Download presentation
Presentation is loading. Please wait.

1
Headache and Subarachnoid Hemorrhage
Carly Thompson February 19, 2009 See Rob Halls’ presentation at the end of Carly’s

2
Objectives Approach to headache in the ED Migraine
Focus on dx, tx Subarachnoid Hemorrhage Other causes of serious headache

3
Headache Epidemiology
4% of ED visits Primary Headaches Migraine Tension-Type Cluster Secondary All others! 1% of headaches are SAH!

4
Headache: Historical Features
Occult Trauma Signs of abuse/neglect Anticoagulation SAH Sudden Onset Maximal soon after onset Different than previous Meningitis Fever Neck stiffness Immune compromise Head/neck infection Temporal Arteritis Jaw claudication Temporal tenderness Visual symptoms Pre-eclampsia Pregnancy Post-partum Space-occupying lesion Progressive Hx of malignancy New onset >50yrs Worse in am, head down Neuro signs Cerebral Venous Thrombosis Bilateral neuro findings Proptosis Hypercoaguable state Recent sinusitis Pregnancy CO Toxicity Worse in am Others affected Environmental exposure

5
Question: Name 5 high risk historical features for Subarachnoid Hemorrhage.

6
High Risk Features for SAH
Thunderclap First or worst headache of my life Altered mental status / Seizure Headache with exertion / intercourse History of exercise Location of pain: occipitonuchal PPV occipitonuchal headache for intracranial pathology is 16% Family history of SAH Up to 4x increased risk in 1st and 2nd degree relatives!

7
Question What is your differential for thunderclap headache? Name 3 (other than SAH). Thunderclap = sudden-onset, severe headache
. Thunderclap = sudden-onset, severe headache.")
8
Thunderclap Headache: Differential Diagnosis
SAH Carotid or vertebral artery dissections Venous sinus thrombosis Pituitary apoplexy Hypertensive emergencies Cluster headache Cerebellar CVA

9
High Risk Examination Findings
Vital signs: htn, fever Decreased, altered, fluctuating LOC Focal neurologic sign Meningismus Toxic appearance Opthamalogic findings: papilledema, subhyaloid hemorrhage, retinal hemorrhages, decreased vision, ciliary flush, sluggish pupillary light response Trauma Temporal artery findings Carotid bruit Nausea and vomiting: Increased ICP, hemorrhage, ANAG Nasal discharge with sinus tenderness: sinusitis

10
Question What is a subhyaloid hemorrhage and when do you see it?

11
Subhyaloid Hemorrhage
Gravity-dependent venous hemorrhage between retina and vitreous membrane, convex at bottom, and flat at top when sitting Highly suggestive of SAH: 11-33% of SAH cases Terson’s syndrome – rapid increase in ICP assoc. with hemorrhage – worse outcome

12
Low Risk Patient No change in headache pattern
No new concerning historical features No focal neurologic symptoms or findings No imaging indicated! Meta-analysis: 2.4% of those with normal neuro exam have neurologic abnormalities on CT 0.4% of those with typical migraine symptoms

13
Question Which subsets of patients with headache require neuroimaging in the ED? Name 3 groups.

14
Neuroimaging Indications
ACEP Clinical Policy (Ann Emerg Med 2008) Level B (1) Headache and new abnormal neuro findings PPV 39% for intracranial pathology LR 3.0 (2) Sudden-onset severe headache 10-15% have serious pathology, often SAH (3) HIV patients with new headache Headache – 35% had mass lesion Neurologic complaint – 24% focal lesion 1 or more of predicted all focal lesions in a series of patients: New seizure Depressed / altered LOC Headache different or > 3 days
 Level B. (1) Headache and new abnormal neuro findings. PPV 39% for intracranial pathology. LR 3.0. (2) Sudden-onset severe headache % have serious pathology, often SAH. (3) HIV patients with new headache. Headache – 35% had mass lesion. Neurologic complaint – 24% focal lesion. 1 or more of predicted all focal lesions in a series of patients: New seizure. Depressed / altered LOC. Headache different or > 3 days.")
15
Neuroimaging Level C Evidence
Age >50 with new headache but normal exam, should be considered for urgent neuroimaging OR 3.3 of pathologic diagnosis

16
Neuroimaging Other worrisome features that increase probability of positive findings, but no clear recommendations: Occipital location Worsening with Valsalva Headache waking from sleep Associated syncope Nausea or sensory distortion

17
Neuroimaging Headache in Pregnancy Most headaches are benign
CVA – risk increases 3-13x SAH – 20/100,000 deliveries Migraines: less common 60-70%have improvement in migraines during pregnancy Conclusion: Insufficient data to drive recommendations for imaging.

18
Question Can response to therapy be used as a diagnostic tool?

19
Response to Therapy Level C No!!! Pain response should not be used.
? Common pathway for pain regardless of etiology No RCT to support or refute this. Class III Evidence: Case reports, case series, showing resolution or improvement in pain with analgesics in SAH, meningitis, CO-induced headache, cerebral venous sinus thrombosis, dissection, etc.

20
Migraine What are the diagnostic criteria for migraine?

21
Migraine: Diagnosis Recurrent headache disorder – IHS Criteria
Headache lasts 2-72 hours At least 2 of: Unilateral Pulsating Moderate to Severe Aggravation by routine activity At least 1 of: Photophobia or Phonophobia Nausea and/or vomiting At least 5 attacks Hx, physical and neurologic exam do not suggest other organic disease

22
Migraine: Diagnosis Migraine without Aura Migraine with Aura:
Aura reversible focal neurologic symptoms that usually develop over 5-20 min and last <60 min, headache begins during aura or within 60 minutes Visual positive / negative features Sensory positive / negative features Dysphasic speech

23
Question TRUE! True or False?
Migraines can be associated with autonomic and sinus symptoms i.e. nasal congestion, rhinorrhea, tearing, colour and temperature change, changes in pupil size TRUE!

24
Question Which of the following are associated with migraine?
Family history of migraine Motion sickness Obesity

25
Associated Factors Family history and motion sickness are risk factors for developing migraine Obesity is associated with increased frequency and severity of migraines

26
Migraine: Treatment US Headache Group:
Educate pts about condition and tx; encourage active participation in management Use migraine specific agents in pts with severe migraine, and those who respond poorly to NSAIDs or combination analgesics Use non-oral route for pts with sig N/V Consider self-administered rescue meds for pts with severe migraine Guard against medication overuse headaches by using prophylactic medication in pts with frequent headaches

27
Question List 5 treatment options for migraine in the emergency department.

28
Treatment Options Fluids Analgesics: NSAIDs, acetaminophen
Serotonin Agonists Ergotamine DHE (Dihydroergotamine) Triptans Dopamine Antagonists Chlorpromazine Prochlorperazine Metoclopramide Opioids Steroids: Dexamethasone
 Triptans. Dopamine Antagonists. Chlorpromazine. Prochlorperazine. Metoclopramide. Opioids. Steroids: Dexamethasone.")
29
Mild Analgesics in Migraine
Some pts can get optimal response with mild analgesics (NSAIDs, acetaminophen) Not advisable >10x /month RCTs: Acetaminophen, ibuprofen, naproxen, diclofenac, ASA, acetaminophen + ASA + caffeine Indomethacin: limited data, some specific migraine types are responsive to indomethacin for abortive therapy, benefit: suppository form
 Not advisable >10x /month. RCTs: Acetaminophen, ibuprofen, naproxen, diclofenac, ASA, acetaminophen + ASA + caffeine. Indomethacin: limited data, some specific migraine types are responsive to indomethacin for abortive therapy, benefit: suppository form.")
30
Triptans Specific tx: 5-HT 1b/d agonist ->inhibit dural nociception
Advantage: multiple preparations SC, IN, PO RCT and systematic reviews: all triptans have been shown effective in acute migraine Pts who don’t respond to one may respond to another

31
Question So, why don’t we commonly use triptans in the ED?

32
Limitations of Triptans
More effective if used early! Development of central sensitization Contraindications: Patients with pregnancy, uncontrolled htn, ischemic heart disease, peripheral vascular disease, Prinzmetal’s angina, ischemic CVA, familial hemiplegic migraine, basilar migraine 24 hours of other 5-HT agonist (ergots), MAOIs with some triptans Severe liver impairment Interactions: P450 cytochrome Advisory July 2006 – concomitant use with SSRIs or SNRIs increases risk of serotonin syndrome; advise discussion of benefit vs risk
, MAOIs with some triptans. Severe liver impairment. Interactions: P450 cytochrome. Advisory July 2006 – concomitant use with SSRIs or SNRIs increases risk of serotonin syndrome; advise discussion of benefit vs risk.")
33
Ergots: Ergotamine Mechanism: Efficacy: Side effects:
5HT 1b/d receptor agonist Efficacy: Alone failed to show efficacy Side effects: Nausea, vomiting Vascular occlusion and rebound headaches Long-term: Associated with CAD Avoid in pts with CAD, PVD, htn, hepatic and renal disease and those with prolonged aura European Consensus Panel: Treatment of choice in few pts due to issues of efficacy and side effects

34
Ergots: Dihydroergotamine
Fewer side effects: no dependence or rebound headaches Advantage: IV, IM, SC, IN use Contraindications: Htn, CAD, PVD, Prinzmetal’s, MAOIs, sepsis, severe hepatic or renal dysfunction, high dose ASA tx, pregnancy Hemiplegic or basilar migraine Within 24 hours of triptan or other serotonin agonists CYP3A4 inhibitors: some macrolides, antifungals, protease inhibitors

35
Question How does DHE compare to the triptans for efficacy?
More effective? Same? Less effective?

36
DHE: Efficacy vs Placebo: vs Triptan: vs Dopamine Antagonist:
Proven by systematic review / RCTs, especially when given with anti-emetic vs Triptan: Less effective on most measures compared head-to-head with sumatriptan vs Dopamine Antagonist: Less effective than chlorpromazine on some measures

37
Dopamine Antagonists Benefits: Antiemetic IV metoclopramide
IV or IM chlorpromazine and prochlorperazine

38
Chlorpromazine: Largactil / Thorazine
Chlorpromazine 5-15mg IV or 0.1mg/kg IV RCT vs Placebo (Bigal 2002 J Emerg Med): Significant improvement in scores of pain, nausea, vomiting, photo/phonophobia at 60 min NNT 2 Side effects: Hypotension / Postural hypotension (18%) May be exacerbated by opioids, pre-tx with fluid bolus Alpha-antagonist Drowsiness Pregnancy: Class C
: Significant improvement in scores of pain, nausea, vomiting, photo/phonophobia at 60 min. NNT 2. Side effects: Hypotension / Postural hypotension (18%) May be exacerbated by opioids, pre-tx with fluid bolus. Alpha-antagonist. Drowsiness. Pregnancy: Class C.")
39
Prochlorperazine: Stemetil, Compazine
Prochlorperazine 10mg IV Side effects: Hypotension Drowsiness Dystonic Reactions Cardiac arrhythmias Pregnancy Class C: Isolated reports of congenital anomalies, jaundice, EPS, hyper/hyporeflexia – if occasional low-dose suggested to be safe FDA Alert (June 2008): Association with increased mortality when used for treating dementia-related psychosis
: Association with increased mortality when used for treating dementia-related psychosis.")
40
Question How does prochlorperazine compare to metoclopramide?

41
Proclorperazine vs Metoclopramide
RCT: Coppola (1995) Annals of Emerg Med > 50% relief Stematil 82% Maxeran 48% Placebo 29% RCT: Jones (1996) Am J of Emerg Med Partial or complete relief Stematil 67% Maxeran 34% Placebo 16%
 Annals of Emerg Med. > 50% relief. Stematil 82% Maxeran 48% Placebo 29% RCT: Jones (1996) Am J of Emerg Med. Partial or complete relief. Stematil 67% Maxeran 34% Placebo 16%")
42
Metoclopramide: Maxeran, Reglan
Maxeran 10mg IV Efficacy: Meta-analysis Colman (2004) BMJ Generally poor studies OR 2.84 for reduction of pain in headache Less effective than chlorpromazine and prochlorperazine in relieving pain, but not always statistically significant 1 Trial: No difference between aggressive metoclopramide (20mg IV q30 min up to 4x with diphenhydramine 25mg IV q1 hour up to 2x) vs sumatriptan 6mg SC Benefits: Pregnancy Class B Can be combined with DHE, other analgesics Side Effects: Drowsiness Dystonic reactions: <1-25%, increased risk in young males
 BMJ. Generally poor studies. OR 2.84 for reduction of pain in headache. Less effective than chlorpromazine and prochlorperazine in relieving pain, but not always statistically significant. 1 Trial: No difference between aggressive metoclopramide (20mg IV q30 min up to 4x with diphenhydramine 25mg IV q1 hour up to 2x) vs sumatriptan 6mg SC. Benefits: Pregnancy Class B. Can be combined with DHE, other analgesics. Side Effects: Drowsiness. Dystonic reactions: <1-25%, increased risk in young males.")
43
Other Options? Some pts will not respond to routine treatment.
Consider wait-times, location (ED vs clinic) Treat aggressively. Do not use following meds on a chronic basis due to habit-forming nature and rebound headaches. Benzos Opioids Barbiturates
 Treat aggressively. Do not use following meds on a chronic basis due to habit-forming nature and rebound headaches. Benzos. Opioids. Barbiturates.")
44
Question How can you prevent migraine recurrence?

45
Parenteral Dexamethasone
Colman I et al. (2008) BMJ Meta-analysis of 7 RCTs. Dexamethasone 10-25mg IV or IM vs placebo Similar acute pain reduction Recurrence rates at 72 hours RR 0.74 ( ) NNT 9 Similar side effect profile
 BMJ. Meta-analysis of 7 RCTs. Dexamethasone 10-25mg IV or IM vs placebo. Similar acute pain reduction. Recurrence rates at 72 hours RR 0.74 ( ) NNT 9. Similar side effect profile.")
46
Question Can you name the complications of a migraine?

47
Migraine: Complications
Status migrainosus Chronic migraine Persistent aura without infarction Migrainous infarction Migraine-triggered seizure

48
Summary: Migraine Tx in the ED
Fluid bolus: NS 1L bolus IV NSAID: If used <10x/month Nausea / vomiting: consider PR indomethacin PO: acetaminophen vs ibuprofen Dopamine antagonist: Stemetil 10mg IV Maxeran 10mg IV (Pregnancy) Opioid: Morphine 2-5mg IV prn DHE / Triptan: If early presentation, contraindications to others Rizatriptan, eletriptan, almotriptan Sumatriptan: IN, SC or Zolmitriptan: IN, PO
 Opioid: Morphine 2-5mg IV prn. DHE / Triptan: If early presentation, contraindications to others. Rizatriptan, eletriptan, almotriptan. Sumatriptan: IN, SC or Zolmitriptan: IN, PO.")
49
Subarachnoid Hemorrhage
Epidemiology SAH 1% of all headaches in ED 10% of hemorrhagic strokes 10% of “worst headache ever” Prevalence: 3-25 / 100,000 Mean age: 55 (Range 20-60) Reported in pediatrics Miss Rate? Variable 5-50% (30% average) Acceptable miss rate: 0%!
 Reported in pediatrics. Miss Rate Variable 5-50% (30% average) Acceptable miss rate: 0%!")
50
Question Can you name 3 causes of SAH?

51
Causes of SAH Causes of SAH: Trauma Saccular Aneurysms
Non aneurysmal: Perimesencephalic (?venous bleed) AVMs / Fistulae Illicit drug use: cocaine, amphetamines Arterial dissections
 AVMs / Fistulae. Illicit drug use: cocaine, amphetamines. Arterial dissections.")
52
Question Can you name 3 risk factors for formation of aneurysms?

53
Etiology of Aneurysms Congenital: Acquired:
Familial intracranial aneurysms (dominant) Genetic condition: Ehlers-Danlos, Marfan’s, PCKD Coarctation Acquired: Traumatic: skull #, penetration, post-op, hemodynamic damage Infectious: syphilis, mycotic Inflammatory: vasculitis Degenerative: atherosclerotic Hypertension is NOT a major factor for aneurysm formation!
 Genetic condition: Ehlers-Danlos, Marfan’s, PCKD. Coarctation. Acquired: Traumatic: skull #, penetration, post-op, hemodynamic damage. Infectious: syphilis, mycotic. Inflammatory: vasculitis. Degenerative: atherosclerotic. Hypertension is NOT a major factor for aneurysm formation!")
54
Question How many people have aneurysms?

55
Aneurysms in the Public
Prevalence of saccular aneurysms 5% at autopsy 20-30% have multiple aneurysms

56
Question Can you name 3 risk factors for rupture?

57
Risk Factors for Rupture of Aneurysms
Smoking Dose-dependent, esp. women, disappears soon after quitting, RR 2.2 Hypertension RR 2.5, OR 2.6 EtOH Moderate to heavy consumption RR 2.1, OR 1.5 Family History OR 4.0 Genetics Autosomal dominant / recessive / multifactorial / anticipation Elastin gene, Platelet adhesive glycoprotein Phenylpropanolamine Appetite suppressants, cold remedies, case-control study – risk factor in women Estrogen deficiency Premenopausal women and reduced risk compared to age-matched postmenopausal women (OR 0.24), HRT (OR 0.47) Physical Exertion Orgasm, moderate exertion OR 2.7 ?Anticoagulants
, HRT (OR 0.47) Physical Exertion. Orgasm, moderate exertion OR 2.7. Anticoagulants.")
58
Question What proportion of patients with SAH from aneurysm have a sentinel bleed?

59
Sentinel Headache 30-50% of patients have a sentinel headache that precedes SAH by 6-20 days

60
Clinical Features Abrupt onset, severe headache “thunderclap”
Lateralized 30% At night 30% (During day / activity 60%) Onset associated with brief LOC, seizure, nausea, vomiting Meningismus / Aseptic meningitis Normal neurologic findings at presentation 50%
 Onset associated with brief LOC, seizure, nausea, vomiting. Meningismus / Aseptic meningitis. Normal neurologic findings at presentation 50%")
61
Question What is the mortality of SAH?

62
Mortality Average: 51% 10% prior to reaching hospital
25% within 24 hours of onset 45% within 30 days

63
Question What are the complications of SAH? Name 4.

64
Complications Rebleeding Vasospasm and delayed cerebral ischemia
Infarction Hydrocephalus (acute / chronic) Increased ICP Seizures Hyponatremia Hypothalamic dysfunction and pituitary insufficiency Cardiac abnormalities ECG Ventricular wall motion abnormalities Elevated BNP
 Increased ICP. Seizures. Hyponatremia. Hypothalamic dysfunction and pituitary insufficiency. Cardiac abnormalities. ECG. Ventricular wall motion abnormalities. Elevated BNP.")
65
Pitfalls in Diagnosis Wasn’t the worst headache of their life!
Neurologic exam was normal! 50% have normal neurologic exam! Pain improved with treatment Remember: SAH CAN improve with treatment! CT head was negative RBCs decreased from tubes 1-3 / Misinterpretation of LP No LP done

66
CT Head: Limitations Technical ability of CT scanners to identify small hemorrhage / artifact / bone Protocol and age of scanner – thin slices Expertise of reader Anemia Hb<100 – blood appears isodense Time: decay in sensitivity Inability to diagnose other causes of headache: meningitis, etc.

67
Question How sensitive is CT scan at day 1 for SAH?

68
CT Scan: Sensitivity As blood is diluted and degraded flowing through SA space -> decreased sensitivity BMJ (2006) <12 Hrs 98% 24 hrs 93% >7 days <50% Memory aide: Day 1 90% Day 2 80% Day 3 70% Day 4 60%
 <12 Hrs 98% 24 hrs 93% >7 days <50% Memory aide: Day 1 90% Day 2 80% Day 3 70% Day 4 60%")
69
Question Why do you do a CT then if ruling out SAH?

70
CT Scan for SAH: Advantages
Traumatic LP: 13% may be traumatic (>400 RBCs) LP Limitations: Cerebral venous thrombosis Unruptured aneurysm Arterial dissection Pituitary apoplexy
 LP Limitations: Cerebral venous thrombosis. Unruptured aneurysm. Arterial dissection. Pituitary apoplexy.")
71
Question Does an LP need to be routinely performed on ED patients to rule out SAH if normal noncontrast CT head? Why?

72
Lumbar Puncture ACEP (2008) Level B Evidence.
Lumbar puncture should be performed to rule out SAH. Rates of SAH confirmed by LP after normal CT %

73
Question What 3 features do you see on LP in SAH?

74
Lumbar Puncture in SAH (1) Elevated opening pressure
(2) Elevated RBC count (3) Xanthochromia
 Elevated RBC count. (3) Xanthochromia.")
75
Opening Pressure Normal? 6-20cmH20 is normal in adults and children
25cmH20 may be normal in obese pts Utility: Helpful to distinguish SAH from traumatic tap 2/3 of SAH may have elevated opening pressure Other diagnoses: spontaneous intracranial hypotension, benign intracranial hypertension, cerebral venous sinus thrombosis

76
Question Does clearing of blood (i.e. declining RBC count from tubes 1->4) rule out SAH?
 rule out SAH")
77
Elevated Red Blood Cell Count
Clearing of blood is unreliable. There is no cutoff which has been shown to reliably exclude SAH. However, if tap done late >12 hours, and absence of xanthochromia, but presence of RBC = negative tap. No way to tell traumatic tap vs SAH if early <12 hours tap.

78
Question What is xanthochromia?
When does it appear? How long does it last?

79
Xanthochromia Yellow colour caused by bilirubin and oxyhemoglobin due to lysis of RBCs OxyHb -> Heme oxidase enzyme -> Bilirubin Process may take 6-12 hours Onset: Blood in CSF for at least 2 hours Peak: 48 hours Duration: Up to 2-4 weeks

80
Question Name 2 methods for analyzing your sample tubes for xanthochromia. Which is more sensitive?

81
Xanthochromia: Analysis
Spectrophotometry Spin CSF, run through spectrophotometer, look for oxyHb or bilirubin peak at 410nm and 460nm Most sensitive Low-moderate specificity Not always available Visual Analysis Spin CSF, compare to identical test tube with equal volume tap water against white background Calgary Health Region’s method Less sensitive, but may be >95% if >12 hours after SAH

82
Question Name 3 false positives for xanthochromia.
(Xanthochromia but no SAH!)
")
83
Xanthochromia: False Positives
Hyperbilirubinemia Rifampin Previous traumatic tap Traumatic tap isn’t analyzed quickly -> xanthochromia Chronic spinal cord abnormalities

84
Question Which patients can safely undergo LP without neuroimaging?

85
LP Before CT? ACEP (2008). Level C Evidence.
Adults patients with headache and signs of elevated ICP should have neuroimaging before LP. Papilledema, absent venous pulsations of fundoscopy, altered LOC, focal neuro deficits, signs of meningeal irritation In the absence of clinical findings suggestive of increased ICP, LP can be performed without obtaining neuroimaging.

86
Question In a patient with sudden-onset, severe headache who has negative findings (both CT head and LP) is there a need for further emergent imaging?
 is there a need for further emergent imaging")
87
Further Investigation
ACEP (2008). Level B Evidence. Patients with sudden-onset, severe headache with negative CT head, normal opening pressure, negative findings on CSF analysis, do NOT need emergent angiography, and can be discharged with follow-up recommended. Note: Consider other causes of sudden-onset, severe headache like pituitary apoplexy, cerebral venous sinus thrombosis, arterial dissections, cerebellar stroke Further imaging may be indicated to rule out these causes.
. Level B Evidence. Patients with sudden-onset, severe headache with negative CT head, normal opening pressure, negative findings on CSF analysis, do NOT need emergent angiography, and can be discharged with follow-up recommended. Note: Consider other causes of sudden-onset, severe headache like pituitary apoplexy, cerebral venous sinus thrombosis, arterial dissections, cerebellar stroke Further imaging may be indicated to rule out these causes.")
88
Further Investigation
Perry et al. (2008) Annals of Emerg Med. 2 Canadian EDs, 592 patients CT and LP to rule out SAH (10.3% had SAH) CT neg No xanthochromia by visual inspection RBCs in final tube <5 x 106RBC/L Others followed 6-36 months Rate of subsequent SAH: 0% Rate of subsequent aneurysm: 1 / 592 required surgery, but “did not contribute to initial presentation”
 Annals of Emerg Med. 2 Canadian EDs, 592 patients. CT and LP to rule out SAH (10.3% had SAH) CT neg. No xanthochromia by visual inspection. RBCs in final tube <5 x 106RBC/L. Others followed 6-36 months. Rate of subsequent SAH: 0% Rate of subsequent aneurysm: 1 / 592 required surgery, but did not contribute to initial presentation")
89
Thank You!

90
Question Can you name 3 causes of headache that might be associated with exertion?

91
Exertional Headache SAH Carotid or Vertebral Artery Dissection
Pts with SAH more likely to have participated in exertion that day, compared to previous OR 2.7 Carotid or Vertebral Artery Dissection Primary Exertional Headache Bilateral pulsatile pain during or after exercise, lasts 5min – 48 hours, not usually assoc. with N/V Rule out: SAH, angina, vascular abnormalities, pheo Tx: indomethacin, propranolol, naproxen Primary Headache Associated with Sexual Activity Preorgasmic: usually secondary to muscle tension Orgasmic: associated with CVA / dissection and SAH Unpredictable Prevention: indomethacin, B-blockers, propranolol Acute tx: triptans

92
Question Can you describe the most common headache symptoms in brain tumour?

93
Brain Tumour 50% have headaches Typical headache:
Tension-type (77%) Migraine (9%) Typical headache: Bilateral, worse ipsilaterally, bending over (32%), nausea and vomiting (40%), worse with Valsalva Classic “early morning headache” – uncommon! Reliable findings: Nausea, vomiting, worsening with change in position, abnormal neurologic exam, significant change in headache pattern
 Migraine (9%) Typical headache: Bilateral, worse ipsilaterally, bending over (32%), nausea and vomiting (40%), worse with Valsalva. Classic early morning headache – uncommon! Reliable findings: Nausea, vomiting, worsening with change in position, abnormal neurologic exam, significant change in headache pattern.")
94
Triptans: Comparison Few trials comparing triptans head to head
Rizatriptan (Maxalt), eletriptan (Relpax), almotriptan (Axert) had highest likelihood of success Sumatriptan was recently released with fast dissolving tabs Sumatriptan (Imitrex): SC, IN, PO Zolmitriptan (Zomig): IN, PO
, eletriptan (Relpax), almotriptan (Axert) had highest likelihood of success. Sumatriptan was recently released with fast dissolving tabs. Sumatriptan (Imitrex): SC, IN, PO. Zolmitriptan (Zomig): IN, PO.")
95
Headache: Emergent Diagnoses
Core Rounds Feb19,2009 Rob Hall MD, FRCPC

96
Case 41yo female PMHx DM1 on insulin
Mild headache and Numbness right arm/mouth and weakness left grip, subacute, 1 week No fever or illicit drug use OCP started 2 weeks ago No hx seizures, no trauma Waiting in ED bed, GTC 1 min sz, chemstrip normal, ativan 2mg iv, post ictal and combative after, no focal findings after sz Investigations? Thoughts on dx?

97
CT head (plain)
")
98
Cerebral Vein Thrombosis
“DVT of the BRAIN” Venous clot then infarct and/or bleed at grey-white junction Transverse sinus most common location, often multiple sinuses

99
Clinical Presentations
STROKE SYNDROME Often not typical arterial distribution SEIZURE HEADACHE Can be basically any description of headache (thunderclap uncommon)
")
100
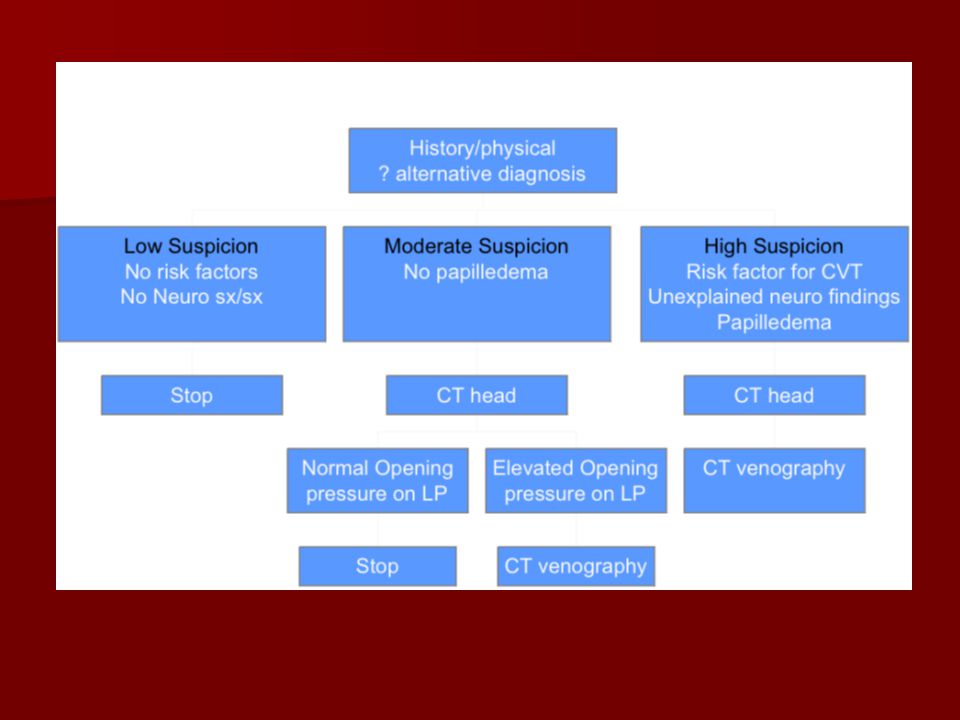
Risk Factors for CVT (present in 85%)
Head and neck infections Hypercoagulable states Estrogens Pregnancy Cancer Hypercoag syndrome: lupus AC, protein C def, etc Hematologic disorders: leukemias, polycythemia, thrombocytosis, sickle cell Vasculitis: SLE, GCA, wegener’s, Bechet’s, etc

101
Exam findings Highly variable Three clues
Head infection + Neuro symptoms Papilledema (? Sensitivitiy) Stroke findings in non-arterial distribution LP will show elevated opening pressure without other cause
 Stroke findings in non-arterial distribution. LP will show elevated opening pressure without other cause.")
102
CT head (plain) findings
Sensitivity 60-70% (30-40% normal) Delta sign = dense triangle from hyperacute thrombosed superior saggital sinus Cord sign = thrombosed cortical vein Venous infarcts with secondary hemorrhage in non-arterial distribution HTN bleeds: thalamus, IC, CB, pons Venous infarct bleeds: bilateral at grey-white junction
 Delta sign = dense triangle from hyperacute thrombosed superior saggital sinus. Cord sign = thrombosed cortical vein. Venous infarcts with secondary hemorrhage in non-arterial distribution. HTN bleeds: thalamus, IC, CB, pons. Venous infarct bleeds: bilateral at grey-white junction.")
103
CT head

104
Definitive Diagnosis CT venography (preferred) MR venography
Hypointense signal of acute thrombus mimics normal flow. RadioGraphics 2006;26:S5-18. Angiography (not used anymore)
")
105
CT Venography

106
CVT and Carotid/vert dissections. Which is better CT or MR?
“I think that most radiologists reading these studies would say that both CTV and CTA have a higher sensitivity due to CT's inherent spatial resolution advantage which is very good on our latest multidetector scanners. CT is our favoured study where there is concern for venous sinus thrombosis and carotid/vertebral dissection. The research will catch up.”

107
ED Management Dilantin if seized Manage elevated ICP Heparin
Majority of evidence shows improvement trends (no major large RCT showing statistically conclusive results) Shown to be safe even with hemorrhages! Cochrane review 2001 RR death 0.33 (95%CI ) RR death or disability 0.46 ( )
 Shown to be safe even with hemorrhages! Cochrane review RR death 0.33 (95%CI ) RR death or disability 0.46 ( )")
108
Further Management Optic nerve fenestrations Acetazolamide
Case reports of lytics LP/VP shunts Hemicraniectomy for severe ICP problems

110
Is Idiopathic Intracranial HTN and CVT a spectrum of disease?
IIHTN > CVT

111
Idiopathic Intracranial HTN (IIHTN)
Old terms = Pseudotumor cerebri, Benign IHTN, meningitis Cerosa Diagnostic criteria for IIHTN requires imaging to rule out CVT

112
Idiopathic Intracranial HTN (IIHTN)
Opening pressure > 20 cm H20 (usu 25-45) Headache MUCH better after LP! Signs/symptoms of increased ICP No focal signs (except 6th palsy) No mass lesion No hydrocephalus Normal CSF values CTV/MRV to exclude CVT
 Headache MUCH better after LP! Signs/symptoms of increased ICP. No focal signs (except 6th palsy) No mass lesion. No hydrocephalus. Normal CSF values. CTV/MRV to exclude CVT.")
113
Idiopathic Intracranial HTN (IIHTN)
Main ED PEARL is to consider the diagnosis and do an LP “Consider” Obese, female, OCP Hypercoag states Subacute, unexplained headaches, return visits, normal imaging Visual symptoms: blurry vision, diplopia

114
Carotid and Vertebral Dissections
2% of ischemic strokes overall but 20% of ischemic CVA < 45yo Think of in young patient Pathology the same with major vs minor trauma May be VERY minor (yoga, cough, stretching, etc) Unknown if “spontaneous” really occur
 Unknown if spontaneous really occur.")
115
Carotid and Vertebral Dissections
Headache + Neck pain, unilateral + neuro symptoms Dx - CTA, MRA, angio CTA preffered

116
Giant Cell (Temporal) Arteritis: the basics
Older person Subacute headache Systemic symptoms Jaw claudication Association with PMR Risk of vision loss Elevated ESR Diagnose by temporal artery biopsy Treat with steriods

117
Giant Cell Arteritis: some pearls
Extremely rare < 50 years old Pooled analysis 1435 pt, only 2 < 50yo Temporal artery findings (large, absent pulse, tenderness) fairly specific but not sensitive Normal ESR (< 20 mm/hr) excludes dx, moderate ESRs don’t (20-50 mm/hr) <20 mm/hr 96% sensitive <40 mm/hr 95% sensitive < 50 mm/hr 89% sensitive
 fairly specific but not sensitive. Normal ESR (< 20 mm/hr) excludes dx, moderate ESRs don’t (20-50 mm/hr) <20 mm/hr 96% sensitive. <40 mm/hr 95% sensitive. < 50 mm/hr 89% sensitive.")
118
Giant Cell Arteritis: some pearls
Temporal artery biopsy Initial bilateral biopsies 88% sensitive Repeat if initial biopsies negative Biopsy will be abnormal for weeks after initiation of steriod; try to have it done soon but not emergently Treatment Prednisone 60 mg po od ASA START before biopsy

119
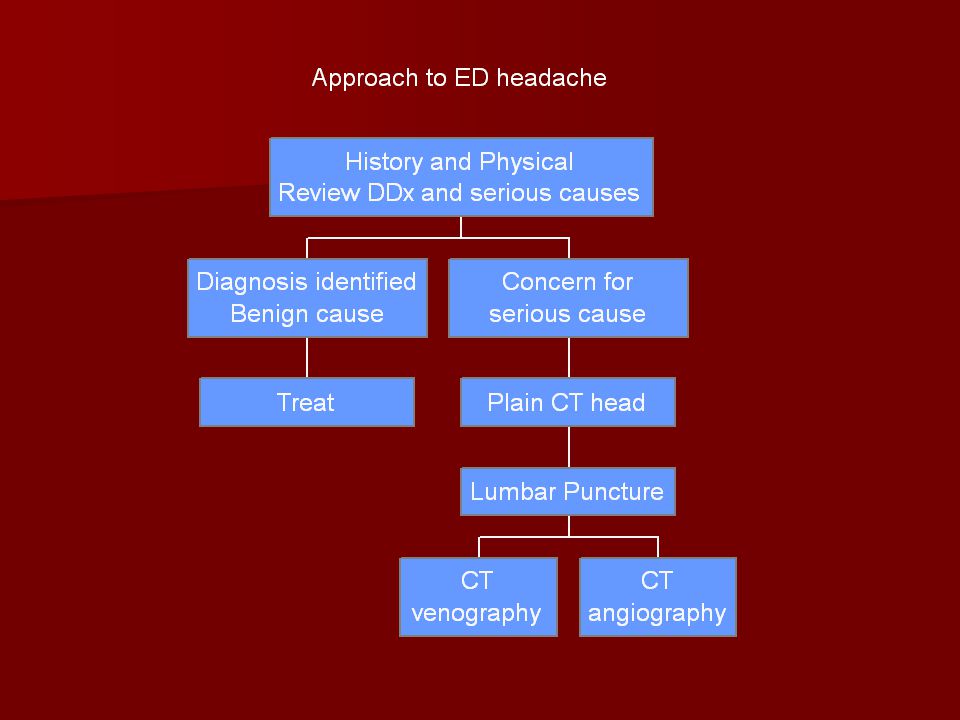
APPROACH to ED HEADACHE
Headache is a high risk complaint. Consider serious causes in every case. Majority of badness excluded with good history and physical. More complex than just ordering CT head!

120
Headache and normal CT head; ddx of “bad” causes?
Ischemic stroke HTN encephalopathy Pre-eclampsia CO toxicity Vasculitis/GCA AACG CNS infection CVT IIHTN SAH Carotid/vertebral dissection Which can be excluded By hx/pe?

121
Headache and normal CT head; ddx of “bad” causes?
Ischemic stroke - hx and physical HTN encephalopathy - physical Pre-eclampsia - hx and physical CO toxicity - hx Vasculitis/GCA - hx AACG - physical CNS infection CVT IIHTN SAH Carotid/vertebral dissection - CTA/MRA Which can be excluded By a normal LP?

122
Headache and normal CT head; ddx of “bad” causes?
Ischemic stroke - hx and physical HTN encephalopathy - physical CO toxicity - hx Vasculitis/GCA - hx AACG - physical CNS infection > LP CVT > LP (+/- CTV) IIHTN > LP SAH > LP Carotid/vertebral dissection - CTA/MRA/Angio
 IIHTN > LP. SAH > LP. Carotid/vertebral dissection - CTA/MRA/Angio.")
123
Lumbar puncture is a useful test to exclude some nasty causes of headache
Opening pressure is worthwhile.

125
Headache motherhood statements
Chronic migrainers with toradol allergies get badness to. Be diligent. Approach headache like chest pain - good hx/pe and directed investigations to exclude badness. Have a ddx of badness and “run the list” with every headache. Headache is more than migraine and SAH. Anyone can thing to order a CT head. A good clinician will pick up the less common but serious diagnoses. Older patient with no hx migraine: be cautious.

126
Miscellaneous pearls What INR before LP?
What platelet level is c/I to LP? 35yo healthy male, collapsed, Vfib arrest, bystander cpr and defib at 5min, persistent coma, diagnosis? How to decrease post LP headache? Needle size, pokes, non-cutting, stylet Bedrest and IVF not helpful

Similar presentations