Download presentation
Presentation is loading. Please wait.

1
Reimbursement The Impact of Health Care Reform and Federal Issues
October 20, 2013 Maryland Association of Nurse Anesthetists Reimbursement The Impact of Health Care Reform and Federal Issues Christine S. Zambricki DNAP, CRNA, FAAN

2
Our Agenda Context Economic, health policy and political contexts
Federal health programs CRNA Issues Legislative and regulatory issues Affordable Care Act Advocacy programs

3
Federal policy environment
Economic Health Political

4
Economic Factors Shaping Health
Going Up Going Down Elderly as a share of the population Workers to retiree ratio Per-capita health spending, more slowly U.S. health compared with industrialized world U.S. debt, >$16.7 T U.S. deficits annually Economic growth Public coverage Private coverage

7
Is It About the Money?

8
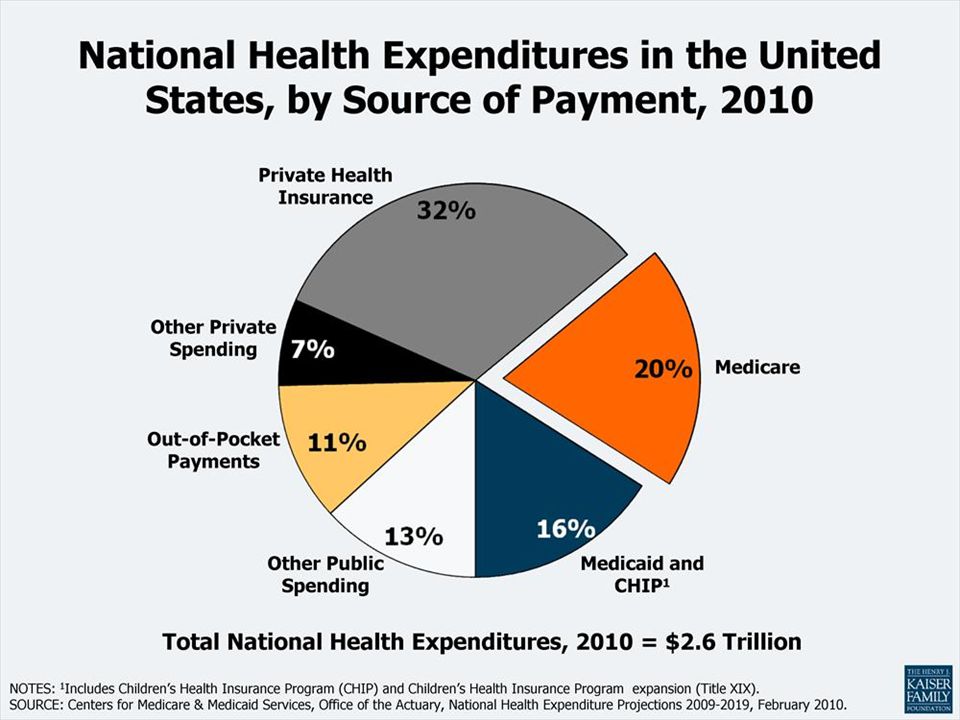
Health spending in the U.S. www.cms.gov
$2.7 T in 2011, up 3.9% in 2011, about 18% of U.S. economy, average $8,680 per person Three years in a row of stable growth Economic downturn Demand Supply Technology

9
Political Forces shaping the 113th Congress
58.7% of vote eligible citizens, 10% latino, 13% black, 19% young voters 65.9M to 60.9M votes, 51-47%, Continuing divided government House Senate 114th Congress? Latino expected to increase by 40% by 2030, black voter turnout higher than white for the first time and young voters to age 29 increased from 18%

10
Political Forces shaping the 113th Congress
Considerable change beneath the surface 12 new Senators of 100, 67 new Representatives of Most of Congress is new since 2006 New leaders in some key health positions Freshman class

12
IOM: The Future of Nursing
The Need to Transform Practice Key Message #1: Nurses should practice to the full extent of their education and training. The Need to Transform Education Key Message #2: Nurses should achieve higher levels of education and training through improved education system that promotes seamless academic progression.

13
IOM: The Future of Nursing
The Need to Transform Leadership Key Message #3: Nurses should be full partners, with physicians and other health professionals, in redesigning health care The Need for Better Data on the Health Care Workforce Key Message #4: Effective workforce planning and policy making require better data collection and an improved information infrastructure

14
Health Programs and CRNA Practice

15
Medicare & CRNAs Part A: Hospital insurance Part B: Physician services
Conditions of participation Physician supervision Pass-through program Part B: Physician services Anesthesia payment Medical Direction Medical Supervision Teaching rules Reimbursement for other services Parts C & D: Managed care, prescription drugs

16
Part A for CRNAs Conditions of participation & of coverage
Anesthesia services ASC surgical services Reasonable cost pass-through Certain qualifying rural and critical access hospitals <800 cases or less CRNA services as a hospital service, no Part B

17
New England Assy of Nurse Anesthetists: Federal Issues & Advocacy
Supervision It is a Medicare requirement, a portion of a regulation, 42 CFR §482.52(a)(4) Anesthesia must be administered only by … (4) A certified registered nurse anesthetist (CRNA), as defined in (b) of this chapter, who, unless exempted in accordance with paragraph (c)of this section, is under the supervision of the operating practitioner or of an anesthesiologist who is immediately available if needed ….
(4) Anesthesia must be administered only by … (4) A certified registered nurse anesthetist (CRNA), as defined in (b) of this chapter, who, unless exempted in accordance with paragraph (c)of this section, is under the supervision of the operating practitioner or of an anesthesiologist who is immediately available if needed ….")
18
Historical Context Part of the Medicare conditions for participation
1997: Proposed to be repealed 1/2001: Repealed in a final rule 2/2001: Suspended 11/2001: Finalized as an opt-out process 11/2001 to today: 17 states have opted out 2013: No rule regarding supervision but good CMS precedents

20
Part B for CRNAs Anesthesia payment Payment for other services
Medical direction Pain care Teaching rules Payment for other services

21
Fee-for-service (Base + time) x ($CF) = anesthesia fee
(Relative value) x ($CF) = physician fee Pays for a thing Does not necessarily pay for Quality The right thing Care coordination Optimal efficiency
 x ($CF) = physician fee. Pays for a thing. Does not necessarily pay for. Quality. The right thing. Care coordination. Optimal efficiency.")
22
Medicare anesthesia payment
(Base + time units) x (anesthesia CF) Rules determined by: Statutes enacted by Congress Regulations adopted by Medicare agency (CMS) Sub-regulatory policy adopted by Medicare Medicare Administrative Contractor that operates Medicare in each state, regionally
 x (anesthesia CF) Rules determined by: Statutes enacted by Congress. Regulations adopted by Medicare agency (CMS) Sub-regulatory policy adopted by Medicare. Medicare Administrative Contractor that operates Medicare in each state, regionally.")
23
Most common anesthesia services
QZ, CRNA non-medically directed (NOT AA!) QX, CRNA medically directed by an anesthesiologist QK, anesthesiologist medically directing 2, 3 or 4 concurrent CRNA cases AA, personally performed by an anesthesiologist
 QX, CRNA medically directed by an anesthesiologist. QK, anesthesiologist medically directing 2, 3 or 4 concurrent CRNA cases. AA, personally performed by an anesthesiologist.")
24
TEFRA medical direction rules
Anesthesiologist performs all seven tasks in each of up to four concurrent cases provided by a CRNA Fee split 50/50 between CRNA and medically directing anesthesiologist A payment model not a standard of care Encourages higher-cost anesthesia delivery without demonstrated quality improvement

25
What are the TEFRA rules?
Performs a pre-anesthetic examination and evaluation; Prescribes the anesthesia plan; Personally participates in the most demanding procedures in the anesthesia plan, including induction and emergence; Ensures that any procedures in the anesthesia plan that he or she does not perform are performed by a qualified anesthetist; Monitors the course of anesthesia administration at frequent intervals; Remains physically present and available for immediate diagnosis and treatment of emergencies; and Provides indicated-post-anesthesia care. MCM Ch 12 Sec 50G MCM Ch 12 Sec 50G

26
Medical Direction Undermined
[DO NOT READ THIS BRACKETED STATEMENT. THESE SLIDES WERE PREPARED BY AANA FGA AND COMMS, 3/14-15, 2012, for the use of American Association of Nurse Anesthetists members making presentations.] As you may have read from President Malina’s message the other day, lapses in anesthesiologist supervision of CRNAs are common even when an anesthesiologist is medically directing as few as two CRNAs, according to an important new study published in the March issue of the journal Anesthesiology. The study, titled “Influence of Supervision Ratios by Anesthesiologists on First-case Starts and Critical Portions of Anesthetics,” looks at over 15,000 anesthesia records in one leading U.S. hospital and raises critical issues about propriety and compliance in the most common and costly model of anesthesia delivery at a time when quality and cost-effectiveness are white-hot healthcare issues at every level. Anesthesiology 2012; 116:

27
Of the anesthetics you personally administer, how often is an anesthesiologist involved in the following activities? Anesthesiologists are present with full-time CRNAs most commonly for pre-anesthetic assessment and emergencies. Anesthesiologists are least often present for emergence from anesthesia. Yet, is patient safety at issue here? No. The AANA has long held that medical direction ratios have nothing to do with quality of care, and everything to do with reimbursement systems—inefficient, unsustainable systems that make healthcare cost too much and divert millions upon millions of scarce healthcare dollars from real patient needs. Recent landmark studies on anesthesia safety and cost-effectiveness published in the journals Health Affairs and Nursing Economic$ have confirmed the safety and cost-effectiveness of CRNAs, and the Institute of Medicine in The Future of Nursing emphasizes APRN safety in arguing for nurses to practice to their full scope. AANA 2011 member survey, unpublished. 2011-2 0809

28
Anesthesiologist Supervision Often Lapses
Now, this study in Anesthesiology confirms anesthesiologist supervision of CRNAs is more honored in the breach than in the observance. This graph is drawn directly from the study itself. Anesthesiology 2012; 116:

29
Part B Medical Direction vs Part A Supervision
By an anesthesiologist By operating practitioner, or by an anesthesiologist who is immediately available if needed Seven services required in order to claim medical direction reimbursement (50% of a fee, up to 4 concurrent cases (TEFRA rules) Required as a condition of participation for your hospital, or a condition of coverage in your CAH or ASC Opt-out does not apply Opt-out does apply; 17 states have opted-out
 Required as a condition of participation for your hospital, or a condition of coverage in your CAH or ASC. Opt-out does not apply. Opt-out does apply; 17 states have opted-out.")
30
Part B Medical Supervision
MDA supervises 5 or more CRNAs MDA bills 3 base units + 1 base unit CRNA bills QX (50%) MAY NOT BE USED FOR FAILED MEDICAL DIRECTION Failed medical direction: CRNA bills QZ and MDA bills “0” per CMS
 MAY NOT BE USED FOR FAILED MEDICAL DIRECTION. Failed medical direction: CRNA bills QZ and MDA bills 0 per CMS.")
31
AANA action on CRNA reimbursement
Anesthesia payment panels Summit on Anesthesia Reimbursement Member education on Business of Anesthesia Building relationships with key payer leaders Comment on changes impacting CRNA reimbursement Development and support of State Reimbursement Director

32
PQRS Reporting program that uses incentive payments and payment adjustments to promote reporting of quality info by eligible professionals (EPs) CRNAs are EPs Report on 50% of Medicare patients by the end of 2013, get a .5% incentive payment In 2015, not reporting results in a 1.5% "adjustment" (meaning reduction). If not reporting, 1.5% cut in your Medicare payments in 2015, which will go to 2% in 2016. CMS proposed rules: 9 measures, registries only
. If not reporting, 1.5% cut in your Medicare payments in 2015, which will go to 2% in CMS proposed rules: 9 measures, registries only.")
33
PQRS CMS cannot accept data codes for reprocessing on a claim that has already been submitted. Providers have until Dec services to add the appropriate code to the claim. There are also registry options. Additional options for avoiding the negative adjustment: reporting one data code for one Medicare patient for one measure in CY13 would help avoid the ding in CY15. If they want a bump in CY15 they have to report 50% plus one. CMS calculate administrative claims for incentives – deadline October 15. (Requires an Individual Access to CMS (IACs) Account). It can take more than a day to calculate.
 Account). It can take more than a day to calculate.")
34
PQRS Payment adjustment information: tip sheet:

35
Provider Nondiscrimination
Part of the Affordable Care Act (Sec. 1206) Promotes consumer choice and cost savings, by prohibiting health plans from discriminating against qualified healthcare providers by licensure Takes effect 2014, subject to notice-and-comment rulemaking Attempts to amend to weaken or strike it
 Promotes consumer choice and cost savings, by prohibiting health plans from discriminating against qualified healthcare providers by licensure. Takes effect 2014, subject to notice-and-comment rulemaking. Attempts to amend to weaken or strike it.")
36
New England Assy of Nurse Anesthetists: Federal Issues & Advocacy

37
ASA on nondiscrimination
New England Assy of Nurse Anesthetists: Federal Issues & Advocacy ASA on nondiscrimination “(T)he Senate bill also includes gratuitous so-called “non-discrimination" language (Sec. 2706). The intentionally vague language, inserted by supporters of paraprofessionals, seeks to prevent health insurers from "discriminating" against non-physician providers in deciding who may participate in their plans. Its practical implications are to open the doors to various disruptive tactics within the insurance marketplace by paraprofessionals, putting Federal law on a collision course with each state’s scope of practice law.”
he Senate bill also includes gratuitous so-called non-discrimination language (Sec. 2706). The intentionally vague language, inserted by supporters of paraprofessionals, seeks to prevent health insurers from discriminating against non-physician providers in deciding who may participate in their plans. Its practical implications are to open the doors to various disruptive tactics within the insurance marketplace by paraprofessionals, putting Federal law on a collision course with each state’s scope of practice law.")
38
Non-discrimination The Obama Administration will not issue regulations interpreting the AANA-backed provider nondiscrimination provision of the Affordable Care Act before it takes effect Jan. 1, 2014 FAQ document issued by Medicare, IRS-Treasury and the Department of Labor Non-grandfathered group health plans and health insurance issuers offering group or individual coverage are expected to implement the provision starting on January 1, 2014, using a good faith, reasonable interpretation of the law.

39
Non-discrimination Rep. Andy Harris (R-MD), the only anesthesiologist in Congress, introduced HR 2817, on July 24 with the backing of the American Society of Anesthesiologists (ASA). “We are deeply concerned that for certain covered services in a number of states, this new part of the Public Health Service Act will be interpreted to provide that all health professional groups be considered as if their education, skills and training were equal even if their state-based medical and healthcare professional licenses or certifications are very different…. This ACA [Affordable Care Act] provision disrupts over a century and a half of dynamic state-based licensure and certification, interjecting the federal government into interpreting the limits of scope of practice and procedure.” The letter was co-signed by medical societies representing dermatologists, family practice physicians, otolaryngologists, ophthalmologists, OB/GYNs and plastic surgeons. Rep. Harris’ legislation was referred to the House Energy and Commerce Committee where he does not serve, and has no cosponsors and no Senate companion bill at this date.
, the only anesthesiologist in Congress, introduced HR 2817, on July 24 with the backing of the American Society of Anesthesiologists (ASA). We are deeply concerned that for certain covered services in a number of states, this new part of the Public Health Service Act will be interpreted to provide that all health professional groups be considered as if their education, skills and training were equal even if their state-based medical and healthcare professional licenses or certifications are very different…. This ACA [Affordable Care Act] provision disrupts over a century and a half of dynamic state-based licensure and certification, interjecting the federal government into interpreting the limits of scope of practice and procedure. The letter was co-signed by medical societies representing dermatologists, family practice physicians, otolaryngologists, ophthalmologists, OB/GYNs and plastic surgeons. Rep. Harris’ legislation was referred to the House Energy and Commerce Committee where he does not serve, and has no cosponsors and no Senate companion bill at this date.")
40
AANA supports direct reimbursement to CRNAs providing pain management services

41
CRNA direct reimbursement for chronic pain management
Medicare has paid CRNAs directly for chronic pain management services The AMA and the ASA oppose CRNAs providing chronic pain management Two Medicare contractors stopped paying CRNAs directly for chronic pain management services These two contractors required that a physician bill for the CRNA chronic pain management services. This is called “incident-to” billing. The Medicare agency has latitude in the Social Security Act, Medicare regulations and the Medicare claims processing manual to authorize direct reimbursement for CRNA chronic pain management services The AMA adopted an ASA resolution to oppose CRNAs providing chronic pain management services and to influence public perception negatively about CRNA education and training This year two Medicare Administrative Contractors (MACs) issued bulletins stopping direct reimbursement to CRNAs for chronic pain management, requiring that a physician bill for the CRNA services and then pay the CRNA - this is called “incident – to” billing
 issued bulletins stopping direct reimbursement to CRNAs for chronic pain management, requiring that a physician bill for the CRNA services and then pay the CRNA - this is called incident – to billing.")
42
Bookmark & Share >> More...

43
NAFA 5/2011 - Health Reform and CRNAs
Physician Resistance American Medical Association Consistently issued resolutions, petitions, and position papers opposing scope of practice AMA Citizens Petition to HCFA (2000) AMA Scope of Practice Partnership (2006) AMA Resolution “Independent Practice of Medicine by Nurse Practitioners” (2006) AMA Scope of Practice Data Series (2009) Health Care Truth and Transparency Act (2011) CMS and CSA sued the State of California (2010) SOPP designed to obstruct scope of practice expansion by nurses and others led by a full time legislative attorney. Developed evidence to discredit access to care arguments. Health Care Truth and Transparency Act ensures that patients receive accurate health care information by prohibiting misleading and deceptive advertising and representation of health care professionals credentials and training
 AMA Scope of Practice Partnership (2006) AMA Resolution Independent Practice of Medicine by Nurse Practitioners (2006) AMA Scope of Practice Data Series (2009) Health Care Truth and Transparency Act (2011) CMS and CSA sued the State of California (2010) SOPP designed to obstruct scope of practice expansion by nurses and others led by a full time legislative attorney. Developed evidence to discredit access to care arguments. Health Care Truth and Transparency Act ensures that patients receive accurate health care information by prohibiting misleading and deceptive advertising and representation of health care professionals credentials and training.")
44
Political Reality Opposition Institute of Medicine Report

45
Continued challenges: Imaging, MACs

46
What Medicare Ruled on Pain Care

47
What Does the Pain Care Rule Say
Medicare will cover services within CRNA scope of practice in a state “The primary responsibility for establishing the scope of services CRNAs are sufficiently trained and, thus, should be authorized to furnish, resides with the states.”

48
Where They Stood For CRNA Pain Care AARP
American Hospital Association and select State Hospital Associations National Rural Health Association Nursing Associations Opposed to CRNA Pain Care AMA “ASA Rebukes CMS Rule for Jeopardizing Patient Safety and Quality Health Care” Source: Comments at and

49
Noridian - LCDs Epidural Steroid Injections: Facet Joint Injections, Medial Branch Blocks, and Facet Joint Radiofrequency Neurotomy:

50
IPRCC HHS charged IPRCC to create a comprehensive population health level strategy for pain prevention, treatment, management, and research. Structure includes 5 Working Panels Professional Education and Training Margaret Faut- Callahan, PhD, CRNA, FAAN Public Health: Care, Prevention, and Disparities Jackie Rowles, CRNA, MS

51
IPRCC Structure

52
VHA Nursing Handbook Update
APRNs as LIPs – Cathy Rick, CNO IOM “Future of Nursing” Consistent with current anesthesia handbook Dear Colleague Letter: The Honorable Eric Shinseki. Secretary of Veterans Affairs ASA Campaign Over 40 nursing groups co-signed letter to Shinseki this week Met with Interim CNO – Christine Engstrom

53
ASA message and response
ASA said CRNA LIPs would be “required” to function without physician oversight. In response, the AANA-AVANA letter stated that “the truth is that neither the VHA draft Nursing Handbook nor the term ‘Licensed Independent Practitioner’ suggest that CRNAs and other APRNs would be ‘required’ to function without physician involvement should the VHA designate APRNs as LIP.” ASA said the Nursing Handbook would result in “effectively eliminating physician-nurse team-based coordinated care. In response, the AANA-AVANA letter stated, “The ASA statement is false. While the VA Anesthesia Handbook supports care provided in teams, it does not require anesthesiologist supervision of CRNAs. Consistent with the Anesthesia Handbook, several VHAs are staffed solely by CRNAs working without anesthesiologist supervision…. Overall care of the patient remains a collaborative effort among physicians, APRNs, nurses and other healthcare professionals, as it should.” ASA cited its long-discredited “Silber” study as justification for concluding “anesthesia care is improved with the involvement of a physician anesthesiologist in a team.” In response, the AANA-AVANA letter stated that “This ASA statement misrepresents the findings of a claims-data based study, the results of which have not been replicated and have been disregarded by Medicare.”

54
Anesthesia Payment Teaching Rules
What Medicare pays for services when education of anesthesia students or residents is involved When it’s 1:1, payment is as though qualified provider (CRNA, anesthesiologist, or medically directed CRNA) is delivering the service 74 FR 61738, /25/2009. 74 FR 61738, /25/2009.
 is delivering the service. 74 FR 61738, /25/ FR 61738, /25/2009.")
55
Teaching Rules: 1 to 2 CRNA uses QZ modifier, present during pre- and post-anesthesia care and during concurrent cases Anesthesiologist uses AA + GC modifier, present during critical or key portions, immediately available

56
Teaching rules: Medically directed
Medically directed CRNA gets 50% of a fee in one SRNA case, and discontinuous time in each of two concurrent SRNA cases

57
Teaching Rules inequity issue: MD with resident vs MD with SRNA

58
Medicaid and CHIP Federal-state program for indigent pregnant women or women with children, and for indigent seniors in post-acute nursing home settings Covered services vary by state Affordable Care Act expansion of Medicaid

59
Private coverage Insurance Self-administered plans By type:
Fee for service Preferred provider organization Health maintenance organization High deductible health plan

60
Comparing average 13-unit anesthesia fee

61
Reimbursement of CRNA services
Past Present and Future Fee-for-service FFS, ACOs, bundled global & capitated systems Periodic SGR cuts Will they fix SGR? 50/50 public/private Trend toward more public as share of retirees grows Small share Medicaid Medicaid expansion

62
The Affordable Care Act of 2010
Expansion of coverage Medicaid expansion, subsidies in exchanges Insurance reforms State-based exchanges for marketing coverage Nondiscrimination, consumer protections Delivery system reforms Accountable Care Organizations Innovation Center Independent Payment Advisory Board Financing

63
Workforce Provisions Title 8 Reauthorization
Graduate Nursing Education National Healthcare Workforce Commission

64
Title 8 Funding, $MM

65
Graduate Nursing Education
Part of ACA, funded through GME Four-year, up to $200MM total to expand education of APRNs in five hospitals Duke (Durham) Memorial-Hermann Texas Medical Center (Houston) Penn (Philadelphia) Rush (Chicago) Scottsdale Healthcare Medical Center (Scottsdale) Evaluation
 Memorial-Hermann Texas Medical Center (Houston) Penn (Philadelphia) Rush (Chicago) Scottsdale Healthcare Medical Center (Scottsdale) Evaluation.")
66
Coverage Provisions Medicaid Expansion Exchanges
Increase eligibility for Medicaid Additional federal funding for new participants Exchanges A regulated means to market health plans

67
Supreme Health Reform Decision
Is requiring a person to purchase health coverage or pay a penalty constitutional? Is expanding Medicaid, a state-run program with some federal funds, constitutional?

68
Medicaid expansion in the ACA
For beneficiaries up to age 65 up to 138% FPL (FPL = $15,415 for an individual in 2012) Starts in 2014, feds pay 100% of expansion, declining to 90% by 2020 and years thereafter Supreme Court: Unconstitutional to take away a state’s Medicaid for refusing to expand it Mississippi is rejecting Medicaid expansion (Gov. Bryant, 11/7/12) Source:
 Starts in 2014, feds pay 100% of expansion, declining to 90% by 2020 and years thereafter. Supreme Court: Unconstitutional to take away a state’s Medicaid for refusing to expand it. Mississippi is rejecting Medicaid expansion (Gov. Bryant, 11/7/12) Source:")
69
Exchanges (Marketplaces) and Essential Health Benefits
Exchanges are for marketing health coverage in a state State-based exchange (As of Oct. 1 working well) Federally facilitated exchange (disaster so far) Combination ( jury is out) Essential Health Benefits link to benchmarks of small business plans in a state
 Federally facilitated exchange (disaster so far) Combination ( jury is out) Essential Health Benefits link to benchmarks of small business plans in a state.")
70
Delivery System Reforms
Accountable Care Organizations Center for Medicare & Medicaid Innovation Independent Payment Advisory Board (IPAB)
")
71
Implementation Timeline
NAFA 5/ Health Reform and CRNAs Implementation Timeline 2011: Various pilot projects and advisory panels launch, Title 8 reauthorization, beginning of Medicaid expansion implementation 2012: Graduate Nursing Education 2012: Supremes decide constitutionality 2013: Finalization of plans 2014: Provider nondiscrimination, state based exchanges take effect

73
Budget Sequestration Sequestration is $1.2 trillion in automatic spending cuts due to go into effect over the next 10 years $85 billion 3/1/12 Half by dollar value from national security Medicare, -2% Other health and research, -8% National security, -9% Exempts Medicaid, Veterans benefits, most student aid Agency flexibility in apportionment?

74
Pew: Increase, decrease or same?
Aid to world’s needy 21 28 48 Aid to needy in U.S. 27 44 24 Health care 38 34 22 Medicare 36 46 11 Education 60 29 10 Social Security 41 Veterans benefits 53 6 Pew Research Center, 2/13-18/2013. Pew Research Center, 2/13-18/2013.

75
AANA supports permanent repeal and replacement of the SGR formula with a payment system that accurately reflects the cost of providing anesthesia care.

76
Briefing: SGR The Sustainable Growth Rate (SGR) is a Medicare Part B payment formula for CRNA and physician services SGR is based on the economy Reduced payment has been threatened since 2002 Every year Congress defers rather than repeals the SGR cuts 2012 CRNA payment will decrease by 26.2% in MARCH The Sustainable Growth Rate (SGR) is a formula used to calculate physician (and CRNA) payments for Medicare patients SGR is based on the national economy but health care costs have risen faster than the GDP For every year beginning in 2002 the SGR formula has called for substantial reductions in physician (CRNA) payment rates The Center for Medicare and Medicaid Services (CMS) projects that the 2012 physician (CRNA) fee schedule conversion factor will decrease 29.5 percent.
 is a formula used to calculate physician (and CRNA) payments for Medicare patients. SGR is based on the national economy but health care costs have risen faster than the GDP. For every year beginning in 2002 the SGR formula has called for substantial reductions in physician (CRNA) payment rates. The Center for Medicare and Medicaid Services (CMS) projects that the 2012 physician (CRNA) fee schedule conversion factor will decrease 29.5 percent.")
77
What’s a 26.2% Medicare Cut? If a CRNA performs unit 100% Medicare cases, that yields $236,700 in fees Minus 30% = $165,690 Difference of -$71,010 if 26.2% cuts hit 3/1/2012 Congress continues struggling with paying for relief from 26.2% Medicare Part B payment cuts scheduled for March 1. The AANA and CRNAs have weighed-in and continue to, but the outlook for long-term relief is dim and short-term relief appears more likely. Approximately $365.00/week But what are these huge Medicare cuts anyway? Say a CRNA performs unit cases, that are all on Medicare patients, that are all paid 100% to the CRNA as nonmedically directed services including the patient’s copay. On the bottom of this page, you can see the effects of what AANA has already done for CRNAs. For the year beginning January 2008, Medicare would have paid about $243 for each of those cases, for a total of $218,700 for the year. But Medicare at that time was predicting total payment cuts of 15% for CRNA and physician services by January Had those cuts taken effect, Medicare would have paid not $243 but $207 for each case, totalling $186,300. That would have been a reduction of more than $32,000 in Medicare anesthesia payment from one year to the next. But AANA was at work. And instead of a cut, CRNAs got an increase, so that those same cases this year pay $236,700. However, if Medicare cuts payments 20% in 2010, that’ll mean a reduction in anesthesia payments approaching $50,000. The actual Medicare cuts coming April 1, 2010, unless Congress acts equal 21.2%. If you’re employed by a hospital, or a group, or in independent business, the question is the same: If those cuts hit, where will that money come from? We have got to keep working together to win in Washington to reverse these extreme cuts.

78
What’s new with SGR Energy and Commerce plan to replace SGR with a quality-based plan that would update payments by .5 – 1 % each year. Update Medicare payment rates by 0.5 percent until 2019, until performance-based payment methods: the Quality Update Incentive Program and the Alternative Payment Model, which could increase doctors’ payments by as much as 1 percent. The CBO scored the SGR reform bill $175.5 billion over 10 years. Freezing SGR payments will cost $139.9 billion. $36 billion comes from the cost of replacing that system with a quality-based payment plan.

79
SGR Key Talking Points 4 years ago Medicare said anesthesia services were undervalued CRNAs do not control service volume CRNAs provide access to care in rural America CRNAs are 25% more cost effective Quality of CRNA care is equal All barriers to the use of CRNAs should be eliminated 4 years ago Medicare increased payment for anesthesia services by 25% 4 years ago because anesthesia services were determined to be persistently undervalued by an independent government agency (GAO 2007) CRNAs are do not control service volume as other specialties do – the intention of SGR was to affect the incentives of individual physicians (CRNAs) concerning the rate of use of services CRNAs as the sole anesthesia provider are 25% more cost effective than the next least costly model (Nursing Economic$ 2010) There is no difference in quality of care between CRNAs and other anesthesia providers (Health Affairs 2010) All barriers should be eliminated to the use of advanced practice registered nurses such as CRNAs (Institute of Medicine 2011)
 CRNAs are do not control service volume as other specialties do – the intention of SGR was to affect the incentives of individual physicians (CRNAs) concerning the rate of use of services. CRNAs as the sole anesthesia provider are 25% more cost effective than the next least costly model (Nursing Economic$ 2010) There is no difference in quality of care between CRNAs and other anesthesia providers (Health Affairs 2010) All barriers should be eliminated to the use of advanced practice registered nurses such as CRNAs (Institute of Medicine 2011)")
80
What Can AANA & CRNAs Do? Know the issues
Participate in AANA advocacy programs Mid-Year Assembly CRNA-PAC FPDs & Key Contacts CRNAdvocacy Alerts Initiatives in reimbursement – SRS State level GRC, PAC and BOD

81
SRS Program

82
SRS Background AANA Anesthesia and Payment Policy Coordinating Panel (APPCP) recommendation to the AANA BOD AANA BOD approved September 2012 Goal: reimbursement advocacy in each state The SRD repository of state reimbursement information coordinator of state advocacy work.

83
State Reimbursement Specialist program
At the direction of the Board A focal point in each state for CRNA reimbursement knowledge, and for advocacy of CRNA reimbursement interests Development of key relationships Private payors – three largest health plans in state Public payors – Medicaid, exchanges, MAC Other interests – Hospital, rural health and health plan associations Coordinated by your AANA FGA team

84
Objectives Monitor trends Serve as a resource
Work with state association to establish key relationships

85
SRS Position Requirements
Keen interest in reimbursement Willing to enhance knowledge Represent with professionalism and enthusiasm Willing to disclose conflicts of interest

86
Job Description Coordinate and improve payment processes and reimbursement in your state Accomplish this task by working with others based on state association’s needs and resources

87
Job Description Establish key contacts with
Top three health plans in your state Exchange Boards Medical Director for Medicare Administrative Contractor Medicaid Director Insurance Commissioner State Hospital Association State Ambulatory Surgery Center Association State Rural Health Association

88
Job Description Serve as a repository of information by monitoring state reimbursement activities: Medicare Local Coverage Determinations (LCDs) Medicaid payment policy Commercial insurance reimbursement Accountable care organizations (ACOs) State exchanges
 State exchanges.")
89
Job Description Assist with state reimbursement issues as a first responder Communication with state leaders Enter state reimbursement information into special SharePoint site Alert the AANA to any emerging issues

90
PALS Volunteers who get others to volunteer or contribute Volunteers - contributors Constituents: Everyone who voted for the candidate Voters who voted for the wrong candidate Registered voters who don’t vote Voting age not registered to vote

91
through federal political advocacy.
What is CRNA-PAC? Separate fund, 100% from CRNAs’ voluntary contributions, not dues Ensures CRNAs have access to DC, where our issues are decided Not partisan Always working for the profession of nurse anesthesia CRNA-PAC’s Mission Statement: Advancing the profession of nurse anesthesia through federal political advocacy.

92
Stats that Make Us Proud
Largest federal nursing PAC in the country Top ten PAC nationwide for healthcare professionals $1.1 million impact on the 2012 national elections with 94% of CRNA-PAC supported candidates elected to office.

93
2013 CRNA-PAC Highlights $1.75 million goal for 2013-2014
“CRNA-PAC Loves the 80’s” Party at Mid-Year Assembly “Remember the RatPAC” Party at Annual Meeting Refreshed Care to Be Counted website, Student-specific engagement New Incentive Club levels

95
Does This Work? A case study
Problem: Present threat to CRNA pain practice Strategy: Research. Grassroots. Local & national allies. Advocacy. Response. Comments. Outcome: Medicare rule covering all CRNA services within state scope of practice published 12/2012, effective 1/2013

96
Thank You from Your AANA FGA
Frank Purcell, Senior Director Federal Goverment Affairs Christine Zambricki, Senior Director Federal Affairs Strategies Kate Fry, Associate Director Political Affairs Romy Gelb-Zimmer, Associate Director Federal Regulatory and Payment Policy Randi Gold, Associate Director Federal Regulatory and Payment Policy Ralph Kohl, Associate Director Federal Government Affairs Candida Richardson, Administrator AANA Division of Federal Government Affairs 25 Massachusetts Ave., Suite 550 Washington, DC // //

Similar presentations







 of 2005 Dan Walter Sr. Health Policy Analyst AAP Division of State Government Affairs AAP National Conference.>")






 implements broad, historic changes to U.S. health care Expanded access to health insurance and care.>")





>")

 Insurance Reforms – No lifetime limits, annual limits – Pre-existing conditions.>")

