Download presentation
Presentation is loading. Please wait.

1
Special Forms of Strabismus
Abbas Attarzadeh MD Professor of ophthalmology SUMS

2
Duane Syndrome Retraction of the globe in actual or attempted adduction. Horizontal eye movement is usually somewhat limited in both directions. Upshoot or downshoot (leash phenomenon) of the affected eye in attempted adduction co-contraction of the medial and lateral rectus muscles and, alternatively, to slipping of the lateral rectus muscle over the outer aspect of the eye.
 of the affected eye in attempted adduction. co-contraction of the medial and lateral rectus muscles. and, alternatively, to slipping of the lateral rectus muscle over the outer aspect of the eye.")
4
Most cases of Duane syndrome are sporadic
5%-10% show autosomal dominant inheritance A higher prevalence in females

5
In most anatomical and imaging studies, the nucleus of the sixth cranial nerve is absent, and an aberrant branch of the third cranial nerve has innervated the lateral rectus muscle

6
Electromyographic studies have shown:
paradoxical innervation of the lateral rectus muscle (innervation on attempted adduction and reduced innervation on attempted abduction). Anomalous synergistic innervation of the medial, inferior, and superior rectus muscles and the oblique muscles
. Anomalous synergistic innervation of the medial, inferior, and superior rectus muscles and the oblique muscles.")
7
Although considered an innervational anomaly: Tight and broadly inserted medial rectus muscles Fibrotic lateral rectus muscles, with corresponding forced duction abnormalities, are often encountered at surgery.

8
Clinical Features Poor abduction, frequently with primary position esotropia Poor adduction and exotropia Poor abduction and adduction, with esotropia, exotropia, or no primary position deviation 50%-80% in several series About 15% of cases are bilateral;

9
DDX with sixth nerve palsy
Careful observation for globe retraction on adduction lack of correspondence between the absent or typically modest primary position esotropia and the usually profound abduction deficit A further point of differentiation is that, even in esotropic Duane syndrome, a small-angle exotropia frequently is present in gaze to the side opposite the affected eye

10
Management Indications for surgery
Primary position deviations Abnormal head position Marked globe retraction Large upshoots or downshoots

11
Duane syndrome with esotropia
Recession of the medial rectus muscle on the involved side Bimedial rectus recession recommended for deviations over 20∆ in primary position Resection of the lateral rectus muscle for Duane syndrome with esotropia is not favored because of the likelihood that globe retraction will worsen, although one study reported favorable results with unilateral recession-resection procedures

12
Bimedial Rectus Recess

13
Partial or full transposition of the vertical rectus muscles has been advocated to improve abduction but may exaggerate the effects of co-contraction. Posterior scleral fixation of the transposed portions of the vertical rectus muscles, as described by Foster, has been found helpful, no only in Duane syndrome but in several types of paralytic strabismus as well

14
Surgery

15
The value of botulinum injection into the medial rectus muscle to improve abduction is controversial

16
Duane syndrome with exotropia and deficient adduction (type 2)
Recession of the lateral rectus on the involved side for small deviations Both lateral recti for large deviations with avoidance of resection of the medial rectus The latter aspect is especially important when an up- or downshoot is present on attempted adduction, because this finding indicates severe co-contraction

17
type 3 Duane syndrome who have poor abduction and adduction
Have straight eyes in or near the primary position and little, if any, head turn Severe globe retraction may be helped by: Recession of both the medial and the lateral rectus muscles Splitting the lateral rectus muscle in a Y configuration A posterior fixation procedure on LR Disinsertion of the lateral rectus muscle and reattachment to the lateral wall of the orbit is the most recent procedure to be tried

18
LLR recess 13 mm + Bifurcation
LMR Bifurcation

19
Brown Syndrome

20
Shortening of the anterior sheath of the superior oblique tendon.
Brown syndrome was described by Harold W. Brown in 1950 as the superior oblique tendon sheath syndrome. restriction of elevation in adduction Shortening of the anterior sheath of the superior oblique tendon. Restriction of the superior oblique tendon at the trochlear pulley abandoned this theory

21
Brown Syndrome Restriction of the superior oblique tendon at the trochlear pulley

22
Brown syndrome Congenital Acquired form
bilateral in approximately 10% of cases Congenital Acquired form Trauma in the region of the trochlea Systemic inflammatory Resolution of congenital Brown syndrome is unusual but possible intermittent Brown syndrome, which may resolve spontaneously.

23
Comparison of Inferior Oblique Muscle Palsy With Brown Syndrome
Deficient elevation in adduction that improves in abduction but often not completely Inferior Oblique Muscle Palsy Brown Syndrome Forced ductions Negative Positive Strabismus pattern A pattern V pattern Superior oblique muscle overaction Usually present None or minimal In adduction, the palpebral fissure widens and a downshoot of the involved eye is often seen; it can be distinguished from superior oblique muscle overaction because downshoot in the latter condition occurs less abruptly as adduction is increased.

24
Brown syndrome OS Divergence in upgaze
Down shoot in attempted elevation in adduction? Down shoot in attempted elev. in adduct. (different than IO palsy)
")
25
Brown syndrome mild moderate severe hypotropia in primary position no
yes downshoot of the eye in adduction. chin-up head posture and sometimes by a face turnaway from the affected eye insever cases

26
in adduction is essential for the diagnosis of Brown syndrome.
An unequivocally positive forced duction test demonstrating restricted passive elevation in adduction is essential for the diagnosis of Brown syndrome. Retropulsion of the globe during this determination stretches the superior oblique tendon and accentuates the restriction. When inferior rectus muscle fibrosis or inferior orbital blowout fracture (the principal entities to be differentiated) produces a restrictive elevation deficiency, the limitation to passive elevation is accentuated by forceps-induced proptosis of the eye rather than by retropulsion.
 produces a restrictive elevation deficiency, the limitation to passive elevation is accentuated by forceps-induced proptosis of the eye rather than by retropulsion.")
27
Management Observation alone in about two thirds of all Brown syndrome cases rheumatoid arthritis or other systemic inflammatory diseases Systemic treatment Corticosteroids injected near the trochlea Sinusitis has also led to Brown syndrome CT of the orbits and paranasal sinuses

28
Surgical treatment is indicated for the most severe cases
Primary position hypotropia Anomalous head posture Iatrogenic superior oblique muscle palsy may occur postoperatively. 44%-82% sheathectomy has been abandoned in favor of ipsilateral superior oblique tenotomy

29
Brown Syndrome SO tenotomy
SR SR LR RM MR LR IR IR IO IO

30
Superior oblique muscle palsy
Reduced: By careful preservation of the intermuscular septum during tenotomy. This modification often produces an early under correction that gradually improves with time

31
Perform simultaneous ipsilateral inferior oblique muscle weakening.
guarded tenotomy using an inert spacer sewn to the cut ends of the superior oblique tendon Controlling the gap between the cut ends with an adjustable suture These procedures eliminate the need for simultaneous inferior oblique muscle weakening but sometimes result in a downgaze restriction due to adhesions to the nasal border of the superior rectus muscle. Care must be taken to avoid contact of the spacer to nearby structures by preserving the intermuscular septum

32
For those surgeons who are a little too chicken to completely cut the SO tendon and cause a SO palsy… Chicken suture technique

33
Brown Syndrome Chicken suture

34
For those surgeons with a sense of humor… Try the rubber chicken trick aka silicone expander

35
Brown Syndrome Silicone expander

36
Facia Lata

37
Third Cranial (Oculomotor) Nerve Palsy
 Nerve Palsy")
38
Traumatic 3rd N palsy

39
The causes of third cranial nerve palsy in children
Congenital disorders (40%-50%) Trauma Inflammation Viral infection Migraine (Infrequently) neoplastic lesions Adults Intracranial aneurysm Diabetes, Neuritis Infection Rarely, tumor Diabetic third cranial nerve palsy generally resolves spontaneously within 3-4 months. The majority of adults referred for surgical treatment have palsy due to trauma
 Trauma. Inflammation. Viral infection. Migraine. (Infrequently) neoplastic lesions. Adults. Intracranial aneurysm. Diabetes, Neuritis. Infection. Rarely, tumor. Diabetic third cranial nerve palsy generally resolves spontaneously within 3-4 months. The majority of adults referred for surgical treatment have palsy due to trauma.")
40
Clinical Features Limited: Adduction Elevation Depression
Exotropia and often Hypotropia Upper lid ptosis usually is present, often with a pseudoptosis

41
Aberrant regeneration (misdirection)
")
42
Niknam Farshad 23 yo accident 4years ago 3rd nerve palsy aberrant regeneration

43
Management Except in congenital cases of third cranial nerve palsy, it is advisable to wait 6-12 monthsfor any spontaneous recovery before surgical correction is planned. Patients with at least partial recovery are much better candidates for good functional, as well as cosmetic, results,

44
Cured III N palsy

45
Third cranial nerve palsies present difficult surgical challenges because multiple extraocular muscles as well as the levator may be involved. Replacing all of the lost rotational forces on the globe is impossible; therefore, the goals of surgery must be thoroughly discussed With patients so their expectations are realistic, Adequate alignment for binocular function in primary position and in slight downgaze for reading may be all that can be expected.

46
Sadravy Bahareh post surgery rt 3rd N palsy 15 years po 9.3.86

47
surgical procedure A large recession-resection procedure on the horizontal rectus muscles to correct the exodeviation, with supraplacement of both to correct the hypotropia Most surgeons reserve correction of ptosis for a subsequent procedure Some surgeons use superior oblique tenotomy instead of supraplacement of the horizontal rectus muscles for hypotropia

48
Sixth Cranial (Abducens) Nerve Palsy
Sixth nerve palsy.ppt

49
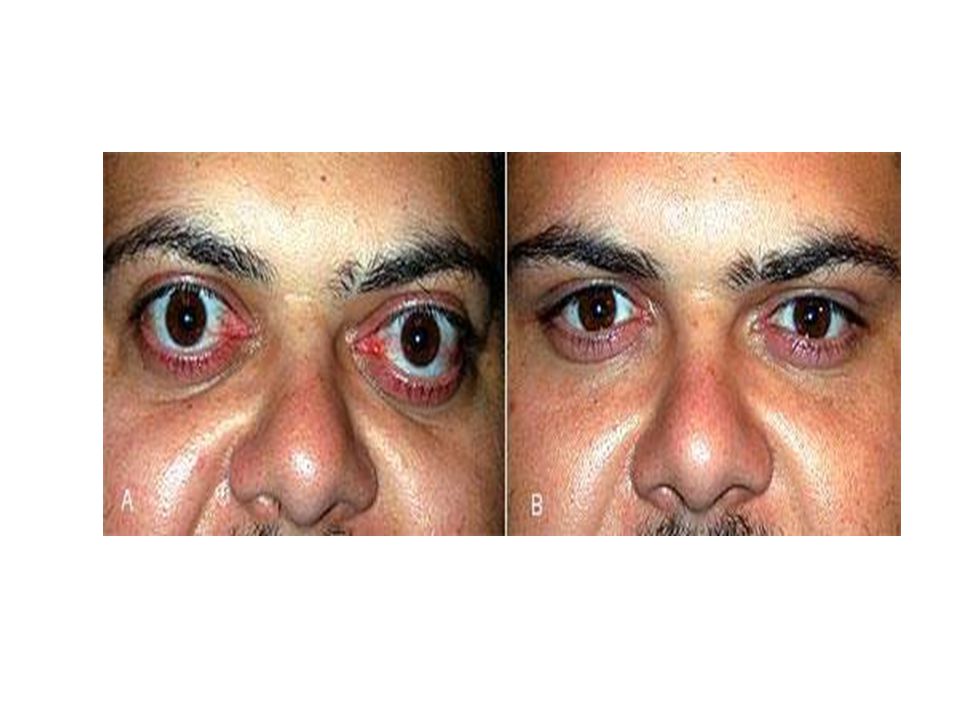
Graves Eye Disease motility disturbances

50
Edema, inflammation, and fibrosis are present in this disease because of lymphocytic infiltration. These conditions result in massive enlargement of affected extraocular muscles and may not only restrict motility but also cause compressive optic neuropathy.

52
Detection of this muscle enlargement by orbital ultrasound, CT, or MRI helps confirm the diagnosis of Graves eye disease.

53
The myopathy is not caused by thyroid dysfunction
Some patients with Graves disease also have myasthenia gravis It is mostly a disease of adults but can occur in children.

54
Clinical Features Severe restrictive, The muscles affected, in decreasing order of severity and frequency: inferior rectus medial rectus Superior rectus lateral rectus The condition most often is bilateral and asymmetric. Forced duction test results are almost always positive in 1 or more directions.

55
Upper eyelid retraction often is present.
The patient presents most often with some degree of proptosis, hypotropia, or esotropia Upper eyelid retraction often is present. Graves eye disease is a common cause of acquired vertical deviation in adults, especially females, but is rare in children

56
Management Indications for strabismus surgery: Diplopia
Abnormal head position Surgery may eliminate diplopia in primary gaze but rarely restores normal motility

57
waiting for at least 6 months is recommended.
It is important to establish stability of the strabismus measurements before surgery is performed waiting for at least 6 months is recommended. Half of the patients required repeated operation Strengthening procedures are rarely performed because they usually worsen restriction

58
Adjustable sutures are helpful in these difficult cases.
Slight initial undercorrection is desirable, because late progressive overcorrection is common, especially with large inferior rectus recessions. Nonabsorbable sutures may decrease the likelihood of overcorrection. Limited depression of the eyes after inferior rectus muscle recessions can interfere with bifocal use by patients Proptosis can become worse after extraocular muscle recessions.

59
Hint If the need for orbital decompression is foreseeable, it is usually preferable to postpone strabismus surgery until that has been accomplishe Likewise, eyelid surgery usually is performed at a later time because upper eyelid retraction may be improved when the patient no longer strains to elevate the eye lid

60
Large recessions of very tight inferior rectus muscles can cause lower eyelid retraction severe enough to require subsequent eyelid surgery. Severing the lower eyelid retractors as part of the strabismus surgery has led to some success at preventing this complication. If necessary, a spacer of banked sclera or synthetic material can be placed to vertically lengthen the lower lid tarsus

61
Which patients require surgery?
Emergent basis optic nerve compression corneal exposure Non emergent severe disfiguring proptosis double vision from restrictive myopathy eyelid retraction

62
What kinds of surgery are done in patients with TRIO?
Orbital decompression Eye muscle surgery Eyelid surgery needs to be done in this order Decompression affects ocular motility and may alter muscle surgery muscle surgery should be completed before eyelid surgery

63
Which patients require orbital decompression?
Optic nerve compression : EOM swelling with relatively little space at the apex of the orbit squeezing of the optic nerve at the apex of the orbit Severe proptosis resulting in corneal exposure or disfigurement

65
When do patients require muscle surgery?
Double vision in functional field Ensure that the inflammation is quiet and the patient's motility pattern is stable Repeated stable measurements over 6+ months help to ensure that motility is stable

66
What are the alternatives to muscle surgery?
prisms in glasses works for patients with double vision and relatively small deviations It is better that the motility become stable before prisms are prescribed Temporary Fresnel prisms may be helpful during periods of instability

67
Botulinum toxin A injection has a good effect in the treatment of restrictive strabismus in TAO.
Early treatment has better results. Dosage in TAO is higher, the mean changes of degree of deviation is slighter, the interval between injections and the duration of effect is shorter. Injection dosage should increase after repeated injections.

68
What type of muscle surgery is required?
Recession of muscles, usually on an adjustable suture basis Muscles are tight and scarred, resection is not indicated Inferior and medical rectus muscles are the most common targets Forced duction test at the time of surgery is indicated

69
Does eye muscle surgery affect the eyelids?
Recession of the tight IR often improves upper eyelid retraction: SR had to work against the tight IR, thus the associated levator muscle was overactive, causing eyelid retraction. When the IR is recessed, the overactivity relatively ends Large recession of IR may worsen inferior lid retraction

70
What kind of eyelid surgery is done?
Eyelid retraction Orbital decompression lowers eye, improving the lower lid retraction Mild lid retraction: recession of the eyelid retractors (upper or lower) is adequate Severe retraction: spacers are needed, such as hard palate in the lower lids and fascia in the upper lids Blepharoplasty and/or brow lift Excessive skin from chronic swelling At the same time or later date
 is adequate. Severe retraction: spacers are needed, such as hard palate in the lower lids and fascia in the upper lids. Blepharoplasty and/or brow lift. Excessive skin from chronic swelling. At the same time or later date.")
72
How many surgeries do patients with TRIO require?
Most do not require surgery Patients who need surgery may need from 1 to as many as 8-10 times over 2-3 years of reconstruction

73
Chronic Progressive External Ophthalmoplegia

74
Clinical Features Chronic progressive external ophthalmoplegia (CPEO) usually begins in childhood with: Ptosis Slowly progresses to total paralysis of the eyelids and extraocular muscles

75
CPEO may be sporadic or familial.
Although a true pigmentary retinal dystrophy usually is absent, constricted fields and electro diagnostic abnormalities can occur.

76
Defects in mitochondrial DNA have been found in some patients.
The triad of : Retinal pigmentary changes CPEO Cardiomyopathy (especially heart block) is called Kearns-Sayre syndrome
 is called Kearns-Sayre syndrome.")
77
Management Treatment options are limited. Cautious surgical elevation (suspension) of the upper eyelids indicated to lessen a severe chin-up head position.
 of the upper eyelids indicated to lessen a severe chin-up head position.")
78
Myasthenia Gravis

79
Myasthenia Gravis Onset of myasthenia gravis may occur at any age but is uncommon in children. A transient neonatal form, caused by the placental transfer of acetylcholine receptor antibodies of mothers with myasthenia gravis, usually subsides rapidly. Another variety is not immune mediated and exhibits a familial incidence.

80
The disease may be purely ocular
(30%-50%) occurs as part of a major systemic disorder Childhood myasthenia gravis is more common in females.
 occurs as part of a major systemic disorder. Childhood myasthenia gravis is more common in females.")
81
Clinical Features The principal ocular manifestation is extraocular muscle weakness, including weakness of the levator muscle. The majority of cases (90%) have both ptosis and limited ocular rotations.
 have both ptosis and limited ocular rotations.")
82
Ptosis typically increases when the patient is
required to look upward for 30 seconds Sleep test, ptosis often resolves after 20-30 minutes in a dark room with the eyelids closed. Cogan twitch overshoot of the eyelid when the patient looks straight ahead after looking down for several minutes

83
Neostigmine (Prostigmine) test Ice test
Tensilon test Neostigmine (Prostigmine) test Ice test External application of ice for 2-5 minutes improves function of the levator and other affected extraocular muscles, giving a rapid and reliable method of establishing this diagnosis without the need for drug administration.
 test. Ice test. External application of ice for 2-5 minutes improves function of the levator and other. affected extraocular muscles, giving a rapid and reliable method of establishing this diagnosis. without the need for drug administration.")
84
Electromyography shows decreased electrical activity of involved muscles after prolonged voluntary innervation an increased activity (including saccadic velocity) after the administration of edrophonium or neostigmine. Documentation of abnormalities in single-fiber electromyography or the presence of circulating antiacetylcholine receptor antibodies is confirmatory although a negative result does not rule out the presence of this disease.
 after the administration of edrophonium or neostigmine. Documentation of abnormalities in single-fiber electromyography or the presence of circulating antiacetylcholine receptor antibodies is confirmatory. although a negative result does not rule out the presence of. this disease.")
Similar presentations







To improve function and apperance 2)To (may) relieve asthenopia and double vision 4)To restore.>")





 Journal of American Association for Peadiatric Ophthalmology and strabismus 2008.>")





 925-4. Classical Signs : TAO A prominent stare. Retraction of all four eyelids Bilateral exophthalmos Hertel exophthalmometer.>")


. Imaging X-ray shows sublaxation, dislocation, narrow joint space, bone erosion, calcification in soft tissues Arthrography.>")
