Download presentation
Presentation is loading. Please wait.

1
CORE Case 2 Workshop Petra Lewis MD Professor of Radiology and OBGYN
Geisel School of Medicine at Dartmouth CORE Case 2 Workshop

2
Learning objectives Understand who should get a pre-op CXR
Know what features affect how we manage SPNs Know some of the ways that we can manage SPNs in patients Understand the radiographic signs of atelectasis Be able to work out when atelectasis is present and what lobe is involved Apply an algorithm to distinguishing the different causes for an opacified hemithorax Recognize the features of a pneumothorax on different views Recognize tension on a radiograph and how to treat it There is a lot here, may not cover all in one session or be selective

3
What questions/difficulties did you have arising from the case
Note down areas that they had problems. If not covered in current session or planned sessions then will come back to at the end

4
Who should get a pre-op CXR?
37 year old man with no cardiorespiratory symptoms currently but a history of asthma pre-op ACL repair 70 year old asymptomatic woman pre-op hip replacement 45 year old diabetic man with no cardiorespiratory symptoms currently pre-op renal transplant In which of these scenarios should a patient have a preop CXR (none using ACR guidelines)
")
5
Who should get a pre-op CXR?
Acute cardiopulmonary findings by history or physical Chronic cardiopulmonary disease in the elderly (>age 70), previous chest radiograph within 6 months NOTE available. Possibly: Chronic cardiopulmonary disease in the elderly (>age 70), previous chest radiograph within 6 months available.
, previous chest radiograph within 6 months NOTE available. Possibly: Chronic cardiopulmonary disease in the elderly (>age 70), previous chest radiograph within 6 months available.")
6
Solitary Pulmonary Nodules

7
What factors might affect whether we see a solitary pulmonary nodule?
Size, radiographic quality, place in lung (danger zones, blind areas), density, surrounding parenchyma
, density, surrounding parenchyma.")
8
Where might we miss a nodule?
Get students identify areas of the lung where we might miss nodules

9
What factors affect how we manage a lung nodule?
Patient factors Radiographic factors Patients –risk factors, smoking, age, sex, history malignancy Radiographic – size, margins, calcification, presence of other nodules, enhancement

10
Benign hamatoma versus a lung cancer, compare and contrast

11
How can we manage an SPN seen on a CXR?
Assess Follow up Open discussion, fairly superficial Ignore Assess by CT, Biopsy – CT, open, videoscopic, FDG PET Follow up CT, CXR

12
Fleischner Criteria McMahon et al. 2005 Radiology, 237, 395-400.
They don’t need to know details, just that there are criteria that we use to follow SPNs

13
Atelectasis

14
What are the characteristics of atelectasis?
Get them to talk about volume loss, opacity, low lung volumes, usually lack of airbronchograms, may be rapid changes

15
What are the causes of atelectasis
Get them to describe = Mucous plug (surgery, intubation, poor inspiration, supine posture), viral infections, tumors – b9 and malignant, compressive etc
, viral infections, tumors – b9 and malignant, compressive etc.")
16
What are the signs of volume loss?
Get students identify the structures that can move with volume loss – diaphragms, hilar, fissures, trachea, heart etc

17
Linear or ‘plate like’ atelectasis. What do they see here
Linear or ‘plate like’ atelectasis. What do they see here? When might we see this in patients?

18
RUL atelectasis. Tell me what they see, how would they describe it
RUL atelectasis. Tell me what they see, how would they describe it? What lobe? Where are the signs of volume loss? What might be the cause in this patient?

19
RUL atelectasis

20
RUL atelectasis Another example

21
RUL atelectasis More difficult example in an ICU patient

22
Pig Bronchus Just for fun – what happens when you intubate a patient with a ‘tracheal or ‘pig’ bronchus (0.1-2% patients)? And why do all vet cxrs and diagrams have the right lung on the right (because they exam animals from their backs)
 And why do all vet cxrs and diagrams have the right lung on the right (because they exam animals from their backs)")
23
LLL atelectasis in a sick ICU patient. What do they see
LLL atelectasis in a sick ICU patient. What do they see? Is this pneumonia or atelectasis? Why cant they tell?

24
Same patient 24 hrs later, bring out the rapid changes seen in atelectasis
Day 1 Day 2

25
RLL atelectasis and RML consolidation. RUL atelectasis
RLL atelectasis and RML consolidation. RUL atelectasis. Tell me what they see, how would they describe it? What lobe or lobes? Where are the signs of volume loss??

26
RLL atect and RML consolidation

27
RML atelectasis. What do they see?

28
RML atelectasis. What do they see. Compare to the normal on the bottom
RML atelectasis. What do they see? Compare to the normal on the bottom. Why don’t you see signs of volume loss? Why don’t you see all of the collapse RML?

29
LUL atelectasis. Get them to describe the findings, Why is this different than RUL atelectasis? Why can we still see vascular markings on the left on the PA? Talk about cause almost always being Ca

30
LUL atelectasis

31
Total lung atelectasis
What would you see if the lung were totally collapsed?

32
Total lung atelectasis
Kid with mucous plug in airway

33
DDx of unilateral hemithorax opacification
Causes Get them to list the ddx of hemithorax opacification, then bring out key concept of volume loss and how it differs between the causes.

34
Left lung atelectasis. Why do we only see one hemidiaphragm on lateral
Left lung atelectasis. Why do we only see one hemidiaphragm on lateral? Why do we see inc retrosternal air? How do we know this patient is s/psurgery not just atelectasis

35
Pneumothorax Note, supine PTX is covered in Case 3/Workshop 3

36
What are the signs of a pneumothorax
Get them to talk about signs of ptx – pleural lines, how thick they are, where do you see them?, absent lung markings, collapsed lung etc

37
What can we do to see pneumothoraces better?
Views that may help, Lighter (less exposed) film, change parameters on PACS, CLAHE filter, mag up apices, Decubitus (abn side up), Expiratory views CT
 film, change parameters on PACS, CLAHE filter, mag up apices, Decubitus (abn side up), Expiratory views. CT.")
38
2 patients. Where is the ptx
2 patients. Where is the ptx? Right image is an exp view of patient post biopsy with a hydropneumo ptx

39
Skin folds. Is there a ptx. Why not
Skin folds. Is there a ptx? Why not? How does this look different (line thickness, can’t follow, lung markings over apex etc..

40
So you find a pneumothorax… What is your next question ALWAYS?
Is there any sign of tension

41
What are the signs of tension?
Clinical Radiographic Clinical – dec BP, tachcardia, venous distension, hypoxia etc CXR: shift mediastinum, depressed diaphragms, +/-major lung collapse, small heart (esp onCT compression of RA/RV). Discuss that lung does not have to be completely collapsed.
. Discuss that lung does not have to be completely collapsed.")
42
Is there tension? What are the signs? Get them to describe/draw them.

43
Another example

44
Is this a tension ptx>?

45
Follow up after tube insertion

46
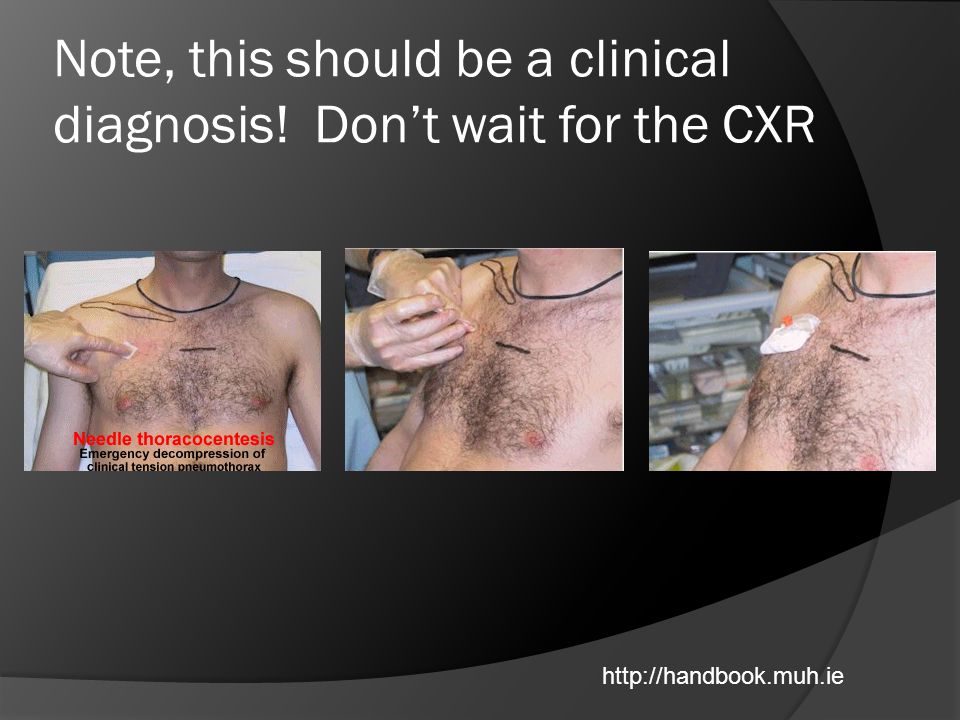
You think your patient has a tension pneumothorax? What will you do?
Talk about inserting needle, pref large bore angiocath into anterior 2nd space, how to find it, going above rib etc.

47
Show them where you go in on the CXR. Avoid the vessels!

48
Note, this should be a clinical diagnosis! Don’t wait for the CXR
49
Appendix

50
Learning Objectives Know the current recommendations for preoperative chest radiographs in people who are healthy and in those with underlying chest and cardiac diseases Understand some of the challenges in detecting small nodules on chest radiographs. Have a concept of the different appearances of pulmonary nodules and their prognostic significance Understand the current status of low dose CT imaging for lung cancer screening. Understand some of the management issues related to pulmonary nodules (including the Fleischner Society recommendations). Have a basic understanding of the use of FDG PET imaging in the management of nodules and lung malignancies. Have reviewed the methods available for nodule biopsy Will understand indications for needle biopsy, how the procedure is done, and the possible complications. Be able to recognize a pneumothorax and understand the meaning and consequences of a tension pneumothorax. Know the options for treating a pneumothorax. Understand the purpose of TNM tumor staging and implications for long term survival Recognize the common appearances of lobar atelectasis on chest radiographs. Recognize the common appearances of linear and subsegmental atelectasis on chest radiographs. Know the different etiologies that may cause complete opacification of a hemithorax Know the expected postoperative appearance of the chest after pneumonectomy.
. Have a basic understanding of the use of FDG PET imaging in the management of nodules and lung malignancies. Have reviewed the methods available for nodule biopsy. Will understand indications for needle biopsy, how the procedure is done, and the possible complications. Be able to recognize a pneumothorax and understand the meaning and consequences of a tension pneumothorax. Know the options for treating a pneumothorax. Understand the purpose of TNM tumor staging and implications for long term survival. Recognize the common appearances of lobar atelectasis on chest radiographs. Recognize the common appearances of linear and subsegmental atelectasis on chest radiographs. Know the different etiologies that may cause complete opacification of a hemithorax. Know the expected postoperative appearance of the chest after pneumonectomy.")
Similar presentations













 M0 - No metastases M1 - Metastases present.>")





