Download presentation
Presentation is loading. Please wait.

1
Stroke In The Young Adult
Victoria E. Judd MD, MBA

3
What Is A Stroke ? A stroke occurs when blood flow to the brain is interrupted by a blocked or a ruptured blood vessel. A brain attack.

4
Stroke Acute stroke is typically characterized by the sudden onset of a focal neurologic deficit, though some patients have a stepwise or gradual progression of symptoms.

5
Stroke Common deficits include: Dysphasia (difficulty swallowing)
Dysarthria (difficulty speaking) Hemianopia (difficulty with sight) Weakness
 Hemianopia (difficulty with sight) Weakness.")
6
Stroke Common Deficits
Ataxia Sensory loss Neglect Consciousness is generally normal but maybe impaired

7
Stroke Warning Signs Sudden weakness or numbness of the face, arm or leg, especially on one side of the body Sudden confusion, trouble speaking or understanding Sudden trouble seeing in one or both eyes

8
Stroke Warning Signs Sudden trouble walking, dizziness, loss of balance or coordination Sudden, severe headaches with no known cause (for hemorrhagic stroke)
")
9
Stroke Warning Signs Acute loss of focal cerebral function
Abrupt onset Symptoms occur in all affected areas at the same time Symptoms resolve gradually Symptoms are “negative”

10
Nature of Symptoms Positive symptoms indicate active discharge from central nervous system neurons. Typical positive symptoms can be visual (e.g., bright lines, shapes, objects), auditory (e.g., tinnitus, noises, music), somatosensory (e.g., burning, pain, paresthesias), or motor (e.g., jerking or repetitive rhythmic movements). Negative symptoms indicate an absence or loss of function, such as loss of vision, hearing, feeling, or ability to move a part of the body.
, auditory (e.g., tinnitus, noises, music), somatosensory (e.g., burning, pain, paresthesias), or motor (e.g., jerking or repetitive rhythmic movements). Negative symptoms indicate an absence or loss of function, such as loss of vision, hearing, feeling, or ability to move a part of the body.")
11
Annual Incidence of Ischemic Stroke
In young adults (15–45 years) has been estimated at approximately 2–11 per 100,000 in Caucasians, 22.8 per 100,000 in African Americans 10/100,000 in a Mayo Clinic study of women ages 15 to 29 About 2–12% of cerebral infarcts occur in young adult patients, with a higher frequency between 31 and 45 years
 has been estimated at approximately 2–11 per 100,000 in Caucasians, 22.8 per 100,000 in African Americans. 10/100,000 in a Mayo Clinic study of women ages 15 to 29. About 2–12% of cerebral infarcts occur in young adult patients, with a higher frequency between 31 and 45 years.")
12
Annual Incidence of Ischemic Stroke
Stroke ranks second after ischemic heart disease as a cause of lost disability-adjusted life-years in high-income countries

13
Mortality of Strokes Mortality in the first month after stroke has been reported to range from 2.5% in patients with lacunar infarcts to 78% in patients with space-occupying hemispheric infarction. Lacunar stroke or lacunar infarct (LACI) is a type of stroke that results from occlusion of one of the penetrating arteries that provides blood to the brain's deep structures.
 is a type of stroke that results from occlusion of one of the penetrating arteries that provides blood to the brain s deep structures.")
14
Stroke Stroke in young adults is surprisingly common.
The differential diagnosis for potential etiologies is broader than that for older adults.

15
Stroke In children and young adults;
Congenital and acquired heart problems, Hematologic conditions, Vasculopathies, Metabolic disorders, Drug ingestion are more common.

16
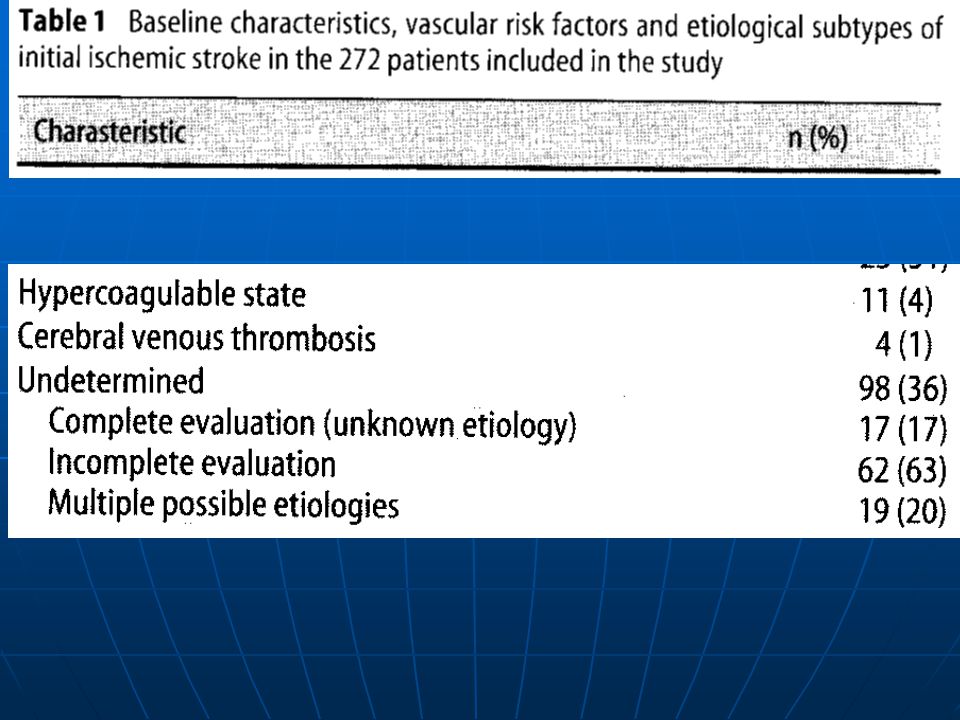
Causes of Stroke The largest series studies of young adults with ischemic stroke cite undetermined as the most frequent etiology (up to 35% of patients) Ischemic stroke is much more common than hemorrhagic
 Ischemic stroke is much more common than hemorrhagic.")
17
Causes of Stroke Up to 45% of strokes in young adults are due to spontaneous intracerebral hemorrhage. Vascular malformations, aneurysms, hypertension, and illicit drug use are the main causes.

18
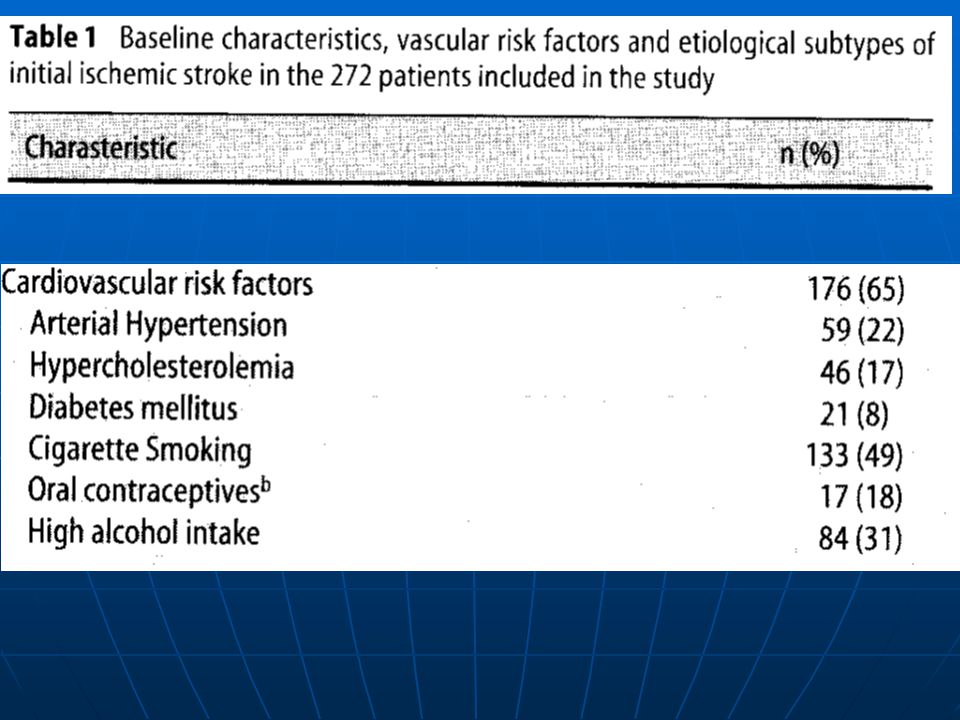
Causes of Ischemic Stroke in Young Adults Eur Neurol 2007;57:212–218

19
Cardiovascular Risk Factors in 272 Young Patients % (n)
Major cardiovascular risk factors 35 (96) Arterial hypertension 22 (59) Diabetes mellitus 8 (21) Hypercholesterolemia 17 (46) Atherosclerosis 5 (14) Causes of Ischemic Stroke in Young Adults Eur Neurol 2007;57:212–218
 Arterial hypertension 22 (59) Diabetes mellitus 8 (21) Hypercholesterolemia 17 (46) Atherosclerosis 5 (14) Causes of Ischemic Stroke in Young Adults Eur Neurol 2007;57:212–218.")
20
Cardiovascular Risk Factors in 272 Young Patients % (n)
Minor cardiovascular risk factors 63 (172) Cigarette smoking 49 (133) Oral contraceptives 18 (17) High alcohol intake 31 (84) Causes of Ischemic Stroke in Young Adults Eur Neurol 2007;57:212–218
 Cigarette smoking 49 (133) Oral contraceptives 18 (17) High alcohol intake 31 (84) Causes of Ischemic Stroke in Young Adults Eur Neurol 2007;57:212–218.")
21
Prevention of Stroke Control high blood pressure Prevent heart disease
Stop cigarette smoking Recognize signs of TIA Reduce blood cholesterol levels

22
Stroke Risk Factors That Can Be Treated
Hypertension/High Blood Pressure Heart Disease Cigarette Smoking Transient Ischemic Attacks

23
Stroke Risk Factors That Can Be Treated
Diabetes Elevated Blood Cholesterol/Lipids Asymptomatic Carotid Bruits

24
Stroke Risk Factors That Cannot Be Treated
Age Gender Race Prior stroke Family history

25
Stroke Risk Factors Less Well-Documented
Geographical Location Socioeconomic Factors Excessive Alcohol Intake Certain Kinds of Drug Abuse

26
What Are the Types of Stroke ?
Ischemic Stroke (Blockage) • Caused by a blockage in blood vessels in brain Hemorrhagic Stroke (Bleeding) • Caused by ruptured or leaking blood vessels in brain
 • Caused by a blockage in blood vessels in brain. Hemorrhagic Stroke (Bleeding) • Caused by ruptured or leaking blood vessels in brain.")
27
Stroke Background Inadequate blood flow Hemorrhage Ischemic stroke
Focal – thrombotic or embolic occlusion of major artery Global – inadequate cerebral perfusion Hemorrhage Parenchymal – into brain tissue Subarachnoid – surrounding subarachnoid space

29
Causes of Stroke Some of the most common causes of ischemia in the young Cardioembolism (20–35%), Dissection of extracranial arteries (6–25%), Migraine with aura (1–20%) Drugs (10%) Hypercoagulable states (5–10%) Premature atherosclerosis (20-25%)
, Migraine with aura (1–20%) Drugs (10%) Hypercoagulable states (5–10%) Premature atherosclerosis (20-25%)")
30
Ischemic Stroke In patients younger than 55 years, only about 10% of strokes are caused by large-vessel atherosclerotic disease.

31
What Are the Causes of Ischemic Stroke?
Large vessel disease Premature atherosclerosis Dissection (spontaneous or traumatic) Inherited metabolic diseases (homocystinuria, Fabry’s, pseudoxanthoma elasticum, MELAS syndrome) Fibromuscular dysplasia Infection (bacterial, fungal, tuberculosis, syphilis, Lyme) Vasculitis (collagen vascular diseases — systemic lupus erythematosus, rheumatoid arthritis, Sjögren’s syndrome, polyarteritis nodosa; Takayasu’s disease, Wegener’s syndrome, cryoglobulinemia, sarcoidosis, inflammatory bowel disease, isolated central nervous system angiitis) Moyamoya disease: (Japanese, "puff of cigar smoke") is an inherited disease in which certain arteries in the brain are constricted Radiation Toxic (illicit drugs — cocaine, heroin, phencyclidine; therapeutic drugs — L-asparaginase, cytosine arabinoside, ephedra, phenylephrine)
 Inherited metabolic diseases (homocystinuria, Fabry’s, pseudoxanthoma elasticum, MELAS syndrome) Fibromuscular dysplasia. Infection (bacterial, fungal, tuberculosis, syphilis, Lyme) Vasculitis (collagen vascular diseases — systemic lupus erythematosus, rheumatoid arthritis, Sjögren’s syndrome, polyarteritis nodosa; Takayasu’s disease, Wegener’s syndrome, cryoglobulinemia, sarcoidosis, inflammatory bowel disease, isolated central nervous system angiitis) Moyamoya disease: (Japanese, puff of cigar smoke ) is an inherited disease in which certain arteries in the brain are constricted. Radiation. Toxic (illicit drugs — cocaine, heroin, phencyclidine; therapeutic drugs — L-asparaginase, cytosine arabinoside, ephedra, phenylephrine)")
32
What Are the Causes of Ischemic Stroke?
Cardiac disease (including congenital, rheumatic valve disease, mitral valve prolapse, patent foramen ovale, endocarditis, atrial myxoma, arrhythmias, cardiac surgery)
")
33
What Are the Causes of Ischemic Stroke?
Small vessel disease Vasculopathy (infectious, noninfectious, microangiopathy) Independent predictors of arteriopathy are sickle cell disease and recent upper respiratory infection.
 Independent predictors of arteriopathy are sickle cell disease and recent upper respiratory infection.")
34
What Are the Causes of Ischemic Stroke?
Hematologic disease Sickle-cell disease Leukemia Hypercoagulable states (antiphospholipid antibody syndrome, deficiency of antithrombin III or protein S or C, resistance to activated protein C, increased factor VIII) Disseminated intravascular coagulation Thrombocytosis Polycythemia vera Thrombotic thrombocytopenic purpura Venous occlusion (dehydration, parameningeal infection, meningitis, neoplasm, polycythemia, leukemia, inflammatory bowel disease)
 Disseminated intravascular coagulation. Thrombocytosis. Polycythemia vera. Thrombotic thrombocytopenic purpura. Venous occlusion (dehydration, parameningeal infection, meningitis, neoplasm, polycythemia, leukemia, inflammatory bowel disease)")
35
Hematologic Disorders
Many hematologic disorders are associated with ischemic stroke. The disorders most likely to cause ischemic stroke in patients younger than 45 years are: Antiphospholipid antibody syndrome Sickle cell anemia Heparin induced thrombocytopenia

36
APS Antiphospholipid syndrome (APS or APLS) or antiphospholipid antibody syndrome is a disorder of coagulation that causes blood clots (thrombosis) in both arteries and veins as well as pregnancy-related complications such as miscarriage, stillbirth, preterm delivery, or severe preeclampsia. The syndrome occurs due to the autoimmune production of antibodies against phospholipid (aPL), a cell membrane substance. In particular, the disease is characterized by antibodies against cardiolipin (anti-cardiolipin antibodies) and β2 glycoprotein.
 or antiphospholipid antibody syndrome is a disorder of coagulation that causes blood clots (thrombosis) in both arteries and veins as well as pregnancy-related complications such as miscarriage, stillbirth, preterm delivery, or severe preeclampsia. The syndrome occurs due to the autoimmune production of antibodies against phospholipid (aPL), a cell membrane substance. In particular, the disease is characterized by antibodies against cardiolipin (anti-cardiolipin antibodies) and β2 glycoprotein.")
37
Hematologic disorders
Most of the common hereditary hypercoagulable disorders, such as factor V Leiden/activated protein C resistance, the prothrombin gene mutation (G20210A), antithrombin III deficiency, protein C deficiency, and protein S deficiency, typically cause venous thrombosis much more often than they cause arterial thrombosis.
, antithrombin III deficiency, protein C deficiency, and protein S deficiency, typically cause venous thrombosis much more often than they cause arterial thrombosis.")
38
What Are the Causes of Ischemic Stroke?
Migraine: especially with aura

39
Embolism: Cardiogenic (atrial fibrillation, mural thrombus, myxoma, valvular vegetations) Artery-to-artery Fat Air Paradoxical (emboli of venous origin passing through a patent foramen ovale)
")
40
Cardiogenic Embolism Major risk factors: Anticoagulation Indicated
Atrial fibrillation Mitral stenosis Prosthetic cardiac valve Recent MI Thrombus in LV or LA appendage Atrial myxoma Infective endocarditis (No anticoagulation) Dilated cardiomyopathy
 Dilated cardiomyopathy.")
41
Cardiogenic Embolism Minor risk factors: Best treatment unclear
Pathologic Mitral valve prolapse (2% of population) Mitral annular calcification Patent foramen ovale (25% 0f population) Atrial septal aneurysm Calcific aortic stenosis LV regional wall motion abnormality Aortic arch atheromatous plaques Spontaneous echocardiographic contrast
 Mitral annular calcification. Patent foramen ovale (25% 0f population) Atrial septal aneurysm. Calcific aortic stenosis. LV regional wall motion abnormality. Aortic arch atheromatous plaques. Spontaneous echocardiographic contrast.")
42
Cardiogenic Embolism One-fifth to one-third of strokes in the young may be caused by cardioembolic phenomena.

43
Cardiogenic Embolism Paradoxical embolization from the right heart to the left is believed to occur via a patent foramen ovale or atrial septal defect (which can be found on autopsy in up to one fourth of all people. Atherosclerosis of the aorta or carotid arteries can be a source of both atheroemboli and thromboemboli

44
Cardiogenic Embolism Left atrial thrombi account for nearly half of cardiac thromboemboli. The most common cause is atrial fibrillation; other causes are dilated cardiomyoapthy, mitral valve stenosis, and some hypercoagulable states.

45
Left atrium Left atrium Right atrium Valsalva Figure 1. Transesophageal Echocardiograms of a Patent Foramen Ovale. In Panel A, a transesophageal echocardiogram in the longitudinal plane shows a separation between the primum septum (arrowhead) and the secundum septum — a finding consistent with the presence of patent foramen ovale. Panel B shows a transesophageal echocardiogram, also in the longitudinal plane, obtained during the injection of agitated-saline contrast material through an antecubital vein with use of the Valsalva maneuver. There is complete opacification of the right atrium, and passage of a cloud of bubbles between the primum and secundum septa into the left atrium is visible. Right atrium
 and the secundum septum — a finding consistent with the presence of patent foramen ovale. Panel B shows a transesophageal echocardiogram, also in the longitudinal plane, obtained during the injection of agitated-saline contrast material through an antecubital vein with use of the Valsalva maneuver. There is complete opacification of the right atrium, and passage of a cloud of bubbles between the primum and secundum septa into the left atrium is visible. Right atrium.")
46
RA LA Figure 2. Transesophageal echocardiogram showing a thrombus (arrows) passing from right atrium (RA) to left atrium (LA) through a patent foramen ovale.
 passing from right atrium (RA) to left atrium (LA) through a patent foramen ovale.")
47
Left atrium Left atrium Right atrium Right atrium Left ventricle Right ventricle Figure 2. Transesophageal Echocardiograms of an Atrial Septal Aneurysm. In Panel A, a transesophageal echocardiogram (in the horizontal plane) shows an atrial septal aneurysm protruding into the right atrium (arrow). Atrial septal aneurysm is defined as either sustained bowing of a 15-mm segment of interatrial septal membrane in the fossa ovalis of at least 11 mm (or at least 15 mm by a more conservative definition) beyond the plane of the interatrial septum or as phasic excursion to either side totaling the same distance. Panel B shows a transesophageal echocardiogram showing the same atrial septal aneurysm (arrow) viewed in the longitudinal plane.
 shows an atrial septal aneurysm protruding into the right atrium (arrow). Atrial septal aneurysm is defined as either sustained bowing of a 15-mm segment of interatrial septal membrane in the fossa ovalis of at least 11 mm (or at least 15 mm by a more conservative definition) beyond the plane of the interatrial septum or as phasic excursion to either side totaling the same distance. Panel B shows a transesophageal echocardiogram showing the same atrial septal aneurysm (arrow) viewed in the longitudinal plane.")
48
PFO Figure 3. Percutaneous Closure of a Patent Foramen Ovale.
With use of a femoral approach, a transvenous sheath is advanced across the foramen into the left atrium, where a folded disk is expanded and pulled back, apposing the primum and secundum septa closed. This step is followed by deployment of a right-sided disk, at which time the two-disk device is released. Clopidogrel and aspirin are recommended for a period of three months to prevent thrombus formation on the device, with aspirin therapy continued for an additional three months, when endothelialization is complete. Antibiotic prophylaxis for six months is recommended. Complete late closure of the foramen has been reported in 80 to 95 percent of patients.

51
Cocaine Abuse Another important cause of ischemic stroke is the use of sympathomimetic drugs such as cocaine amphetamines, ephedra, or phenylephrine. The strongest association is with cocaine, which has been seen in case series to cause cerebral vasoconstriction in a dose-dependent manner. Vasoconstriction is also related to a longer duration of cocaine use. Several case-control studies have found that the risk of stroke is 4.5 to 6.5 times higher in drug abusers than in controls, and that use of catecholamines or cocaine alone was associated with a significantly increased risk of stroke.

52
What Are the Causes of Hemorrhagic Stroke?
Occurs when a weakened blood vessel ruptures • Aneurysms: Ballooning of a weakened region of a blood vessel • Arteriovenous Malformations (AVMs): Cluster of abnormal blood vessels
: Cluster of abnormal blood vessels.")
53
Arteriovenous Malformations
Cerebral AVMs are most commonly discovered in young adults aged years. These lesions are usually detected in patients as the result of a seizure or hemorrhage. AVMs hemorrhage at a rate of 4% per year. Approximately half of these hemorrhages will carry significant morbidity or mortality.

54
HEMORRHAGIC Arteriovenous malformation
Neoplasm (primary central nervous system, metastatic, leukemia) Hematologic (sickle-cell disease, neoplasm, thrombocytopenia) Moyamoya disease Drug use (warfarin, amphetamines, cocaine, phenypropanolamine) Iatrogenic (peri-procedural)
 Hematologic (sickle-cell disease, neoplasm, thrombocytopenia) Moyamoya disease. Drug use (warfarin, amphetamines, cocaine, phenypropanolamine) Iatrogenic (peri-procedural)")
55
Moyamoya Moyamoya syndrome is characterized by progressive stenosis of the internal carotid arteries and formation of collateral vessels that give a "puff of smoke" appearance on angiography. Moyamoya disease occurs mainly in Japanese and other Asian populations and may have a genetic basis. Secondary moyamoya syndrome is seen in association with neurofibromatosis, Down syndrome, Williams syndrome, sickle cell disease, and as a sequela of cranial irradiation. Intracranial hemorrhage is common in young adults. Dissection — Arterial dissection is the most common vascular abnormality in some young adult series

56
Intracerebral Hemorrhage
Diffuse – subarachnoid hemorrhage Focal – intraparenchymal Accounts for 20% of all strokes Acute rise in intracranial pressure from arterial rupture frequently results in loss of consciousness at outset Some patients die from herniation

57
Causes of Spontaneous Intracerebral Hemorrhage (ICH)
Intraparenchymal hemorrhage Trauma Hypertension Amyloid angiopathy Arteriovenous malformation Bleeding diathesis (anticoagulants, thrombolytics) Drugs (amphetamines, cocaine)
 Drugs (amphetamines, cocaine)")
58
Causes of Spontaneous Intracerebral Hemorrhage (ICH)
Cervical arterial dissection causes up to 20% of strokes in patients younger than 45 years. Dissections usually involve the extracranial portion of the vessel, and involve the internal carotid arteries at least three times as often as the vertebral arteries.

59
Causes of Spontaneous Intracerebral Hemorrhage (ICH)
In many cases the dissection is preceded by mild neck trauma, which may be as minor as a vigorous cough or turning of the head. Typical features of dissection include: Neck pain, headache, and Horner syndrome, followed minutes to hours later by symptoms of ocular or cerebral ischemia, usually a transient ischemic attack rather than a stroke.

60
Causes of Spontaneous Intracerebral Hemorrhage (ICH)
Inherited disorders that are associated with increased risk of cervical arterial dissection include: Ehlers-Danlos syndrome type IV Marfan syndrome Autosomal dominant polycystic kidney disease Osteogenesis imperfecta type I Fibromuscular dysplasia

61
Diagnosis, Management, and Prognosis of ICH
CT diagnostic test of choice Hyperintense area with mass effect and later hypointense surrounding edema MRI less sensitive in early stages

62
Diagnosis, Management, and Prognosis of ICH
Management depends on size and location In acute phase, mass effect far greater than in large cerebral infarction, so greater risk of herniation and death In chronic phase, prognosis for surviving patients much better than with ischemic stroke

63
Subarachnoid Hemorrhage
Aneurysms can rupture any time but more common during strenuous activity Most common manifestation is headache “worst headache of my life” Neck pain and rigidity Loss of consciousness and vomiting common Seen on CT in 95% of cases – location may suggest site of rupture Normal CT does not rule out so do lumbar puncture – xanthochromia (develops after 6 hours)
")
64
Causes of Spontaneous Intracerebral Hemorrhage (ICH)
Subarachnoid hemorrhage Congenital saccular aneurysm (85%) Unknown (15%)
 Unknown (15%)")
65
What Parts of the Brain Are Affected by Stroke?

66
Right (Non-dominant) Hemisphere Stroke: Common Pattern
Neglect of left visual field Extinction of left-sided stimuli Left hemiparesis Left-sided sensory loss Left visual field defect Poor left conjugate gaze Dysarthria Spatial disorientation

67
Left (Dominant) Hemisphere Stroke: Common Pattern
Aphasia Right hemiparesis Right-sided sensory loss Right visual field defect Poor right conjugate gaze Dysarthria Difficulty reading, writing, or calculating

68
Brain Stem / Cerebellum / Posterior Hemisphere Stroke: Common Pattern
Motor or sensory loss in all four limbs Crossed signs Limb or gait ataxia Dysarthria Dysconjugate gaze Nystagmus Amnesia Bilateral visual field defects

69
Small Subcortical Hemisphere or Brain Stem Stroke: Common Pattern
Pure Motor Weakness of face and limbs on one side of the body without abnormalities of higher brain function, sensation, or vision Pure Sensory Decreased sensation of face and limbs on one side of the body without abnormalities of higher brain function, motor function, or vision

70
Physical Exam Neurologic Exam Carotid Bruits Cardiac Exam
Peripheral Pulses Dermatologic Ophthalmologic

71
Dermatologic Splinter hemorrhages and needle tracks (endocarditis)
Xanthoma (hyperlipidemia) Café-au-lait spots Neurofibromas (neurofibromatosis) Purpura (coagulopathy) Capillary angiomata (cavernous malformation)
 Café-au-lait spots. Neurofibromas (neurofibromatosis) Purpura (coagulopathy) Capillary angiomata (cavernous malformation)")
72
Xanthoma, eruptive CAFÉ AU LAIT spots Neurofibromas splinter hemorrhages

73
Opthalmlogic Corneal arcus (hypercholesterolemia)
Corneal opacity (Fabry’s disease) Lisch nodules Optic atrophy (neurofibromatosis) Lens subluxation (Marfan’s syndrome, homocystinuria) Retinal perivasculitis (sickle-cell disease, syphilis, connective tissue diseases, inflammatory bowel disease) Occlusions (emboli) Angioma (cavernous malformation) Hamartoma (tuberous sclerosis).
 Lisch nodules. Optic atrophy (neurofibromatosis) Lens subluxation (Marfan’s syndrome, homocystinuria) Retinal perivasculitis (sickle-cell disease, syphilis, connective tissue diseases, inflammatory bowel disease) Occlusions (emboli) Angioma (cavernous malformation) Hamartoma (tuberous sclerosis).")
74
Corneal arcus optic atrophy in tuberous sclerosis lens dislocation in marfan syndrome

75
Diagnostic Testing for Patients With Stroke
Basic stroke evaluation Cranial computed tomography (CT) Carotid ultrasonography ± transcranial Doppler Transthoracic echocardiography EKG monitoring Routine blood studies (complete blood count with differential and platelet count, prothrombin time (international normalized ratio), activated partial thromboplastin time, glucose, chemistries, serology for syphilis, and an erythrocyte sedimentation rate)
 Carotid ultrasonography ± transcranial Doppler. Transthoracic echocardiography. EKG monitoring. Routine blood studies (complete blood count with differential and platelet count, prothrombin time (international normalized ratio), activated partial thromboplastin time, glucose, chemistries, serology for syphilis, and an erythrocyte sedimentation rate)")
76
Diagnostic Testing for Patients With Stroke
Comprehensive stroke evaluation Cranial magnetic resonance imaging (MRI) Imaging of the intracranial arteries (MR, CT, or catheter angiography of the brain) Imaging of the extracranial arteries (MR, CT, or catheter angiography of the neck) Transesophageal echocardiography (TEE) Prolonged EKG monitoring with Holter or event loop recorder Urine toxicology screen (often productive) Urine pregnancy test Blood testing for a hypercoagulable state anticardiolipin antibodies, lupus anticoagulants, protein S, protein C, activated protein C resistance, antithrombin III) is requested in patients without a firmly identified cause of stroke or if the patient or family members have a history of thromboses. It is advantageous to send such a profile prior to initiating anticoagulation, as heparin can alter interpretation of some of those assays. In select cases, blood testing for rare genetic causes of stroke (CADASIL, Fabry disease, MELAS)
 Imaging of the intracranial arteries (MR, CT, or catheter angiography. of the brain) Imaging of the extracranial arteries (MR, CT, or catheter angiography. of the neck) Transesophageal echocardiography (TEE) Prolonged EKG monitoring with Holter or event loop recorder. Urine toxicology screen (often productive) Urine pregnancy test. Blood testing for a hypercoagulable state anticardiolipin antibodies, lupus anticoagulants, protein S, protein C, activated protein C resistance, antithrombin III) is requested in patients without a firmly identified cause of stroke or if the patient or family members have a history of thromboses. It is advantageous to send such a profile prior to initiating anticoagulation, as heparin can alter interpretation of some of those assays. In select cases, blood testing for rare genetic causes of stroke (CADASIL, Fabry disease, MELAS)")
77
How Are Strokes Treated?
Ischemic Stroke • Clot-busters e.g., t-PA • Anticoagulants – warfarin, aspirin Carotid Endarterectomy Angioplasty/Stents

78
Treatment of Strokes Antiplatelet therapy remains treatment of choice to prevent recurrent thromboembolism in majority of patients Anticoagulation may be appropriate Atrial fibrillation Recent MI Suspected propagation of thrombus or stroke in evolution

79
Treatment of Strokes CT or MRI of the brain should be performed promptly; MRI is more sensitive for early ischemic changes, but either method can fully rule out hemorrhage. Treatment of TPA was associated with an increase of about 1.2 with minimal or no disability for every 10 patients treated.

80
Limitations of Imaging
CT will miss a minority of acute bleeds MRI with DWI (diffusion weighted imaging), quite sensitive for acute stroke, has an occasional false negative result (17 out of 782 patients in a recent study) MRA’s resolution is not yet on par with conventional angiography.
, quite sensitive for acute stroke, has an occasional false negative result (17 out of 782 patients in a recent study) MRA’s resolution is not yet on par with conventional angiography.")
81
Thrombolysis t-PA Guidelines for treatment:
Present within 3 hours of onset of clearly defined stroke – frequency of symptomatic hemorrhage most likely increases after this time CT scan shows no evidence of intracranial hemorrhage No anticoagulants or antiplatelet agents given for 24 hours Avoid BP values > 185/110

82
Guidelines Not to Treat
Previous stroke or serious head trauma in preceding 3 months History of intracranial hemorrhage Repeated systolic BP’s > 185 mm Hg or diastolic BP’s > 110 mm Hg

83
Guidelines Not to Treat
Requires aggressive treatment to reduce BP to specified limits Taking anticoagulants or propensity to hemorrhage Recent invasive surgical procedure Rapidly improving neurological deficit or minor symptoms

84
How Are Strokes Treated
Hemorrhagic Stroke Surgical Intervention Endovascular Procedures, e.g., “coils”

86
What Is the Impact of Stroke?
Stroke is the third leading cause of death in the United States • On average, someone suffers a stroke every 40 seconds • About 795,000 Americans suffer a stroke each year • About every 4 minutes, someone dies of a stroke

87
What Is the Impact of Stroke?
Stroke is a leading cause of serious, long term disability About 6.4 million Americans are stroke survivors Americans will pay about $73.7 billion in 2010 for stroke-related medical costs and lost productivity long-term

88
Rehabilitation After suffering a stroke, it’s important to begin a rehabilitation program as soon as possible. Types of rehabilitation programs: Hospital programs Extended care facilities Outpatient programs Home-based programs

89
Rehabilitation Specialists
Provider Rehabilitation specialist Physical therapist Speech therapist Occupational therapist Physiatrist Psychiatrist

90
Family Relationships Overall, 13 studies reported consequences of stroke for family relationships and in those studies, 5% to 54% of the samples experienced family problems. Nine studies reported marital problems after stroke, including separation or divorce. Six of these reported that marital problems were a direct consequence of the stroke. One study reported that 5% of the sample had experienced deterioration in the spousal relationship, whereas another found that 38% of couples had experienced conflict since the stroke.

91
Sexual Relationships Ten studies investigated the impact of stroke on sexual relationships, reporting problems in participants’ sexual relationships or frequency of sexual activities. Prevalence of deterioration in sexual relationships reported in 8 studies ranged from 5% to 76%.

92
Social Activities Nine studies reported consequences of stroke on social or leisure activities with 4 of these reporting deterioration or decrease in these activities. Five studies quantified reported decrease in leisure activities ranging from 15% to 79%.

104
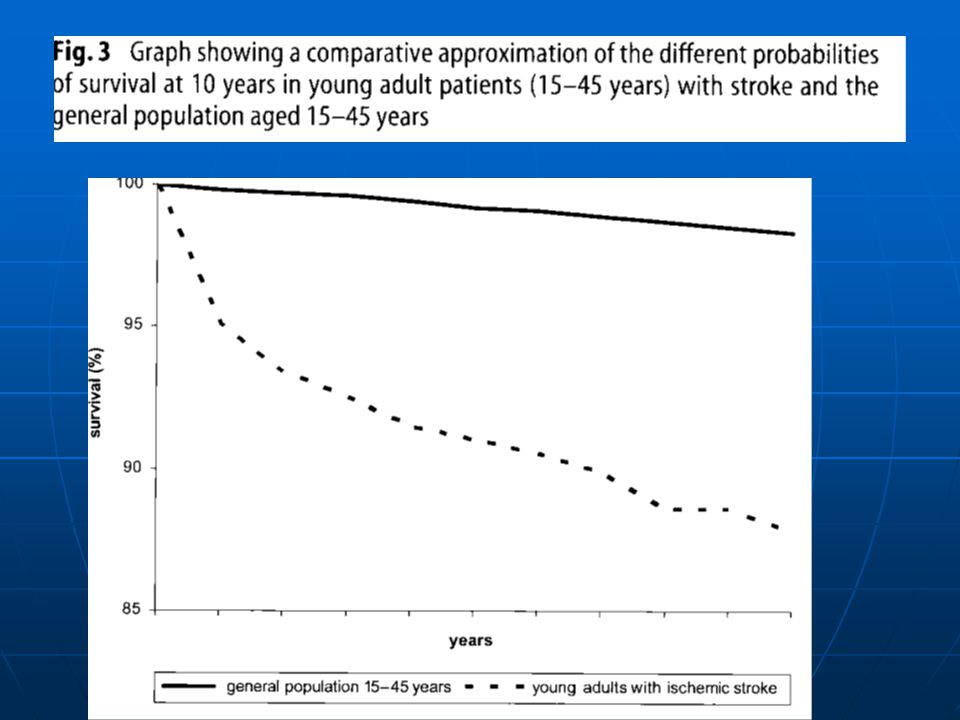
Prognosis The outcome of stroke in young adults is better than that for older adults. In a recent study of 330 patients with first stroke or transient ischemic attack, followed for an average of 96 months, 8% died, 3% had another stroke, and 3% had a myocardial infarction. Approximately 16% were dependent, but 56% had returned to work. Unfortunately, only a minority of those who smoked at the time of their stroke subsequently stopped using tobacco. The overall annual recurrence rate is less than 1%. Prognosis is often closely associated with the underlying cause. A relatively good outcome may be found after many cases of arterial dissection. Risk of stroke recurrence is low (2% over 5 years) in women whose first stroke occurred in pregnancy.
 in women whose first stroke occurred in pregnancy.")
107
Stroke Chameleons Strokes with atypical presentations that take on the appearance of other disease process may be termed stroke chameleons, for like the chameleon, these disguised strokes may change and evolve with time. The provider is left with the daunting problem of discovering the unusual manifestation of an uncommon clinical process. The presence of historical risk factors for cerebrovascular disease and the abrupt onset of symptoms may be the best clues available to the provider to detect these unusual stroke syndromes.

108
Stroke Chameleons In the majority of cases of stroke, making the diagnosis is straightforward. Especially in patients with unusual features (e.g., Gradual onset, Seizure at the onset of symptoms Impaired consciousness The differential diagnosis should include migraine, postictal paresis, hypoglycemia, conversion disorder, subdural hematoma, and brain tumors.

109
Stroke Chameleons Atherosclerosis (leading to thromboembolism or local occlusion) and cardioembolism are the leading causes of brain ischemia. Unusual causes should be considered, especially if patients are younger (e.g., below 50 years of age) and have no apparent cardiovascular risk factors. Some clinical clues that suggest alternative diagnoses are ptosis and miosis contralateral to the deficit (carotid-artery dissection), fever and a cardiac murmur (infective endocarditis), and headache and an elevated erythrocyte sedimentation rate.
 and have no apparent cardiovascular risk factors. Some clinical clues that suggest alternative diagnoses are ptosis and miosis contralateral to the deficit (carotid-artery dissection), fever and a cardiac murmur (infective endocarditis), and headache and an elevated erythrocyte sedimentation rate.")
110
Differential Diagnosis
Seizures and migraine auras characteristically (but not always) begin with positive symptoms, while TIAs invariably are characterized by negative symptoms. Seizures occasionally cause paralytic attacks but, on close observation, there are usually features of the history and physical examination that suggest the presence of a seizure disorder such as minor twitching of a finger or toe or a tingling sensation in the affected limb.
 begin with positive symptoms, while TIAs invariably are characterized by negative symptoms. Seizures occasionally cause paralytic attacks but, on close observation, there are usually features of the history and physical examination that suggest the presence of a seizure disorder such as minor twitching of a finger or toe or a tingling sensation in the affected limb.")
111
Differential Diagnosis of Stroke
Intracranial mass: Tumor, Subdural hematoma Seizure with persistent neurological signs Migraine with persistent neurological signs Metabolic

112
Differential Diagnosis of Stroke
Hyperglycemia (nonketotic hyperosmolar coma) Hypoglycemia Post-cardiac arrest ischemia Drug/narcotic overdose
 Hypoglycemia. Post-cardiac arrest ischemia. Drug/narcotic overdose.")
113
Focal symptoms Nonfocal symptoms Common disorders Seizures ++ TIAs ++++ occasionally Migraine Syncope Less common disorders Vestibulopathy Metabolic + +++ "Tumor attacks" Multiple sclerosis Psychiatric Nerves and nerve root Transient global amnesia

114
Differential Diagnosis of Transient Neurological Diseases
Seizure Migraine with aura Syncope Hypoglycemia

115
Hypoglycemia That transient hypoglycemia may produce a stroke like picture with hemiplegia and aphasia has been known for years. These patients may be drowsy but are often alert and do not show the more common response to hypoglycemia of confusion, diminished level of consciousness, or coma. Aphasia may make the history of diabetes more difficult to discover. Syndrome has also been reported in alcoholics with hypoglycemia. The pathogenesis of this focal CNS dysfunction is unclear. Hypoglycemia is generally defined as a blood glucose level of less than 45 mg/dl in these studies. The wide use of bedside rapid laboratory testing for glucose now makes this easily detectable and treatable. The hemiplegia may resolve immediately with the administration of intravenous glucose but resolution over a hours is also reported.

116
Mass Lesions Subdural hematoma, cerebral abscess, primary CNS tumors, and metastatic tumors are among the clinical conditions simulating stroke in the studies cited above. The typical clinical presentation of a slowly increasing mass is a progressive syndrome; an abrupt onset of symptoms of these masses seems counter-intuitive. A review of patients with brain tumors presenting to an ED showed that 6% of patients had symptoms that were of less than one day’s duration; it was thought that these patients with brief symptom duration might reflect a sub-population who suffer acute deterioration from hemorrhage into the tumor or who develop obstructive hydrocephalus. Secondary effects of mass or edema on cerebral vasculature have been identified as possible causes of abrupt onset of seizures as well. Chronic subdural hematoma has been frequently reported as a cause of stroke and TIA-like symptoms.

117
Functional Hemiparesis
Little is written about a factitious or feigned stroke yet several studies discover rare patients initially thought to have cerebrovascular disease but later determined to have a functional cause of the hemiparesis or other stroke syndrome. Conversion disorder is the most commonly assigned psychiatric disorder. One study of emergency department presentations of conversion disorder noted that symptoms of paresis, paralysis, or movement disorders were common and were a presentation in almost 30% of patients. They noted significant comorbidity in this population, often other psychiatric disorders, and emphasized that conversion disorder is a diagnosis of exclusion. Patients often undergo multiple diagnostic tests before the diagnosis is assigned.

118
Seizures Demographics
Any age, often younger

119
Seizures CNS Symptoms Light-headed, dim vision, noises distant, decreased alertness Transient loss of consciousness

120
Seizures CNS Symptoms Positive symptoms: limb jerking, head turning, loss of consciousness Negative symptoms may develop, remain postictally, and persist

121
Seizures Timing 20 to 80 seconds
Absence, atonic seizures and myoclonic jerks are shorter Postictal depression Spells occur over years

122
Seizures Associated Symptoms
Tongue biting, incontinence, sore muscles, headache after attack

123
Focal Seizure Partial (focal) seizure
Positive sensory or motor symptoms Spread quickly (60 seconds) Negative symptoms afterward (Todd’s paresis) Multiple attacks
 Negative symptoms afterward (Todd’s paresis) Multiple attacks.")
124
What is a TIA Acute loss of focal cerebral function
Symptoms last less than 24 hours Due to inadequate blood supply Thrombosis Embolism

125
Transient Ischemic Attacks (TIAs)
Warning strokes” that can happen before a major stroke Occur when blood flow through a brain artery is blocked or reduced for a short time Symptoms are temporary (<24 hours) but similar to those of a full fledged stroke A person who has a TIA is 9.5 times more likely to have a stroke
 but similar to those of a full fledged stroke. A person who has a TIA is 9.5 times more likely to have a stroke.")
126
TIA Risk Factors/Epidemiology
300,000 TIAs per year in US 5-year stroke risk after TIA 29% 43.5% in 2 years with >70% carotid stenosis treated medically Many stroke patients have had a TIA 25% - 50% in large artery atherothrombotic strokes 11% - 30% in cardioembolic strokes 11% to 14% in lacunar strokes

127
Risk Factors for a TIA Risk factors are the same as stroke
Increasing age Sex Family history / Race Prior stroke / TIA Hypertension Diabetes Heart disease Carotid artery / Peripheral artery disease Obesity High cholesterol Physical inactivity

128
TIA Symptoms Symptoms last less than 24 hours
Most last less than one hour Less than 10 percent > 6 hours Amaurosis fugax up to five minutes (Amaurosis fugax is loss of vision in one eye due to a temporary lack of blood flow to the retina. Symptoms include the sudden loss of vision in one eye.)
")
129
TIA Demography Older patients Stroke risk factors present Men>women

130
TIA Presentation Acute loss of focal cerebral function Abrupt onset
Symptoms occur in all affected areas at the same time Symptoms resolve gradually Symptoms are “negative”

131
TIA Presentation Acute loss of focal cerebral function Motor symptoms
Weakness or clumsiness on one side Difficulty swallowing Speech disturbances Understanding or expressing spoken language Reading or writing Slurred speech Calculations

132
TIA Presentation Acute loss of focal cerebral function
Sensory symptoms Altered feeling on one side Loss of vision on one side Loss of vision in left or right visual field Bilateral blindness Double vision Vertigo

133
TIA Presentation Non-focal Symptoms (Not TIA)
Generalized weakness or numbness Faintness or syncope Incontinence Isolated symptoms (symptoms occurring alone) Vertigo or loss of balance Slurred speech or difficulty swallowing Double vision
 Vertigo or loss of balance. Slurred speech or difficulty swallowing. Double vision.")
134
TIA Presentation Non-focal Symptoms (Not TIA) Confusion Disorientation
Impaired attention/concentration Diminution of all mental activity Distinguish from Isolated language or visual-spatial perception problems (may be TIA) Isolated memory problems (transient global amnesia)
 Isolated memory problems (transient global amnesia)")
135
TIA Significant risk factor for recurrent stroke, with average 5% risk per year Prophylactic antiplatelet therapy shown to prevent secondary effects Aspirin Ticlopidine: thrombotic stroke reduction Clopidogrel: reduce events associated with atherosclerosis that include strokes, MI, PVD

136
TIA Treat with warfarin if significant risk for cardiogenic thromboembolism Hospital admission for new-onset and recurrent TIA’s unless confident in diagnosis of etiology Angiography – treat medically or surgically

137
TIA Usually minutes, mostly <1 hour
Spells during days, weeks, months; not usually years

138
TIA Associated Symptoms
Headaches may occur during time period of a TIA

139
Migraine Demography Younger age Women>men (4:1)
10-20% of the population The risk of migraine with aura and transient ischemic attacks (TIA’s) is greater than 2 fold. 1/3 have migraine with aura
 is greater than 2 fold. 1/3 have migraine with aura.")
140
Migraine with Aura Migraine with aura
Positive symptoms Spread over minutes Visual disturbances Somatosensory or motor disturbance Headache within 1 hour Migraine with aura is associated with a twofold risk of ischemic stroke. This risk is higher in women, age < 45, smokers, and women who used oral contraceptives. BMJ2009;339:b3914, Migraine and cardiovascular disease

141
Migraine with Aura Aura without Headache 98% Visual symptoms
30% with other symptoms 26% sensory 16% aphasia 6% dysarthria 10% weakness Mean age 48.7 (vs. 62.1) Fewer cardiovascular risk factors
 Fewer cardiovascular risk factors.")
142
Migraine CNS Timing Usually 20 to 30 minutes
Sporadic attacks during years

143
Migraine with Aura

144
Migraine Associated Symptoms
Headache after attack, nausea, vomiting, photophobia, phonophobia (usually GI or autonomic nervous system)
")
145
Migraine Auras typically occur before the onset of migraine headache, and the headache usually begins simultaneously with or just after the end of the aura phase. However, headache onset can rarely occur an hour or more after the end of the aura phase. Although atypical, an aura can develop during or after the onset of headache, and many patients have migraine aura with only a minimal or no headache.

146
Migraine Most migraine auras resolve in 20 to 30 minutes and seldom last more than one hour. Typical auras may involve any of the following manifestations: Visual disturbances ( the most common type of aura) Sensory symptoms Motor weakness Speech disturbances
 Sensory symptoms. Motor weakness. Speech disturbances.")
147
Migraine vs. TIA Positive visual symptoms Gradual onset / evolution
Sequential progression Repetitive attacks of identical nature Flurry of attacks mid-life Duration up to 60 minutes Headache follows ~ 50% Visual loss Abrupt Simultaneous occurrence Duration <15 minutes Headache uncommon accompaniment

148
Syncope Demography Any age, often younger Women>men

149
Syncope Timing Usually a few seconds Sporadic attacks during years

150
Syncope Associated Symptoms
Sweating, pallor, nausea

151
Most Common Types of Syncope
Neurocardiogenic (vasovagal) syncope Situational syncope (during or immediately after urination, defecation, cough, or swallowing) Orthostatic syncope (associated with orthostatic hypotension) Syncope related to cardiac ischemia or cardiac arrhythmia
 syncope. Situational syncope (during or immediately after urination, defecation, cough, or swallowing) Orthostatic syncope (associated with orthostatic hypotension) Syncope related to cardiac ischemia or cardiac arrhythmia.")
152
Seizures TIAs Migraine Syncope Demography Any age, often younger
Differential diagnosis of transient neurologic symptoms Seizures TIAs Migraine Syncope Demography Any age, often younger Older patients Younger age Stroke risk factors present Women>men Men>women Central nervous system symptoms Positive symptoms: limb jerking, head turning, loss of consciousness Negative symptoms: numbness, visual loss, paralysis, ataxia First positive symptoms, then negative in same modality: scintillating scotomas and parasthesias most common; second sensory modality is involved after first clears Light-headed, dim vision, noises distant, decreased alertness Negative symptoms may develop, remain postictally, and persist All sensory modalities affected simultaneously Transient loss of consciousness Timing 20 to 80 seconds Usually minutes, mostly <1 hour Usually 20 to 30 minutes Usually a few seconds Absence, atonic seizures and myoclonic jerks are shorter Spells during days, weeks, months; not usually years Sporadic attacks during years Postictal depression Spells occur during years Associated symptoms Tongue biting, incontinence, sore muscles, headache after attack Headaches may occur during time period of TIAs Headache after attack, nausea, vomiting, photophobia, phonophobia Sweating, pallor, nausea

153
Transient Global Amnesia
Sudden disorder of memory Antegrade and often retrograde Recurrence 3% per year Etiology unclear Migraine Epilepsy (7% within 1 year) Unknown
 Unknown.")
154
Transient Global Amnesia
No difference in vascular risk factors compared with general population Fewer risk factors when compared with TIA patients Prognosis significantly better than TIA

155
Structural intracranial lesion
Tumor Partial seizures Vascular steal Hemorrhage Vessel compression by tumor

156
Intracranial hemorrhage
ICH rare to confuse with TIA Subdural hematoma Headache Fluctuation of symptoms Mental status changes

157
Multiple sclerosis Usually subacute but can be acute
Optic neuritis Limb ataxia Age and risk factors Signs more pronounced than symptoms

158
Labyrinthine Disorders
Central vs. Peripheral vertigo Ménière's disease Benign positional vertigo Acute vestibular neuronitis

159
Others in the Differential Diagnosis
Metabolic perturbations, such as hypoglycemia, can be associated with focal neurologic deficits. Multiple sclerosis occasionally can cause paroxysmal attacks, particularly of ataxia and dysarthria. Brain tumors can occasionally result in transient neurologic symptoms; the mechanism in these cases is thought to involve mechanical changes that result in pressure on structures adjacent to the tumor.

160
Others in the Differential Diagnosis
Subdural hematomas may cause attacks of transient neurologic dysfunction, again due to mechanical changes that result in pressure on structures adjacent to the hematoma. Cerebral amyloid angiopathy, better known as a cause of intracerebral hemorrhage, may also cause transient neurologic symptoms. Affected patients complain of recurrent, brief (minutes), often stereotyped spells of weakness, numbness, paresthesias, or other cortical symptoms that can spread smoothly over contiguous body parts.
, often stereotyped spells of weakness, numbness, paresthesias, or other cortical symptoms that can spread smoothly over contiguous body parts.")
161
Others in the Differential Diagnosis
Hepatic, renal, and pulmonary encephalopathies can produce temporary aberrations in alertness, behavior and movement. Compressive myelopathy may rarely cause sudden transient sensory changes and motor deficits. Pressure- or position-related peripheral nerve or nerve root compression can cause transient paresthesias and numbness.

162
Others in the Differential Diagnosis
Peripheral vestibulopathies can cause transient episodic dizziness. Hysteria and other psychiatric disorders may underlie attacks that include swoons, falls, and episodic blindness, deafness, and paralysis, which can be confused with organic loss of function.

163
Case 1 A 19 year old man had a history of a murmur since birth and intermittent episodes of hemiparesis that he ignored. He presented with collapse while playing handball.

164
Case 1 He fell and had tonic clonic movement of his extremities. He was in distress at presentation His BP was 110/70, HR 76, RR 18. He had a persistently split S2 with a systolic ejection murmur in the upper left second intercostal area. His neurological exam was consistent with a right middle cerebral infarction with a left hemiplegia and left hemisensory defect.

166
Case 2 When 22-year-old Ms. KS began experiencing left arm weakness, she went to a clinic only to be told that nothing was seriously wrong. But when her symptoms persisted, so did she. She was finally referred to the Medical Center, where neurologists confirmed that her symptoms were the result of a stroke.

167
Case 2 Further testing in the Coagulation Laboratory revealed activated protein C resistance, the result of a heterozygous mutation in factor V Leiden, as well as a homozygous mutation in the methylene tetrahydrofolate reductase gene, responsible for elevated homocystine

168
Case 2 Although she had had only one clinical stroke, multiple other strokes were evident by imaging studies. Factors contributing to her hypercoagulable state included: 1. the methylene tetrahydrofolate reductase deficiency, which elevated her homocystine level, 2. the heterozygous state for factor V Leiden, causing activated protein C resistance, 3. oral contraceptives, 4. smoking, and 5. hypertension. She is doing well, without recurrence, on aspirin, and antihypertensive medicines, having stopped smoking and birth control pills.

169
Case 3 In another case, a 20-year-old female college student was sent to the Medical Center after a brain scan showed what her physicians thought to be a brain tumor. Neurosurgeons quickly realized there was no tumor, and that the young woman had suffered a stroke. After thrombosis of intracranial venous sinuses was diagnosed she was treated with heparin, and then Warfarin. Repeat imaging revealed recanalization of the previously thrombosed sinuses.

171
Case 3 Investigation in the Special Coagulation Laboratory revealed deficiency of antithrombin III, on two separate occasions, several weeks apart. This patient suffered a venous infarction secondary to a hypercoagulable state induced by inherited antithrombin III deficiency, probably exacerbated by use of oral contraceptives. With anticoagulation and careful monitoring, her prognosis is good.

172
Case 4 A 28-year-old man has sudden weakness of the left arm and leg and slurred speech. Except for untreated hypertension, his medical history is unremarkable. He is a current smoker. On arrival at the emergency department 1 hour 15 minutes after the onset of symptoms, he reports no headache or vomiting. His blood pressure is 180/100 mm Hg, and his pulse is 76 beats per minute and is regular. Neurologic examination shows dysarthria, a left homonymous hemianopia, severe left-sided weakness, and a failure to register light touch on the left side of the body when both sides are touched simultaneously (left tactile extinction).
.")
173
Case 4 He had sudden left-sided hemiparesis, strongly suggestive of a right hemisphere stroke.

174
Summary These are not isolated cases. Frequently young patients, even teenagers, who have suffered stroke are misdiagnosed. Though they may have presented with classic symptoms - dizziness, severe headache, weakness in a limb, or unilateral loss of sensation, for example - they often have been misdiagnosed by their provider, most likely because they do not fit the profile of the "typical" stroke patient.

175
Summary Misdiagnosis has included patients being told they had vertigo, migraine, alcohol intoxication or other conditions. They were discharged from clinic and later discovered to have suffered a stroke.

176
Summary The second important point is that the causes of stroke in young people are much more diverse, and less likely to be the ones that commonly cause stroke in older people, such as atherosclerosis of brain-supplying vessels and emboli from cardiac disorders related to coronary artery disease. Without the right resources, providers may be at a loss to pinpoint the cause in order to treat it and prevent further damage.

177
Summary Abuse of amphetamine-like drugs ("speed" and cocaine, for example) can lead to stroke in teenagers and young adults. These drugs are popular in rural and urban areas alike.
 can lead to stroke in teenagers and young adults. These drugs are popular in rural and urban areas alike.")
178
Summary However, one of the increasingly recognized causes of stroke in a young person is a blood disorder that predisposes to blood clotting.This allows clots to form too readily, often in the veins, leading to stroke. Once such a disorder has been identified, treatment can help prevent future damage. Diagnosis of a hereditary disorder can also lead to identification of other family members who may be at high risk.

179
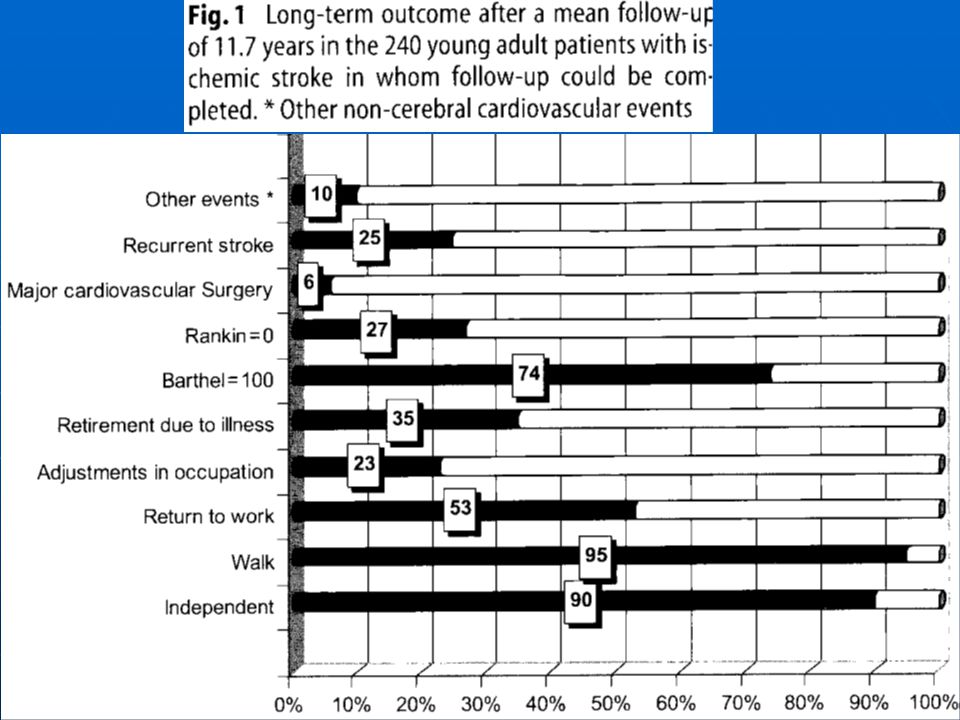
Summary The long term outcome of cerebral infarction is better in young adults than in older patients, morbidity and mortality are still significant. Despite a good functional and motor outcome young adult patients usually encounter difficulties in social and work caused by cognitive impairment.

180
Summary The bottom line: for young stroke patients, extensive testing and careful evaluation may be necessary to determine the underlying cause.

Similar presentations























>")



 Stroke - Overview Third leading cause of death in industrialized countries. Total cost of strokes in the U.S. is roughly.>")

 neurological defecit of sudden onset and lasting> 24h (or leading to death), and of presumed vascular origin 5-10 per.>")




