Download presentation
Presentation is loading. Please wait.

1
Management of Respiratory Problems in Children
DR SADASIVAM SURESH

2
Learning objectives: Increase understanding of common respiratory disorders in children To be able to recognise common respiratory symptoms and presentations in a child under 2 years of age To understand the ongoing management and surveillance in paediatric asthma Investigations in children with respiratory problem - a systematic approach Multidisciplinary management in chronic conditions. Antibiotics and physiotherapy - synergy in management of chronic respiratory conditions

3
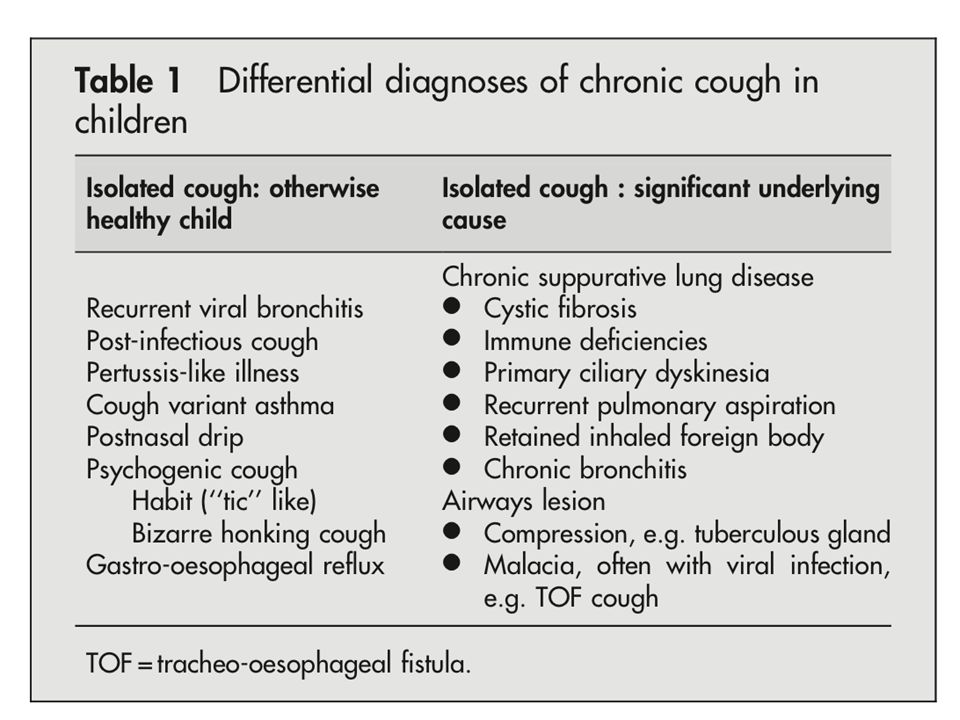
Chronic Cough in Children

4
Road Map Definition Clinical presentation Differential diagnosis
Investigations Management

5
Mechanism of Cough

6
Definition Chronic cough – daily cough for more than 4 weeks
Dry Cough - Discussed separately Moist cough This presentation

7
Figure 1 Differentiated cough patterns.
Marais, B J et al. Arch Dis Child 2005;90: Copyright ©2005 BMJ Publishing Group Ltd.

8
Clinical Presentation
Cough as a symptom Associated symptoms Wheeze Pyrexia Diurnal variation Exercise & activity Sleep Other systemic symptoms Reflux Cardiac Congenital abnormality

11
Suppurative Cough

12
Decision Tree

16
Investigations

17
Management points Value of CXR Chronic Bronchitis of unknown aetiology
Follow-up CXR & timing Chronic Bronchitis of unknown aetiology Physiotherapy Prolonged course of antibiotics Role of Bronchoscopy Sequential investigation

18
Family/Patient preference

19
Cough Benefits

20
What is it and what to do about it.
Bronchiolitis Croup What is it and what to do about it.

21
bronchiolitis Affects infants, males = females
At risk - bottle fed, crowding - CHD, CNLD Causes RSV Human metapneumovirus Influenza parainfluenza (3) adenovirus Illness predominately seen in infants Hospitalized - 80% in 1st year 50% 1-3 months Severe bronciolitis more severe in males
 adenovirus. Illness predominately seen in infants. Hospitalized - 80% in 1st year 50% 1-3 months. Severe bronciolitis more severe in males.")
22
Figure 1 Comparison of the frequency of detection of human metapneumovirus (hMPV) with other respiratory viral pathogens. RSV, respiratory syncytial virus. Garcia-Garcia, M L et al. Arch Dis Child 2006;91: Copyright ©2006 BMJ Publishing Group Ltd.

23
Figure 4 Age distribution of hMPV and RSV single infections.
Garcia-Garcia, M L et al. Arch Dis Child 2006;91: Copyright ©2006 BMJ Publishing Group Ltd.

24
Figure 3 Monthly distribution of hMPV and RSV single infections.
Garcia-Garcia, M L et al. Arch Dis Child 2006;91: Copyright ©2006 BMJ Publishing Group Ltd.

25
RSV Predominant pathogen 2 strains - A and B
All children exposed by 3 years Spreads from nasopharynx to lungs Kills respiratory epithelial cells In vitro - large syncytia A may be associated with more severe disease

26
Pathogenesis Ciliated epithelial necrosis
Mononuclear cell infiltrate, oedema, mucous plugs CXR - hyperinflation and patchy infiltrates, collapse Repair - cilia by day 15 Thought to be little smooth muscle contraction - little response to bronchdiloators

27
Clinical Incubation - 5 days Coryza
tachypnoea, wheeze, crackles, hypoxia - 1 to 3 weeks Bacterial superinfection rare (1-2%) Residual symptoms Wheeze average 9 days, ceases with coincident rise in secretory IgA
 Residual symptoms. Wheeze average 9 days, ceases with coincident rise in secretory IgA.")
28
diagnosis Clinical NPA - respiratory viruses

29
Management Oxygen - saturations < 94%
Fluids - oral feeds, NG feeds, IV fluids, ventilation NOT - antibiotics, steroids, bronchodilators, physiotherapy Ribavirin - expensive antiviral, no proven efficiency Bronchodilators may be trialed - FHx asthma, atopy

30
RSV prevention RSV immunoglobulin - monthly injection during winter, CNLD Oxygen dependent, < 2 years Decreases hospital admissions (NNT 17) and ICU admission (NNT 50) IMPACT study
 and ICU admission (NNT 50) IMPACT study.")
31
Croup - laryngotracheobronchitis
Changing epidemiology Viral cause - most common: Parainfluenza

32
symptoms Barking cough Stridor Hoarse voice +/- URTI symptoms

33
BEWARE <4 months: structural airway lesions High fevers
Day time onset Cord, laryngeal cyst, paillomatosis, extrinsic compression eg vascular ring Tracheitis, abscess, epiglottitis (rare since HIB immunization)
")
34
treatment Humidification - placebo effect
Steroids - parenteral, oral, nebulized Rapid onset of therapeutic effect - improvement within 1-2 hours and sustained Nebulized adrenaline intubation Little work done on oral steroids - most on parental dexamethasone Asthma doses benefit - duration of hospital stay, need for adrenaline, clinical parameters, dose can be repeated 24 hours later - prolonged courses unnecessary Nebulized budesonide 2mg Nebulized adrenaline: rapid improvement, duration of effect 2-3 hours Traditionally admitted to hospital?home if no stridor at 2-3 hours, one dose only Intubation - virtually never: if previous airway abnormality

35
Admit if Stridor at rest Needed nebulized adrenaline < 12 months
Past Hx severe croup High risk child eg Down syndrome

36
Under 2 years Stridor -Laryngomalacia -Congenital lesion - biphasic
Congenital lung lesions -CCAM

37
Thanks to Dr Scott Burgess PhD FRACP
Asthma in children Thanks to Dr Scott Burgess PhD FRACP

38
Outline What is asthma Pre-school wheeze Montelukast (Singulair)
Inhaled corticosteroids LABAs Difficult asthma / when to refer Managing acute asthma in general practice

39
What is asthma? Asthma is characterised by four key features: Symptoms
Bronchoconstriction Bronchodilation Inflammation

40
What is asthma? Asthma is characterised by four key features: Symptoms
Bronchoconstriction Bronchodilation Inflammation Wheeze: Due to vibration of airways as gas flows through them Most commonly expiratory Parents often become confused by rattle from large airway secretions.

41
What is asthma? Asthma is characterised by four key features: Symptoms
Bronchoconstriction Bronchodilation Inflammation Cough: Cough is a common feature of asthma However, a chronic isolated cough is not asthma and will not respond to salbutamol and ICS.

42
What is asthma? Asthma is characterised by four key features: Symptoms
Bronchoconstriction Bronchodilation Inflammation Bronchoconstriction: Narrowing of airways in response to a trigger Basis of challenge testing and can be helpful in difficult diagnosis.

43
What is asthma? Asthma is characterised by four key features: Symptoms
Bronchoconstriction Bronchodilation Inflammation Bronchodilation – reversible airways narrowing Improvement in work of breathing and lung function following salbutamol Again very helpful – lung function testing when child is unwell.

44
What is asthma? Asthma is characterised by four key features: Symptoms
Bronchoconstriction Bronchodilation Inflammation Inflammation – most commonly eosinophilic Basis of steroid treatment Difficult to test – exhaled nitric oxide and induced sputum Little known about inflammation in preschool wheeze.

45
Pre-school wheeze Small children have small air-pipes
Poiseuille’s law: flow is proportional to 4th power of the radius of the pipe Small changes in the size of the pipes results in big changes in flow Viral induced oedema can cause wheeze independent of smooth muscle constriction Half of all children wheeze at some point Infants whose mother’s smoke have narrower small airways Some infants have narrower airways and wheeze with viral infections but grow out of the tendency to wheeze with time – transient wheezers.

46
Pre-school wheeze Pragmatically we divide children into:
Viral induced wheeze [viral exacerbations only] Multi-trigger wheeze [viral exacerbations as well as symptoms with exercise, at night, exposure to smoke and allergens] (Brand 2008) Mixed evidence regarding oral steroids in pre-school wheeze Probably little and more likely no benefit (Csonka 2003 and Panickar 2009) No benefit from parent initiated oral steroid in preschool wheeze (Vuillermin 2011) No benefit from ICS in viral induced wheeze (Wilson 1995) Modest benefit from ICS in children with multi-trigger wheeze [treat 7 children to prevent 1 exacerbation] (Castro-Rodriguez 2009) ICS do not modify disease progress at any age.
 Mixed evidence regarding oral steroids in pre-school wheeze. Probably little and more likely no benefit (Csonka 2003 and Panickar 2009) No benefit from parent initiated oral steroid in preschool wheeze (Vuillermin 2011) No benefit from ICS in viral induced wheeze (Wilson 1995) Modest benefit from ICS in children with multi-trigger wheeze [treat 7 children to prevent 1 exacerbation] (Castro-Rodriguez 2009) ICS do not modify disease progress at any age.")
47
Montelukast (Singulair)
Leukotreine receptor antagonist block receptors on smooth muscle and other cells, preventing the action of these mediators The effects are modest: Preschool wheeze – 9 children to prevent exacerbation and 19 to prevent medical review, no effect on hospitalisation rates School aged wheeze – more effective but not as effective as ICS Modest effect as add on to low dose ICS (not supported by PBS for this role) Side-effects are very uncommon Consider as first line for school aged children whose parents don’t want ICS (although low does ICS don’t have measurable side effects) Role in exercise induced asthma.
 Side-effects are very uncommon. Consider as first line for school aged children whose parents don’t want ICS (although low does ICS don’t have measurable side effects) Role in exercise induced asthma.")
48
Inhaled corticosteroids steroids (ICS)
When to start? Frequent exacerbations (every 4-6 weeks regularly) Persistent disease: Symptoms between exacerbations (waking at night, minimal exertion, frequent wheeze) Using reliever 2-3 times per week (except for exercise) Abnormal lung function with bronchodilator response Medication and dose All inhaled steroids are much the same Start low or moderate (eg Fluticasone ug/day) and wean as able Steep dose response curve (most children controlled with 100 micrograms per day) Side-effects more likely as increase, especially at 500 ug/day or higher.
 Persistent disease: Symptoms between exacerbations (waking at night, minimal exertion, frequent wheeze) Using reliever 2-3 times per week (except for exercise) Abnormal lung function with bronchodilator response. Medication and dose. All inhaled steroids are much the same. Start low or moderate (eg Fluticasone ug/day) and wean as able. Steep dose response curve (most children controlled with 100 micrograms per day) Side-effects more likely as increase, especially at 500 ug/day or higher.")
49
Inhaled corticosteroids steroids (ICS) 2
How to give? Puffer and spacer unless child refuses to use Dry powder device only in those >= 7 years of age Face mask only in those < 3 years of age Must know how to use and demonstrate to child / parent Check inhalation technique as regularly as you can Placebos and information on lung delivery can be helpful Wash spacer in soapy water and air dry to reduced static and increase delivery.

50
Long acting beta agonists (LABA) Seretide / Symbicort
Pre-school children: There are no trials of LABAs in pre-school children and no indications for prescription in this group (Do not prescribe to pre-school children) LABA as add on to ICS: BTS guidelines LABA plus low dose ICS vs moderate dose ICS Safety and a note of caution: No evidence of significant adverse effects when used in combination with ICS. Adverse event profile in younger children not well recorded.
 LABA as add on to ICS: BTS guidelines. LABA plus low dose ICS vs moderate dose ICS. Safety and a note of caution: No evidence of significant adverse effects when used in combination with ICS. Adverse event profile in younger children not well recorded.")
51
Difficult asthma / when to refer
Asthma that is not well controlled despite moderate dose ICS plus add on medication eg Seretide 500 ug / day Previously - Difficult asthma clinic at Mater Children’s Hospital 6 years and older Poorly controlled asthma Physician, nurse, scientists, psychologist and research assistant Top 3 reasons: Not asthma, poor inhalation technique, poor adherence Comprehensive Asthma Assessment and Management Program When to refer? Worried about diagnosis: Chronic moist cough, poor weight gain, focal signs Not well controlled on Flixotide 250 ug per day and good inhalation technique.

52
Managing acute asthma in your practice
Stay calm and keep them calm Call for help (000) if severe or dose not respond to first dose of salbutamol Airway and oxygen (keep sats >94%) Given salbutamol [a lot] – Asthma foundation 4 puffs (but can give up to 12puffs) Given oral prednisone 2mg/kg orally (no need for IV) If responds: Give written plan Ensure knows how to give medication Follow-up to review management Patient should go to hospital if needing reliever more than every 3 hours.
 if severe or dose not respond to first dose of salbutamol. Airway and oxygen (keep sats >94%) Given salbutamol [a lot] – Asthma foundation 4 puffs (but can give up to 12puffs) Given oral prednisone 2mg/kg orally (no need for IV) If responds: Give written plan. Ensure knows how to give medication. Follow-up to review management. Patient should go to hospital if needing reliever more than every 3 hours.")
53
Lung function testing in General Practice
Who performs LFT in children? What are the barriers to performing lung function testing?

54
Top Tips Confirm the diagnosis ICS
History of musical not rattly wheeze, wheeze not cough Review when unwell Lung function testing ICS Low or moderate dose (Flixotide 50ug twice daily or 125 ug twice daily) Do not use LABA 1st line or in pre-school children Demonstrate use of spacer and check technique Check for concerns as well as provide general educational information Provide asthma plan Ask about smoking / encourage stop smoking even if away from child.
 Do not use LABA 1st line or in pre-school children. Demonstrate use of spacer and check technique. Check for concerns as well as provide general educational information. Provide asthma plan. Ask about smoking / encourage stop smoking even if away from child.")
55
Lung Volumes VT: Tidal Volume VC: Vital capacity
IRV: Inspiratory reserve volume IC: Inspiratory capacity ERV: Expiratory reserve volume FRC: Functional reserve capacity RV: Residual volume TLC: Total lung capacity

56
In summary: Rapid flight through respiratory paediatrics
Common presentations to general practice High percentage managed by general paediatricians Definite role for tertiary specialists to treat, empower, educate and advocacy

57
Helping Kids Breathe and Sleep Better
OUR VISION: To provide high quality holistic care in paediatric respiratory and sleep medicine to children and their families. OUR MISSION: Q-Class will provide readily accessible comprehensive care to children with respiratory and sleep problems in a multidisciplinary setting and promote ongoing health and well-being in partnership with their family. Helping Kids Breathe and Sleep Better

58
CASE STUDY - 1

59
Case Study - 1 Interpret flow volume loop Possible diagnosis

60
CASE STUDY - 2

61
CASE STUDY - 2 Comment on flow volume loop
Comment on Bronchodilator response Comment on FVC

62
CASE STUDY - 3

63
CASE STUDY - 4

64
CASE STUDY 3 & 4 Comment on the lung function values What is the likely diagnosis Comment on the mid expiratory flow values

65
CASE STUDY - 5 Comment on lung function values/loop
The residual volume is 230% predicted –likely diagnosis?

66
CASE STUDY -6

67
CASE STUDY - 6 Patient attended respiratory clinic for follow-up after ICU admission The green highlighted value was at the time of ICU admission Comment on possible diagnosis and long term outlook

68
CASE STUDY 7 These are lung function value of a 32 year old adult
What more information would you like to know?

69
CASE STUDY - 8 Well controlled asthmatic what other history would you ask?

Similar presentations








 Dr. Walaa Nasr Lecturer of Adult Nursing Second year.>")



 -based on the recognition of a characteristic pattern of symptoms and signs and the absence of an alternative.>")
: i1-i92.>")

 What’s new in GINA 2015?>")





