Download presentation
Presentation is loading. Please wait.

1
PRE-CONFERENCE WORKSHOP PPRNet 101

2
introductions Who you are Why you are here What you hope to learn

3
Workshop Goals To (begin to) answer the question: “How can I maximize the benefit of PPRNet in my practice?” Introduce (or reintroduce) PPRNet and its mission Provide an overview of PPRNet reports Share examples of how practices use PPRNet reports to achieve recognition and/or incentives Allow time for participants to use reports and network with one another
 PPRNet and its mission. Provide an overview of PPRNet reports. Share examples of how practices use PPRNet reports to achieve recognition and/or incentives. Allow time for participants to use reports and network with one another.")
4
agenda 1:00pm-1:15pm Introductions Vanessa Congdon Andrea Wessell
What is PPRNet? 1:30pm-2:00pm PPRNet Performance Reports and FAQs 2:00pm-2:30pm Using PPRNet Tools for Recognition and Incentive Programs 2:30pm-2:45pm Break 2:45pm-3:00pm Recognition/Incentive Programs, continued 3:00pm-3:15pm PPRNet Top 10 List for Quality Improvement 3:15pm-4:00pm Open Session Demonstrations, Follow-up Discussions All Participants

5
Revise agenda? 1:00pm-1:15pm Introductions Vanessa Congdon
Andrea Wessell 1:15pm-1:30pm What is PPRNet? 1:30pm-2:00pm PPRNet Performance Reports and FAQs 2:00pm-2:30pm Using PPRNet Tools for Recognition and Incentive Programs 2:30pm-2:45pm Break 2:45pm-3:00pm Recognition/Incentive Programs, continued 3:00pm-3:15pm PPRNet Top 10 List for Quality Improvement 3:15pm-4:00pm Open Session Demonstrations, Follow-up Discussions All Participants

6
What is pprnet? “A practice-based learning and research organization designed to improve health care in its member practices and elsewhere in the United States.”

7
What is pprnet? Primary (care) Practices Research Network
A virtual network of primary care practice teams and researchers that aims to: Turn EHR data into actionable information for clinicians and practice staff Empirically test theoretically sound primary care quality improvement interventions Disseminate interventions that improve primary health care

8
“Blur the distinction between quality improvement and research”
PPRNet Aims to… “Blur the distinction between quality improvement and research” 3 aims

9
PPRNet: Primary Care Practice-Based Research and learning Network

10
PPRNet Agency for Healthcare Research and Quality Center for Primary Care Practice-Based Research and Learning Answer questions relevant to practice Disseminate findings

11
Pprnet research Primary Care-Relevant Questions
“Preventive Services Delivery in Patients With Chronic Ilnesses: Parallel Opportunities Rather Than Competing Obligations” “Learning from Primary Care Meaningful Use Exemplars” Translating Research into Practice (TRIP) Interventions Impact studied across a variety of clinical areas Prevention, chronic disease management, acute care and medication safety A-TRIP, C-TRIP, SO-TRIP, MS-TRIP, AM-TRIP, CKD-TRIP…
 Interventions. Impact studied across a variety of clinical areas. Prevention, chronic disease management, acute care and medication safety. A-TRIP, C-TRIP, SO-TRIP, MS-TRIP, AM-TRIP, CKD-TRIP…")
12
Practice spotlight: NEW London Family Medicine

13
Disseminating “lessons learned”
Ongoing PPRNet Activities Annual meetings Monthly webinars Listserv Social media Publications Presentations

14
PPRNET PERFORMANCE REPORTS
Patient & Provider- Level Report Practice-Level Performance Report

15
Clinical Practice Quality Measures
MEASURE CONDITION # Diabetes Mellitus 12 Cardiovascular Disease 17 Women’s Health Care 2 Cancer Screening 3 Immunizations 8 Mental Health & Substance Abuse 6 Respiratory Disease 4 Medication Safety 15 TOTAL: 67

16
Practice Performance Report
67 Quality Indicators 3 Summary Measures SPC Methodology Time trends – Monthly over 2 years Comparison with PPRNet benchmark (ABC) Comparison with national benchmarks (when available)
 Comparison with national benchmarks (when available)")
17
Patient-Level Report (PLR)
Excel Spreadsheet with 78 tabs: PPRNet Switchboard Practice Performance on Individual Measures Provider Performance on Individual Measures Patient Registry PPRNet Measure Groupings (8 tabs) Patient Lists of those not meeting criteria for each of 67 Individual Measures Same indicator criteria as practice report All “active” patients ≥ 3 months age
 Patient Lists of those not meeting criteria for each of 67 Individual Measures. Same indicator criteria as practice report. All active patients ≥ 3 months age.")
18
PPRNet Switchboard

19
PRACTICE PERFORMANCE ON Individual Measures

20
Provider Performance on Individual Measures

21
Patient Registry

22
CMS MU CQM

23
CMS ACO CQM

24
USPSTF Recommendations (Grade A and B)
")
25
CDC Advisory Committee on Immunization Practices Recommendations

26
NIAAA Alcohol Screening and Intervention Recommendations

27
CDC Get Smart Treatment Guidelines for URI’s

28
CMS PQRS CQM Groupings

29
PQRS DM TAB All Pts with DM

30
PQRS DM LIST

31
ACC/AHA Cholesterol Guidelines for ASCVD Risk Reduction

32
ACC/AHA Cholesterol Guidelines for ASCVD Risk Reduction Hierarchical Statin Benefit Groups
ADULTS >=21 years old Diagnosis of ASCVD (CHD or Atherosclerosis) Highest LDL-C >=190 mg/dL Diagnosis of Diabetes Mellitus; age yr Estimated 10-yr ASCVD Risk >=7.5% age yrs
 Highest LDL-C >=190 mg/dL. Diagnosis of Diabetes Mellitus; age yr. Estimated 10-yr ASCVD Risk >=7.5% age yrs.")
33
ACC/AHA Cholesterol Guidelines for ASCVD Risk Reduction Estimated 10-yr ASCVD Risk Equations
Age Sex Race Total Cholesterol HDL-CSystolic BP Hypertension Dx Diabetes Mellitus Dx Smoking Status Systolic BP Hypertension Dx Diabetes Mellitus Dx Smoking Status

34
Q: What data are used for calculating performance?

35
A (part 1): Report guide details data source for each measure
Highlight other things in appendix

36
Identifiers (ie, CMS id, NQF # or PQRS id) cited in reports
A (part 2): PPRNet measures are now aligned with Meaningful Use Clinical Quality Measures Applies to some new measures (ie, eye exam in patients with diabetes) and new categories (ie, ACO CQMs) Identifiers (ie, CMS id, NQF # or PQRS id) cited in reports
: PPRNet measures are now aligned with Meaningful Use Clinical Quality Measures. Applies to some new measures (ie, eye exam in patients with diabetes) and new categories (ie, ACO CQMs) Identifiers (ie, CMS id, NQF # or PQRS id) cited in reports.")
37
How do I UPLOAD MY DATA EXRACT AND access my reports?

38
New DATA Extract PP users will be migrating to a new extract process for October reports McKesson support for prxtract ends in October The MUSC OCIO has worked with us to develop a “vendor neutral” extraction process New reports will include patient identifiers!

39
Summary: PPRNet Reports in Practice
Evaluate performance over time Identify patients overdue for care Engage, motivate, and incentivize practice team Demonstrate quality of care for quality recognition and incentive programs

40
questions To (begin to) answer the question: “How can I maximize the benefit of PPRNet in my practice?” Introduce (or reintroduce) PPRNet and its mission Provide an overview of PPRNet reports Share examples of how practices use PPRNet reports to achieve recognition and/or incentives Allow time for participants to use reports and network with one another
 PPRNet and its mission. Provide an overview of PPRNet reports. Share examples of how practices use PPRNet reports to achieve recognition and/or incentives. Allow time for participants to use reports and network with one another.")
41
USING REPORTS FOR RECOGNITION AND INCENTIVE PROGRAMS

42
Recognition and incentive programs
PPRNet practices use reports for a variety of local and national quality recognition and pay for performance programs During this session, we will highlight: NCQA Patient-Centered Medical Home CMS Physician Quality Reporting System

43
Pprnet 101: glossary NCQA PCMH CMS PQRS ABFM PLR SQUID
What is your experience with these recognition programs? How has your practice benefited from recognition?

44
NCQA PCMH 2014 Standards Published in March 2014 (must be used by March 2015) Revisions to align with MU Stage 2, reflect PCMH evidence base and from stakeholder input Major edits in the areas of: Care management of high-need populations Team-based care Focus on triple aim domains (patient experience, cost, clinical quality) Sustaining transformation Integration of behavioral health NCQA = national co for quality assurance
 Sustaining transformation. Integration of behavioral health. NCQA = national co for quality assurance.")
45
NCQA PCMH 2014 Content and Scoring (6 standards/27 elements)
1: Enhance Access and Continuity *Patient-Centered Appointment Access 24/7 Access to Clinical Advice Electronic Access Pts 4.5 3.5 2 10 2: Team-Based Care Continuity Medical Home Responsibilities Culturally and Linguistically Appropriate Services (CLAS) *The Practice Team 3 2.5 4 12 3: Population Health Management Patient Information Clinical Data Comprehensive Health Assessment *Use Data for Population Management Implement Evidence-Based Decision- Support 5 20 4: Plan and Manage Care Identify Patients for Care Management *Care Planning and Self-Care Support Medication Management Use Electronic Prescribing Support Self-Care and Shared Decision-Making Pts 4 3 5 20 5: Track and Coordinate Care Test Tracking and Follow-Up *Referral Tracking and Follow-Up Coordinate Care Transitions 6 18 6: Measure and Improve Performance Measure Clinical Quality Performance Measure Resource Use and Care Coordination Measure Patient/Family Experience *Implement Continuous Quality Improvement Demonstrate Continuous Quality Improvement Report Performance Use Certified EHR Technology Practice Team is new Care Management was must pass – now combined with “care planning and self-care support” All other must pass are the same Same total points Scoring Levels Level 1: points. Level 2: points. Level 3: points. *Must Pass Elements 45
 *The Practice Team : Population Health Management. Patient Information. Clinical Data. Comprehensive Health Assessment. *Use Data for Population Management. Implement Evidence-Based Decision- Support : Plan and Manage Care. Identify Patients for Care Management. *Care Planning and Self-Care Support. Medication Management. Use Electronic Prescribing. Support Self-Care and Shared Decision-Making. Pts : Track and Coordinate Care. Test Tracking and Follow-Up. *Referral Tracking and Follow-Up. Coordinate Care Transitions : Measure and Improve Performance. Measure Clinical Quality Performance. Measure Resource Use and Care Coordination. Measure Patient/Family Experience. *Implement Continuous Quality Improvement. Demonstrate Continuous Quality Improvement. Report Performance. Use Certified EHR Technology. Practice Team is new. Care Management was must pass – now combined with care planning and self-care support All other must pass are the same. Same total points. Scoring Levels. Level 1: points. Level 2: points. Level 3: points. *Must Pass Elements. 45.")
46
PCMH 2: Team-based care Element 2D: The Practice Team
The practice uses a team to provide a range of patient care services by: Defining roles for clinical and nonclinical team members Identifying practice organizational structure and staff leading and sustaining team based care Having regular patient care team meetings or a structured communication process focused on individual patient care* Using standing orders for services Training and assigning members of the care team to coordinate care for individual patients (continued) 2 and 8 are new 3 is critical factor Other factors were a part of 2011 Standard 1 “Enhance Access and Continuity” Documentation for Factor 3 – description of communication and at least 3 examples Factor 2: The practice delineates responsibilities for sustaining team-based care, and specifies how care teams align to provide patient-centered care. Specific team units may focus on providing care coordination across and beyond the practice (factor 5). An organizational chart may be used to illustrate how a care team fits in the practice. 8 (regular team mtngs) Factor 8: Description of staff communication processes and sample
 2 and 8 are new. 3 is critical factor. Other factors were a part of 2011 Standard 1 Enhance Access and Continuity Documentation for Factor 3 – description of communication and at least 3 examples. Factor 2: The practice delineates responsibilities for sustaining team-based care, and specifies how care teams align to provide patient-centered care. Specific team units may focus on providing care coordination across and beyond the practice (factor 5). An organizational chart may be used to illustrate how a care team fits in the practice. 8 (regular team mtngs) Factor 8: Description of staff communication processes and sample.")
47
PCMH 2: Team-based care Training and assigning members of the care team to support patients/families/caregivers in self-management, self-efficacy and behavior change Training and assigning members of the care team to manage the patient population Holding regular team meetings addressing practice functioning Involving care team staff in the practice’s performance evaluation and quality improvement activities Involving patients/families/caregivers in quality improvement activities or on the practice’s advisory council 2 and 8 are new 3 is critical factor Other factors were a part of 2011 Standard 1 “Enhance Access and Continuity” Documentation for Factor 3 – description of communication and at least 3 examples Factor 2: The practice delineates responsibilities for sustaining team-based care, and specifies how care teams align to provide patient-centered care. Specific team units may focus on providing care coordination across and beyond the practice (factor 5). An organizational chart may be used to illustrate how a care team fits in the practice. 8 (regular team mtngs) Factor 8: Description of staff communication processes and sample
. An organizational chart may be used to illustrate how a care team fits in the practice. 8 (regular team mtngs) Factor 8: Description of staff communication processes and sample.")
48
PPRNet Tools PPRNet Improvement Model as background
Build team meeting agendas based on PPRNet reports, webinars or network meeting topics Use plans for Element 3D (Population Management) or 4A (Care Management and Support) to document responsibilities for team-based care
 or 4A (Care Management and Support) to document responsibilities for team-based care.")
49
PCMH 3: Plan and Manage Care
Element 3D: Use Data for Population Management (MUST PASS) At least two different preventive care services At least two different immunizations At least three different chronic or acute care services Patients not recently seen by the practice Medication monitoring or alert Documentation: Factors 1-5: Lists or summary reports of patients who need services within past 12 mo. (Health plan data okay if 75% of patient population) and Factors 1-5: Documented process demonstrating staff responsibilities and desired timing of reminders and materials showing how patients were notified for each service. The practice must perform these functions at least annually and make documentation of each reminder available to NCQA upon request.
 At least two different preventive care services. At least two different immunizations. At least three different chronic or acute care services. Patients not recently seen by the practice. Medication monitoring or alert. Documentation: Factors 1-5: Lists or summary reports of patients who need services within past 12 mo. (Health plan data okay if 75% of patient population) and. Factors 1-5: Documented process demonstrating staff responsibilities and desired timing of reminders and materials showing how patients were notified for each service. The practice must perform these functions at least annually and make documentation of each reminder available to NCQA upon request.")
50
PCMH 3: PLAN AND MANAGE CARE
PPRNet Patient-level Report (PLR) includes lists of patients: With specific diagnoses Needing preventive services, including immunizations Requiring clinician review or action Taking specific medications Factor 1- Pts who need preventive screening or immunizations (at least 3 different immunizations or screenings) Factor 2-Pts who need acute or chronic care services (at least 3 different services) Factor 3-Pts who have not had recent appointment (practice may use own criteria) Factor 4-Pts on specific medications
 includes lists of patients: With specific diagnoses. Needing preventive services, including immunizations. Requiring clinician review. or action. Taking specific medications. Factor 1- Pts who need preventive screening or immunizations (at least 3 different immunizations or screenings) Factor 2-Pts who need acute or chronic care services (at least 3 different services) Factor 3-Pts who have not had recent appointment (practice may use own criteria) Factor 4-Pts on specific medications.")
51
PPRNet Tools Add narrative describing who does what
Save examples of letters or chart flags Pick 2-3 areas to work on every quarter to “complete” all in 12 months

52
PCMH 4: Care Management and Support
Element 4A: Identify Patients for Care Management Systematic process and criteria for identifying patients who may benefit from care management The process includes consideration of the following: 1. Behavioral health conditions 2. High cost/high utilization 3. Poorly controlled or complex conditions 4. Social determinants of health 5. Referrals by outside organizations (e.g., insurers, health system, ACO), practice staff or patient/family/caregiver 6. The practice monitors the percentage of the total patient population identified through its process and criteria* Factors 1-6 are new, previously you could define it on your own. Documentation Factors 1-5: Criteria and process for identifying patients. Factor 6: Report showing number and percentage of patients identified as likely to benefit from care management through one or any combination of the other five factors or other criteria determined by the practice. Must meet #6 to get any points
, practice staff or patient/family/caregiver. 6. The practice monitors the percentage of the total patient population identified through its process and criteria* Factors 1-6 are new, previously you could define it on your own. Documentation. Factors 1-5: Criteria and process for identifying patients. Factor 6: Report showing number and percentage of patients identified as likely to benefit from care management through one or any combination of the other five factors or other criteria determined by the practice. Must meet #6 to get any points.")
53
PCMH 4: Care Management and Support
Performance Reports Use Summary Quality Index (SQUID) as marker of “poorly controlled or complex conditions” Define your practice’s target SQUID Patients that fall below this = patients that may benefit from care management Use a screen shot of PLR to document the number of patients that fall into this category Track this number (and % of total patients) Design and implement care management plan for Element 4B (MUST PASS)
 as marker of poorly controlled or complex conditions Define your practice’s target SQUID. Patients that fall below this = patients that may benefit from care management. Use a screen shot of PLR to document the number of patients that fall into this category. Track this number (and % of total patients) Design and implement care management plan for Element 4B (MUST PASS)")
54
PCMH 6: measure and improve performance
“The practice uses performance data to identify opportunities for improvement and acts to improve clinical quality, efficiency and patient experience.” Measure Clinical Quality Performance Measure Resource Use and Care Coordination Measure Patient/Family Experience *Implement Continuous Quality Improvement Demonstrate Continuous Quality Improvement Report Performance Use Certified EHR Technology

55
PCMH 6: measure and improve performance
Element 6A: Measure Clinical Quality Performance At least annually, the practice measures or receives data on: At least 2 immunization measures At least 2 other preventive care measures At least 3 chronic or acute care clinical measures Performance data stratified for vulnerable populations (to assess disparities in care) Vulnerable populations are “those who are made vulnerable by their financial circumstances or place of residence, health, age, personal characteristics, functional or developmental status, ability to communicate effectively, and presence of chronic illness or disability,” (AHRQ) and include people with multiple comorbid conditions or who are at high risk for frequent hospitalization or ER visits.
 Vulnerable populations are those who are made vulnerable by their financial circumstances or place of residence, health, age, personal characteristics, functional or developmental status, ability to communicate effectively, and presence of chronic illness or disability, (AHRQ) and include people with multiple comorbid conditions or who are at high risk for frequent hospitalization or ER visits.")
56
PCMH 6: measure and improve performance
Element 6D: Implement Continuous Quality Improvement (MUST PASS) Ongoing QI process that includes regular review of performance data and evaluation of performance against goals or benchmarks to: Set goals and analyze at least 3 CQM from A Act to improve at least 3 CQM from A Set goals and analyze at least 1 measure from B Act to improve at least one measure from B Set goals/analyze at least 1 patient experience measure from C Act to improve at least one patient experience measure from C Set goals and address at least one identified disparity in care/service for identified vulnerable populations Vulnerable populations are “those who are made vulnerable by their financial circumstances or place of residence, health, age, personal characteristics, functional or developmental status, ability to communicate effectively, and presence of chronic illness or disability,” (AHRQ) and include people with multiple comorbid conditions or who are at high risk for frequent hospitalization or ER visits.
 Ongoing QI process that includes regular review of performance data and evaluation of performance against goals or benchmarks to: Set goals and analyze at least 3 CQM from A. Act to improve at least 3 CQM from A. Set goals and analyze at least 1 measure from B. Act to improve at least one measure from B. Set goals/analyze at least 1 patient experience measure from C. Act to improve at least one patient experience measure from C. Set goals and address at least one identified disparity in care/service for identified vulnerable populations. Vulnerable populations are those who are made vulnerable by their financial circumstances or place of residence, health, age, personal characteristics, functional or developmental status, ability to communicate effectively, and presence of chronic illness or disability, (AHRQ) and include people with multiple comorbid conditions or who are at high risk for frequent hospitalization or ER visits.")
57
PCMH 6: measure and improve performance
Element 6E: Demonstrate Continuous Quality Improvement Ongoing effort of assessing, improving and reassessing Emphasis on ongoing QI to demonstrate that practice has gone beyond setting goals Measuring effectiveness of actions it takes to improve measures selected in D Achieving improved performance on at least 2 CQM Achieving improved performance on one utilization or care coordination measure Achieving improved performance on at least one patient experience measure

58
PCMH 6: measure and improve performance
Element 6F: Report Performance Results reflect care provided to all patients in the practice, not only patients covered by a specific payer and shares: Individual clinician performance results with the practice Practice-level performance results with the practice Individual clinician or practice-level performance results publicly Individual clinician or practice-level performance results with patients

59
PCMH 6: measure and improve performance
Use PPRNet reports to show how your practice measures clinical quality performance, implements QI, demonstrates QI and reports performance across: Clinical processes Clinical outcomes

60
More on PPRNet research and PCMH saturday…
Engaging patients in upcoming and planned projects as part of the “Practice Team” element

61
Other pcmh examples What other ways have you applied PPRNet tools to PCMH work? How has your practice benefited from PCMH recognition?

62
BREAK

63
CMS Physician Quality Reporting System (PQRS)
“A reporting program that uses a combination of incentive payments and payment adjustments to promote reporting of quality information by eligible professionals (EPs).” Evolved from the Physician Quality Reporting Initiative (PQRI) Aims to reach 50% of EPs by 2015 Regulations made permanent in 2008
. Evolved from the Physician Quality Reporting Initiative (PQRI) Aims to reach 50% of EPs by Regulations made permanent in")
64
PQRS Is this “old news”? Have you used PPRNet reports for this program in the past?

65
PQRS incentives/adjustments
2014: % of total estimated allowed charges for Medicare Part B Physician Fee Schedule during reporting period 2015: % based on 2013 participation 2016-: -2% based on 2014 participation Additional +0.5% incentive with Maintenance of Certification Program participation Regulations made permanent in 2008 2009 avg payment (2% incentive) ~$1100 MOC with practice assessment
 ~$1100. MOC with practice assessment.")
66
PQRS Reporting Mechanisms
Claims Registry Qualified Clinical Data Registry (QCDR) Certified EHR Technology Group Practice Reporting Options Stay tuned – PPRNet will apply for 2015! CMS recognized Registry or EHR – not the same as MU 30 pts seen Jan – Dec 2011 Registry options: NCQA DRP for ex Clinicians Applying for Recognition and Submitting Data for PQRS: For clinicians who achieve Recognition in 2011 or who apply for Recognition in 2011 with the appropriate fee, the PQRS application fee is $50.00 per clinician in addition to the Recognition application fee of $500. Clinicians Already Recognized and Submitting Data for PQRS Only: For clinicians who have a current Recognition with a start date prior to 2011, i.e., 2008, 2009, 2010, the application fee is $150 per clinician.
 Certified EHR Technology. Group Practice Reporting Options. Stay tuned – PPRNet will apply for 2015! CMS recognized Registry or EHR – not the same as MU. 30 pts seen Jan – Dec Registry options: NCQA DRP for ex. Clinicians Applying for Recognition and Submitting Data for PQRS: For clinicians who achieve Recognition in 2011 or who apply for Recognition in 2011 with the appropriate fee, the PQRS application fee is $50.00 per clinician in addition to the Recognition application fee of $500. Clinicians Already Recognized and Submitting Data for PQRS Only: For clinicians who have a current Recognition with a start date prior to 2011, i.e., 2008, 2009, 2010, the application fee is $150 per clinician.")
67
All Pts with DM tab in pprnet plr

69
PQRS is pay for reporting
See note regarding > 0% requirement for full sample

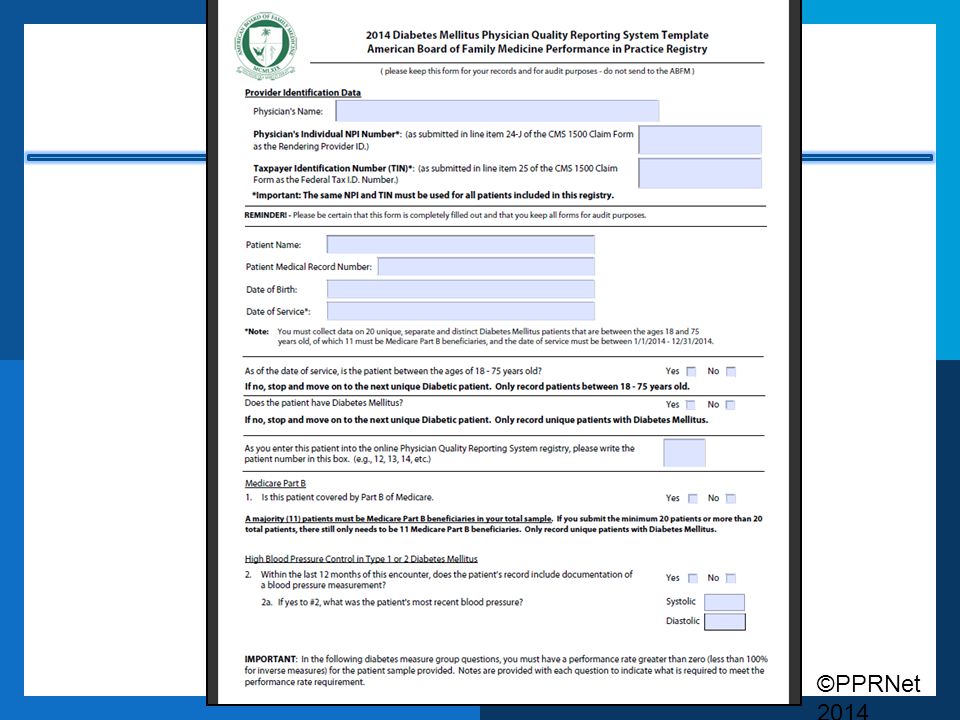
72
Using pprnet reports for pqrs
For 2014, use October 2014 PLR to fill out ABFM registry/report to CMS ABIM diplomates, check PQRS page for other registry options ($) For 2015, look for news of PPRNet becoming a Qualified Clinical Data Registry More tomorrow!
 For 2015, look for news of PPRNet becoming a Qualified Clinical Data Registry. More tomorrow!")
73
Physician compare

74
PPRNet’s “Top 10” List for Quality Improvement

75
1. Identify a Clinician Leader

76
2.Use PPRNet reports to identify opportunities for improvement and monitor progress.

77
3. Select a limited number of priorities for improvement and build on incremental successes

78
4. Adopt standing orders and have all staff function at the top of their licenses

79
5. Educate staff members as needed for their expanded roles

80
6. Hold regular practice “PPRNet meetings”

81
7. Use HM broadly and establish a practice goal to “get the red out”

82
8. Use PPRNet patient-level reports (PLRs) for patient case management and/or outreach.
 for patient case management and/or outreach.")
83
9. Provide staff incentives for achieving improvement goals.

84
10. Participate in PPRNet projects and attend PPRNet meetings.

85
Open Session “Making the Most” of PPRNet

86
recap First time attendees, how many new acronyms have you learned today? “Refresher” attendees, what new thing(s) did you learn?
 did you learn.")
87
recap To (begin to) answer the question: “How can I maximize the benefit of PPRNet in my practice?” Introduce (or reintroduce) PPRNet and its mission Provide an overview of PPRNet reports Share examples of how practices use PPRNet reports to achieve recognition and/or incentives Allow time for participants to use reports and network with one another
 PPRNet and its mission. Provide an overview of PPRNet reports. Share examples of how practices use PPRNet reports to achieve recognition and/or incentives. Allow time for participants to use reports and network with one another.")
88
Use your reports! Talk to each other!
Open session Use your reports! Talk to each other! Identify patients for NCQA PCMH population management or care management standards Identify 1 or 2 areas for improvement from your practice report

89
agenda 5:30 pm Happy Hour Rooftop at Vendue Inn, 19 Vendue Range
Presenters Dinner (Invitation only) Blossom, 171 East Bay Street Friday, August 22, 2014 7:15 am Breakfast & Registration 8:00 am Welcome 8:15 am Plenary: Improving the Quality of Primary Care Through "Meaningful" EHR Use
 Blossom, 171 East Bay Street. Friday, August 22, :15 am. Breakfast & Registration 8:00 am. Welcome 8:15 am. Plenary: Improving the Quality of Primary Care Through Meaningful EHR Use")
90
Follow-up needs assessment
Webinar topic suggestions

Similar presentations












 and Physician Privileging>")

>")






