Download presentation
Presentation is loading. Please wait.

1
HIV and the Surgeon Paul MacPherson PhD, MD, FRCPC
Assistant Professor of Medicine Division of Infectious Diseases Ottawa Hospital, General Campus University of Ottawa

2
Summary HIV today HIV infection and natural history Current treatments for HIV infection Indications for surgery in HIV+ patients Surgical outcomes for HIV+ patients Needlestick injuries

3
Today’s Reality

4
HIV: A Global Pandemic

7
6,850/day 285/hour

9
5,753/day 240/hour

10
Current Demographics in Canada

11
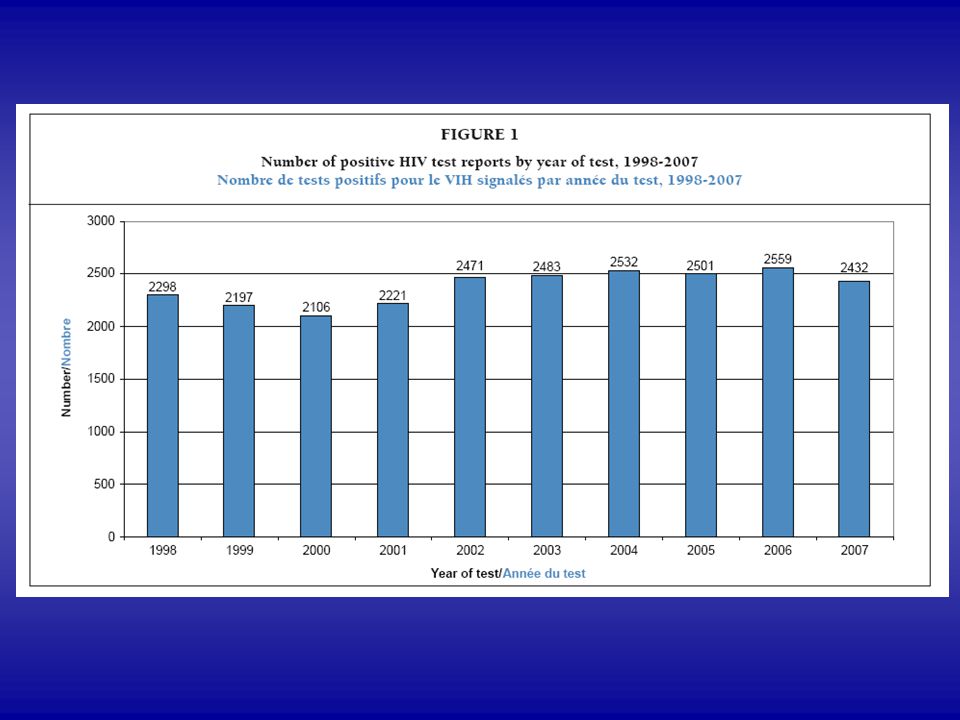
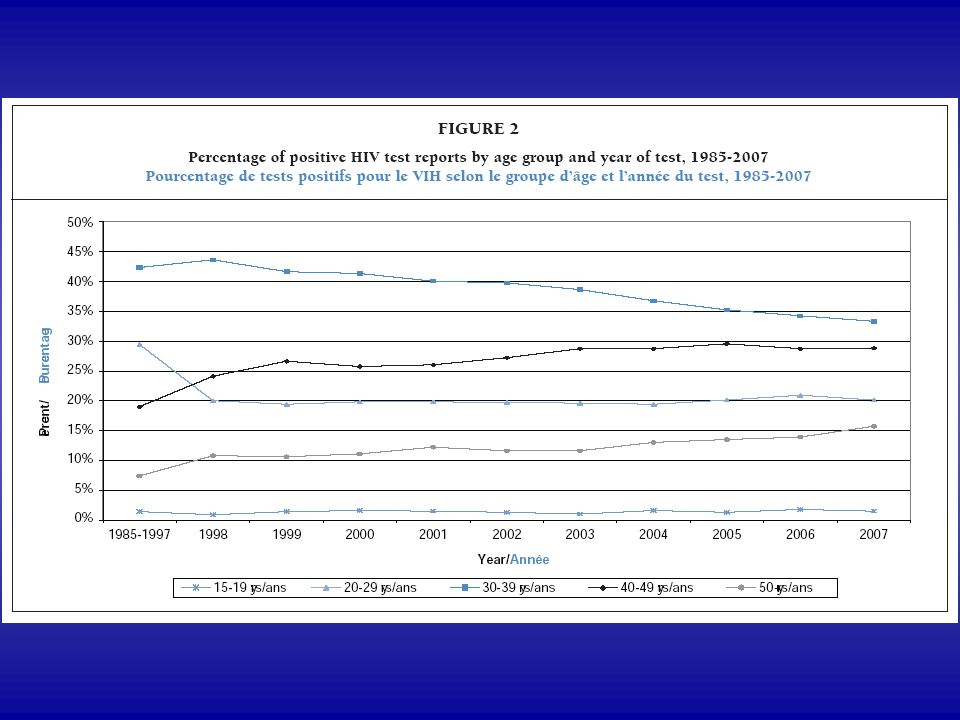
Demographic Trends 1. HIV+ tests (all ages) highest in 1995 at 2,990
lowest in 2000 at 2,106 increased in 2001 and 2002 and then plateaued at 2,500 2. Increasing among older adults (age >40 yrs) 3. HIV+ tests among MSM: increasing since 2001 4. Steady decline among injection drug users 5. Steady increase among Heterosexuals 68% increase in Ontario over the past 5 years (11%/yr)
 3. HIV+ tests among MSM: increasing since Steady decline among injection drug users. 5. Steady increase among Heterosexuals. 68% increase in Ontario over the past 5 years (11%/yr)")
15
HIV Epidemiology Developing World Developed World
Heterosexual men and women Children Developed World Men who have sex with men People from endemic countries Aboriginals People who use injection drugs

16
HIV Transmission

17
Sexual contact with exchange of bodily fluids
Transmission Sexual contact with exchange of bodily fluids Exposure of mucous membranes Sharing injection drug paraphernalia Needles, snorting straws Transfusion of infected blood or blood products Currently 1 in 500,000 Mother to child (vertical) Perinatal and breast feeding
 Perinatal and breast feeding.")
18
Sexual Transmission of HIV:
HIV is contained in: Semen Vaginal secretions Rectal secretions (Saliva at very low levels)
")
19
Exposure to HIV In these fluids: HIV is present as free virus HIV is contained in infected CD4 cells

20
Mucous Membranes: the target
Mucous membranes are the moist epithelial linings of body cavities including the: oral cavity rectum vagina and cervix inner foreskin Live cells line the surface.

21
Mucous Membrane: the target
Only 2% of the body’s immune cells circulate in the blood 98% of the body’s immune cells are located in the lymph nodes and the mucous membranes Mucous membranes are rich in T-cells and macrophages to provide defence The majority of these cells are organized into “lymphoid follicles” just under the surface of the mucosal membrane

22
Mucous Membrane: rectum
Lymphoid follicles: 15/cm2 in the colon and increase to 25/cm2 in the rectum.

23
Mucous Membrane: the target
M-cells transport HIV directly into the lymphoid follicle Owen, RL. Pathobiology, 1998.

24
Mucous Membrane: cervix
Lymphoid follicle in the cervix. CD4 cells are stained brown Kobayashi, Am J Pathology, 2002

25
Mucous Membrane: the target
Hladik F. Immunity, 2007. McCoombe. AIDS, 2006.

26
Transmission: Injection drug paraphernalia
Sharing injection drug paraphernalia Access to clean needles Drug rehabilitation programs

27
Transmission: Blood transfusion
Transfusion of infected blood or blood products Screening donated blood ELISA: 2-3 month window period PCR: essentially no window period

28
Transmission: Mother to child
Mother to child (vertical) In utero (trans-placental) Peri-natal accounts for majority of cases By blood-blood mixing Breast feeding.
 In utero (trans-placental) Peri-natal accounts for majority of cases. By blood-blood mixing. Breast feeding.")
29
Virus

30
Human Immunodeficiency Virus

32
HIV and Immunology

33
Immunologic: Peripheral Blood
CD4 T-cells: infected, decrease, dysfunction, alterations in subsets CD8 T-cells: dysfunction, anergic, alterations in subsets Macrophages: infected, dysfunction NK cells: dysfunction B-cells: dysfunction- polyclonal hypergammaglobulinemia Cytokine dysregulation Lymph Nodes Hyperplastic and eventually fibrotic

34
Clinical

35
Natural History of HIV Disease

36
HIV Disease HIV enters the body and slowly destroys the immune system
without treatment, HIV is continuously active without treatment, the average length of time between infection and the onset of symptomatic disease is years the competency of the immune system is reflected by the CD4 count

37
Viral Load What is the viral load? How much virus per ml of blood
Range 100’s to >500,000 Viral load and progression are roughly correlated Each patient has their own “set-point”

38
CD4 Count What is the CD4 count? 800-1000 is normal >500 no worry
a bit of a gray zone. <200 at risk <50 at significant risk

39
Risk of Illness based on CD4 Count
>500: usually no symptoms. May have fever, night sweats, lymphadenopathy, weight loss : recurrent HSV, zoster, sinusitis, pneumonia candidiasis (oral, vaginal), lymphoma <200: PCP, Toxo, KS, Cryptococcus <50: MAC, CMV, PML, dementia, wasting
, lymphoma. <200: PCP, Toxo, KS, Cryptococcus. <50: MAC, CMV, PML, dementia, wasting.")
41
Cerebral Toxoplasmosis

42
Progressive Multifocal Leucoencephalopathy

43
CNS Lymphoma

44
Cryptococcal Meningitis

45
CMV Retinitis

46
Pneumocystis jeroveci pneumonia

47
Tuberculosis

48
Oral candidiasis

49
Esophageal Candidiasis

50
Kaposi’s Sarcoma

51
Bacillary angiomatosis
Red papular skin lesions Bartonella henselae CD4 < 50 Rx: Doxycycline Macrolide

52
Zoster VZV reactivation Acyclovir IV

53
Molluscum contagiosum
Umbilicated papules Pearly in appearance CD4 < 100 Rx: Liquid nitrogen Rx: HAART

54
Eosinophilic Folliculitis
CD4 < 200 Waxing and waning Moderate to severe pruritis 90% occur above T2 Rx: topical steroids

55
Seborrheic dermatitis
Erythematous plaques with greasy scales Face, ears, scalp, axilla Topical steroids with or without ketoconazole

56
HIV-Associated Wasting Syndrome

57
Antiretroviral Therapy The new era

58
Antiretrovirals Save Lives

59
Antiretrovirals reduce the rate of progression
No treatment Antiretrovirals years

61
Why Antiretroviral Therapy?

62
Why Antiretroviral Therapy?

63
Treatment Goals Maximal viral suppression (VL<50)
Undetectable does not mean absent Durable suppression Restoration and preservation of immune function Improved quality of life Reduction in morbidity and mortality Current projected life-expectancy from time of diagnosis: 43 years!

64
Antiretrovirals

65
Antiretrovirals: NRTI’s NNRTI’s Prot Inh’s
Abacavir Efavirenz Amprenavir Didanosine (EC) Nevirapine Atazanavir Emtricitabine Delavirdine Indinavir Lamivudine Etravirine Lopinavir Stavudine (XR) Other Nelfinavir Tenofovir T20 Ritonavir (Zalcitabine) Maraviroc Saquinavir Zidovudine Raltegravir Tipranavir Combivir (AZT+3TC) Darunavir Kivexa (ABC+3TC) Truvada (TDF+FTC)
 Nevirapine Atazanavir. Emtricitabine Delavirdine Indinavir. Lamivudine Etravirine Lopinavir. Stavudine (XR) Other Nelfinavir. Tenofovir T20 Ritonavir. (Zalcitabine) Maraviroc Saquinavir. Zidovudine Raltegravir Tipranavir. Combivir (AZT+3TC) Darunavir. Kivexa (ABC+3TC) Truvada (TDF+FTC)")
66
First Line Combinations (DHHS):
Protease Inhibitor-Based Regimens: ABC/TDF + 3TC/FTC + Kaletra (LPV/rit) ABC/TDF + 3TC/FTC + ATZ/rit ABC/TDF + 3TC/FTC + SQV/rit ABC/TDF + 3TC/FTC + DRV/rit NNRTI-Based Regimens: ABC/TDF + 3TC/FTC + EFV Avoid d4T + AZT d4T + ddI 3TC + emtricitabine
 ABC/TDF + 3TC/FTC + ATZ/rit. ABC/TDF + 3TC/FTC + SQV/rit. ABC/TDF + 3TC/FTC + DRV/rit. NNRTI-Based Regimens: ABC/TDF + 3TC/FTC + EFV. Avoid. d4T + AZT. d4T + ddI. 3TC + emtricitabine.")
67
Adverse Drug Effects

68
Adverse Effects: Drug Specific
AZT: marrow suppression, nausea d4T: neuropathy, lactic acidosis and lipodystrophy Abacavir: hypersensitivity reaction Tenofovir: renal failure Didanosine: peripheral neuropathy, pancreatitis Efavirenz: CNS symptoms, sleep disturbance Nevirapine: rash, hepatotoxicity Atazanavir: hyperbilirubinemia Lopinavir: diarrhea Saquinavir: GI intolerance Indinavir: nephrolithiasis

69
Adverse Effects: Lipodystrophy Syndrome
Hyperlipidemia: Total cholesterol, LDL and triglycerides Risk of atherosclerosis Pravastatin, Crestor and Fibrates are drugs of choice Lipodysmorphic Features Fat atrophy of face and limbs Fat accumulation dorsocervical pad, stomach, breasts Insulin Resistance May consider metformin

71
Mother to child transmission

72
Transmission of HIV from mother to infant occurs predominantly at the time of delivery.

73
Women and Infant Transmission Study, 1999
Viral Load Transmission < % 1000 – 10, % 10,000 – 50, % 50,000 – 100, % > 100, % Average risk of transmission to the infant: 30%

74
ACTG 076 Study (1994) Protocol: AZT given IV during labour
AZT to the infant for 6 weeks Success: 67.5% reduction in transmission From 30% to 8.3%

75
Reducing Mother to Child Transmission:
If mother not diagnosed previously: perinatal AZT and C-section (risk < 5%) If mother known HIV+: antiretroviral therapy beginning week 28 If mother known HIV+ and on antiretroviral therapy: continue therapy (change if on EFV) If maternal VL < 50, then risk of perinatal transmission < 1% Breast feeding only if no access to formula
 If mother known HIV+: antiretroviral therapy beginning week 28. If mother known HIV+ and on antiretroviral therapy: continue therapy (change if on EFV) If maternal VL < 50, then risk of perinatal transmission < 1% Breast feeding only if no access to formula.")
76
2008

78
Indications for surgery in HIV+ patients

79
Indications for Surgery: not on therapy
Intracranial lesion Primary CNS lymphoma Toxoplasma TB Gumma PML Bacterial abscess Stereotactic needle biopsy

80
Indications for Surgery: not on therapy
Lymph node biopsy lymphoma, TB, MAC Cholecystitis Cholelithiasis Crytosporidium, CMV, MAC

81
Indications for Surgery: on therapy
Coronary by-pass Antiretrovirals associated with increased lipids 50% of HIV+ individuals smoke cigarettes Increased rates of CVD Resection of malignancies Cervical cancer (HPV) Anal cancer (HPV) Lymphoma Hepatoma (No increase in breast or lung cancer)
 Anal cancer (HPV) Lymphoma. Hepatoma. (No increase in breast or lung cancer)")
82
Plastic Surgery

83
Lipoatrophy

84
HIV and Surgical Outcomes

85
HIV + ARV = excellent surgical outcomes

86
ARV and Surgery Impact of highly active antiretroviral therapy on outcome of cholecystectomy in patients with human immunodeficiency virus infection. Department of S. Siro Clinical Institute, University of Milan, Milan, Italy. Br J Surg Nov; 93(11): HAART was shown to be protective. A low HIV RNA load and a high CD4(+) cell count were significant predictors of uncomplicated surgical outcomes. CONCLUSION: HAART significantly reduces the risk of complications after cholecystectomy in patients with HIV infection.
: HAART was shown to be protective. A low HIV RNA load and a high CD4(+) cell count were significant predictors of uncomplicated surgical outcomes. CONCLUSION: HAART significantly reduces the risk of complications after cholecystectomy in patients with HIV infection.")
87
ARV and Surgery Outcomes of hysterectomy in HIV-seropositive women compared to seronegative women. Department of Gynecology and Obstetrics, Emory University, Atlanta, USA. Infect Dis Obstet Gynecol Sep;13(3):167-9. No significant differences in complication rates were found among HIV-infected women compared with uninfected women.
: No significant differences in complication rates were found among HIV-infected women compared with uninfected women.")
88
ARV and Surgery HIV-positive renal recipients can achieve survival rates similar to those of HIV-negative patients. Terasaki Foundation Laboratory, Los Angeles, CA, USA. Transplantation Jun 27;81(12): Although not statistically significant, graft survival was higher among HIV-positive patients compared with their negative controls, as was patient survival. Graft survival: 76.1% vs. 65.1% at 5 years (p=0.21) Patient survival: 91.3% vs. 87.3% at 5 years (p=0.72)
: Although not statistically significant, graft survival was higher among HIV-positive patients compared with their negative controls, as was patient survival. Graft survival: 76.1% vs. 65.1% at 5 years (p=0.21) Patient survival: 91.3% vs. 87.3% at 5 years (p=0.72)")
89
ARV and Surgery Excellent outcomes of cardiac surgery in patients infected with HIV in the current era. Department of Cardiothoracic Surgery, Mount Sinai Medical Center, New York Clin Infect Dis Aug 15;43(4):532-6. The surgeon and AIDS: twenty years later. Department of Surgery, Medical Center, University of California-Irvine, CA Arch Surg Oct;140(10):961-7. Since the first reports on indications and outcome for abdominal procedures in the HIV/AIDS patient were published 20 years ago, the epidemiology and presentation of surgical illness have changed remarkably with the advent of new antiviral regimens.
: The surgeon and AIDS: twenty years later. Department of Surgery, Medical Center, University of California-Irvine, CA. Arch Surg Oct;140(10): Since the first reports on indications and outcome for abdominal procedures in the HIV/AIDS patient were published 20 years ago, the epidemiology and presentation of surgical illness have changed remarkably with the advent of new antiviral regimens.")
90
Occupational Exposure

91
Occupational Exposures
Pietrabissa et al (1997) - surveyed 15,375 procedures in 39 hospitals by 122 surgeons over 6 months: a) 3.9% of procedures had percutaneous or eye exposures b) needle sticks accounted for 84% of injuries c) 58% occurred at wound closure d) direct correlation between length of procedure and number of injuries
 - surveyed 15,375 procedures in 39 hospitals by 122 surgeons over 6 months: a) 3.9% of procedures had percutaneous or eye exposures. b) needle sticks accounted for 84% of injuries. c) 58% occurred at wound closure. d) direct correlation between length of procedure and number of injuries.")
92
Occupational Exposures
Prospective surveillance of HCW exposed to HIV conducted by CDC from 1983 to 1992: 89% percutaneous 5% mucous membrane Of Percutaneous: 34% by syringe needles 40% by suture needles 4% by scaples 2% by lancets 4% other

93
Needle stick Injuries

94
What do we worry about? 1) Hepatitis B: 30% risk
- chronic hepatitis, cirrhosis, carcinoma 2) Hepatitis C: 3% risk 3) HIV: 0.3% risk
 Hepatitis C: 3% risk. 3) HIV: 0.3% risk.")
95
What do I do? 1) Don’t panic!
2) Dispose of the needle in a sharps container 3) Express blood from the wound 4) Clean thoroughly with Providone iodine, or chlohexidine, or soap and water 5) If eyes or mucous membranes: lots of water 6) Go to the Emergency Dept.
 Dispose of the needle in a sharps container. 3) Express blood from the wound. 4) Clean thoroughly with Providone iodine, or chlohexidine, or soap and water. 5) If eyes or mucous membranes: lots of water. 6) Go to the Emergency Dept.")
96
Risk Assessment: 1) You 2) The patient 3) The Injury
 You 2) The patient 3) The Injury")
97
You: 1) Are you vaccinated against HepB? 2) Are you immune to HepB?
Get your titers measured! 3) General health 4) Blood work: CBC, lytes, liver function
 General health. 4) Blood work: CBC, lytes, liver function.")
98
The Patient: 1) HIV status 2) HepB status 3) HepC status
Don’t Know? Then request: 1) HIV test STAT, with consent from patient 2) HBsAg, HBsAb 3) HCV-Ab and PCR
 HIV test STAT, with consent from patient. 2) HBsAg, HBsAb. 3) HCV-Ab and PCR.")
99
The Patient: Do know: 1) HIV: what is the viral load?
how sick is the patient? 2) HepB: is he/she sAg+
 HepB: is he/she sAg+")
100
The Injury: Risk Factors: depth of skin invasion?
Exposure to broken skin? hollow bore or suture needle? did the needle enter a blood vessel of the pt? visible blood on the needle? were you wearing gloves?

101
Post Exposure Prophylaxis

102
HIV Post Exposure Prophylaxis
There is minimal evidence for PEP: 1) case controlled study of HCW 2) ACTG 076, perinatal HIV transmission 3) Animal models
 case controlled study of HCW. 2) ACTG 076, perinatal HIV transmission. 3) Animal models.")
103
HIV Post Exposure Prophylaxis
AZT 300 mg BID 3TC 150 mg BID Kaletra II tabs BID should begin ASAP, within 48 hours of injury total course = 28 days side effects: nausea, vomiting, diarrhea, headache, fatigue, anemia, drug interactions

104
HIV Post Exposure Prophylaxis
Seen in clinic within 2 days Repeat HIV tests at 1, 3 and 6 months use condoms with all sex partners do not donate blood cost: $1200 for one month supply

105
Hepatitis B You should be vaccinated!
If not vaccinated and not immune, liver function tests HBIG and HepB vaccination HBsAg and HBsAb at 1, 3 and 6 months

106
Hepatitis C Takes up to three months to develop antibodies
HCV RNA detectable in blood within days

107
Hepatitis C Recent trial of 44 health care workers exposed to HCV via needle sticks received IFN daily for 1 month followed by IFN 3x per week for 5 months 95% response rate

108
Infection Control and HIV

109
Protecting Yourself

110
Protecting Yourself and Others
What body fluids contain HIV?

111
Protecting Yourself and Others
What body fluids contain HIV? Blood semen vaginal fluids

112
Protecting Yourself and Others
What body fluids do not contain HIV? Saliva Tears Sweat Urine Stool/diarrhea Vomit *unless contaminated with blood

113
Protecting Yourself and Others
Wear gloves for venipuncture Wear gloves for cleaning up any body fluids Carefully dispose of sharps!! Bedding, towels, etc stained with blood or vaginal fluids are laundered normally No gowns! No masks! (except for bloody procedures)
")
114
Protecting the Patient
Do Not isolate because of HIV!!! HIV+ individuals deserve your respect If you don’t know about HIV, learn something Maintain confidentiality!!

115
The new face of HIV

Similar presentations















 Fellow in Industrial Health ( Ahmadabad)>")





 is a disease of the human immune system caused by the Human Immunodeficiency.>")

- virus that primarily infects cells of the __________ _________________.>")


