Download presentation
Presentation is loading. Please wait.

1
DEBATE Role Of IVIG In RH isoimmunization
Dr. Najat Rooh-Al-Deen Consultant Hematology Maternity Hospital

2
IVIG—Is It the Answer? Disease Nature ----
Does IVIG has a real role----- IUT – related issues Maternity Hospital – related issues Long term outcome in children treated with IUT d/t RBC alloimmunization Research interest in the monitoring and treatment of fetal anemia

3
IVIG—Is It the Answer? Disease Nature –----
Does IVIG has a real role----- Maternity Hospital – related issues IUT – related issues Long term l outcome in children treated with IUT d/t RBC alloimmunization Reaserch interest in the monitoring and treatment of fetal anemia

4
About 1 in 10 pregnancies involve an Rh-negative mother and an Rh-positive father

5
Background Hemolytic disease of the newborn (HDN)
-Devastating effects on fetal and maternal health. -Clinical management is challenging and fetal prognosis # High maternal antibody titer # Multiple alloantibodies presence It may start very early in pregnancy in severe

7
IVIG—Is It the Answer? Disease Nature –----
IUT – related issues Does IVIG has a real role----- Maternity Hospital – related issues Long term l outcome in children treated with IUT d/t RBC alloimmunization Reaserch interest in the monitoring and treatment of fetal anemia

8
IVIG—Is It the Answer? Disease Nature – related issues-----
IUT – related issues is an invasive procedure IUT-complication IUT- limitation in early severe maternal isoimmunization Does IVIG has a real role----- Maternity Hospital – related issues

9
IVIG—Is It the Answer? Disease – related issues-----
IUT – related issues is an invasive procedure IUT-complication IUT- limitation in early severe maternal isoimmunization Does IVIG has a real role----- Maternity Hospital – related issues

10
IVIG—Is It the Answer? Disease – related issues-----
IUT – related issues is an invasive procedure IUT-complication IUT- limitation in early severe maternal isoimmunization Does IVIG has a real role----- Maternity Hospital – related issues

11
Complications of intravascular IUT Leiden Experience
740 transfusions (254 fetuses), median 3 (1-7) per fetus First IUT: 27.1 ( ) wk, hydrops 38%, Hct 15 (4-38)% Survival 89%
, median 3 (1-7) per fetus. First IUT: 27.1 ( ) wk, hydrops 38%, Hct 15 (4-38)% Survival 89%")
12
Intrauterine transfusions -Complication
Brady cardia % Preterm labor. Excessive bleeding and mixing of fetal and maternal blood 65% if placenta anterior and 16% if placenta posterior %. Amniotic fluid leakage from the uterus. Fetal death 2.7%. Uterine infection rare. Fetal infection rare. Abruptio placentae

13
Complications associated with intrauterine procedures such as cord hematoma, hemorrhage, fetal bradycardia and intrauterine death could increase in the future (Illanes S and Soothill PW, 2006).
.")
14
IVIG—Is It the Answer? Disease – related issues-----
IUT – related issues is an invasive procedure IUT-complication IUT- limitation in early severe maternal isoimmunization Does IVIG has a real role----- Maternity Hospital – related issues

15
severe maternal red cell alloimmunization is before 20 weeks ’ gestation
a “ challenging ” due to even if the IUT is completed successfully, the premature anemic fetus will not tolerate the acute hemodynamic changes. The technically difficult access in fetal intravascular system despite improved ultrasound resolution. The operator has to target the umbilical cord vessels that measure < 3 – 5 mm in diameter The estimated overall IUT procedure-related fetal loss rate was 5.6 % when performed at < 20 weeks ’ gestation especially if the Hgb level is < 5 SD for gestation fetal hydrops

16
IVIG

17
IVIG—Is It the Answer? Disease Nature --------
IUT – related issues Does IVIG has a real role----- Maternity Hospital – related issues Long term outcome in children treated with IUT d/t RBC alloimmunization Reaserch interest in the monitoring and treatment of fetal anemia

18
Management of severe red cell alloimmunisation - IV Immune globulin

19
Landmarks in the History of Immunoglobulin Replacement Therapy
IVIG introduced and becomes standard therapy due to reduction of bacterial and non-bacterial infections4 Renewed interest in SCIG as alternative to IV therapy, especially for home use5 Janeway and Gitlin prefer IM injections, and this becomes standard of care in US2 1952 1953 1955 1980 1990s 2006 Bruton treats first patient diagnosed with agammaglobulinemia with SC injections of immune serum globulin (ISG)1 Berger introduces battery-powered pumps to slowly administer IM ISG by SC route3 First Sub-cu IgG Licensed in US Landmarks in the History of Immunoglobulin Replacement Therapy The era of accurate diagnosis and therapy of immunodeficiency states began in the 1950s. Bruton, Janeway and Gitlin were leaders in the field and treated some of the first patients to be diagnosed with primary immunodeficiency, and established that subcutaneous and IM injections of gammaglobulin were viable methods of treating these patients.1,2 Techniques were improved and in the early 1980s, Berger introduced the battery pump to slowly administer ISG (immune serum globulin).3 In the early 1980s, IVIG replacement therapy became standard of care when preparations with an acceptable incidence of systemic reactions were finally achieved, and it was demonstrated that the incidence of bacterial and non-bacterial infections could be significantly reduced with IVIG treatment.4 In the 1990s there was a renewed interest in the SC method of delivery, especially for home use.5 Bruton OC. Agammaglobulinemia. Pediatrics. 1952;9: Berger M. Subcutaneous immunoglobulin replacement in primary immunodeficiencies. Clin Immunol ;112:1-7. Berger M. et al. Immunoglobulin Replacement by Slow Subcutaneous Infusion. Ann Intern Med.1980;98:55-56. Quartier P. et al. Early and prolonged immunoglobulin replacement therapy in childhood aggamaglobulinemia: A retrospective survey of 31 patients. Journal of Pediatrics. 1999;134:5: Abrahamsen TG, et al. Sanderson H. Home Therapy With Subcutaneous Immunoglobulin Infusions in Children with Congenital Immunodeficiencies. Pediatrics. 1996;98: Bruton OC. Pediatrics. 1952;9: Berger M. Clin Immunol. 2004;112:1-7. Berger M. et al. Ann Intern Med. 1980;98:55-56. Quartier P. et al. Jour Pediatrics. 1999;134:5: Abrahamsen TG. Et al. Pediatrics. 1996;98:
1. Berger introduces battery-powered pumps to slowly administer IM ISG by SC route3. First Sub-cu. IgG. Licensed in US. Landmarks in the History of Immunoglobulin Replacement Therapy. The era of accurate diagnosis and therapy of immunodeficiency states began in the 1950s. Bruton, Janeway and Gitlin were leaders in the field and treated some of the first patients to be diagnosed with primary immunodeficiency, and established that subcutaneous and IM injections of gammaglobulin were viable methods of treating these patients.1,2. Techniques were improved and in the early 1980s, Berger introduced the battery pump to slowly administer ISG (immune serum globulin).3. In the early 1980s, IVIG replacement therapy became standard of care when preparations with an acceptable incidence of systemic reactions were finally achieved, and it was demonstrated that the incidence of bacterial and non-bacterial infections could be significantly reduced with IVIG treatment.4. In the 1990s there was a renewed interest in the SC method of delivery, especially for home use.5. Bruton OC. Agammaglobulinemia. Pediatrics. 1952;9: Berger M. Subcutaneous immunoglobulin replacement in primary immunodeficiencies. Clin Immunol. 2004;112:1-7. Berger M. et al. Immunoglobulin Replacement by Slow Subcutaneous Infusion. Ann Intern Med.1980;98: Quartier P. et al. Early and prolonged immunoglobulin replacement therapy in childhood aggamaglobulinemia: A retrospective survey of 31 patients. Journal of Pediatrics. 1999;134:5: Abrahamsen TG, et al. Sanderson H. Home Therapy With Subcutaneous Immunoglobulin Infusions in Children with Congenital Immunodeficiencies. Pediatrics. 1996;98: Bruton OC. Pediatrics. 1952;9: Berger M. Clin Immunol. 2004;112:1-7. Berger M. et al. Ann Intern Med. 1980;98: Quartier P. et al. Jour Pediatrics. 1999;134:5: Abrahamsen TG. Et al. Pediatrics. 1996;98:")
20
Management of severe red cell alloimmunisation - IV Immune globulin
Prevent placental Fc-mediated endocytosis reduce passage maternally-derived alloantibodies

21
IVIG and Viral Safety No disease transmission by any products since 1994 Viral inactivation continue to improve Solven/ Detergent remains the most commonly used method of viral inactivation The requirements for donor screening and transmissible disease testing of input plasma are stringent . In addition, the IVIG manufacturing process itself includes at least 1 and usually 2 steps of viral inactivation

22
Role Of IVIG in Management of red cell alloimmunisation Options for severe early disease ( studies )
 .")
23
Retrospective case series (n=1-30) interpretation difficult;
- Variable severity (pre- or post- first IUT) - 1g/kg/wk (from as early as 8w) -Variable effects
 - 1g/kg/wk (from as early as 8w) -Variable effects.")
24
Management of severe red cell alloimmunisation IV Immune globulin
IV IG IVIG + IUT IV IG + plasmaphoresis +/- IUT

25
Management of severe red cell alloimmunisation IV Immune globulin
IV IG IVIG + IUT IV IG + plasmaphoresis +/- IUT

26
Margulies et al. conducted the largest prospective series
to date in which 24 severely Rh-sensitized pregnant women were treated with IVIG alone until delivery and Demonstrated that IVIG use should be initiated before 28 weeks or before the appearence of hydrops.

27
Management of severe red cell alloimmunisation IV Immune globulin
IV IG IVIG + IUT IV IG + plasmaphoresis +/- IUT

29
GA first IUT greater and fetal mortality 36% lower in combined group
Voto et al IUT vs IUT + IVIG GA first IUT greater and fetal mortality 36% lower in combined group

30
Connan et al. reported a case series of six women at high-risk for severe disease who were treated with weekly IVIG infusions and were monitored with MCA Doppler ultrasound to time the required IUTs; All experienced improved perinatal outcomes

31
Management of severe red cell alloimmunisation IV Immune globulin
IV IG IVIG + IUT IV IG + plasmaphoresis +/- IUT

32
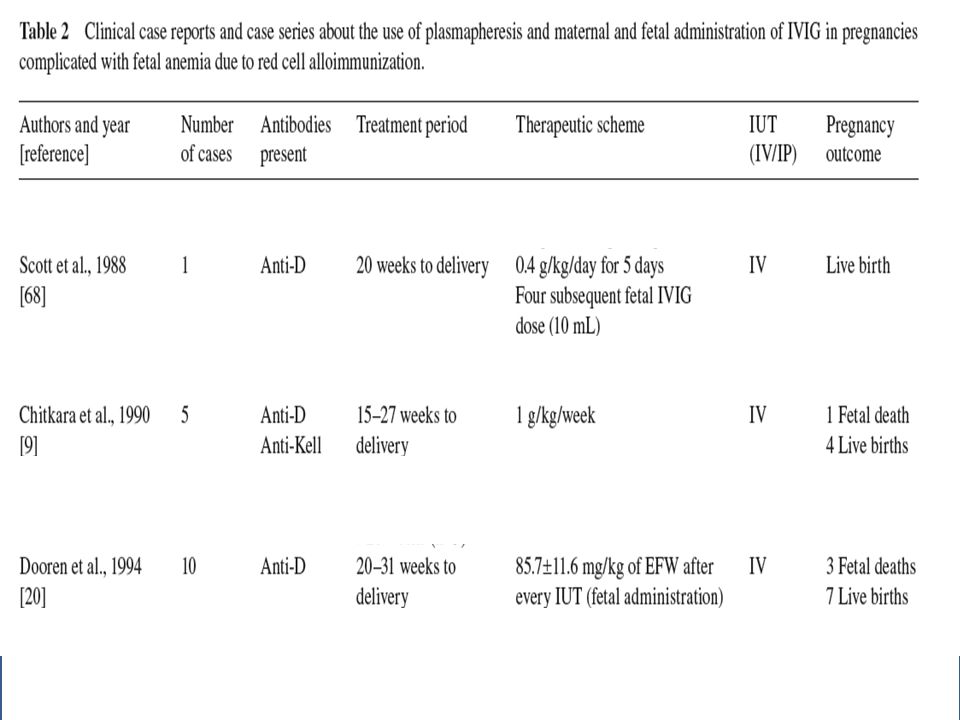
Management of severe red cell alloimmunisation-IV IG + plasmaphoresis +/- IUT
in a case series with nine fetuses (fi ve with anti-D and four with anti-K), concluded that the combined immunomodulation could be theorized a successful treatment modality because all the fetuses survived, with a mean gestational age at delivery of 34 weeks, maternal antibody titers were significantly reduced after plasmapheresis and remained stable during IVIG therapy
, concluded that the. combined immunomodulation could be theorized a successful treatment modality because all the fetuses survived, with a mean gestational age at delivery of 34 weeks, maternal antibody titers were significantly reduced after plasmapheresis and remained stable during IVIG therapy.")
33
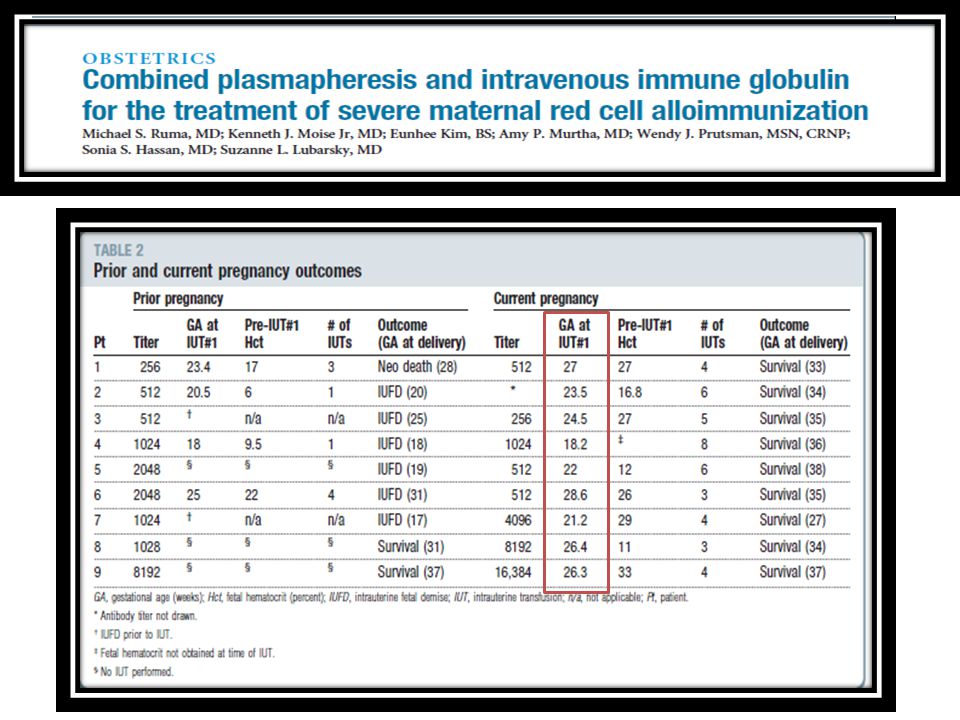
Management of severe red cell alloimmunisation Combined plasmapheresis & IVIG
Ruma et al severe cases (IUFD w or high titre) 3 x single volume plasmaphersis (after 12 w) with volume replaced with 5% albumin then IVIG 1g/kg/wk to 20 wk
 3 x single volume plasmaphersis (after 12 w) with volume replaced with. 5% albumin then. IVIG 1g/kg/wk to 20 wk.")
35
Management of severe red cell alloimmunisation Combined plasmapheresis & IVIG
RESULTS Fetus : All 9 fetuses subsequently required intrauterine transfusions (median 4; range 3-8). Infant : All infants survived with a mean gestational age at delivery of 34 weeks (range weeks). Maternal antired cell titers : were significantly reduced after plasmapheresis (P <.01) and remained decreased during IVIG therapy. Serial peak middle cerebral artery velocities : remained below the threshold for moderate to severe fetal anemia during therapy.
. Infant : All infants survived with a mean gestational age at delivery of 34 weeks (range weeks). Maternal antired cell titers : were significantly reduced after plasmapheresis (P <.01) and remained decreased during IVIG therapy. Serial peak middle cerebral artery velocities : remained below the threshold for moderate to severe fetal anemia during therapy.")
36
Management of severe red cell alloimmunisation Combined plasmapheresis & IVIG
RESULTS Fetus : All 9 fetuses subsequently required intrauterine transfusions (median 4; range 3-8). Infant : All infants survived with a mean gestational age at delivery of 34 weeks (range weeks). Maternal antired cell titers : were significantly reduced after plasmapheresis (P <.01) and remained decreased during IVIG therapy. Serial peak middle cerebral artery velocities : remained below the threshold for moderate to severe fetal anemia during therapy. CONCLUSION Combined immunomodulation with plasmapheresis and IVIG represents a successful approach to the treatment of severe maternal red cell alloimmunization.
. Infant : All infants survived with a mean gestational age at delivery of 34 weeks (range weeks). Maternal antired cell titers : were significantly reduced after plasmapheresis (P <.01) and remained decreased during IVIG therapy. Serial peak middle cerebral artery velocities : remained below the threshold for moderate to severe fetal anemia during therapy. CONCLUSION. Combined immunomodulation with plasmapheresis and IVIG represents a successful approach to the treatment of severe maternal red cell alloimmunization.")
37
Management of severe red cell alloimmunisation-IV IG + plasmaphoresis +/- IUT

38
Case Report

39
Successful Management of Severe Hemolytic Disease of Newborn using a
Management of severe red cell alloimmunisation Combined plasmapheresis & IVIG- Case Report Successful Management of Severe Hemolytic Disease of Newborn using a Combined Immunomodulatory Regimen: TPE, IVIG, Intrauterine Transfusion and RhIG Bandarenko N., Stagg K.,Immel Caroline C., Moise K.M., Moise K

40
5 subsequent successful IUTs over 3 months
Management of severe red cell alloimmunisation Combined plasmapheresis & IVIG- Case Report First IUT at 19.2 weeks 5 subsequent successful IUTs over 3 months anti D, anti-C and anti-G Jka 60% reduction with each procedure sensitized mother with Severe HDN multiple alloantibodies with markedly elevated titers (Multiple more 1:16000). 3 TPE procedures performed every other day Loading dose of IVIG (2 gm/kg) Immediately following after the 3rd TPE Bandarenko N., Stagg K.,Immel Caroline C., Moise K.M., Moise
. 3 TPE procedures. performed every other day. Loading dose of IVIG (2 gm/kg) Immediately following after the 3rd TPE. Bandarenko N., Stagg K.,Immel Caroline C., Moise K.M., Moise")
42
RED CELL ALLOIMMUNIZATION Immune Therapy
• Single volume plasmapheresis in week 10 on M, W, F (5% albumin for replacement) • 1 gr/kg IVIG load after last plasmapheresis • 1 gr/kg IVIG load the following day • 1 gr/kg IVIG weekly until 20 weeks’ gestation
 • 1 gr/kg IVIG load after last plasmapheresis. • 1 gr/kg IVIG load the following day. • 1 gr/kg IVIG weekly until 20 weeks’ gestation.")
43
IVIG—Is It the Answer? Disease Nature --------
IUT – related issues Does IVIG has a real role----- Maternity Hospital – related issues Long term outcome in children treated with IUT d/t RBC alloimmunization Reaserch interest in the monitoring and treatment of fetal anemia

44
IVIG—Is It the Answer? Disease Nature IUT – related issues Does IVIG has a real role----- Maternity Hospital – related issues Absence of highly qualified feto-maternal specialist Long term outcome in children treated with IUT d/t RBC alloimmunization Reaserch interest in the monitoring and treatment of fetal anemia

45
IVIG—Is It the Answer? Disease Nature --------
IUT – related issues Does IVIG has a real role----- Maternity Hospital – related issues Long term outcome in children treated with IUT d/t RBC alloimmunization Reaserch interest in the monitoring and treatment of fetal anemia

47
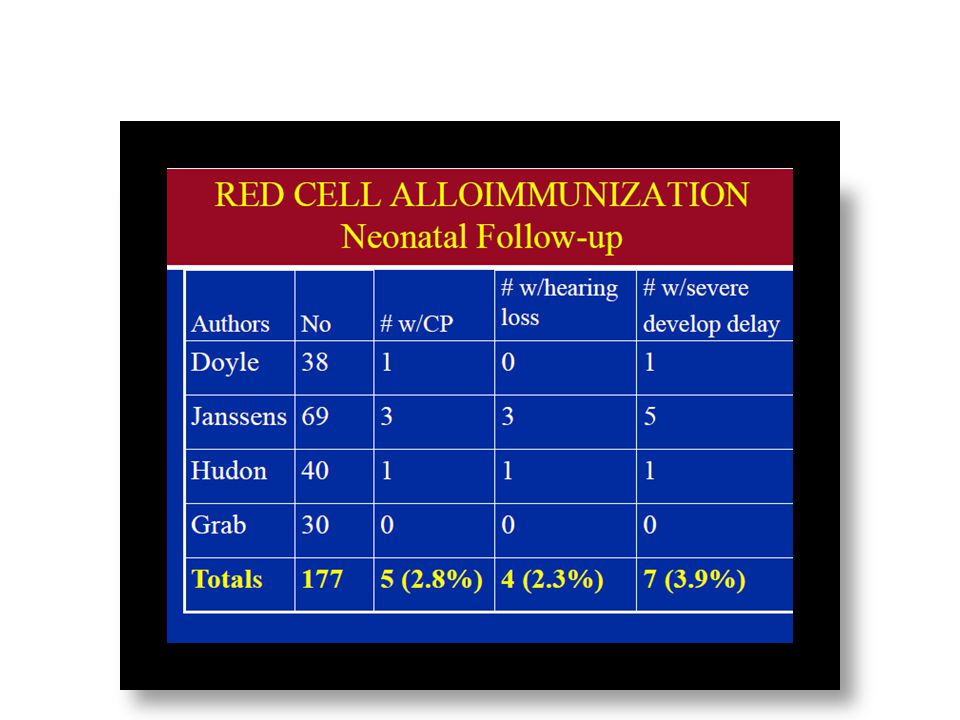
Long-Term Outcome- the LOTUS study
Perinatal survival-91% (389/426) •338 (87%) children were included (age 2-17) • neurodevelopmental impairment was detected in 9% (31/338): –Severe developmental delay ( 23) –Cerebral palsy (5) –Bilateral deafness (3) study SMFM 2011
 •338 (87%) children were included (age 2-17) • neurodevelopmental impairment was detected in 9% (31/338): –Severe developmental delay ( 23) –Cerebral palsy (5) –Bilateral deafness (3) study SMFM")
48
Long-Term Outcome- the LOTUS study
•Risk factors for NDI: –Hemoglobin at first IUT –Presence of fetal hydrops –Number of IUT’s –Severe neonatal morbidity SMFM 2011

49
IVIG—Is It the Answer? Disease Nature --------
IUT – related issues Does IVIG has a real role----- Maternity Hospital – related issues Long term outcome in children treated with IUT d/t RBC alloimmunization Reaserch interest in the monitoring and treatment of fetal anemia

52
The focus of research interest has shifted from the invasive management to a non-invasive monitoring and treatment of fetal anemia

54
Future Immune Therapy Maternal intravenous immune globulin
Paternal Leukocyte immunization to create antibodies Intranasal RHD peptides to desensitize Whitecar et al. Am J Obstet Gynecol 2002;187: Hall et al. Blood 2005;105:2175-9

55
IVIG—Is It the Answer? Intravenous immune globulin should not be expected to eliminate the need for intravascular transfusions but can prolong the interval before the first procedure is necessary the inactivation of the FcRn receptor ( prevents the catabolism of IgG,) resulting in increased catabolism of the harmful antibodies as well IVIG has been noted to decrease the passage of maternal anti-D CONCLUSIONS IVIg may enter fetal blood circulation via placenta, and adjust fetal immune ability to reduce the degree of fetal hemolysis. Immune therapy in established cases of alloimmunisation show promise but has yet to be translated into routine clinical management.
 resulting in increased catabolism of the harmful antibodies as well. IVIG has been noted to decrease the passage of maternal anti-D. CONCLUSIONS IVIg may enter fetal blood circulation via placenta, and adjust fetal immune ability to reduce the degree of fetal hemolysis. Immune therapy in established cases of alloimmunisation show promise but has yet to be translated into routine clinical management.")
56
Intravenous immunoglobulin
Early-onset Rh alloimmunization was offered as a promising therapy limited data were available to support it widespread use. evaluated in patients with Severe Rh immunization, High maternal antibody titers, and Previous pregnancy with early-onset hydrops and intrauterine death and has been related to Reduction in overall IUT requirements and Beneficial effect on pregnancy outcome.

57
Management of red cell alloimmunisation Options for severe early disease
Weekly US (from 14 w) with intravascular transfusion if hydropic (from 17 w) Intraperitoneal transfusion (from 14 w) (Howe & Michailidis 2007) Plasmapheresis (from 12 w) IV immune globulin (1g/kg/wk from 12 wk)
 with intravascular. transfusion if hydropic (from 17 w) Intraperitoneal transfusion (from 14 w) (Howe & Michailidis 2007) Plasmapheresis (from 12 w) IV immune globulin (1g/kg/wk from 12 wk)")
58
THANK YOU

Similar presentations





>")
















