Download presentation
Presentation is loading. Please wait.

1
Homework/Recap Review the flipchart for the whole process of pre and post testing (pink section). Write down exactly which pages you would go to for counselling in these sitatuations: 1. testing HIV exposed infant 2. testing child who turns out to be positive 3. testing a child who turns out to be negative 4. testing an adolescent who tests HIV positive and needs SRH counselling [Go to the next slide of Topic 1 to review the answers.]

2
1. Testing exposed infants:
For pre-test: 2, 3, 6 Post-testing: 5, 6, 7 2. Testing child who turns out to be positive: For pre-test: 2, 3, 4 Post-testing: 5, 8 3. Testing a child who turns out to be negative: Post-testing: 5, 9 4. Testing an adolescent who tests positive and need SRH counselling: Post-testing: 5, 8, Topic 4

3
Module IV: Preparing to Start ARVs and Supporting Adherence
In this module, we will discuss: Unit 1: Understanding Staging and ART Initiation Process Unit 2: Counselling for the Start of ARVs Unit 3: Supporting Adherence As you introduce the units in this module, also introduce the following key questions. Write the key questions on a flipchart, so that they can be referred to while the module is presented. Note that the key questions are answered in the slides called “key points” at the end of the module. Key Questions for M4 When should children under 2 years start ART? What are the criteria for “readiness to start ART”? Why is disclosure important for good adherence? How can side effects affect adherence? How can adherence problems be prevented?

4
Counselling to Start ARVs and Supporting Adherence
Who is this counselling for? Patients who have received a positive HIV test, have been staged and are eligible to start ART Goals: Explain the process of staging and ARV initiation Determine if the patient is able to adhere to ARVs Help the patient understand what to expect during the first weeks on treatment Provide ongoing counselling to support adherence [slide is animated– ask participants to brainstorm about who this type of counselling is for and the goals] Preparing to Start ARVs: After testing positive, the patient is referred to the clinic for staging. At that point, the clinician may recommend starting treatment or waiting for a while. Once the clinician has determined that the patient is eligible to start treatment, the patient will come for counselling to ensure readiness for ARVs. The counsellor may provide more than one counselling session, depending on the client’s situation. *note that children under 2 years should start ART right away– counselling should not delay the start of ART for infants. Supporting Adherence: After the patient has started ARVs, they may face some challenges. Over time, patients may struggle with long-term adherence, side effects and toxicities and challenges related to disclosure. Also, as the child grows and experiences changes in life, additional counselling may be needed to support healthy behaviours. Keep in mind that in this module, we are talking about a series of counselling sessions– the exact number will vary depending on the clients’ knowledge about ARVs and adherence.

5
Module IV: Preparing for ART Unit 1: Understanding the Staging and ART Initiation Process
By the end of this unit, participants should be able to: Explain how eligibility is determined. Explain the new paediatric ART eligibility guidelines. Unit Time: 1 hour

6
Understanding Staging
A clinician will determine eligibility by: 1. Using WHO criteria Stages I (asymptomatic), II (mild), III (advanced) and IV (severe). ARVs are usually started in Stage III or IV. 2. By doing a CD4 cell count (or CD4 %) The child should only come for counselling if a clinician has determined that the child is eligible, check this is written in the patient’s chart. Ensure that the caregiver correctly understands the stage and implications of the child’s condition.
, II (mild), III (advanced) and IV (severe). ARVs are usually started in Stage III or IV. 2. By doing a CD4 cell count (or CD4 %) The child should only come for counselling if a clinician has determined that the child is eligible, check this is written in the patient’s chart. Ensure that the caregiver correctly understands the stage and implications of the child’s condition.")
7
Understanding CD4 and Viral Load
The CD4 count The viral load Measures ability to keep ahead of HIV infection Predicts risk of opportunistic infection Predicts risk of death Measures level of infection Predicts CD4 decline Predicts risk of opportunistic infection & other complications Predicts risk of death Testing for CD4 count and viral load should be done regularly.

8
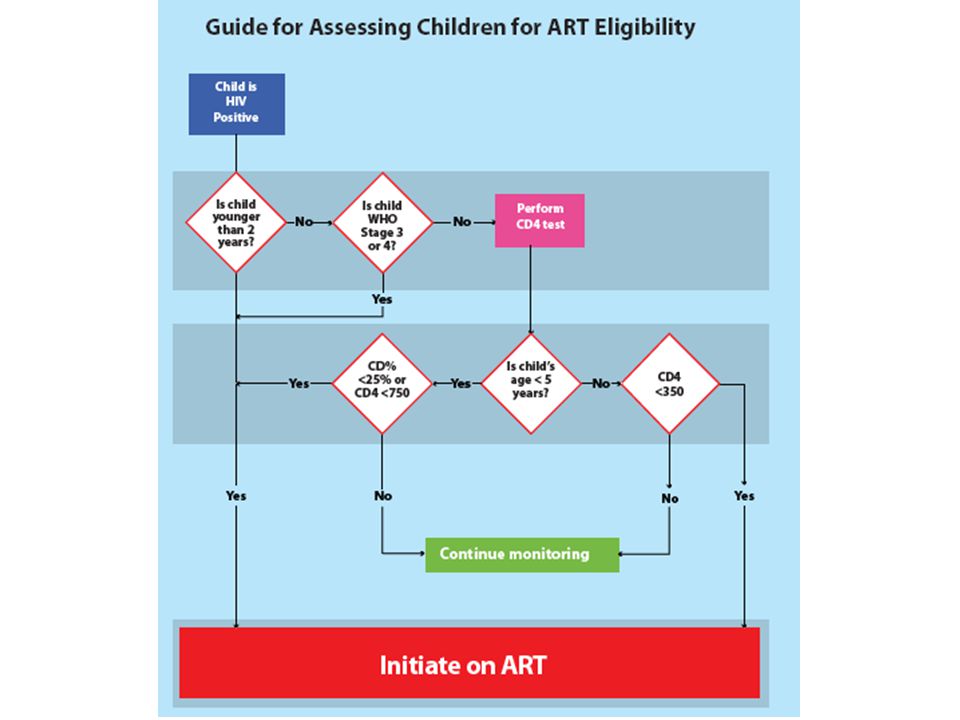
Remember that these are new guidelines issued by the MoH in 2012
Remember that these are new guidelines issued by the MoH in Children under 2 years are started on ART when their HIV status is confirmed, irrespective of CD4 count or clinical staging.

10
HIV/ART Card (Front Side)
Remember that every child who is diagnosed with HIV should have a blue HIV/ART card in their file. There is a place on the back of the card to document your counselling session. Every counselling session should be documented here. Look in your participant manual for a full-size copy of this card, including the section to document counselling.

11
Staging and ART Initiation
How is eligibility determined? What are the new paedriatric eligibility guidelines?

12
Module IV: Preparing for ART Unit 2: Counselling for the Start of ARVs
By the end of this unit, participants should be able to: Describe the benefits of good adherence Counsel caregivers to anticipate adherence challenges that many children and adolescents face Describe several symptoms of side effects that require the counsellor to refer the client to a clinician. Unit Time: 2 hours

13
What is Adherence? ARV adherence means....
the right drug, in the right dose at the right time, with the right frequency and in the right way Adherence is an informed choice–a joint decision. Children have a right to participate in issues that affect their lives. [slide is animated to encourage brainstorming– the title will appear first]

14
Take a look in your manuals to find a larger copy of this diagram.
In short, the clinician assesses the patients clinical condition and decides if he/she is physically ready to start ART. This is called “determining eligibility.” The counsellor is responsible for deciding if the patient fully understands the implications of ART and will be able to adhere to treatment. This is called “determining readiness.”

15
Take a look in your manuals to find a larger copy of this diagram.
As you look at this flow chart of the ART preparation process, what do you notice? The overall focus is on the counsellor driving the process. It is very important that patients– especially children-- not be “lost to follow-up” at this stage. ART improves survival, and loosing or delaying treatment can be fatal for the patient.

16
Key Determinants of Patient Readiness to Start ARVs
ASSESS Do the caregiver and child understand what it means to be HIV infected? Do the caregiver and child understand the importance of taking ARV and how they work Can the caregiver and child demonstrate how to take them? Can the caregiver and child explain what to do if the child experiences side effects of ARVs? Have the caregiver and child both agreed to an adherence plan and are able to address barriers? If the answer to any of these questions is NO, you should address the relevant areas and schedule a follow-up counselling session. But, within the guidelines and most adherence counselling is ongoing and should not stop you from initiating ART, especially in young or sick children. For the first question, it is important to raise the issue of disclosure with the caregiver. Is the child aware of his/her status? If the caregiver is ready to disclose (or if the child is 10 years or older) then the child should be disclosed to about his/her status before starting ART. For children who are not aware that they are HIV infected, the caregiver should have a plan for disclosure to the child at a future time. The child should still understand that he/she is taking medicines that will keep him/her healthy and understand the importance of taking medications each day, without fail. We will discuss helping children understand adherence in the coming slides. Take a look at the Paediatric Counselling Flipchart– on which page to you find these screening questions?
 then the child should be disclosed to about his/her status before starting ART. For children who are not aware that they are HIV infected, the caregiver should have a plan for disclosure to the child at a future time. The child should still understand that he/she is taking medicines that will keep him/her healthy and understand the importance of taking medications each day, without fail. We will discuss helping children understand adherence in the coming slides. Take a look at the Paediatric Counselling Flipchart– on which page to you find these screening questions")
17
In the Table of Contents of the flipchart, under Topic 2 (the green topic), you will see that the sub-topics in this section match the determinants of readiness (except the first screening question which is also addressed on the first page). [Go to the previous slide if need be to show the questions asked.]

18
Turn to page 10, to see another critical aspect of the flipchart and how it works.
Each topic has a ‘profiling’ or ‘screening’ page. The profiling/screening means that you ask a series of questions to determine the precise counselling needs of the client. You do not want to interrogate the client, but the questions can help guide you. Do not feel that you have to ask a question if it has already been discussed and you know the answer. So, first, you need to know if this is the first session with this client. If it is the first session, you will likely start with the first page and flow through all the pages in this Topic---the green topic. However, if the client has been counselled many times, they might just need to review adherence issues, which are toward the end of this section.

19
Turn to the counsellor side of the flipchart that looks like this.
Each question is written as a closed question so that there are a limited number of choices. Each answer from the client either leads to another question, or to instructions about which page to go to in order to start the ‘advise’ part of your session. There is no need to ask the questions if you have already gathered that information from that client and can go right to the page with the content for that client. Once you have turned from this page, there is no reason to come back. You then follow the instructions on the bottom of each page.

20
For instance in Topic 2 (green) on the page after the profile, there is content about ‘How ARVs work’. [Go through the content on this page and point out the ‘Talking with children’ section as well as the illustration.] Once you go through this with your client, you need to make a decision to either flow to the next page about ‘How to take ARVs’, or if you think your client as had enough for one day, (or you are out of time for this client) you can go straight to the ‘Closing’ of that counselling session.
 you can go straight to the ‘Closing’ of that counselling session.")
21
There is an arrow at the bottom of each page that gives instructions
There is an arrow at the bottom of each page that gives instructions. Here, you could go to the next page on ‘How to take ARVs or skip to the ‘Closing’. On each of the pages in this section, you will be instructed to either go to the next page or to the closing. It is more straightforward than the HIV testing section.

22
Although we will look closely at the ‘Closing for adherence’ in a minute, at the bottom of the page, in italics, you will see that you will be reminded about the criteria for being ready to start ARVs. Remember that once the client is ready enough, they should start on the ARVs, but continue to be counselled for good adherence for as many visits as necessary, otherwise, counselling sessions should be on positive living.

23
What are the Benefits of ARVs?
ASSESS Ask clients: What do you see as the benefits of taking ARVs? Slow HIV multiplication in the body Keep your body’s natural defenses strong Ensure good health and continued growth Reduce HIV-related illnesses (OIs) Ensure proper growth and development Improve the quality of life– ability to play, go to school and enjoy life [This slide is animated– the heading will appear first to allow brainstorming. Encourage participants to imagine that they are talking to a child of 10 years– explain the goals using simple, non-clinical language.] Ensure that caregivers are aware that there are significant advantages to starting ART. However, starting ART requires a strong commitment from both the caregiver and the child.
 Ensure proper growth and development. Improve the quality of life– ability to play, go to school and enjoy life. [This slide is animated– the heading will appear first to allow brainstorming. Encourage participants to imagine that they are talking to a child of 10 years– explain the goals using simple, non-clinical language.] Ensure that caregivers are aware that there are significant advantages to starting ART. However, starting ART requires a strong commitment from both the caregiver and the child.")
24
Counselling Process: Explaining ARVs to Younger Children
ADVISE Most caregivers and HCWs struggle with how to explain complex concepts to children This is an opportunity for the HCW to model a good, clear, complete explanation of HIV Explain to the caregiver that we all face challenges in explaining certain concepts to children. As health workers, our understanding of HIV is deeper and we have more experience explaining these concepts to adults and children. Counselling is a good opportunity for us to model a simple explanation for the caregiver and helping the child reach a good understanding of his/her illness. Having said that, keep in mind that explanations will vary depending on the child’s age and whether the child has been told of his/her HIV status. The following example is one way to explain HIV infection to children. This method should be adapted, depending on the circumstances. Counsellors should utilize the counselling flipchart for guidance on how to explain ARVs to children.

25
How To Say It: Explaining ARVs to Younger Children
ADVISE Our body has many CD4 cells. These are the most important part of our defense system. When HIV enters the body, it uses the CD4 cells to make more HIV. This kills the CD4 cells. When CD4 cells are few, the body becomes weak and a person may become sick. Having lots of CD4 cells will help you to stay healthy. These medicines (ARVs) help to slow down HIV multiplication, keeping CD4 cells strong and many.
 help to slow down HIV multiplication, keeping CD4 cells strong and many.")
26
Case Study– Counselling Juma
ADVISE Juma, a boy of 6 yrs, is HIV positive. Both parents died of AIDS when he was 3 yrs– he was taken for testing by his aunt, who is his primary caregiver. Juma comes to the clinic frequently with recurrent infections. The aunt has not told Juma about his HIV status. Now, the clinician has told Juma’s aunt that he soon needs start ART. He refers her to a counsellor to talk more about ART for children. Role Play: With the aunt in the room, explain to Juma that he needs to start ART. Activity Time: 10 min role play + 10 min discussion = total 20 min Purpose: To practice using the flipchart explaining the start of ART in child-friendly language, to children who have not been disclosed to. Activity Instructions: The facilitator should read the case study from the slide. Ask for three volunteers to role play the scenario and demonstrate using simple language to explain what is happening to Juma. Remind the participants that Juma has not yet been disclosed to about his HIV status and the focus of this role play is on TALKING TO JUMA. [Have the volunteers to use the Paediatric HIV Counselling Flipchart as the rest of the class uses the Observation Tool to see that the key steps and content is covered during the role play. Give volunteers no more than 10 min to perform the role play in front of the group, facilitators should step in and assist when needed. ] When the role play is finished, debrief with these questions: What went well in this session? What counselling skills did you see the counsellor use? What was most challenging for the counsellor? How can we address those challenges?

27
Different Needs ADVISE Children:
Have unique needs; they are not just small adults Are constantly developing; new issues emerge Should be involved through age-appropriate language in their care: tell them the truth Caregivers: Must understand how to give medications to children, including liquid forms Need to know that 100% adherence is important for treatment success

28
Different Needs ADVISE Caregivers need to understand:
When treatment will be started What it means to be “eligible” for ART What side effects to watch for When to bring the child back to the clinic

29
Once the clients understand how ARVs work, they need to know how to take them.
Go to page 12 and let’s review this content.

30
Case Study– Counselling Juma’s Aunt
ADVISE Juma, a boy of 6 yrs, is HIV positive. Both parents died of AIDS when he was 3 yrs– he was taken for testing by his aunt, who is his primary caregiver. Juma comes to the clinic frequently with recurrent infections. The aunt has not told Juma about his HIV status. Now, the clinician has told Juma’s aunt that he soon needs start ART. He refers her to a counsellor to talk more about ART for children. Role Play: What do you need to discuss with Juma’s aunt? Refer to flipchart to answer this question Activity Time: 10 min role play + 10 min discussion = total 20 min Purpose: To practice talking with caregivers about the process of starting ART. Activity Instructions: We are now returning to the case study that we talked about earlier with Juma and his aunt. In the previous activity, we explained to Juma that he will start taking medication to help him feel better. Now, we need to counsel his aunt on other aspects of Juma’s treatment. The case study is on the slide to remind you of Juma’s circumstances. I would like for 3 new volunteers to continue the role play with Juma. The focus of this role play is on explaining the treatment plan to Juma’s aunt using the flipchart as a guide. [Give volunteers no more than 10 min to perform the role play in front of the group, facilitators should step in and assist when needed– note that Juma is in the role play to start, but since he has not been disclosed to, the counsellor should first vacate Juma from the session before talking to the aunt.] When the role play is finished, debrief with these questions: What went well in this session? What counselling skills did you see the counsellor use? What was most challenging for the counsellor? How can we address those challenges?

31
Once they know how to take ARVs, they need to know a bit about side effects. Turn to page 13 and let’s review the content on this page. Although you need to know a bit more about side effects, clients only need to know what is on this page.

32
Case Study Practice ADVISE Form 6 teams— review the side effects chart
For each case study presented, identify the key counseling messages Activity Time: 5 min for instructions + 10 min for each case study = total 35 min Purpose: To practice explaining mild to severe side effects to caregivers– the focus here is on talking to caregivers, not diagnosing side effects. Activity Instructions: You will form six teams (use the same ones as earlier in the course) for this activity. I will read a case study from the slide and show a picture to accompany the case study. Then, each team will try to identify the possible drug causing the side effect and the counselling messages that should be given to the child, caregiver or adolescent. You will have a few minutes to discuss your answer as a team. The team with the best answer will receive 10 points (the facilitators will judge). There are only 3 case studies, so every point counts! Use the worksheet in your participant manual to take notes on this activity. It is especially important in this section to remind counsellors of their role. They should not try to diagnose patients or recommend treatment. For all suspected side effects, adverse events and toxicities, the first recommendation should be to seek guidance from an experienced clinician.
 for this activity. I will read a case study from the slide and show a picture to accompany the case study. Then, each team will try to identify the possible drug causing the side effect and the counselling messages that should be given to the child, caregiver or adolescent. You will have a few minutes to discuss your answer as a team. The team with the best answer will receive 10 points (the facilitators will judge). There are only 3 case studies, so every point counts! Use the worksheet in your participant manual to take notes on this activity. It is especially important in this section to remind counsellors of their role. They should not try to diagnose patients or recommend treatment. For all suspected side effects, adverse events and toxicities, the first recommendation should be to seek guidance from an experienced clinician.")
33
Support Clients to Understand and Anticipate Side Effects
ADVISE ARVs are strong drugs—sometimes people have negative effects when they first start It will take a child’s body about 4-6 weeks to get used to the effects of ARVs If any health problems occur within the first few weeks, it is important to return to the clinic right away Continue taking your drugs unless the clinician tells you to stop taking them You have a role to play in helping children and caregivers to identify serious conditions. Help the patient to understand that side effects are difficult to experience, but are expected. Encourage patients to continue taking ARVs, unless the clinician recommends stopping. Remind clients to return to the clinic right away for an assessment if there are suspected side effects. You will find a chart with common ART side effects and the likely cause in the Participant Manual.

34
Nabatanzi, 7 months ADVISE
Nabatanzi is a 7 month old girl who was started on ART tablets 6 days ago. Her grandmother returns today to see you because Nabatanzi has developed an itchy rash on her neck and back last evening. She has no fever, and the rash has not formed any blisters. Her neighbour, who also has a child with HIV, has told her the rash is a sign that the drugs make the child sicker and asked her to stop them. She is confused. Activity Time: To discuss this case (next 2 slides) 10 min Purpose: To practice explaining mild to severe side effects to caregivers Activity Instructions: Read the slide above, show the picture (next slide) and allow each time to give an answer. After both teams have given answers, show the last slide and announce the winner for that case study.
 10 min. Purpose: To practice explaining mild to severe side effects to caregivers. Activity Instructions: Read the slide above, show the picture (next slide) and allow each time to give an answer. After both teams have given answers, show the last slide and announce the winner for that case study.")
35
What would you tell her grandmother?
This is a mild NVP rash—Nevirapine is the most common cause of skin rash.The rash usually appears in the first 6 weeks of starting treatment. Health workers should also watch for signs of liver problems such as yellow eyes, abdominal pain, vomiting and lethargy. Advice for the grandmother: Refer the child and grandmother to the clinician for examination and treatment Reassure her that while the reaction may be difficult for the child, but it is an expected side effect. Usually, it does not require change in ART Remind her to continue monitoring the child Return to the clinic immediately if the rash gets worse and develops blistering [All side effect photos courtesy of Dr. Israel Kalyesubula] What would you tell her grandmother? 35

36
Mbabazi, 5 years ADVISE Mbabazi is a 5 year old boy who has been on ART for 10 days. His concerned mother brings him to see you because he has developed peeling on his skin His mother says his condition began as a rash all over the body and has steadily gotten worse over the last 2 days She says that he has not been burned Activity Time: To discuss this case (next 2 slides) 10 min Purpose: To practice explaining mild to severe side effects to caregivers Activity Instructions: Read the slide above, show the picture (next slide) and allow each time to give an answer. After both teams have given answers, show the last slide and announce the winner for that case study.
 10 min. Purpose: To practice explaining mild to severe side effects to caregivers. Activity Instructions: Read the slide above, show the picture (next slide) and allow each time to give an answer. After both teams have given answers, show the last slide and announce the winner for that case study.")
37
What would you tell his mother?
This is Steven Johnson Syndrome, a severe reaction affecting the skin and the mucous membranes. It can be caused by any drug, even Septrin. The clinician may recommend temporarily stopping ART, then restarting when the rash has healed. Guidance for his mother: This is a very serious side effect See the clinician immediately for examination and recommendations Ensure the child has adequate hydration & nutrition Watch the child closely– if any sign of worsening, bring the child back to the clinic right away What would you tell his mother?

38
Acayo, 4 years ADVISE Acayo is a 4 year old child who has been on ART for 4 months Her mother brought her for a routine monitoring visit. You notice that she tires easily when she runs around your office. You also notice her hands and inner eyes are pale Activity Time: To discuss this case (next 2 slides) 10 min Purpose: To practice explaining mild to severe side effects to caregivers Activity Instructions: Read the slide above, show the picture (next slide) and allow each time to give an answer. After both teams have given answers, show the last slide and announce the winner for that case study.
 10 min. Purpose: To practice explaining mild to severe side effects to caregivers. Activity Instructions: Read the slide above, show the picture (next slide) and allow each time to give an answer. After both teams have given answers, show the last slide and announce the winner for that case study.")
39
What would you tell her mother?
This is AZT induced anaemia, which can cause severe anaemia as a side effect. Anaemia can also be caused by malaria or other infectious for causes– only tests can determine the cause.Health workers should watch for signs of severe disease, including fast heart beat and swollen feet. Advice for her mother: Excessive tiredness and pale hands/eyes can be a sign of a serious iron deficiency called anaemia See a clinician immediately for an assessment and lab work Although you need to be aware about the more serious problems that some people have with the medication, usually you will just refer the client to a clinician. All a client needs to know is what is on page 13. Let’s review the content on this page. What would you tell her mother?

40
Determining Readiness: AGREE
Caregiver & child should agree on a plan for how to: Achieve excellent adherence Keep regular clinic appointments Identify and seek treatment for possible side effects Secure needed support for the child’s treatment from family, school, community

41
How to Say It: Adherence Planning With Children
AGREE These medicines must be taken EVERY DAY, just as the directions say What happens if you forget to take your medicine? HIV can multiply and your CD4 cells can go very low. Do you think you can take your medicine every day? How can you be sure to remember? Who will help you? Mon Tues Wed Thurs Fri Sat Sun

42
Adherence Planning includes Disclosure
ASSIST Probe disclosure with the caregiver—encourage discussions with the child starting at 5 years old Ideally, children should be fully disclosed by 10 years. Disclosure can take place little by little.

43
[Since this page was reviewed in the first module, so it is not necessary to review all the content, but remind them that the page is there to help them under the positive living section.]
![[Since this page was reviewed in the first module, so it is not necessary to review all the content, but remind them that the page is there to help them under the positive living section.]](http://slideplayer.com/slide/3767893/13/images/43/%5BSince+this+page+was+reviewed+in+the+first+module%2C+so+it+is+not+necessary+to+review+all+the+content%2C+but+remind+them+that+the+page+is+there+to+help+them+under+the+positive+living+section.%5D.jpg "[Since this page was reviewed in the first module, so it is not necessary to review all the content, but remind them that the page is there to help them under the positive living section.]")
44
[Have the participants turn to page 14 and have volunteers read each part.]
This page will help you take your client through adherence planning.
![[Have the participants turn to page 14 and have volunteers read each part.]](http://slideplayer.com/slide/3767893/13/images/44/%5BHave+the+participants+turn+to+page+14+and+have+volunteers+read+each+part.%5D.jpg "This page will help you take your client through adherence planning.")
45
Closing: ARRANGE ARRANGE
If the caregiver and child are ready, arrange for them to visit the clinician on the same day for ARVs to be prescribed Schedule follow-up counselling sessions, which should be on the same days as clinical follow-up Document the counselling session on the patient’s HIV Care/ART card (blue)
")
46
[Have the participants turn to page 15. Go through each section briefly.]
What should you do if children refuses to take medicine? This provides support for adherence. When will your child start on ARVs? This provides support for the caregiver to understand everything that should be in place. Talking with caregivers: These are the questions to ask in order to ensure that adherence planning is addressed at every session. At the bottom is a section that lets the counsellor know what needs to be in place. Remember that once the client is ready enough, they should start on the ARVs but continue to be counselled for good adherence for as many visits as necessary. This is the last page in Topic 2– the green section. Go back to page 10 to see how the sections relate to each other. Based on feedback from counsellors such as you, the tool was designed to be flexible. Sometimes you will go through every subtopic in the green section. Sometimes you will take a client straight to one subtopic such as the ‘Planning for adherence’ and then straight to the ‘Closing for adherence’. Other times you might go to one or two sub topics and then to the ’Closing for adherence’. The goal is to make sure that you are getting the right information to the client when they are best ready to hear it and act on it. You are the best judge of that.
![[Have the participants turn to page 15. Go through each section briefly.]](http://slideplayer.com/slide/3767893/13/images/46/%5BHave+the+participants+turn+to+page+15.+Go+through+each+section+briefly.%5D.jpg "What should you do if children refuses to take medicine This provides support for adherence. When will your child start on ARVs This provides support for the caregiver to understand everything that should be in place. Talking with caregivers: These are the questions to ask in order to ensure that adherence planning is addressed at every session. At the bottom is a section that lets the counsellor know what needs to be in place. Remember that once the client is ready enough, they should start on the ARVs but continue to be counselled for good adherence for as many visits as necessary. This is the last page in Topic 2– the green section. Go back to page 10 to see how the sections relate to each other. Based on feedback from counsellors such as you, the tool was designed to be flexible. Sometimes you will go through every subtopic in the green section. Sometimes you will take a client straight to one subtopic such as the ‘Planning for adherence’ and then straight to the ‘Closing for adherence’. Other times you might go to one or two sub topics and then to the ’Closing for adherence’. The goal is to make sure that you are getting the right information to the client when they are best ready to hear it and act on it. You are the best judge of that.")
47
Reviewing the Process Review the Counselling Observation Tool– Preparing for the Start of ART Since we are at the end of the unit on starting ART, ensure that all of the steps have been discussed.

48
Counselling for the Start of ART
What are the benefits of good adherence? What challenges do children commonly face with adherence? Adolescents? What are some of the symptoms of serious side effects that require the client to be referred to a clinician?

49
Module IV: Preparing for ART Unit 3: Supportive Adherence Counselling
By the end of this unit, participants should be able to: Explain 3 methods for measuring adherence for children and adolescents Identify reasons why adherence might become more challenging over time Explain strategies for helping families address adherence challenges Unit Time:1 hour

50
Brainstorm: Measuring Adherence
ASSESS How will we know if a child or adolescent misses doses of ART? How do we measure adherence for adults? Is it the same for children? Activity Time: 5 min discussing in pairs + 5 min as large group. Total: 10 min Purpose: To help trainees identify several ways to measure adherence in children Activity Instructions: Discuss the questions on the slide. Flipchart responses. Remind participants that it is particularly important to ask caregivers about how they are giving medicine to children. There are some strategies that work better than others and caregivers need support to resolve adherence challenges.

51
Assessing Adherence ASSESS Adherence from pill counts:
May be announced or unannounced (home visit) Adherence from self report: Ask the child and caregiver about missed doses Assessing missed clinic appointments Checking pharmacy records to determine if clients have picked up their drugs
 Adherence from self report: Ask the child and caregiver about missed doses. Assessing missed clinic appointments. Checking pharmacy records to determine if clients have picked up their drugs.")
52
Calculating Adherence: John
ASSESS John is a 1 year old child. His last clinic visit which was 28 days ago. He was given 60 tablets of the drug. He takes 1 tablet twice daily. He returns today and has a balance of 8 tablets. Calculate his adherence. Activity Time: 10 min Purpose: To practice calculating adherence using pill counts Activity Instructions: Now, for this case study, work in groups of 4 people– for the sake of time, join with those sitting next to you. Review the case study and calculate adherence. You will have 5 minutes to work. Use the worksheet in your participant manual. [after 5 minutes have passed, call time] Now, let’s see if we have all come up with the same answer. [Ask each group to read off their % adherence to see if there is consistency. If any group has arrived at the wrong answer, go over the formula below] Answer: Adherence= No of tablets taken ( No of tablets given- balance of tablets) X100 No of Tablets patient was supposed to take = (60-8) x100 56 (28 daysX2 tables per day) =52/56X100=92.8% (fair adherence) This formula is found on the blue HIV Care/ART card.
 X100. No of Tablets patient was supposed to take. = (60-8) x (28 daysX2 tables per day) =52/56X100=92.8% (fair adherence) This formula is found on the blue HIV Care/ART card.")
53
Supportive Adherence Counselling
ASSESS Regular discussions with child, caregiver on any problems faced taking medication— school, peer pressure, side effects etc. Open-door policy for child to see counsellor May need to offer specific strategies for encouraging child to take meds Recognize that the child may go through periods where it is harder to adhere

54
Addressing Missed Doses
ADVISE If a child misses one dose, give the next dose as normal If the child vomits before 30 minutes, give the full dose again If the child vomits after 30 minutes, do not give the dose again AGREE Develop a plan to address adherence challenges Emphasize to the child and caregiver that they should continue to take ARVs despite feeling unwell See the clinician for an evaluation of symptoms

55
Children and Adherence
ASSIST Support identification of strategies to overcome adherence challenges What do you think are the most common challenges that children and caregivers face with ART adherence? Child factors Caregiver factors Medication factors Provider factors OH NO! That was horrible!!! As a large group, brainstorm challenges to adherence and record the responses on a flipchart. Ensure that the following are mentioned: Child factors: age, temperament, experiences with medication, ability to swallow pills Medication factors: taste, frequency of dosing, side effects, food requirements Caregiver factors: lack of understanding, resistance to treatment, literacy, ill health, stigma, disclosure issues Provider factors: relationship with child, cultural sensitivity, provider stress/burnout, communication skills, trust

56
Closing: ASSIST and ARRANGE
Ask about sources of community support, suggest involvement in support groups Review disclosure plan and probe barriers ARRANGE Referrals Follow-up visits to the counsellor and/or clinician Document the session on the HIV Care/ART card

57
If your client has already been on ARVs for a while so that they know about ARVs, how they work, how to take them and what side effects are, then you are likely only to come to the last subtopic to probe for any adherence issues that are emerging and the ‘Closing’.

58
Reviewing the Process Review the Counselling Observation Tool– Starting and Supportive Adherence Counselling Since we are at the end of the module, ensure that all of the steps have been discussed.

59
Macdot Video Clip Adolescent Adherence Discussion:
What questions does the counsellor ask to better understand Macdot’s challenges with adherence? How does she probe adherence in a non-judgmental way? What were the issues that Macdot struggled with? How did the counsellor support Macdot to improve his adherence? Video Duration: 10 min + 5 min discussion = total 15 min Purpose: To help trainees understand how to counsel on adherence by observing a strong counsellor in action In this video, we meet Macdot, an adolescent who is currently taking ART. The counsellor discusses adherence issues with him and explores possible barriers. A few things to keep in mind when counselling adolescents: Takes time to build trust in counsellor and settle into counselling process May feel confused and fear rejection by others Less likely to return to clinic when problems arise May cope with stress through alcohol/drug abuse Adolescents need: Positive responses from adults A balance between structure & freedom to express feelings Communication with warmth, genuineness, empathy and honesty

60
Discussing Adherence– Case Studies
In your 6 groups, read the case studies (Vincent, Tom, Mary) Discuss the following: What are the barriers to adherence? How can we promote adherence in each case? What would you emphasize to the child? To the caregiver? Activity Time: 10 min group work + (5 min for 3 groups) + (2 min for 3 groups) for plenary. Total: 30 min Purpose: To practice identifying barriers to adherence and identify key messages for children and caregivers Activity Instructions: For this activity, you will form 6 groups (the ones we formed on the first day of this course) and each will work on one case study. You will have 10 minutes to read and discuss the case that has been assigned to you. Remember to use your tools: Lukia’s story, Paediatric HIV Flipchart, Caregiver Booklet, Adolescent Booklet. Use the case studies and worksheet in your participant manual. Group 1 and 2-- Vincent, a 10 year old boy, has been doing well with his medication until their father dies. Now he is living with his grandmother who does not believe that ART works. Her church tells her that HIV can be cured through prayer and that the tables are the cause of the boy’s illness (and, in fact, doctors are becoming rich by prescribing them). Discuss the implications for adherence and how you would deal with them. Group 3 and 4-- Tom is 14 years old. He is a bright student attending a well known boarding school. He has been on ARVs for 6 months. He waits to take his medication when no one else is looking, not even his best friend. Because of this, he sometimes forgets to take his pills. Discuss how you would deal with this issue and the possible consequences for adherence. Group 4 and 5-- Mary is 2 years old, her mother is very unwell and therefore Mary is cared for by many ‘aunties’. She is on ARVs in liquid form which is bitter to taste. She spits out the medication and is refusing to take it anymore. Discuss the adherence issues of this case and how you would deal with them. [After the groups have finished working, ask each group to read their case aloud and discuss their answers to the questions above. The second group that worked on each case study should listen carefully to the first group’s presentation and only add on or challenge something that the other group said. The first group for each case study should have only 5 minutes in plenary and the second group should take about 2 minutes to add or critique. Then, move to the second case study.]
 Discuss the following: What are the barriers to adherence How can we promote adherence in each case What would you emphasize to the child To the caregiver Activity Time: 10 min group work + (5 min for 3 groups) + (2 min for 3 groups) for plenary. Total: 30 min. Purpose: To practice identifying barriers to adherence and identify key messages for children and caregivers. Activity Instructions: For this activity, you will form 6 groups (the ones we formed on the first day of this course) and each will work on one case study. You will have 10 minutes to read and discuss the case that has been assigned to you. Remember to use your tools: Lukia’s story, Paediatric HIV Flipchart, Caregiver Booklet, Adolescent Booklet. Use the case studies and worksheet in your participant manual. Group 1 and 2-- Vincent, a 10 year old boy, has been doing well with his medication until their father dies. Now he is living with his grandmother who does not believe that ART works. Her church tells her that HIV can be cured through prayer and that the tables are the cause of the boy’s illness (and, in fact, doctors are becoming rich by prescribing them). Discuss the implications for adherence and how you would deal with them. Group 3 and 4-- Tom is 14 years old. He is a bright student attending a well known boarding school. He has been on ARVs for 6 months. He waits to take his medication when no one else is looking, not even his best friend. Because of this, he sometimes forgets to take his pills. Discuss how you would deal with this issue and the possible consequences for adherence. Group 4 and 5-- Mary is 2 years old, her mother is very unwell and therefore Mary is cared for by many ‘aunties’. She is on ARVs in liquid form which is bitter to taste. She spits out the medication and is refusing to take it anymore. Discuss the adherence issues of this case and how you would deal with them. [After the groups have finished working, ask each group to read their case aloud and discuss their answers to the questions above. The second group that worked on each case study should listen carefully to the first group’s presentation and only add on or challenge something that the other group said. The first group for each case study should have only 5 minutes in plenary and the second group should take about 2 minutes to add or critique. Then, move to the second case study.]")
61
Supporting Adherence What are 3 methods for measuring adherence in children and adolescents? Why might adherence become more challenging over time? How can counsellors encourage families to better support ART adherence? [After reflecting briefly on the questions on the slide, which are the end of unit questions, refer back to the module questions that you wrote on flipchart and hung up. Give participants a chance to think about the answers and even answer out loud if you have time. Then proceed to the next three slides which are the answers to the questions.]

62
Key Messages from this Module
Eligibility criteria for starting ART varies by age. All HIV+ children under 2 years start ARVs right away. Readiness criteria includes whether or not the client has an adherence plan and the support mechanism to adhere. Disclosure is important for good adherence, since children are more cooperative if they understand their situations.

63
Key Messages (2) Counsellors need to screen for side effects and refer patients to the clinician because adherence might be affected if clients feel unwell. When clients are on ARVs they need ongoing counselling to support their treatment and solve problems that arise over time.

Similar presentations



>")







 1IMCI for athens.>")







