from 6-24 months) Toxic regimens Cost increases fold High death rates Disastrous outcomes in HIV settings
 Toxic regimens. Cost increases fold. High death rates. Disastrous outcomes in HIV settings.")
60
Adverse Reactions including Immune Reconstitution Syndrome

61
Case 4 A 36-year-old man from Mexico presents to the ER with symptoms consistent with TB with extreme weight loss of 40 pounds, cough, fevers, and night sweats. His chest x-ray is abnormal and he is isolated and started on TB meds at appropriate doses. His records are reviewed and it is determined that he was actually found to be HIV-positive a year ago and was not adherent to ART despite having advanced disease with a CD4 of 127 cells/µl and a viral load of 350,000. He is started on TB therapy along with efavirenz and combivir while he is in the hospital

62
Case 4 He responds quickly to the TB therapy with improvement in symptoms in about 2 weeks and he is released home. After 6 weeks of therapy he has the insidious onset of lower extremity weakness. After 8 weeks of therapy you are informed by the health department that he can no longer walk. An MRI is performed.

63
MRI C-spine

64
Case 4 Which of the following answers is the most likely explanation for what has occurred? A drug reaction between the anti-retrovirals and the TB medications, specifically the INH and rifabutin Immune reconstitution syndrome Multi-drug resistant TB Drug toxicity from the combined neurotoxic effects CNS lymphoma

65
Paradoxical Response Immune Reconstitution Syndrome

Similar presentations



























 Gram (+) rod (bacilli). Acid-fast Pulmonary.>")
