Download presentation
Presentation is loading. Please wait.

1
Neuronal Transmission
BN Fall 2011 Julia Sobesky

2
Outline Types of synapses Neurotransmitters Receptor types
Electrical Chemical Neurotransmitters Criteria Types Release Inactivation Receptor types Ionotropic Metabotropic Ligand binding Plasticity Outline

3
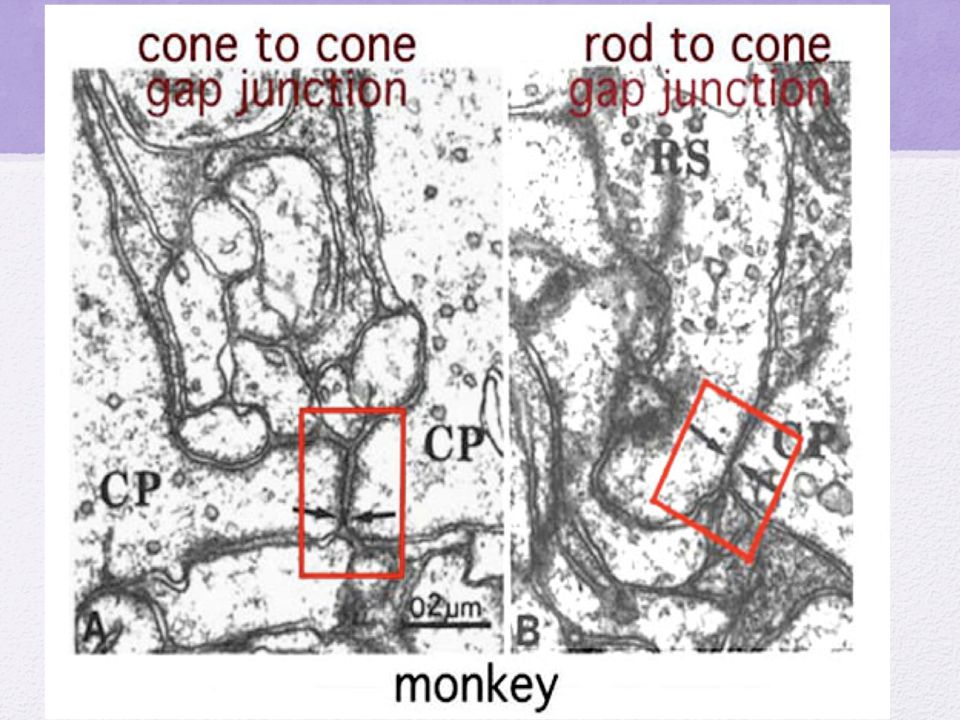
Electrical synapse: gap junctions
~3nm apart Very fast communication Direct pore between cells, allows bidirectional flow of ions 6 connexins= 1 connexon Allows rapid and synchronous firing of interconnected cells Examples are contractions during childbirth or cardiac contractions

5
Why would we need anything more?
Why don’t our brains just use electrical transmission?

6
Benefits of Chemical signaling
60+ different NTs and neuromodulators Each NT can have up to 15 different receptors Co-localization of several NTs in one synapse One neuron can have TONS of different synapses Simple or complex post-synaptic responses Post synaptic responses: differ in temporal action, more than just alterations in membrane potential When you think about how complex our thoughts and actions are, and that this is basically a series of synaptic connections, it makes more sense that we would need to have this much complexity to make it happen

7
The chemical synapse ~20-50 nm apart
NTs released by pre- synaptic cell bind receptors on post-synaptic membrane EPSP, IPSP or complex responses *** The RECEPTOR determines the response, not the NT *** Binding of NT is transitory, the more NT in the synapse, the greater the receptor responses

8
Criteria for NTs Synthesized in pre- synaptic cell
Activity dependent release Mechanism for deactivation Predictable pharmacological activity

9
Major classes of neurotransmitters
Small neurotransmitter molecules Synthesized near axon terminals Acetylcholine, monoamines, indolamines, amino acids Large neurotransmitter molecules- Neuropeptides Synthesized in soma hormones enkephalin/ endorphin Soluble gasses nitric oxide carbon monoxide WHY would small NTs be synthesized at terminals while large NTs in soma? -bc small NTs have dietary precursor components, Large NTs must be translated and transcribed Enk/end- work as endogenous morphine like molecules/NTs that decrease pain. Runners high Soluble gasses…. Don’t want to talk about, because not classical ---- but I have read estimations up to 2% of neurons in the brain use nitric oxide signaling. Soluble gasses.

10
Small Neurotransmitters
1. Amino Acids Glutamate/ Gamma-aminobutyric acid (GABA) MAJOR NTs in the CNS/ All over 2. The Monoamines Catecholamines Dopamine- DA- reward/movement Norepinephrine- NE –sympathetic Epinephrine-released from adrenals Indolamines Serotonin -5-HT 3. Acetylcholine (ACh) Glut is major excitatory NT in CNS/ GABA is major inhibitory. Glut- long axon neurons. GABA is primarily in interneuron (in one nucleus--- in between the input/out put neurons in one nucleus.) In a way, you can can anything else a neuromodulator… because these are the major NTs in the CNS, all the rest regulate whats going along the GABA or glutamatergic connections. 2. acetylcholine: contracts skeletal muscles/ ANS. Important in Alzheimer's disease in basal forebrain (Ach decreased)./ interneurons 3. Biogenic amines. Catechol/indol refers to their molecular structure. Localized in small cell groups/ clusters within the brain. Not widespread/ dispersed like the amino acids, but are equally important. NO SMALL EFFECT. Axon collaterals to cortex/ high order functions…… Da----- for example---- involved in addiction. VTA-- NAc. This pathway which utilizes DA transmission is vital to almost all kinds of addiction.
 MAJOR NTs in the CNS/ All over. 2. The Monoamines. Catecholamines. Dopamine- DA- reward/movement. Norepinephrine- NE –sympathetic. Epinephrine-released from adrenals. Indolamines. Serotonin -5-HT. 3. Acetylcholine (ACh) Glut is major excitatory NT in CNS/ GABA is major inhibitory. Glut- long axon neurons. GABA is primarily in interneuron (in one nucleus--- in between the input/out put neurons in one nucleus.) In a way, you can can anything else a neuromodulator… because these are the major NTs in the CNS, all the rest regulate whats going along the GABA or glutamatergic connections. 2. acetylcholine: contracts skeletal muscles/ ANS. Important in Alzheimer s disease in basal forebrain (Ach decreased)./ interneurons. 3. Biogenic amines. Catechol/indol refers to their molecular structure. Localized in small cell groups/ clusters within the brain. Not widespread/ dispersed like the amino acids, but are equally important. NO SMALL EFFECT. Axon collaterals to cortex/ high order functions…… Da----- for example---- involved in addiction. VTA-- NAc. This pathway which utilizes DA transmission is vital to almost all kinds of addiction.")
11
L-Dihydroxyphenylalanin (L-Dopa)
Amino Acids Glutamate GABA Catecholamines Tyrosine L-Dihydroxyphenylalanin (L-Dopa) Dopamine Norepinephrine Epinephrine Tyrosine Hydroxylase Glutamic Acid Decarboxylase (GAD) Important in understanding some of the examples of degradation. Just interesting to see that some NT that serve very different purposes in the CNS are precursors for each other. DA vs. NE. Stress response….. Fight of flight response. TYROSINE HYDROX IS RATE LIMITING FACTOR Parkinson’s- Da deficiency in pathways bt SN-striatum/ SN-GP. One treatment for PD is L-dopa. Glut is a precursor for GABA
 Dopamine. Norepinephrine. Epinephrine. Tyrosine. Hydroxylase. Glutamic. Acid. Decarboxylase. (GAD) Important in understanding some of the examples of degradation. Just interesting to see that some NT that serve very different purposes in the CNS are precursors for each other. DA vs. NE. Stress response….. Fight of flight response. TYROSINE HYDROX IS RATE LIMITING FACTOR. Parkinson’s- Da deficiency in pathways bt SN-striatum/ SN-GP. One treatment for PD is L-dopa. Glut is a precursor for GABA.")
12
Nuclei are the home of the cell bodies of the neurons that make and release the respective NTs

13
Then what? NTs are synthesized at terminal and packaged Or
Neuropeptides are transcribed, translated, packaged and trafficked down to the terminal How does an Action Potential initiate their release?

14
Exocytosis Ca++ facilitated SNARE Proteins
Voltage-gates Ca++ channels in the axon terminal open from AP and allow CA++ to enter. SNARE proteins allow vesicle to dock to the internal membrane, Ca++ enables SNARE proteins to fuse the vesicular and cell membranes together, allowing NT release into the synapse BOTOX SNARE Proteins

15
What happens to NTs after release?
Diffusion through synapse to post-synaptic cell NT binding to receptors is TRANSITORY, more NT around to bind, the greater the receptor effects ……. Uptake and recycled Enymatically broken down Taken up by glia cells, released later, like a sponge to soak up excess Passive diffusion away (can have distal effects)
")
16
2 Main Types of Receptors
Ionotropic Ligand-gated ion channels Directly alters the membrane potential Metabotropic Slower, but can have greater effects 2 types: G-protein coupled Tyrosine Kinase receptors Ionotropic receptors are ion-specific, when the NT binds and produces a conformational change to open the pore, the pore is wide enough to allow specific ions to pass through

17
Ionotropic Receptors Excitatory (EPSP) or Inhibitory (IPSP) responses
K+, Na+, Ca++ CL- Some can be ligand and voltage-gated (NMDA) Slow ionotropic: closes K+
 Slow ionotropic: closes K+")
18
Complex effects of metabotropic receptors
NO PORE, but binding can initiate: 2nd messenger system Other products could open ion channels Modulate enzyme activity Regulate ion channels in membrane Initiate gene transcription/translation Regulation of ion channels, both ligand gated (to alter the sensitivity of a cell to NT) and voltage gated, to alter electrical excitability and firing properties
 and voltage gated, to alter electrical excitability and firing properties.")
19
What happens to NTs after release?
Diffusion through synapse to post-synaptic cell NT binding to receptors is TRANSITORY, more NT around to bind, the greater the receptor effects NT must be cleared removal just as important as release Multiple things can happen…. Uptake and recycled Enymatically broken down Taken up by glia cells, released later, like a sponge to soak up excess Passive diffusion away (can have distal effects)
")
20
Uptake and degradation

21
Glial Sponge Glial cells can act as buffers for excess NTs
Can process and release NTs Passive diffusion away from the synapse Why? Distal effects, some cells have very distal receptors, if the receptor is able to identify an NT that has passively diffused away, there is TOO much, so the receptor initiates a negative feedback mechanism to release less NT

22
NT binding to receptor shape-specific
Lock and key arrangement Endogenous vs. exogenous Drugs work because we already have the receptors in place to receive them Drug actions are so intense because they cause actions so far above and beyond what endogenous compounds do Agonists Antagonists Full vs. partial Competitive vs. non- competitive Allosteric Allosteric- modifies the receptor to be more or less effected by the natural NT Competitive: based on affinity of the ligand to the receptor

23
Receptor agonists and antagonists
Full, partial, competative, non-competative, allosteric

24
Organization dictated by experience
Synapses can grow and retract, continually being altered by use Plasticity can occur in a variety of ways: Create new synapses Strengthen or weaken existing synapses Break old connections LTP Tolerance to drugs: can up or down regulate receptor numbers

25
Synaptic connections change over time
These are microglia, but I want you to see how cells move and interact, neurons do this too!

26
Putting it all together: Neuropharmacology
Tolerance develops due to cellular and receptor alterations in response to chronic drug use The changes also mediate withdrawal symptoms Withdrawal= opposite of drug effects Depression is most likely not due to a lack of serotonin (i.e. SSRIs) …Serotonin receptor is metabotropic Severe alcohol withdrawal can kill you: Seizures Glutamate excitotoxicity Alcohol= agonizes GABA, GABA receptors are down regulated because there was too much inhibition, cold-turkey= not enough GABA to keep inhibited= overly excited In an addicted state= drug + altered brain morphology = normal
 …Serotonin receptor is metabotropic. Severe alcohol withdrawal can kill you: Seizures. Glutamate excitotoxicity. Alcohol= agonizes GABA, GABA receptors are down regulated because there was too much inhibition, cold-turkey= not enough GABA to keep inhibited= overly excited. In an addicted state= drug + altered brain morphology = normal.")
27
Organization dictated by experience

28
Thanks! Questions?

Similar presentations