Download presentation
Presentation is loading. Please wait.

1
Choanal Atresia Saad A. Alsaleh

2
Questions What is Choanal Atresia (CA)? Why does it happen?
Are there risk factors for developing CA? What is CHARGE syndrome? How do patients with CA present? How do you evaluate a patient with CA? What are the treatment options?

3
What is CA?

4
What is CA? Total obstruction of the posterior nasal choana (the opening between the nose and the nasopharynx). first described by Roederer In 1755. In 1854, Emmert reported the first successful surgical procedure for congenital choanal atresia in a 7-year-old boy using a curved trocar transnasally. 3- after that it had more attention and transnasal ans transplatal approaches were explored

5
What is CA? Incidence of 1 in 5000 – 8000 live births. F : M = 2 : 1
Unilateral : Bilateral = 2 : 1 ( Rt. Side ) J.S. Fraser in 1910 reported that it was 90% bony and 10% membranous atresia. Brown et al in 1996 reported that it was 29% pure bone, 71% mixed membranous and bone, NO pure membranous atresia present. 3- He had no access to modern workup of computer tomography 4- There is a recent study looking at the CT and histologic specimens in 63 patients and this
 J.S. Fraser in 1910 reported that it was 90% bony and 10% membranous atresia. Brown et al in 1996 reported that it was 29% pure bone, 71% mixed membranous and bone, NO pure membranous atresia present. 3- He had no access to modern workup of computer tomography. 4- There is a recent study looking at the CT and histologic specimens in 63 patients and this.")
6
Why does it happen?

7
Etiology Failure of the bucconasal membrane of Hochstetter to rupture ( the most widely accepted ). Misdirection of mesodermal flow due to local factors ( Hengerer, 1982) Medial outgrowth of vertical and horizontal processes of the palatine bone. 2- The nasal cavities extend posteriorly during development under the influence of the posteriorly directed fusion of the palatal processes. Thinning of the membrane occurs, which separates the nasal cavities from the oral cavity. By the 38th day of development, the 2-layer membrane consisting of nasal and oral epithelia ruptures and forms the choanae (posterior nares). Failure of this rupture results in choanal atresia . 5- The development begins with the migration of neural crest cells from their origin in the dorsal neural folds laterally around the eye and transversing the frontonasal process. It begins the 4th week and nasal architecture is completed by the 12th week. During this time the neural crest cells migrate beneath the epithelium through a meshwork of hyaluronic acid and attach to collagen filaments within the facial processes. These pleuropotential cells then undergo rapid proliferation and differentiation into a matrix of mesenchymal tissue which will be transformed into muscle, cartilage, and bone. Some of these changes may occur within minutes to hours and require unbelievable precision.
 Medial outgrowth of vertical and horizontal processes of the palatine bone. 2- The nasal cavities extend posteriorly during development under the influence of the posteriorly directed fusion of the palatal processes. Thinning of the membrane occurs, which separates the nasal cavities from the oral cavity. By the 38th day of development, the 2-layer membrane consisting of nasal and oral epithelia ruptures and forms the choanae (posterior nares). Failure of this rupture results in choanal atresia . 5- The development begins with the migration of neural crest cells from their origin in the dorsal neural folds laterally around the eye and transversing the frontonasal process. It begins the 4th week and nasal architecture is completed by the 12th week. During this time the neural crest cells migrate beneath the epithelium through a meshwork of hyaluronic acid and attach to collagen filaments within the facial processes. These pleuropotential cells then undergo rapid proliferation and differentiation into a matrix of mesenchymal tissue which will be transformed into muscle, cartilage, and bone. Some of these changes may occur within minutes to hours and require unbelievable precision.")
8
Are there risk factors for developing CA?

9
Choanal Atresia Associated With Prenatal Methimazole Exposure: Three New Patients P. Barbero, C. Ricagni, G. Mercado, R. Bronberg, and M. Torrado American Journal of Medical Genetics 129A:83–86 (2004)
.")
10
What is CHARGE syndrome?

11
What is CHARGE Syndrome?
Choanal atresia is associated with other congenital abnormalities 50% of the time. (bilateral > unilateral) Mutation in CHD7 gene in chromosome 8. In 1979, CHARGE syndrome or Hall-Hittner syndrome was originally delineated by Bryan Hall in 17 children with multiple congenital anomalies. In 1981, R Pagon coined the term ‘CHARGE’ , an acronym summarizing six cardinal clinical features. Sanlaville D and Verloes A. CHARGE syndrome: an update. European Journal of Human Genetics (2007) 15, 389–399.
 Mutation in CHD7 gene in chromosome 8. In 1979, CHARGE syndrome or Hall-Hittner syndrome was originally delineated by Bryan Hall in 17 children with multiple congenital anomalies. In 1981, R Pagon coined the term ‘CHARGE’ , an acronym summarizing six cardinal clinical features. Sanlaville D and Verloes A. CHARGE syndrome: an update. European Journal of Human Genetics (2007) 15, 389–399.")
12
What is CHARGE Syndrome?
Ocular Coloboma Heart defects Atresia of choanae Retardation of growth Genito-urinary anomalies Ear anomalies

13
What is CHARGE Syndrome?
Ocular Coloboma Chorioretineal coloboma, with (40%) or without microphthalmia, is present in 75–90%. Other anomalies include hypoplasia of optic nerve, anophthalmia, nystagmus, squint and refractive errors Heart defects Atresia of choanae Retardation of growth Genito-urinary anomalies Ear anomalies 1-1 also it happen in the iris
 or without microphthalmia, is present in 75–90%. Other anomalies include hypoplasia of optic nerve, anophthalmia, nystagmus, squint and refractive errors. Heart defects. Atresia of choanae. Retardation of growth. Genito-urinary anomalies. Ear anomalies. 1-1 also it happen in the iris.")
14
What is CHARGE Syndrome?
Ocular Coloboma Heart defects Congenital heart defects (CHD) are observed in 50–85% of cases. Fallot tetralogy (1/3 of cases), atrioventricular canal, VSD, ASD, aortic coarctation and PDA represent 75% of the defects. Atresia of choanae Retardation of growth Genito-urinary anomalies Ear anomalies
 are observed in 50–85% of cases. Fallot tetralogy (1/3 of cases), atrioventricular canal, VSD, ASD, aortic coarctation and PDA represent 75% of the defects. Atresia of choanae. Retardation of growth. Genito-urinary anomalies. Ear anomalies.")
15
What is CHARGE Syndrome?
Ocular Coloboma Heart defects Atresia of choanae Retardation of growth Most patients have low normal birth weight and length (around 10th centile). Postnatal growth retardation should be in relation to feeding difficulties and/or surgical problems. Growth tends to catch up after infancy. Due to hypothalamo-hypophyseal dysfunction. Genito-urinary anomalies Ear anomalies
. Postnatal growth retardation should be in relation to feeding difficulties and/or surgical problems. Growth tends to catch up after infancy. Due to hypothalamo-hypophyseal dysfunction. Genito-urinary anomalies. Ear anomalies.")
16
What is CHARGE Syndrome?
Ocular Coloboma Heart defects Atresia of choanae Retardation of growth Genito-urinary anomalies Genital anomalies observed in 50–70% of cases (males: 80– 90%, females: 15–25%). Hypoplastic external genitalia is the most common anomaly. Anomalies of the urinary tract in 10–40%, such as renal ectopia, horseshoe kidneys, ureteral anomalies. Ear anomalies 2- 80% of boys have micropenis and/or cryptorchidism, and 1/3 of the girls have hypoplastic labiae majorae
. Hypoplastic external genitalia is the most common anomaly. Anomalies of the urinary tract in 10–40%, such as renal ectopia, horseshoe kidneys, ureteral anomalies. Ear anomalies % of boys have micropenis and/or cryptorchidism, and 1/3 of the girls have hypoplastic labiae majorae.")
17
What is CHARGE Syndrome?
Ocular Coloboma Heart defects Atresia of choanae Retardation of growth Genito-urinary anomalies Ear anomalies In 95–100%, the pinnae are asymmetrically misshaped, low set, anteverted, cup-shaped, wide, but with reduced vertical height.

19
What is CHARGE Syndrome?
Ocular Coloboma Heart defects Atresia of choanae Retardation of growth Genito-urinary anomalies Ear anomalies Preauricular tags, hypoplastic auditory canal and microtia can be associated. ME: absence of the stapedius muscle, absence of the oval window, and hypoplastic incus and stapes, with ossicular chain fixation. 1- External ear. 2- Middle ear can also be affected:

20
What is CHARGE Syndrome?
Ocular Coloboma Heart defects Atresia of choanae Retardation of growth Genito-urinary anomalies Ear anomalies Inner ear anomalies prevelance could be > 90%. Malformation of the inner ear (CHARGE type of Mondini dysplasia). Complete absence of the pars superior (utricle and semicircular canals) with or without Mondini dysplasia of the pars inferior (cochlea and saccule). 3- although relatively nonspecific, and can be observed in many syndromal deafness but aplasia of the semicircular canals and hypoplastic uncus are probably the most specific anomaly of CHARGE syndrome. And mondini’s dysplasia is basically that instead of the normal 2 and half turns of the cochlea it has only one or one and a half turns.
. Complete absence of the pars superior (utricle and semicircular canals) with or without Mondini dysplasia of the pars inferior (cochlea and saccule). 3- although relatively nonspecific, and can be observed in many syndromal deafness but aplasia of the semicircular canals and hypoplastic uncus are probably the most specific anomaly of CHARGE syndrome. And mondini’s dysplasia is basically that instead of the normal 2 and half turns of the cochlea it has only one or one and a half turns.")
21
What is CHARGE Syndrome?
Ocular Coloboma Heart defects Atresia of choanae Retardation of growth Genito-urinary anomalies Ear anomalies Deafness affects 60–90% of cases. The commonest are severe conductive or mixed loss, and usually affects more the high frequencies than the low ones. Many other anomalies are assocaited with CHARGE like CNS, Immunity, limb anomalies and others.

22
CHARGE Syndrome Diagnostic Criteria

23
CHARGE Syndrome Diagnostic Criteria

24
What is CHARGE Syndrome?
Verloes major diagnostic criteria concentrated on the 3 C triad: Ocular Coloboma. Choanal atresia. Abnormal semicircular Canals. The presence of these three gives a diagnosis CHARGE or 2 with 2 minor criteria mentioned in the previous table

25
Other Syndromes?

26
Other Syndromes? Choanal and ileal atresia: a new syndrome or association? Adi Yoskovitch, et al. International Journal of Pediatric Otorhinolaryngology 49 (1999) 237–240
 237–240.")
27
How do patients with CA present?

28
Presentation ( Bilateral )
A newborn infant is an obligate nasal breather. Due to the posterior soft palate covering the oropharynx and the neonate's tongue in close proximity with the hard and soft palate. The hallmark is the cyclic cyanosis of the neonate. When the infant’s mouth and nasal passages are closed → cyanosis → He cries, air flow occurs through the mouth and the cyanosis disappears. 2- creating a vaccum causing oral airway obstruction and they start breathing from the mouth at about 4-6 weeks.

29
Presentation ( Unilateral )
Unilateral atresia is rarely a cause of neonate respiratory distress. Often not recognized at birth. The most common presentation is a 1 to 2 y/o child with unilateral copious mucoid rhinorrhea or sinusitis.

30
Are Infants Really Obligatory Nasal Breathers?
Paul S. Bergeson and J. Chris Shaw Clin Pediatr (Phila) 2001; 40; 567
 2001; 40; 567.")
31
Are Infants Really Obligatory Nasal Breathers?
Rodenstein et al and deAlmieda et al, indicate that most children can initiate oral breathing after nasal occlusion. Other studies suggest there is a subset of infants who cannot begin mouth breathing after blocking their noses . Studies claim anywhere between 0% and 50% of very young infants are not able to breathe through their mouths except when crying.

32
Examination

33
Examination ABCs V/S and signs of respiratory distress, dysmorphia.
Complete head & neck examination. The diagnosis of atresia can be made by: failing to pass no. 8 french catheter at least 32mm pass the anterior nares into the oropharynx. The lack of movement of a thin wisp of cotton. Administering methylene blue and assessing passage into nasopharynx. Flexible fiberoptic endoscopy to assess the deformity. 4-2 under the nares while the mouth is closed

35
Differential Diagnosis

36
Differential Diagnosis
Congenital stenosis of the pyriform aperture. Dacryocystoceles (nasolacrimal duct cysts). Encephaloceles. Gliomas. Dermoid cysts. Teratomas. 1- due to bony overgrowth of the nasal lateral process of the maxilla
. Encephaloceles. Gliomas. Dermoid cysts. Teratomas. 1- due to bony overgrowth of the nasal lateral process of the maxilla.")
37
How do you evaluate a patient with CA?

38
Evaluation Genetics evaluation Cardiology (EKG, Echo)
Ophthalmology evaluation Hearing assessment U/S kidneys

39
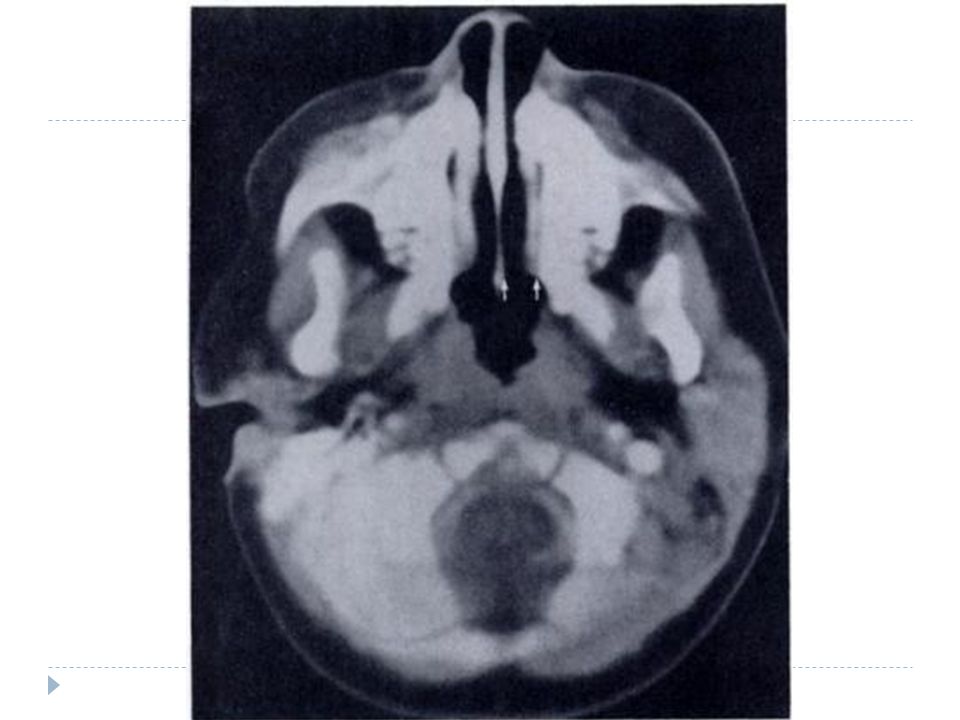
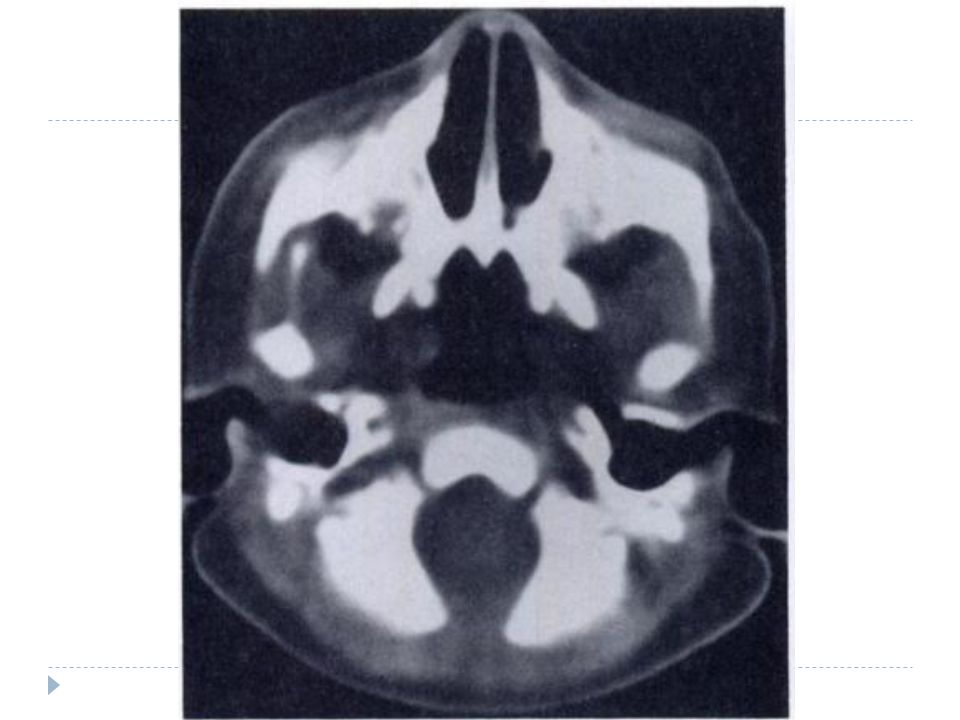
Imaging CT scan: The method of choice in evaluating CA.
Confirm the diagnosis of choanal atresia (unilateral or bilateral). Evaluate choanal atresia (vomer bone width and choanal airspace distance). Determine the degree of bony, membranous, or mixed atresia. Exclude other possible nasal causes of obstruction & Delineates abnormalities in the nasal cavity and nasopharynx for pre-op planning.
. Evaluate choanal atresia (vomer bone width and choanal airspace distance). Determine the degree of bony, membranous, or mixed atresia. Exclude other possible nasal causes of obstruction & Delineates abnormalities in the nasal cavity and nasopharynx for pre-op planning.")
40
Imaging CT scan: In bony CA: Medial bowing and thickening of the lateral wall of the nasal cavity, composed of the perpendicular plate of the palatine bone and the pterygoid process; enlargement of the vomer and fusion of these bony elements. In membranous CA: the air passage between the lateral wall of the nasal cavity and the vomer is small when compared with the control group. *Slovis TL et al. Choanal Atresia: Precise CT Evaluation. Radiology. 1985;155:

44
What are the treatment options?

45
Management Once the diagnosis is made → secure the child's airway and prevent asphyxiation. Oropharyngeal airway or a McGovern nipple (temporary solution). Surgical repair is the definitive treatment
. Surgical repair is the definitive treatment.")
46
Management Bilateral atresia is emergent and usually is repaired within the first week to month of life. Unilateral atresia can be repaired at a later date when the child's anatomy is larger and the procedure will be technically less difficult. The method of repair is controversial, with no technique having gained universal acceptance. And it depends on the thickness of the atretic plate and the presence of anomalies, so…. The more extensive is the surgery and the need for stenting is more.

47
Management Main approaches are:
Transpalatal Transnasal Transseptal External Rhinoplasty approach Laser repair With the advent of miniaturized endoscopic equipment and powered instrumentation, the most popular and successful method over the past decade has been the transnasal technique* *Schoem S. Transnasal endoscopic repair of choanal atresia: Why stent? Otolaryngology– Head and Neck Surgery 2004;131,4:

48
Management ( Transpalatal )
The approach is through the palate directly to the atretic plate. Pros: provides excellent exposure. high success rate. Cons: requires more operative time. increased blood loss. longer recovery time. possible occurrence of palatal fistula, palatal dysfunction, and maxillofacial growth disturbance.

49
Management ( Transpalatal )
")
50
Management ( Transnasal )
The evolution of optical telescopes, miniaturization of conventional instruments, and development of powered microdebriders with drill attachments have revolutionized the transnasal approach.

51
Management ( Transnasal )
Pros: Clear vision of the operative field. Accurate removal of the atresia plate and posterior vomerine bone, thus reducing the rate of restenosis significantly. It is a short and safe procedure. Swift recovery and short hospitalization. Does not impair development of dental arches. Cons: The potential for rapidly aspirating orbital and cerebral contents when laminae are violated.

52
Stenting??

53
Transnasal endoscopic repair of choanal atresia: Why stent. Schoem S
Transnasal endoscopic repair of choanal atresia: Why stent? Schoem S. Otolaryngology– Head and Neck Surgery 2004;131,4: Debate still surrounds postoperative stenting. 13 children ages 2 days to 13 years old (mean 45 months) who presented with unilateral or bilateral CA underwent transnasal endoscopic surgery with NO stents used. 4 who had unilateral CA, underwent office serial examinations alone after surgery and all remained patent (<50% restenosis).
 who presented with unilateral or bilateral CA underwent transnasal endoscopic surgery with NO stents used. 4 who had unilateral CA, underwent office serial examinations alone after surgery and all remained patent (<50% restenosis).")
54
Transnasal endoscopic repair of choanal atresia: Why stent. Schoem S
Transnasal endoscopic repair of choanal atresia: Why stent? Schoem S. Otolaryngology– Head and Neck Surgery 2004;131,4: 9 pts underwent reexamination under GA 3 to 4 weeks after initial surgery followed by serial office nasal endoscopy at 1-,3-, 6-, and 12-month intervals. 7 out of the 9 pts (78%) had varying amounts of emerging granulation tissue or minor synechiae that resolved with microdebrider reexcision. All serial office endoscopies demonstrated no restenoses, No office dilations were performed, and there were no long-term complications.
 had varying amounts of emerging granulation tissue or minor synechiae that resolved with microdebrider reexcision. All serial office endoscopies demonstrated no restenoses, No office dilations were performed, and there were no long-term complications.")
55
Topical Mitomycin?

56
Topical mitomycin as an adjunct to choanal atresia repair. Prasad M et
Topical mitomycin as an adjunct to choanal atresia repair. Prasad M et.al. Arch Otolaryngol Head Neck Surg Apr;128(4): 20 pts. with either unilateral or bilateral congenital choanal atresia underwent repair using the transnasal endoscopic approach, the transpalatal approach, or both with 1 or 2 applications of mitomycin (0.5 mg/ml) for 3 minutes. 17 retained patent airways. 3 pts. experienced improvement from a total atresia to a narrowed, stenotic choana.
: pts. with either unilateral or bilateral congenital choanal atresia underwent repair using the transnasal endoscopic approach, the transpalatal approach, or both with 1 or 2 applications of mitomycin (0.5 mg/ml) for 3 minutes. 17 retained patent airways. 3 pts. experienced improvement from a total atresia to a narrowed, stenotic choana.")
57
Effect of use of mitomycin C on the outcome of Choanal atresia repair Al-Ammar AY Saudi Med J Oct;28(10): Endoscopic repair of CA was performed in 20 cases. Intra-operative application of topical MMC (0.4 mg/mL for 4 minutes) was carried out in 13 children, and 7 children did not receive MMC. The follow-up period ranged between 9 months and 6 years.
 was carried out in 13 children, and 7 children did not receive MMC. The follow-up period ranged between 9 months and 6 years.")
58
69 % of the cases receiving MMC had a successful outcome compared with 57% of non-MMC cases, The difference was not statistically significant (p=0.230). In unilateral CA, 70% of those who received MMC had a successful outcome compared with 60% of those who did not; again the difference was not statistically significant (p=0.566)
")
59
Postoperative Care

60
Postoperative Care Stent irrigation and routine suctioning.
The patients are maintained on oral antibiotics (amoxicillin or a cephalosporin) while stented. The stents are left in place from 2 days – 6 weeks (Debate??) At the time of stent removal, examination under GA or fiberoptic nasopharyngoscope is performed to assess mucosalization and diameter.
 while stented. The stents are left in place from 2 days – 6 weeks (Debate ) At the time of stent removal, examination under GA or fiberoptic nasopharyngoscope is performed to assess mucosalization and diameter.")
61
Postoperative Care If granulation tissue is found, it is debrided, cultured and abx are continued. Systemic or local steroids are often used. Repeat dilatation with a urethral sound and revision surgery is required for restenosis.

62
Predictive factors of restenosis are:
Predictive Factors for Success After Transnasal Endoscopic Treatment of Choanal Atresia Teissier N, et al. Arch Otolaryngol Head Neck Surg Jan;134(1):57-61 To analyze the different factors affecting the outcome of transnasal endoscopic repair of choanal atresia (CA) in children with a follow-up of 43 months. Predictive factors of restenosis are: The presence of GERD Age younger than 10 days at the time of surgery Insufficient postoperative endoscopic revision previous surgery and associated malformations are not predictive of a poor surgical outcome.
: To analyze the different factors affecting the outcome of transnasal endoscopic repair of choanal atresia (CA) in children with a follow-up of 43 months. Predictive factors of restenosis are: The presence of GERD. Age younger than 10 days at the time of surgery. Insufficient postoperative endoscopic revision. previous surgery and associated malformations are not predictive of a poor surgical outcome.")
63
Questions What is Choanal Atresia (CA)? Why does it happen?
Are there risk factors for developing CA? What is CHARGE syndrome? How do patients with CA present? How do you evaluate a patient with CA? What are the treatment options?

64
Thank You

Similar presentations