Download presentation
Presentation is loading. Please wait.

2
How Good is Your Stroke Scale?
Sean Kivlehan, MD, MPH, NREMT-P September 2013

4
Outline Stroke Review Treatment review Scale development and flaws
Rehab tPA recognition & time matters Scale development and flaws Systems issues Future directions

5
Case #1 62 year old male, low speed MVC into pole, conscious with flaccid left arm, facial droop, and slurred speech. BP 220/100

6
Case #2 89 year old female, daughter called because she has been vomiting for past 2 hours, is dizzy, and can’t stand. No facial droop, normal speech, no focal weakness. BP 220/100. Actively vomiting.

7
Case #3 70 year old female found down in her apartment when son went to check on her. Last seen normal at dinner last night. Now semi-conscious but following commands, not moving right side. BP 200/90.

8
We’ve come far but still have a long way…
HISTORY

9
“Apoplexy” What they called it from Hippocrates on… 1950’s: TIA’s
25 years ago: Imaging 10 years ago: Imaging in community hospitals 1970 WHO definition: “rapidly developing clinical signs of focal (or global) disturbance of cerebral function, lasting more than 24 hours or leading to death, with no apparent cause other than that of vascular origin.” Sacco 2013
 disturbance of cerebral function, lasting more than 24 hours or leading to death, with no apparent cause other than that of vascular origin. Sacco")
10
TIA’s 1975: “episodes of temporary and focal dysfunction of vascular origin, which are variable in duration, commonly lasting from 2 to 15 minutes, but occasionally lasting as long as a day (24 hours). They leave no persistent neurological deficit.” 2002: “A TIA is a brief episode of neurologic dysfunction caused by focal brain or retinal ischemia, with clinical symptoms typically lasting less than one hour, and without evidence of acute infarction.”
. They leave no persistent neurological deficit. 2002: A TIA is a brief episode of neurologic dysfunction caused by focal brain or retinal ischemia, with clinical symptoms typically lasting less than one hour, and without evidence of acute infarction.")
11
Unclear 2009: “a transient episode of neurological dysfunction caused by focal brain, spinal cord, or retinal ischemia without acute infarction.”

12
What is a Stroke Today? Ischemic Stroke
(clot: thombotic vs embolic) – 87% 2. Hemorrhagic Stroke (bleed: intracerebral vs subarachnoid; aneurysms & AVM’s) – 13% 3. Transient Ischemic Attack (TIA) Caused by clot, last <5 min, no permanent injury
 – 87% 2. Hemorrhagic Stroke. (bleed: intracerebral vs subarachnoid; aneurysms & AVM’s) – 13% 3. Transient Ischemic Attack (TIA) Caused by clot, last <5 min, no permanent injury.")
13
A long way to go Number 4 cause of death in US (down from #3 in 2008)
785,000 in US a year Less than half of 911 calls made within 1 hour of onset Newest AHA/ASA outreach: FAST 1 of 3 in 88% of strokes Recalled well in 3 months (public) Only 53% of strokes arrive by EMS in US
 Only 53% of strokes arrive by EMS in US.")
14
Jauch 2013

15
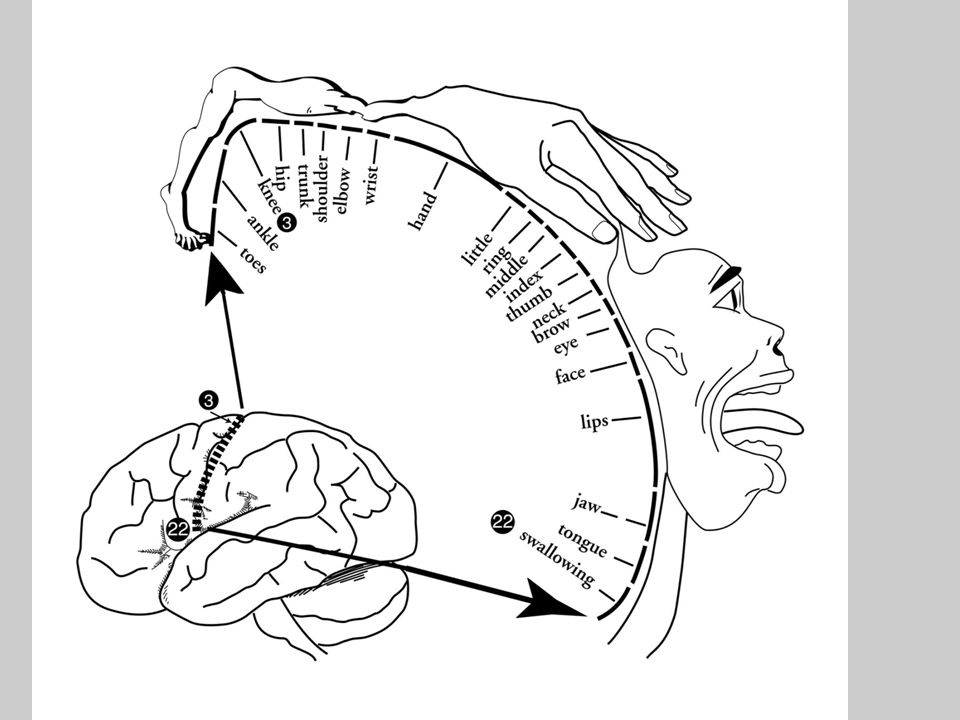
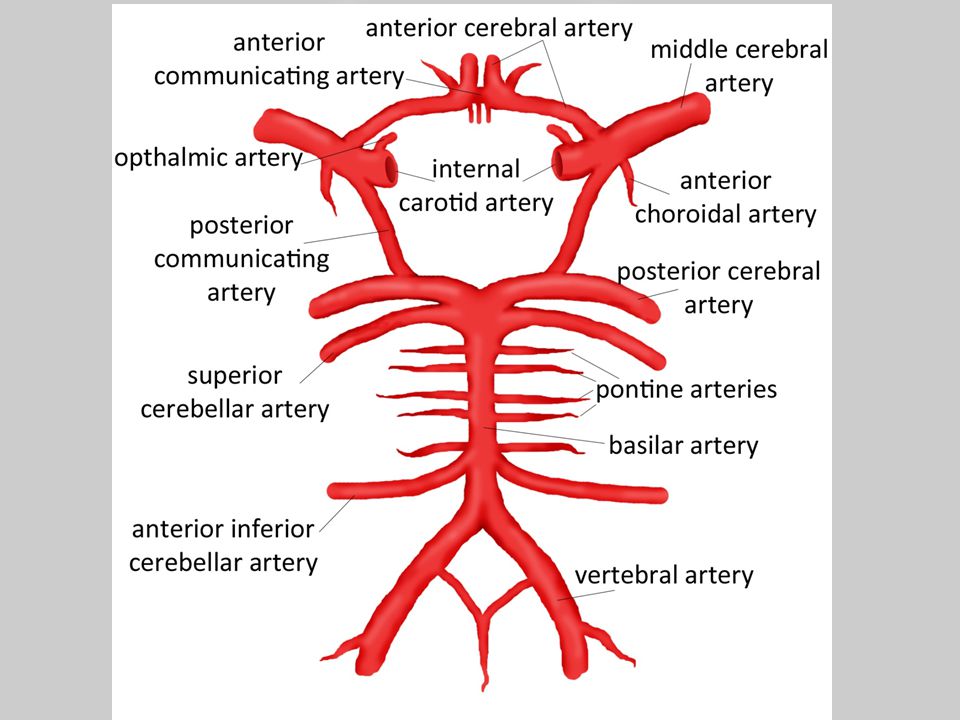
Vessels & Risk ANATOMY OF A STROKE

21
Where is the Stroke? Anterior Circulation Posterior Circulation
Weakness Aphasia Sensory deficit Posterior Circulation Dizzy Vomiting Ataxia

22
Now that we have the vessels down, how do they get messed up?

23
Source: Arizona.edu

24
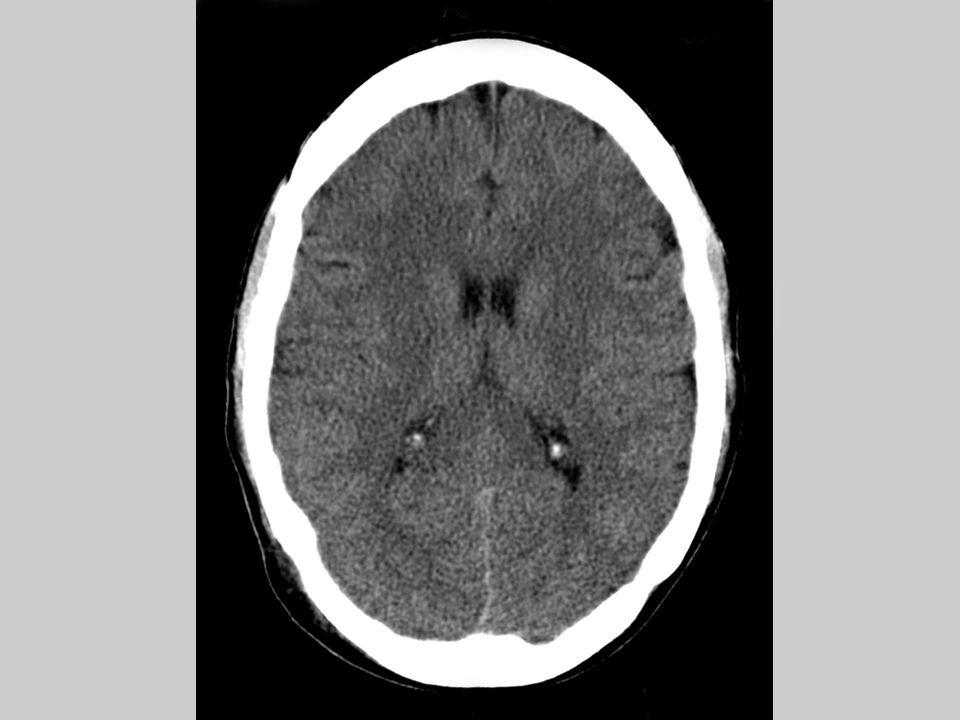
Ischemic

25
Hemorrhagic 40% 30 days! Sacco 2013

29
What Causes These Things?
Embolic Bacterial emboli from valvular vegetations Blood clots from cardiac dysrhythmias Platelet-fibrin complex from atherosclerotic plaque disruption Septic emboli from infection Fat emboli from traumatic injury Particulate emboli from IV drug injection Thrombotic Secondary to intrinsic vascular disease in the occluded vessel Atherosclerotic disease most common cause in U.S. Other causes include Vasculitis Hypercoagulable states Polycythemia Vascular dissection

30
Risk CAD: Double HTN: Triple Cardiac Failure: Quadruple
A-Fib: Quintuple Wolf, Stroke, 1991

32
And what about those TIA’s?
4 to 20% will progress to stroke within 90 days Half of those in first 24 hours ABCD2 score Age (>60) Blood Pressure (>140/90) Clinical Features (weakness/speech) Duration (>60 minutes) Diabetes Koenig, NEJM, 2007
 Blood Pressure (>140/90) Clinical Features (weakness/speech) Duration (>60 minutes) Diabetes. Koenig, NEJM,")
33
From Rehab to Cure TREATMENT

34
Treatment Old teaching – 5 pages out of 1100 Focused on recognition, managing airway, manage herniation symptoms

35
Suddenly, a cure!

36
What we KNOW Earlier recognition Earlier EMS
Earlier EMS Earlier ED notification Earlier ED notification Earlier imaging Earlier imaging Earlier tPa Earlier tPa Better outcomes

37
AHA Implementation Strategy for EMS within Stoke Systems of Care (1997)
")
38
Key Things Check a sugar And the pupils! Prior stroke/seizures?
Time of onset! Wake up strokes Stroke mimickers

40
EMS Interventions ABC’s etc Oxygen to maintain SpO2 >94%
Head of bed flat for SBP <120 and give isotonic saline Antihypertensive treatment controversial (>220) Glucose if FS <60 Establish PIV Labs if build into system None of this should delay transport Jauch 2013
 Glucose if FS <60. Establish PIV. Labs if build into system. None of this should delay transport. Jauch")
41
The most important piece of info….
Time patient last seen normal EMS often the only people that can get this info on scene (family, bystanders) Also: Signs of hx of seizures or trauma on scene PMHx (prior stroke, diabetes, HTN, AF Meds on scene (anticoagulants) Recent illness, surgery, trauma Collect phone numbers, code status, family members Bring family to ED EMS are the eyes & ears of the ED
 Also: Signs of hx of seizures or trauma on scene. PMHx (prior stroke, diabetes, HTN, AF. Meds on scene (anticoagulants) Recent illness, surgery, trauma. Collect phone numbers, code status, family members. Bring family to ED. EMS are the eyes & ears of the ED.")
42
tPA (Fibrinolytic Therapy)
FDA approved in 1996 for 3 hour window Showed symptom improvement at 24 hours and 1 year (OR 1.9; CI ) ICH: 6.4% in tPA and 0.6% in placebo 3 to 4.5 hour window w/ extra exclusions 4.5 to 6 hour window did not help NINDS, NEJM, 1995
 ICH: 6.4% in tPA and 0.6% in placebo. 3 to 4.5 hour window w/ extra exclusions. 4.5 to 6 hour window did not help. NINDS, NEJM,")
43
Jauch 2013

44
Mechanical Retrieval & IA tPA
Merci Penumbra Solitaire Trevo IA tPA ok for up to 6 hours Good for patients with IV tPA contraindications Can give in addition to IV tPA

53
So Now, TIME MATTERS

55
And we need to Recognize
Can we? 1995: Reading EMS (Ohio) 58 months, 4,413 patients 96 (2%) dx with stroke or TIA by EMS 10 excluded (lost data) 86 62 (72%) dx with stroke or TIA in ED So, 24 patients (28%) were misdiagnosed by EMS (false positive) Dispatch: 30 of 62 dispatched as something other than stroke BUT WE DON’T KNOW: how many people were having strokes & EMS called it something else? Kothari, 1995
 58 months, 4,413 patients 96 (2%) dx with stroke or TIA by EMS 10 excluded (lost data) 86 62 (72%) dx with stroke or TIA in ED So, 24 patients (28%) were misdiagnosed by EMS (false positive) Dispatch: 30 of 62 dispatched as something other than stroke BUT WE DON’T KNOW: how many people were having strokes & EMS called it something else Kothari,")
56
Maybe it’s because of the education?

57
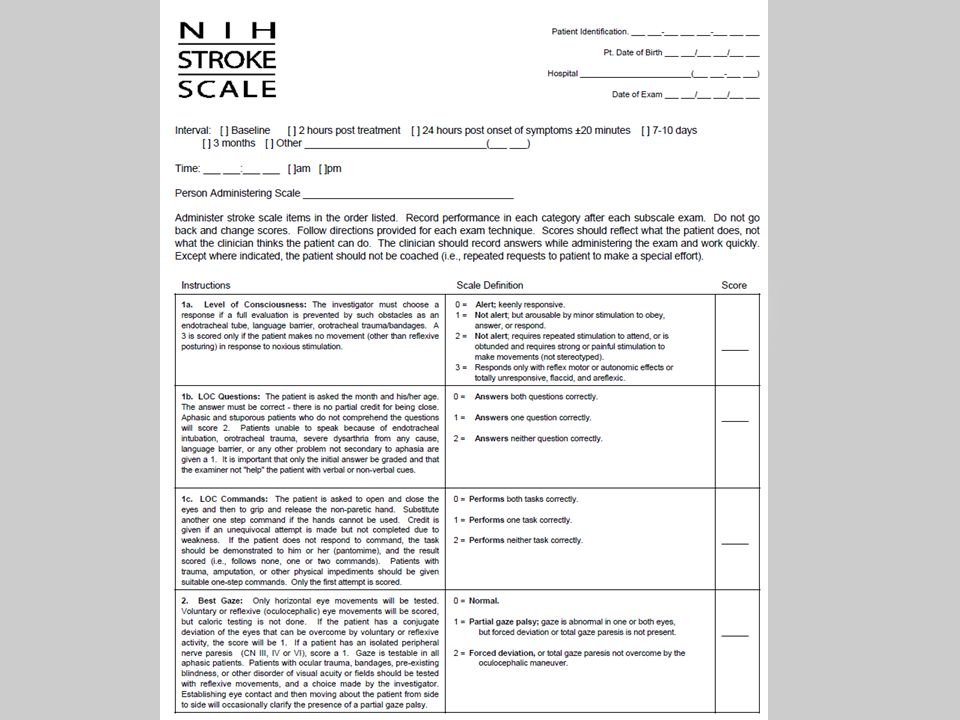
The NIH Stroke Scale WHO IS HAVING A STROKE?

63
What they did in Cincinatti
NIH stroke scale – huge & takes a while Watered it down to what matters: Facial palsy Asymmetric arm weakness Speech abnormalities

64
100% Sensitivity 88% Specificity Kothari, 1997
They took 299 patients (74 known stroke from previous study compared to 225 randoms in ED Kothari, 1997

65
What does that mean? Sensitivity: True Positive
(you found all strokes) Specificity: True Negative (you found all non strokes) So this test (in theory): Catches every stroke 1 in 9 aren’t really having a stroke (false positive)
 Specificity: True Negative. (you found all non strokes) So this test (in theory): Catches every stroke. 1 in 9 aren’t really having a stroke (false positive)")
66
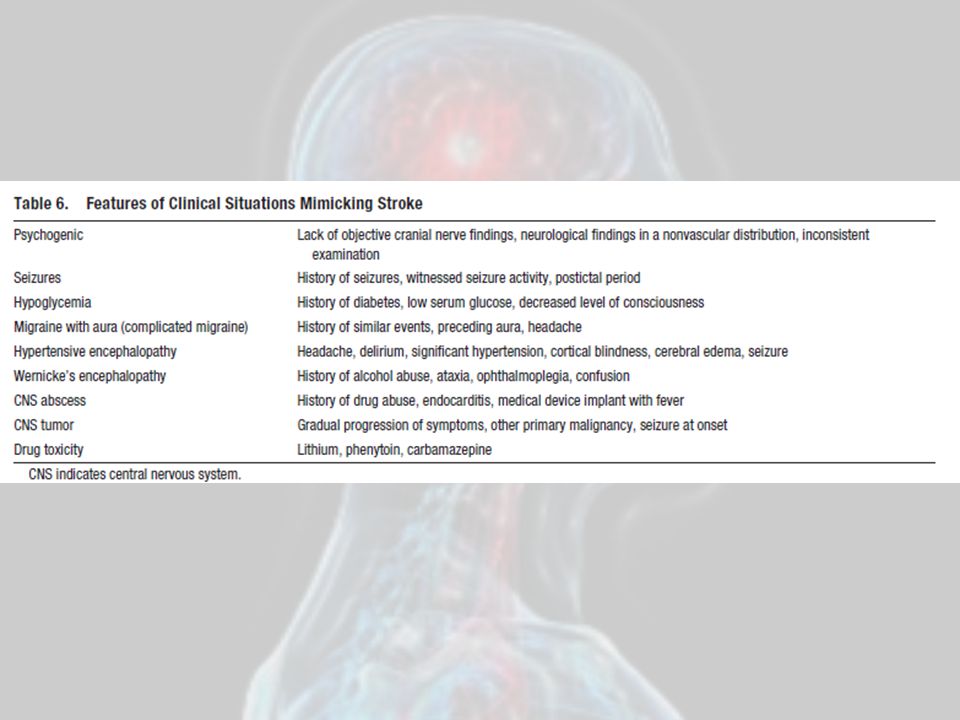
Who was falsely labeled? (also, our differential)
Seizure (3) Alcohol Intox (3) Cardiac Arrest (2) Abdominal Pain (2) Dizziness/Vertigo (2) Sepsis/Pneumonia (2)
 Alcohol Intox (3) Cardiac Arrest (2) Abdominal Pain (2) Dizziness/Vertigo (2) Sepsis/Pneumonia (2)")
67
Limitations Done by ED Physicians (not EMS)
Stroke patients were sick – enrolled in stroke trial Done in hospital (not in field) Misses posterior circulation strokes
 Misses posterior circulation strokes.")
68
Next: Test on EMS 24 EMS Providers (17 medics, 7 EMTs)
4 EMS providers & 1 ED physician did CPSS on each patient 860 scales on 171 patients (38 with stroke, 11 with TIA) Scoring for each component same between ED physician, Medic, EMT CPSS had sensitivity 59% and specificity 89% Missed: 10 posterior circ & 3 anterior circ (atypical) Kothari 1999
 Scoring for each component same between ED physician, Medic, EMT. CPSS had sensitivity 59% and specificity 89% Missed: 10 posterior circ & 3 anterior circ (atypical) Kothari")
69
Paramedics vs Physicians
Nor 2004

70
Kothari 1999

71
What about this posterior circ thing?
10/14 were missed! Testing ataxia would have caught 6/10 Downplayed: ataxia difficult to reproduce, least reproducible item on NIHSS, rarely treated w/ tPa Kothari 1999

72
What happened? 1997: all stroke dx patients were in a thrombolytic trial, so they had more severe symptoms and all received tPa 1999: neurologists were asked to find stroke mimickers, and stroke patients were just “discharge dx” of stroke, didn’t necessarily get tPa 1997 1999 Sensitivity 100% 59% Specificity 88% 89%

73
Did it get better? San Diego, 2005, 12 month period, 86,989 calls
Matched CAD (stroke), EMS report w/ CPSS done & stroke dx, & hospital ICD-9’s by billing info Dispatch as stroke: 2,140 (2%) 882 to study hospital 367 (42%) hospital stroke dx EMS dx as stroke: 995 (1.3%) 493 to study hospital 193 (40%) hospital stroke dx Missed: Dispatch: 73, EMS: 247 Ramanujam 2008
, EMS report w/ CPSS done & stroke dx, & hospital ICD-9’s by billing info. Dispatch as stroke: 2,140 (2%) 882 to study hospital 367 (42%) hospital stroke dx. EMS dx as stroke: 995 (1.3%) 493 to study hospital 193 (40%) hospital stroke dx. Missed: Dispatch: 73, EMS: 247. Ramanujam")
74
Verdict? EMS Sensitivity 44%, PPV 40%
Flaws: didn’t follow all patients in SD, so don’t really know true neg. Possible data is missing, or labeled “AMS etc” Others? Bray – 78% sensitivity No scale (Smith) – 61% sensitive, PPV 77%
 – 61% sensitive, PPV 77%")
75
Nail in the coffin? Durham, 2004 They use CPSS
All transports are discretely coded (so no missed EMS dx’s) Hospital (Duke) has stroke registry, compared this to EMS transports’ dx’s Frendl 2009
 Hospital (Duke) has stroke registry, compared this to EMS transports’ dx’s. Frendl")
76
Durham 184 EMS stroke/TIA charts 30 excluded (uncon), leaving 154
CPSS only used on 37% of stroke patients! 70% of patients w/ actual stroke had at least 1 CPSS finding (Sensitivity) 52% of patients w/ CPSS finding had a stroke (Specificity) No effect of scene time or L&S use to ED Frendl 2009
 52% of patients w/ CPSS finding had a stroke (Specificity) No effect of scene time or L&S use to ED. Frendl")
77
What are you goals? IF: identify greatest # of stroke patients, then add more elements (11% of missed strokes had grip strength/visual deficit/numbness or tingling) BUT: if you are going to active stroke teams off of this, this will put false positives through the roof IF: justify transport diversion, then the specificity NEEDS to increase. Is it better to bypass a patient’s primary hospital when we are only right half of the time? PRO CON No missed strokes Loss of Continuity Best care for stroke patients Increased cost (system & patient) EMS unit OOS time Accident Risk
 BUT: if you are going to active stroke teams off of this, this will put false positives through the roof. IF: justify transport diversion, then the specificity NEEDS to increase. Is it better to bypass a patient’s primary hospital when we are only right half of the time PRO. CON. No missed strokes. Loss of Continuity. Best care for stroke patients. Increased cost (system & patient) EMS unit OOS time. Accident Risk.")
78
Another option? Yes – the competitor! LAPSS Starts with exclusions:
>12 hour onset Age <45 yo Hx seizures Wheelchair/bedbound Finger stick <50 or >400 Then does: Arm weakness Grip Testing Facial droop Kidwell 1998

79
LAPSS Plans to miss: This is in the name of increasing specificity
Isolated visual field cuts Isolated aphasias Brainstem & Cerebellar infarcts This is in the name of increasing specificity Focuses on motor deficits Tested by ED physicians retrospectively on known stroke patients in thrombolytic trial (similar to CPSS), 93% sensitive Held up in testing – 89% sensitive & 99% specific Kidwell 2000 Kidwell 1998
, 93% sensitive. Held up in testing – 89% sensitive & 99% specific. Kidwell Kidwell")
80
The Australians Studied CPSS vs LAPSS
…and threw in their own, the MASS (Melbourne Ambulance Stroke Screen) Supposed to be a combo of the 2 Showed better sens/spec but the approach was flawed – didn’t track stroke discharge from hospital (so we have no idea how many were missed) “Faster Access to Stroke Therapies (FAST)” study Bray 2005
 Supposed to be a combo of the 2. Showed better sens/spec but the approach was flawed – didn’t track stroke discharge from hospital (so we have no idea how many were missed) Faster Access to Stroke Therapies (FAST) study. Bray")
81
MASS? Facial Droop Unilateral hand grip/weakness Unilateral arm drift
Slurred/abnormal speech ADDS: rule out mimics <45 yo Hx seizures/epilepsy Abnormal BSL Bray 2005

82
Bray 2010

83
Bray 2005

84
The British don’t want to be left out
Face Arm Speech Test (FAST) Same as CPSS but you don’t need the patient to repeat the sentence Validated in Newcastle, UK EMS caught 144/183 (79%) of strokes Still high levels of missed posterior strokes Can’t measure the false negatives (a theme) Harbison 2003
 Same as CPSS but you don’t need the patient to repeat the sentence. Validated in Newcastle, UK. EMS caught 144/183 (79%) of strokes. Still high levels of missed posterior strokes. Can’t measure the false negatives (a theme) Harbison")
85
Scale Summary CPSS: based off of NIHSS, misses post circ
LAPSS: Longer, but rules out non-tpa candidates and increases specificity FAST: Even quicker than CPSS, basically the same thing, from the UK MASS: Combo of the CPSS & LAPSS, building on strengths, from Australia

86
Wait – There’s More! Miami Emergency Neurological Deficit (MEND)
Precursor to new Advanced Stroke Life Support (ASLS) course CPSS + 6 more NIHSS components level of consciousness, orientation, commands, visual fields, gaze, leg motor, limb ataxia, sensation Brotons 2012
 course. CPSS + 6 more NIHSS components. level of consciousness, orientation, commands, visual fields, gaze, leg motor, limb ataxia, sensation. Brotons")
87
Ontario CPSS w/ more exclusions Chenkin 2009

88
Case #1 62 year old male, low speed MVC into pole, conscious with flaccid left arm, facial droop, and slurred speech. BP 220/100 Right MCA (anterior circulation), positive on all scales
, positive on all scales")
89
Case #2 89 year old female, daughter called because she has been vomiting for past 2 hours, is dizzy, and can’t stand. No facial droop, normal speech, no focal weakness. BP 220/100. Actively vomiting. Posterior circulation stroke. Abbreviated scales negative, NIHSS positive.

90
Case #3 70 year old female found down in her apartment when son went to check on her. Last seen normal at dinner last night. Now semi-conscious but following commands, not moving right side. BP 200/90. Left MCA, large stroke, positive on CPSS but out of window.

91
Now, transport Where, how ALS v BLS Air? Stoke centers Retriage

92
Field tPA, telemedicine, & ultrasound
FUTURE

93
PHANTOM-S Pre-Hospital Acute Neurologic Therapy and Optimization of Medical Care in Stroke
The ambulance: Neurologist Paramedic Radiographer CT Scanner POC Lab Teleradiology The dispatch: For any suspected stroke Weber 2013

95
The Results 23 patients got tPA in 3 months
Door-to-needle 62 minutes (vs 98 minutes) 2 patients bled, 1 died Weber 2013
 2 patients bled, 1 died. Weber")
96
Source: Mayfield Clinic.com & Radiographics

98
Does EMS notification reduce door to needle?
Yes! And door to imaging And pretty much every other metric Bae 2010, Mosley 2007

99
Summary Stoke management AHA Scales Transport

100
Why does this matter? EMS are the first medical contact for 38-70% of stroke patients EMS recognition is key to hospital notification Notification shortens door-to-needle time That improves outcomes for stroke patients BUT, we are missing a LOT of stroke patients (up to 40%) They go to non-stroke center or wait in triage Bray 2005
 They go to non-stroke center or wait in triage. Bray")
Similar presentations






































?>")


 Stroke - Overview Third leading cause of death in industrialized countries. Total cost of strokes in the U.S. is roughly.>")
