Download presentation
Presentation is loading. Please wait.

1
Neonatal Thrombocytopenia
Suzanne Reuter MD SDPA 2014 Deadwood, SD

2
Financial Disclosure I have no relevant financial relationships to disclose.

3
Objectives Definition of thrombocytopenia
Understand the pathophysiology of neonatal alloimmune thrombocytopenia Review bone marrow function as it relates to platelet production and release Differential Diagnosis in a well, term infant Differential Diagnosis in a sick, term infant

4
Neonatal Alloimmune Thrombocytopenia (NAIT)
* * * * *

5
Neonatal Alloimmune Thrombocytopenia (NAIT)
Mom Fetus * * * Placenta * *

6
Neonatal Alloimmune Thrombocytopenia (NAIT)
Mom Fetus * * * Placenta * *

7
Would you treat the severe thrombocytopenia in NAIT?
a. Yes, the risk of bleeding is really high b. No, this condition will spontaneously resolve and the risk of bleeding is only a threat in premature infants. c. Depends on what the doctor wants to do

8
Would you treat the severe thrombocytopenia in NAIT?
a. Yes, the risk of bleeding is really high b. No, this condition will spontaneously resolve and the risk of bleeding is only a threat in the fetus and premature infants. c. Depends on what the doctor wants to do

9
Baby Lydia – 37 weeks Delivered with spontaneous cry. Apgars 8/9
Dried, suctioned, admitted to NBN Initial platelet count of 177,000 Nadir 120,000 at 36 hr of age Bili 48 hr of age

10
Baby ‘Lila’ – 37 weeks (No Tx)
Delivered with spontaneous cry. Apgars 8/9 Dried, suctioned, admitted to NICU Initial platelet count of 8,000 PE: diffuse petechiae, bruising over lower extremities Platelet transfusion 15 ml/kg Administered intravenous immunoglobulin 1 gm/kg Repeat platelet count 4 hours later 94,000 Platelet f/u 31,000 IVIG repeated x2 – normalization of platelet counts

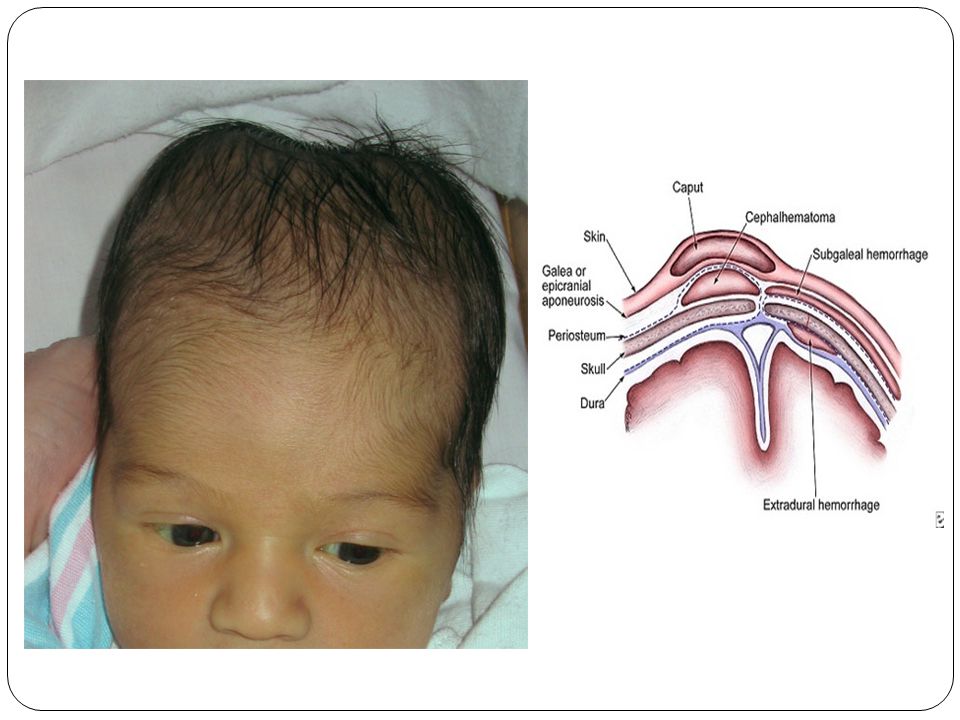
11
Head Ultrasound – Day 1

12
Neonatal Alloimmune Thrombocytopenia (NAIT)
Develops in first pregnancy (unlike Rh sensitization) Fetal platelet antigens form early in gestation Maternal antibodies cross early 2nd trimester Thrombopoietin level is normal Megakaryocytes and platelets produced bind to it Severely low platelet counts in the newborn < 20,000 /microL Normal maternal platelet count
 Fetal platelet antigens form early in gestation. Maternal antibodies cross early 2nd trimester. Thrombopoietin level is normal. Megakaryocytes and platelets produced bind to it. Severely low platelet counts in the newborn. < 20,000 /microL. Normal maternal platelet count.")
13
Neonatal Alloimmune Thrombocytopenia (NAIT)
Most severe complication is intraventricular hemorrhage Occurs in 10-20% of affected newborns ¼ - ½ occurs in utero

14
Neonatal Alloimmune Thrombocytopenia
Rate of recurrence in future pregnancies 75%-90% As severe or more severe than previous Fetal therapies In utero platelet transfusions Maternal therapies IVIG Corticosteroids

15
Which is the best treatment for thrombocytopenia in NAIT in the first 48 hr of life in an infant with a platelet count of 6,000 /microL? a. Random donor platelet transfusion b. Washed maternal platelets c. Intravenous Immunoglobulin d. Methylprednisolone **Remember 98% of Caucasians have HPA-1a on their platelets. Washing maternal platelets takes hours to collect and process.

16
Which is the best treatment for thrombocytopenia in NAIT in the first 48 hr of life in an infant with a platelet count of 6,000 /microL? a. Random donor platelet transfusion b. Washed maternal platelets c. Intravenous Immunoglobulin d. Methylprednisolone **Remember 98% of Caucasians have HPA-1a on their platelets. Washing maternal platelets takes hours to collect and process.

17
What is the definition of neonatal thrombocytopenia?
a. Platelet count < 100, 000/microL b. Platelet count < 50,000/microL c. Platelet count < 25, 000/microL d. Platelet count < 150, 000/microL

18
What is the definition of neonatal thrombocytopenia?
Platelet count < 150,000 /microL Actually, platelet count < 5th percentile 5th percentile decreases with decreasing gestational age 34-36 weeks – 123, 100 /microL 32 weeks – 104, 200 /microL J Perinatol. 2009;29(2):130
:130.")
19
Definition Platelet count < 150,000/microL Ensure a central sample
Clumping with capillary specimens

20
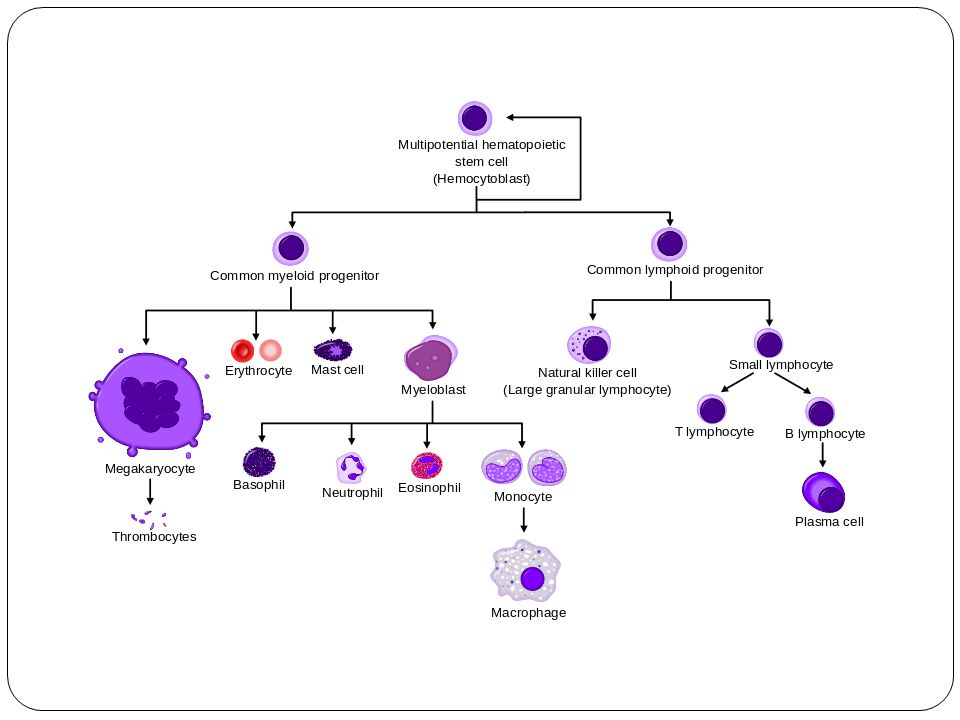
Mechanisms of Thrombocytopenia
Increased destruction Decreased production

23
The most likely physical symptom of neonatal thrombocytopenia is:
a. Petechiae b. Bruising c. Oozing from the umbilical cord d. No symptoms

24
The most likely physical symptom of neonatal thrombocytopenia is:
No physical sign or symptom is the most likely presentation of isolated thrombocytopenia. Petechiae, bruising, bleeding can be appreciated on physical exam

26
Treatment with which of the following medications increases the risk of thrombocytopenia in premature infants: a. Quinidine b. Digoxin c. Indomethacin d. Heparin e. All of the above Quinidine – antiarrythmic, blocks Na channels Digoxin – cardiac medication used to slow the HR in CHF

27
Treatment with which of the following medications increases the risk of thrombocytopenia in premature infants: a. Quinidine b. Digoxin c. Indomethacin d. Heparin e. All of the above Quinidine – antiarrythmic, blocks Na channels Heparin – immune and non immune mediated (nonimmune due to direct effect on plt activation) abnormal ab that activate platelets to clots and low plts Digoxin – immune mediated
 abnormal ab that activate platelets to clots and low plts. Digoxin – immune mediated.")
28
If maternal thrombocytopenia follows drug exposure and is mediated by IgG antibody, the Ab may cross the placenta and affect fetal platelets. Indomethacin and Heparin have been implicated in neonatal thrombocytopenia. Indomethacin – platelet dysfunction Heparin – development of platelet antibodies

29
Thrombocytopenia in a Well, Term Newborn

30
Well, Term Newborn Maternal history
History of immune thrombocytopenic purpura (ITP) or systemic lupus erythematosus (SLE)? Previous infant with thrombocytopenia or family history? Any infections during pregnancy? Drug/medication use during pregnancy? History of HELLP, preeclampsia What is mom’s platelet count? Decreased -- may be autoimmune Normal – may be autoimmune of alloimmune
 or systemic lupus erythematosus (SLE) Previous infant with thrombocytopenia or family history Any infections during pregnancy Drug/medication use during pregnancy History of HELLP, preeclampsia. What is mom’s platelet count Decreased -- may be autoimmune. Normal – may be autoimmune of alloimmune.")
31
(Auto)Immune Thrombocytopenia (1st and early 2nd trimester)
Antibodies coat platelets When traversing the spleen, the platelets are “eaten” by splenic macrophages At birth, infants have minimal splenic function After birth, splenic function increases and risk of severe thrombocytopenia .

32
Splenic Function at Birth
Not functional at birth Howell-Jolly bodies on smear – DNA remnants left over in RBC Usually Howell-Jolly bodies removed on passage of RBC thru spleen

33
Immune Thrombocytopenia
Must follow neonate’s platelet levels closely after birth Especially as splenic function improves Monitoring the fetus during pregnancy and labor is no longer recommended

34
Which immunoglobulin does not cross the placenta?
a. IgA b. IgE c. IgM d. IgG

35
Which immunoglobulin does not cross the placenta?
a. IgA (300,000 D) b. IgE (190,000 D) c. IgM (900,000 D) d. IgG (150,000 D) Which immunoglobulin will not cross the placenta due to size? IgM IgE 190,000 MW IgA 300,000 IgM 900,000 IgG 150,000
 b. IgE (190,000 D) c. IgM (900,000 D) d. IgG (150,000 D) Which immunoglobulin will not cross the placenta due to size IgM. IgE 190,000 MW. IgA 300,000. IgM 900,000. IgG 150,000.")
36
Gestational Thrombocytopenia
Mild and asymptomatic thrombocytopenia No past history of thrombocytopenia (except possibly during a previous pregnancy) Occurrence during late gestation No association with fetal thrombocytopenia Spontaneous resolution after delivery
 Occurrence during late gestation. No association with fetal thrombocytopenia. Spontaneous resolution after delivery.")
37
Gestational Thrombocytopenia
Considered benign Mild and transient ITP? Less antibodies compared to ITP No thrombocytopenia in neonate To make the diagnosis: Thrombocytopenia not severe Occurs during last part of pregnancy/term Platelet count returns to normal after pregnancy Infant’s platelet count is normal

38
The Placenta May reveal: Congenital infection (CMV, syphilis)
Vasculopathy (Preeclampsia) Hemorrhage Infarcts Thrombi Vascular malformations Placenta with syphilis – acute/chronic villitis, spirochetes noted on stain CMV, Herpes – viral inclusions noted with special stains
 Hemorrhage. Infarcts. Thrombi. Vascular malformations. Placenta with syphilis – acute/chronic villitis, spirochetes noted on stain. CMV, Herpes – viral inclusions noted with special stains.")
39
Maternal Pre Eclampsia
Estimated 1 in 100 births Thrombocytopenia, neutropenia in newborns Decreased production Neutrophil, platelet inhibitor Present at birth Nadir is 2-4 days of age

40
Thrombosis If you cannot explain thrombocytopenia, evaluate for clot
Infants with RVT , more likely to have inherited prothrombotic condition like: factor V Leiden mutation, protein C and S deficiency, methylenetetrahydrofolate reductase (MTHFR) mutation, and elevation of lipoprotein
 mutation, and elevation of lipoprotein.")
41
Thrombocytopenia in a Sick, Term Newborn

42
Birth Asphyxia True mechanism is unknown May relate to hypoxia

43
Bacterial Infection Mechanism Disseminated intravascular coagulation
Platelet aggregation caused by bacterial products on platelet membranes Injury to megakaryocytes too Megakaryocyte – giant cell in bone marrow which produces plt

44
Congenital Infection Most common: Others: Cytomegalovirus (CMV)
Toxoplasmosis Herpes Rubella

46
Disseminated Intravascular Coagulation
Systemic process producing: Thrombosis Hemorrhage Characterized by: Prolonged protime (PT) Prolonged activated partial thromboplastin time (PTT) Decrease in fibrinogen Increase in fibrin split products or D-Dimers Decreased platelets Prolonged PT and this INR Fibrinogen – Factor 1 (fibrinogen to fibrin which is a clot) FSP/Ddimer : a small protein fragment present in the blood after a blood clot is degraded by fibrinolysis Preterm infants have hyporeactive plat compared to term infants.
 Prolonged activated partial thromboplastin time (PTT) Decrease in fibrinogen. Increase in fibrin split products or D-Dimers. Decreased platelets. Prolonged PT and this INR. Fibrinogen – Factor 1 (fibrinogen to fibrin which is a clot) FSP/Ddimer : a small protein fragment present in the blood after a blood clot is degraded by fibrinolysis. Preterm infants have hyporeactive plat compared to term infants.")
47
Disseminated Intravascular Coagulation
Due to Sepsis Asphyxia (acidosis) Meconium aspiration Severe respiratory distress syndrome
 Meconium aspiration. Severe respiratory distress syndrome.")
48
Syndromes with Thrombocytopenia

49
Thrombocytopenia, Absent Radii (TAR)
")
51
Kasabach-Merritt Syndrome
Capillary Hemangiomas DIC Thrombocytopenia Shortened platelet survival Sequestration in vascular malformation Tx is pred, vincristine, cyclophosphamide **abnormal endothelium and convoluted architecture of the tumor vasculature promote platelet adhesion and trapping [12]. Platelet aggregation and activation result in thrombocytopenia, consumption of fibrinogen, and ongoing fibrinolysis, leading to intralesional bleeding and tumor enlargement

52
Wiskott-Aldrich Syndrome
X-linked MPV (mean platelet volume) 3-5 fL (nl 7-10) Immunodeficiency Thrombocytopenia Eczema Thrombocytopenia with small platelets This condition primarily affects males. WBC are nonfunctional fL =metric unit of volume equal to 10−15 (femtoliter)
 3-5 fL (nl 7-10) Immunodeficiency. Thrombocytopenia. Eczema. Thrombocytopenia with small platelets. This condition primarily affects males. WBC are nonfunctional. fL =metric unit of volume equal to 10−15 (femtoliter)")
53
Summary Points Neonatal Thrombocytopenia
Platelet levels < 150,000 Neonatal Alloimmune Thrombocytopenia Severely low fetal platelet levels Maternal platelet value – normal Obtain a good accurate specimen Central specimen

55
References NeoReviews Vol. 14 No. 2 February 1, 2013, pp. e74 -e82
Incidence and Consequences of Neonatal Alloimmune Thrombocytopenia: A Systematic Review. Pediatrics Mar 3. Neonatal Thrombocytopenia, Up to Date 2014. Wiedmeier SE, Henry E, Sola-Visner MC, Christensen RD, SO. J Perinatol. 2009;29(2):130
:130.")
Similar presentations