Download presentation
Presentation is loading. Please wait.

1
SENIORS WHAT DO YOU NEED TO KNOW? Lynne Nash, MSW, RSW
Geriatric Mental Health Consultant Geriatric Mental Health Consulting Services Calgary Health Region

2
WHY DO WE NEED TO KNOW ABOUT SENIORS?

3
Between 2006 and 2026, the number of seniors in Canada will increase from 4.3 million to 8 million Oct/07 issue of Alive Magazine

4
In 1991, people aged 65 and older made up 12% of the Canadian population. By 2011, this number will rise to almost 22%. By 2031, there will be approximately 9 million seniors, and they will account for 25% of the total population. Healthy Aging in Canada, p. 7

5
The average life span is increasing in Canada – 100 years ago, the average life span was 78.3 years. It is now 84.2 years Oct/07 issue of Alive Magazine The 85+ group is growing 4x faster than any other segment of the population

6
From 1991 to 2001, the percentage of Canadian seniors aged 80+ increased by 41% to 932, By 2011, it is expected to have increased another 43% to 1,300,000, the majority being women. Healthy Aging in Canada, p. 7

7
In the coming decades, seniors will comprise a larger share of the Canadian population, growing from 3.5 million people in 1996 to an estimated 6.9 million by 2021.

8
By 2015, there will be more Canadians aged 65 or older than children under the age of Healthy Aging in Canada, p. 7

9
There are presently over 250,000 seniors with dementia in Canada This number is expected to rise to 778,000 by There will be over 60,000 new cases of dementia in Canada each year until then RNAO, 2003

10
“New diagnostic approaches which are detecting Alzheimer’s disease at earlier stages, the addition of the ‘baby boom’ numbers to the aging population, and the increasing incidence of the risk factors for Alzheimer’s disease are causing a striking increase in the number of younger people who are being diagnosed with the disease.” Alzheimer’s Society, 2006, p. 1

11
By 2011, almost 12,000 people in the Calgary Health Region will require access to services for dementia-related concerns This number exceeds the total number of clients currently using home care services CHR

12
Although most seniors enjoy good mental health, at least 20% suffer mild to severe depression National Advisory Council on Aging

13
Seniors have the highest suicide rates of any age group The highest suicide rate is among single, white men aged 85 and older and they are more likely to succeed than females in the same age group Statistics Canada, 2002; RNAO, 2003

14
“Our civilization’s greatest victory is that it has conquered disease
“Our civilization’s greatest victory is that it has conquered disease. Its greatest failure is that it has not conquered fear of aging.” Jacques Seguela

15
HEALTHY AGING AND AGEISM

16
Healthy aging includes three components:
Low risk of disease and disease-related disability High level of mental and physical functioning An active interaction with life Maintaining close relationships with others Continuing involvement in activities that have personal meaning and purpose Gall & Swabo, Psychosocial Aspects of Aging

17
“All persons confront age-specific issues and obstacles that must be surmounted if they are to successfully cope with various life stages.” Gall & Swabo, Psychosocial Aspects of Aging

18
“Older Canadians are living longer and with fewer disabilities than the generations before them. At the same time, the majority of seniors have at least one chronic disease or condition. . . If [healthy aging is] left unaddressed, the aging of the population will have far-reaching social, economic and political impacts … that will far outweigh the cost of investing in healthy aging now.” Healthy Aging in Canada, p. vi

19
“Older adults can live longer, healthier lives by staying socially connected, increasing their levels of physical activity, eating in a healthy way, taking steps to minimize their risks for falls and refraining from smoking. But there are real environmental, systemic and social barriers to adopting these healthy behaviours. Some relate to inequities as a result of gender culture, ability, income, geography, ageism and living situations.” Healthy Aging in Canada, p. vii

20
“Ageism - discrimination based on age, especially prejudice against older people - is common in all societies. Ageism occurs when people believe that enabling and promoting healthy living among seniors is unimportant or too late to make a difference. For example, it is widely recognized that promoting activity is important for children and youth. There are many initiatives designed to do just that. But there is a prevailing attitude that it is not as important to be physically active in later life - that it may be too late, that the cost is prohibitive, and that the benefits aren't as great at this stage of life. This prejudice reflects our minimized expectations of older adulthood and misconceptions about seniors' ongoing and future participation and roles in society.” Healthy Aging in Canada, p. 11

21
As an older adult ages, society’s assumptions and stereotypes greatly restrict the roles that are available for that person. Gall & Swabo, Psychosocial Aspects of Aging

22
Society’s beliefs regarding the inevitability of decline in health, functioning and mental abilities as we age are prevalent. Many older persons themselves believe aging = loss of “joie de vive”. Gall & Swabo, Psychosocial Aspects of Aging

23
Ageism and the discrimination it creates can increase the vulnerability of older adults. Assumptions about old age may result in symptoms of trauma being mistaken for age-related illness HelpAge International, 2003

24
“It is time for a new vision on healthy aging – a vision that:
values and supports the contributions of older people; celebrates diversity, refutes ageism and reduces inequities; and provides age-friendly environments and opportunities for older Canadians to make healthy choices, which will enhance their independence and quality of life.” Healthy Aging in Canada, p. vii

25
Why is it important that seniors stay as healthy as possible?
Some 69% of older Canadians provide one or more types of assistance to spouses, children, grandchildren, friends and neighbours Older Canadians make an important contribution to the voluntary sector More than 300,000 Canadians 65 or older were in the labour force in Healthy Aging in Canada, p. vi

26
Healthy aging can delay and minimize the severity of chronic diseases and disabilities in later life, thus saving health care costs and reducing long-term care needs Not surprisingly, older people in vulnerable communities (Aboriginal, economically disadvantaged groups) have the greatest chance of aging poorly Chronic diseases are responsible for 67% of total direct costs in healthcare and 60% of total indirect costs ($52 billion) as a result of early death, loss of productivity and foregone income Healthy Aging in Canada, p. vii
 have the greatest chance of aging poorly. Chronic diseases are responsible for 67% of total direct costs in healthcare and 60% of total indirect costs ($52 billion) as a result of early death, loss of productivity and foregone income. Healthy Aging in Canada, p. vii.")
27
What does Canada’s older population look like?
Canadian seniors are a highly diverse group Men and women experience aging differently There are huge differences between a 65-year-old and an 85-year-old, yet both are lumped into the same category In 2001, almost 20% of the immigrant population of Canada was over 65, significantly higher than the national average Although a relatively small proportion of Aboriginal Canadians are seniors, the number is expected to rise significantly by 2016 Healthy Aging in Canada, p. 2-3

28
What does Canada’s older population look like?
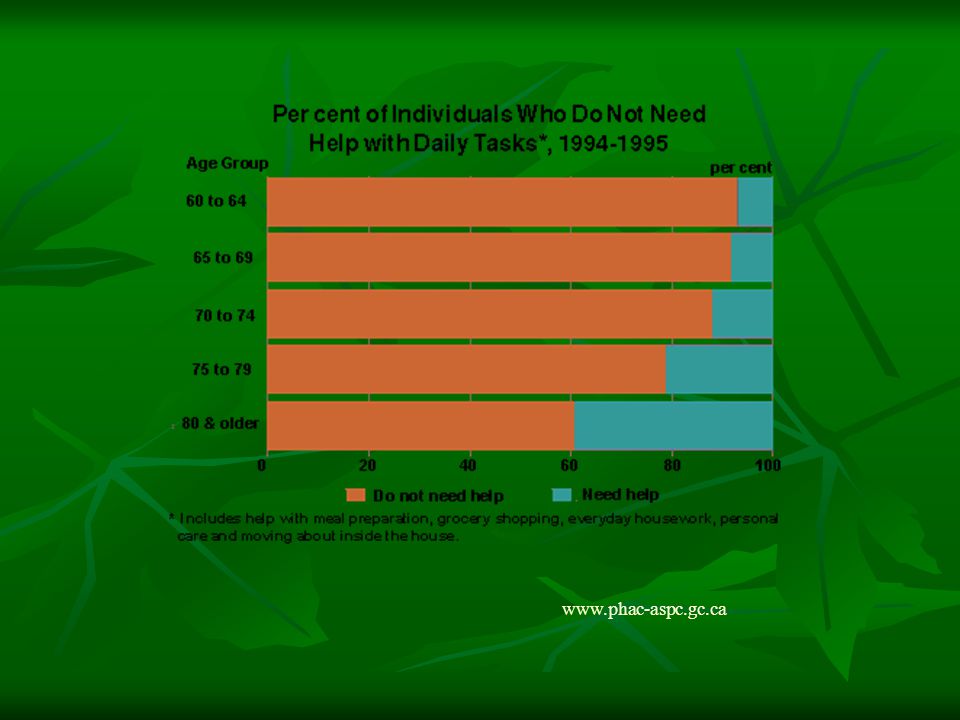
More than 90% of seniors live independently in the community and want to remain there Only 7% of those over 65 live in long term care; this number increases to 14% in the 75+ age group Most seniors aged 80 or older are women, the majority of whom live alone and are poor Around 1/3 of Canadian seniors live alone Healthy Aging in Canada, p. 2-3

29
What is Healthy Aging? “Healthy aging is ‘a lifelong process of optimizing opportunities for improving and preserving health and physical, social and mental wellness, independence, quality of life and enhancing successful life-course transitions’ (Health Canada, 2002). This definition takes a comprehensive view of health that includes physical, mental, social and spiritual well-being.” Healthy Aging in Canada, p. 4 “Health is seen as a positive resource … not the objective of living or the absence of disease” Healthy Aging in Canada, p. 3
. This definition takes a comprehensive view of health that includes physical, mental, social and spiritual well-being. Healthy Aging in Canada, p. 4. Health is seen as a positive resource … not the objective of living or the absence of disease Healthy Aging in Canada, p. 3.")
30
What is Healthy Aging? “Promoting good mental health is increasingly recognized as a priority in policy and program development for seniors. By working to increase self-efficacy, self-esteem, coping skills and social support, mental health promotion empowers people and communities to interact with their environments in ways that enhance emotional and spiritual strength. It fosters individual resilience and mutual aid. Mental health promotion also challenges discrimination against those with mental health problems and fosters respect for culture, equity, social justice and personal dignity.” Healthy Aging in Canada, p. 3-4

31
Social Connectedness and Healthy Aging
“Social connectedness has a positive effect on health. People who remain actively engaged in life and connected to those around them are generally happier, in better physical and mental health, and more empowered to cope effectively with change and life transitions. Distress, isolation and social exclusion increase substantially the risk of poor health and loneliness, and may even act as predictors of death.” Healthy Aging in Canada, p. 15

32
Social Connectedness and Healthy Aging
Social Support usually provided by family, friends, neighbours and members of supportive organizations such as a church group is a critical part of staying healthy physically (i.e., others provide encouragement and support to eat regularly) and mental health-wise Positively influences self-perceptions of health Healthy Aging in Canada, p. 15
 and mental health-wise. Positively influences self-perceptions of health. Healthy Aging in Canada, p. 15.")
33
Social Connectedness and Healthy Aging
Social Networks Much smaller than the social networks of younger adults, as many family and friends are deceased As they age, some seniors start to avoid making new social contacts, as the experience of more loss is too painful Declining health, decreased mobility, physical changes and sensory loss can make it very difficult for older adults to travel to or enjoy social outings Social activity is also influenced by poor accessibility to public transport, substance abuse, living in poverty, language barriers and living geographically remote areas or far away from family Healthy Aging in Canada, p. 17

34
Social Connectedness and Healthy Aging
“Studies have consistently found associations between loneliness and poor health … However, the relationship between loneliness and ill-health remains ambiguous. It is unclear whether loneliness occur as a result of poor health or if poor health is a result of loneliness” A recent study found that older women experiencing psychological stress (anxiety, feeling worthless or hopeless) were 60% more likely to die within eight years than those with lower stress levels. Healthy Aging in Canada, p. 19
 were 60% more likely to die within eight years than those with lower stress levels. Healthy Aging in Canada, p. 19.")
35
Social Connectedness and Healthy Aging
Although great strides have been made to reduce poverty amongst Canada’s seniors, those that remain poor are more likely to be women over the age of 80, divorced or separated, and have immigrated to Canada On average, women have more social connections than men, but older women are more likely to feel lonely, perhaps because they often outlive their spouse by several years Healthy Aging in Canada, p

36
Social Connectedness and Healthy Aging
Research indicates that seniors that are socially isolated and eat alone are more unlikely to have unhealthy eating habits and poor nutrition Poor nutrition, especially inadequate intake of B vitamins, contributes to cognitive decline and dementia Healthy Aging in Canada, p. 29

37
Social Connectedness and Healthy Aging
“Living alone (for both sexes) increases the person’s vulnerability to financial difficulty, chronic health problems and loneliness. Such persons commonly are in need of financial assistance and social services, and they are at risk for premature institutionalization.” Gall & Swabo, Psychosocial Aspects of Aging
 increases the person’s vulnerability to financial difficulty, chronic health problems and loneliness. Such persons commonly are in need of financial assistance and social services, and they are at risk for premature institutionalization. Gall & Swabo, Psychosocial Aspects of Aging.")
38
The majority of seniors live in urban areas
About 10% of Calgarians and Edmontonians are seniors (18% of those living in Victoria)
")
40
Healthy aging in the senior population is seriously affected by the 3 D’s – Delirium, Dementia and Depression Yet all three are often unrecognized due to their complexity and multi-faceted nature RNAO, 2003

41
Lack of recognition of Delirium, Dementia and Depression impacts the quality of life, morbidity and mortality of the older client RNAO, 2003

42
DELIRIUM

43
What is Delirium? Delirium involves a sudden change in behaviour, attention and/or memory Delirium usually develops over several hours or days Delirium is a medical emergency

44
What is Delirium? DSM-IV diagnosis:
disturbance of consciousness with a reduced ability to focus, sustain or shift attention a change in cognition or the development of a perceptual disturbance that is not better accounted for by a pre-existing, established or evolving dementia The disturbance evolves over a short period of time (usually hours or days) and tends to fluctuate during the course of the day
 and tends to fluctuate during the course of the day.")
45
Who Gets Delirium? Babies and children with high temperatures
Adults who are very ill Older adults – for a variety of reasons, they can be very susceptible to delirium CHR

46
Delirium - Prevalence In hospital, as many as 50-65% of older adults become delirious, for a variety of reasons Certain groups are at high risk: Postcardiotomy – 35% Post hip fracture – 40-65% Geriatric/neuropsychiatric patients – 40-60% CHR

47
Delirium Issues Commonly under-diagnosed in the elderly
Contributes significantly to morbidity and mortality in the geriatric age group Associated with increased length of hospitalization and risk of placement Often misdiagnosed as dementia GMHCS

48
Delirium Consequences
Prolonged cognitive impairment Cognitively, most elderly people with delirium never return to baseline The longer they are delirious, the greater the chance there will be irreversible cognitive changes GMHCS

49
Signs and Symptoms of Delirium
Don’t make sense when they speak Hallucinations and delusional thinking (dead babies, pregnant, think they’re dead, kidnapped, transported by aliens, conspiracy theory, etc.) Don’t pay attention to or recognize family or friends Don’t recognize everyday objects Forget things they’ve recently been told Forget where they are and think they are somewhere else Either restless and fidgety or sleepy and unresponsive
 Don’t pay attention to or recognize family or friends. Don’t recognize everyday objects. Forget things they’ve recently been told. Forget where they are and think they are somewhere else. Either restless and fidgety or sleepy and unresponsive.")
50
Signs and Symptoms of Delirium
Believe someone is trying to harm them Imagine things, people and events that never really occurred Try to get out of bed, crawling over bedrails Try to pull tubing and IV lines out Unable to control their bladder or bowel Become either very withdrawn or may yell or scream or be physically aggressive CHR

51
Common Medical Causes of Delirium in the Elderly
Alcohol – intoxication, withdrawal Cardiovascular – MI, cardiac arrhythnmia, CHF, hypertensive encephalopathy, TIA, cerebral embolism Infarction, acute CVA Infection – pneumonia, UTI, sepsis, cellulitis, encephalitis, meningitis Medications – any medication can cause delirium, but in particular antihista-mines, anticholinergics, psychotropics, anticon-vulsants, sedatives, digitalis, analgesics (opiates)
")
52
Common Medical Causes of Delirium in the Elderly
Metabolic – renal, pan-creatic or liver compro-mise, anemia (silent bleed), COPD, carbon monoxide poisoning, hypo- or hyper-thyroid-ism, hypo- or hyper-glycemia, hypo- or hyper-parathyoid states, Addisonian crisis, vitamin deficiency Physiological – epilepsy Post-anasthesia Primary psychiatric – manic delirium, catatonic excitement Trauma (fracture) Tumor Caine & Grossman, 1992
, COPD, carbon monoxide poisoning, hypo- or hyper-thyroid-ism, hypo- or hyper-glycemia, hypo- or hyper-parathyoid states, Addisonian crisis, vitamin deficiency. Physiological – epilepsy. Post-anasthesia. Primary psychiatric – manic delirium, catatonic excitement. Trauma (fracture) Tumor. Caine & Grossman,")
53
Common Non-Medical Causes of Delirium in the Elderly
Dehydration Decreased oxygen High temperature Severe pain Moving an elderly person from one place to another (i.e., home to the hospital, hospital to long term care, one room to another in hospital) Sensory overload/deprivation Isolation Use of restraints Drinking grapefruit juice – interferes with how some medications work CHR
 Sensory overload/deprivation. Isolation. Use of restraints. Drinking grapefruit juice – interferes with how some medications work. CHR.")
54
The rate of diagnosis of delirium by medical professionals is 20%! CHR

55
For the delirium to clear, treatment must be aimed at the cause of the problem. If there is more than one cause for delirium, all the problems need to be treated. CHR

56
Psychotropic medication is not recommended for delirium unless there is a specific issue, such as aggression, and should only be used until the delirium clears CHR

57
Delirium at End of Life Occurs in about 80% of cases involving terminal illness But – 50% of the time, if it’s the first time they’ve had delirium, the delirium is reversible Second time having a delirium, 26% reversible Physician and family need to discuss whether or not diagnostic work-up and treatment is appropriate CHR

58
Questions to ask Current year, month Age, birth date Are they married?
How many children, grandchildren? Names of husband, children, grandchildren Where are they? What time of day is it (lunchtime, evening, etc.) Count backwards from 20 Say the months of the year in reverse order CHR
 Count backwards from 20. Say the months of the year in reverse order. CHR.")
59
CAM – Confusion Assessment Method Instrument
Acute onset Inattention Disorganized thinking Altered level of consciousness Disorientation Memory impairment Perceptual disturbances Psychomotor agitation or retardation Altered sleep/wake cycle Inouye, et. al.

60
CAM – Confusion Assessment Method Instrument
To have a positive CAM result, the person must display: Presence of acute onset and fluctuating discourse AND Inattention AND EITHER Disorganized thinking OR Altered level of consciousness Inouye, et. al.

61
DEPRESSION

62
Prevalence of Depression
15-27% of those over 65 living in the community have depressive symptoms Only 1-3% actually diagnosed with major depression Prevalence may be much higher than studies indicate, especially in long term care centres (up to 47%) 46% of those with Parkinson’s disease suffer from depression 60% of stroke patients develop depression 45% of hospitalized medically ill elderly are depressed 25% of people with Alzheimer’s are depressed GMHCS
 46% of those with Parkinson’s disease suffer from depression. 60% of stroke patients develop depression. 45% of hospitalized medically ill elderly are depressed. 25% of people with Alzheimer’s are depressed. GMHCS.")
63
Prevalence of Depression
Many seniors with undiagnosed and untreated depression are admitted to long term care, bringing their chronic depression with them Survival rates for depressed long term residents are 10% less at six months and 15% less at one year, compared to non-depressed residents GMHCS

64
10-15% of seniors in the community suffer from depressive symptoms and/or clinical depression Healthy Aging in Canada, p. 6

65
Depression Risk Factors - Biological
Female gender (2:1) Possible genetic factors (twin studies) Changes in neurotransmitter activity and metabolism with aging Dysregulation – thyroid, growth hormone, circadian rhythm, Overall physical and cognitive decline Medical issues (pain, decreased mobility, respiratory and cardiac issues) Polypharmacy (lots of meds can cause depression) GMHCS
 Possible genetic factors (twin studies) Changes in neurotransmitter activity and metabolism with aging. Dysregulation – thyroid, growth hormone, circadian rhythm, Overall physical and cognitive decline. Medical issues (pain, decreased mobility, respiratory and cardiac issues) Polypharmacy (lots of meds can cause depression) GMHCS.")
66
Depression Risk Factors – Biological Medical illnesses associated with depression:
Metabolic – uremia, hypoxia, electrolyte imbalance, dehydration, etc. Endocrine – thyroid dysfunction, diabetes, hyperparathyroidism, Cushing’s, Addison’s Infections – UTI, pneumonia, TB, endocarditis, encephalitis Cardiovascular – CHF, MI, angina Pulmonary – COPD, malignancy GI – malignancy (pancreas), irritable bowel syndrome, ulcer, hepatitis MSK – arthritis, osteoporosis, fractures Neurological, stroke, TIA, dementia, tumors, Parkinson’s Other – anemia, vitamin deficiencies, malignancy, sensory loss, substance abuse GMHCS
, irritable bowel syndrome, ulcer, hepatitis. MSK – arthritis, osteoporosis, fractures. Neurological, stroke, TIA, dementia, tumors, Parkinson’s. Other – anemia, vitamin deficiencies, malignancy, sensory loss, substance abuse. GMHCS.")
67
Vitamin D deficiency is common among older adults
Depression Risk Factors – Biological Medical illnesses associated with depression: Vitamin D deficiency is common among older adults Vitamin D deficiency has been shown to be associated with symptoms of depression and poor cognitive performance Wilkins, et. al., 2006

68
Depression Risk Factors – Psychosocial
Loss, loss, loss, loss – roles, financial, home environment, bereavement (family, friends, pets), independence, cognitive function, health Social isolation Previous history of depression Cognitive distortions GMHCS
, independence, cognitive function, health. Social isolation. Previous history of depression. Cognitive distortions. GMHCS.")
69
What does depression in the elderly look like?
“Older persons with significant depression may have fewer symptoms than the number required by the DSM-IV criteria” Gallo & Rabins, 2005, p. 2 “Older adults who are physically ill are especially at risk for inadequate treatment of depression … depression may not be easy to recognize” Gallo & Rabins, 2005, p. 4

70
What does depression in the elderly look like?
Irritability Anxiety or worries Psychomotor changes – slowing down or agitation, complaints of having “bad nerves” Sleep disturbance Loss of interest in activities previously enjoyed Lack of interest in personal care (dishevelled look) Low energy and excessive fatigue Difficulty concentrating and what may appear to be cognitive impairment (misdiagnosed as dementia) Feelings of hopelessness
 Low energy and excessive fatigue. Difficulty concentrating and what may appear to be cognitive impairment (misdiagnosed as dementia) Feelings of hopelessness.")
71
What does depression in the elderly look like?
Weepy Loss of appetite, often accompanied with weight loss Fixation on somatic complaints, such as digestion, bowels, headaches, pain Feelings of guilt or excessive preoccupation with regrets of the past Feeling punished Suicidal ideation Symptoms often coincide with life changes and have an abrupt onset GMHCS

72
What does depression in the elderly look like?
Seniors will commonly deny feelings of sadness or feeling depressed Although it is normal for a senior to think about death on a regular basis, suicidal ideation is not normal – watch for statements such as “I might as well be dead” or “what’s the use?” Gallo & Rabins, 2005

73
Geriatric Depression Scale
Are you basically satisfied with your life? Have you dropped many of your activities and interests? Do you feel that your life is empty? Do you often get bored? Are you in good spirits most of the time? Do you feel happy most of the time? Do you often feel helpless?

74
Geriatric Depression Scale
Do you prefer to stay at home, rather than going out and doing new things? Do you feel you have more problems with memory than most? Do you think it is wonderful to be alive now? Do you feel full of energy? Do you feel that your situation is hopeless? Do you think that most people are better off than you are?

75
Geriatric Depression Scale – Short Form
Are you basically satisfied with your life? Do you feel that your life is empty? Are you afraid that something bad is going to happen to you? Do you feel happy most of the time?

76
Cornell Scale for Depression in Dementia
Anxiety (anxious expression, worrying) Sadness (sad voice, fearfulness) Lack of reactivity to pleasant events Irritability (easily annoyed, short tempered) Agitation (restlessness, hand wringing, hair pulling) Slowed movements, speech or reactions Multiple physical complaints Loss of interest, less involved in usual activities
 Sadness (sad voice, fearfulness) Lack of reactivity to pleasant events. Irritability (easily annoyed, short tempered) Agitation (restlessness, hand wringing, hair pulling) Slowed movements, speech or reactions. Multiple physical complaints. Loss of interest, less involved in usual activities.")
77
Cornell Scale for Depression in Dementia
Appetite loss, eating less than usual Weight loss Lack of energy, fatigues easily, unable to sustain activities Sleep difficulties – falling asleep later, multiple awakenings, early morning awakening Mood is worse in the morning Feels life is not worth living, death wishes or suicide attempts Poor self-esteem – self-blame, apologetic, feeling like a failure, “I’m so stupid” Pessimism – anticipating the worst Delusions of poverty, illness, loss

78
Questions to ask for Depression
How’s your appetite? How are you sleeping – do you have trouble falling asleep or waking up during the night, do you feel rested in the morning? How would you describe your mood? Do you ever feel sad, anxious or depressed? Do you worry about anything? How’s your energy level, do you feel motivated to do the things you used to enjoy or visit with others? Do you feel guilty about anything, or as if you were being punished? Do you go to bed at night and wish you wouldn’t wake up in the morning? GMHCS

79
Stress can cause: Suppression of the immune system
Impaired decision making Difficulty problem-solving Hypervigilance and paranoia Decreased perceptual and motor skills Gall & Swabo, Psychosocial Aspects of Aging

80
A major sources of stress for seniors as they age involves loss, such as loss of:
Family, friends and pets through death Social network due to sensory loss and/or mobility issues Primary control over decision-making regarding health, mobility, living situation and finances Occupational and/or role status Income Physical and sensory functioning Home and sense of belonging Gall & Swabo, Psychosocial Aspects of Aging

81
“Do not regret growing older
“Do not regret growing older. It is a privilege denied to many” Anonymous

82
MEMORY – WHEN TO WORRY!

83
MEMORY TEST #2

84
Memory problems can be due to:
Illness Dehydration Poor diet Lack of sleep Medications Depression Thyroid problems Vitamin deficiencies Alcohol and drug abuse Many other causes – most of which are treatable

85
But don’t panic – poor memory may simply be due to:
Lack of focus (not paying attention) Trying to rush Being disorganized Being anxious
 Trying to rush. Being disorganized. Being anxious.")
86
Seven problems with memory
1. Transience “Use it or lose it” Memories from the distant past fades with time Happens to most of us

87
Seven problems with memory
2. Absent-mindedness “Where are my flippin’ keys?” “What was I just about to do?” This is an attention problem, rather than a memory problem – related to lack of attention and superficial processing of information

88
Seven problems with memory
3. Blocking Can’t remember a name or particular word, but know “it’s on the tip of my tongue!” Temporarily can’t access the information More common as we grow older Usually nothing to worry about

89
Seven problems with memory
4. Misattribution The memory is present, but we attribute it to the wrong thing, person, place, etc. We remember the general picture of what happened, but fill in the details “I remember the night we met – you wore a red dress and had your hair cut short” “No I didn’t – I had long hair and wore a green dress!” Confabulation – the “time” and “source” tags fall off the memories, so you’re not making things up, just misattributing them

90
Seven problems with memory
5. Suggestibility We incorporate information from other people into our memories “Remember I told you” ruse – someone insists they told you something, you assume you forgot what they said and end up taking the blame - “I guess I forgot” More common with age

91
Seven problems with memory
6. Bias Pre-existing knowledge/beliefs/feelings influence our recall See a group of teenage boys walking down the street and assume they’re up to no good - “I remember they had an angry looks on their faces and I just knew they were going to do something”

92
Seven problems with memory
7. Persistence Can’t forget Chronic fears, PTSD “I remember every little detail of what happened as if it was yesterday” Memory works better, we remember more detail, when we’re scared Emotional arousal makes for stronger recall “Natural selection” – we gain an evolutionary advantage by remembering the things that scare us

93
How to improve your memory
Pay attention! Write it down Repeat it out loud Have a set spot in your home (by the door) for items such as keys Use word association to help remember facts
 for items such as keys. Use word association to help remember facts.")
94
How do you know if memory issues are becoming a problem?
They’re noticeable to others They make it difficult for someone to manage their daily activities They come on after a serious illness (stroke, head injury, heart attack), etc.
, etc.")
95
Remember Significant memory loss is not an inevitable result of aging. In fact, the brain is capable of producing new brain cells and learning new things at any age.

96
Recent research indicates the brain is like any other muscle in the body: use it or lose it
Both mental stimulation and physical exercise are necessary to keep your mind fit as you age The more the brain is involved in new learning, the better it works to gain, process and retain information Seniors who walk regularly have less chance of cognitive decline, especially executive functioning (planning, organizing and the ability to juggle more than one task at once) Runners can look forward to having better long-term memory Alive Magazine, 2007
 Runners can look forward to having better long-term memory. Alive Magazine,")
97
To keep the brain fit, the key principles are:
Novelty Variety Constant challenge Some of the best ways to keep fit are reading, doing puzzles, playing cards or board games, playing a musical instrument or painting Alive Magazine, 2007

98
Harvard Medical School’s 12 tips for keeping the brain (and memory) healthy
Get mental stimulation Get physical exercise Improve your diet Improve your blood pressure Improve your blood sugar levels Improve your cholesterol Consider taking a low dose of aspirin daily Harvard Men’s Health Watch, 2006

99
Harvard Medical School’s 12 tips for keeping the brain (and memory) healthy
Avoid tobacco Don’t abuse alcohol Maintain good mental health Protect your head Build social networks Harvard Men’s Health Watch, 2006

100
It is estimated that 750,000 Canadians will have dementia by 2031

101
“Some people, no matter how old they get, never lose their beauty – they merely move it from their faces into their hearts” Martin Buxbaum

102
Dementia - Definition An acquired impairment in intellectual functioning in at least two spheres: Language Visuospacial Memory Executive function Ability to do routine tasks, recognition Abstraction, calculation Symptoms usually progress slowly and/or are relatively stable over a few years, unlike delirium Richardson, 1995

103
Prevalence of Dementia
5% of those aged 65 Prevalence increases significantly with age By age 85, about 35% of individuals suffer from dementia By age 95, the prevalence is about 45% GMHCS

104
Prevalence of Dementia
Today, one out of every 20 Canadians over the age of 65 has Alzheimer’s disease. Over the age of 85, the chances of having Alzheimer’s increases to one in four Alzheimer Society of Canada, 2006

105
Types of Dementia Alzheimer’s disease
up until recently, thought to be the most common type % Insidious onset, progressive deterioration Vascular dementia pure vascular quite rare – 5-10% Often a step-wise progression related to CVA’s or TIA’s Often positive neuroimaging findings Treatable risk factors Mixed (Alzheimer’s and vascular dementias) now recognized as being the most common form of dementia – 50-60% GMHCS
 now recognized as being the most common form of dementia – 50-60% GMHCS.")
106
Types of Dementia Dementia with Lewy bodies
5-15% prevalence, likely underdiagnosed Memory problems may not be an early feature Must have two of the following early in the course of the disease: Parkinson’s features, fluctuation cognition, psychotic features (usually hallucinations) GMHCS
 GMHCS.")
107
Types of Dementia Pick’s disease/frontotemporal dementia
5-10% prevalence Onset often before the age of 65 Usually only mild memory loss Progressive behavioural change Early loss of social judgement and empathy Impulsivity Loss of insight early in course Language problems may be prominent early and predate the dementia GMHCS

108
Types of Dementia Other – 5% (i.e., Parkinson’s disease, alcohol-induced, normal pressure hydrocephalus, MS, HIV-related dementia, Creutzfeldt Jakob disease, thyroid disease) Less than 5% are reversible GMHCS
 Less than 5% are reversible. GMHCS.")
109
Diagnosing Alzheimer’s disease and other dementias
Postmortem examination of the brain to detect plaques and tangles is the only way to identify Alzheimer’s disease with certainty A number of psychological and memory tests have been developed which quite accurately (90-95%) allow a diagnosis of Alzheimer’s disease (or other dementia) to be made Psychological and memory testing, medical examination and gathering of collateral information helps to identify the appropriate dementia(s) CAT scans and brain imaging techniques such as Magnetic Resonance Imaging (MRI) are used to more accurately identify what type of changes occur in the brain Genetic testing for the “Alzheimer’s gene” is now available, but not widely undertaken in Canada at present - Alzheimer’s Society of Canada, 2006
 allow a diagnosis of Alzheimer’s disease (or other dementia) to be made. Psychological and memory testing, medical examination and gathering of collateral information helps to identify the appropriate dementia(s) CAT scans and brain imaging techniques such as Magnetic Resonance Imaging (MRI) are used to more accurately identify what type of changes occur in the brain. Genetic testing for the Alzheimer’s gene is now available, but not widely undertaken in Canada at present. - Alzheimer’s Society of Canada,")
110
The Brain Limbic System

111
Alzheimer’s Society 8

112
Alzheimer’s Society 9

113
Brain Changes that Occur with Alzheimer’s Disease
Plaques and tangles develop in the brain, in a sense choking the cells of the brain to death. Messages in the brain cannot get past the damaged cells and therefore cannot get from one part of the brain to another (i.e., the back muscles send a message to the brain that they are in pain, but the message cannot get through to the part of the brain that deciphers the message, so the person is unable to identify they are in pain; rather, they become agitated “for no apparent cause” and will even say “no” if asked if they do have pain.) Inflammation of the brain – the body’s normal response to trauma is to defend itself by intensifying an immune response, unfortunately escalating the death of brain cells Shrinkage and degeneration of nerve cells – originates in the part of the brain responsible for thinking and memory and eventually spreads to all parts of the brain - Alzheimer’s Society of Canada, 2006
 Inflammation of the brain – the body’s normal response to trauma is to defend itself by intensifying an immune response, unfortunately escalating the death of brain cells. Shrinkage and degeneration of nerve cells – originates in the part of the brain responsible for thinking and memory and eventually spreads to all parts of the brain. - Alzheimer’s Society of Canada,")
114
Alzheimer’s Disease - Early Stage
Memory loss Time and spatial disorientation Poor judgement Personality changes Withdrawal or depression Perceptual disturbances GMHCS

115
Alzheimer’s Disease – Mid-Stage
Recent and remote memory worsens Increased aphasia (slowed speech and understanding) Hyperorality Apraxia (decreased ability to make the moves to do routine tasks such as brushing teeth) Disorientation to time and place Restlessness or pacing Perseveration Irritability Loss of impulse control GMHCS
 Hyperorality. Apraxia (decreased ability to make the moves to do routine tasks such as brushing teeth) Disorientation to time and place. Restlessness or pacing. Perseveration. Irritability. Loss of impulse control. GMHCS.")
116
Alzheimer’s Disease – Late Stage
Incontinence of bladder and bowel Loss of motor skills, rigidity Decreased appetite and dysphagia Agnosia (inability to recognize and identify objects) Apraxia (can’t find the right words) Communication severely impaired May not recognize family members or self in mirror Loss of most or all self-care abilities Cognition severely impaired Immune system depressed GMHCS
 Apraxia (can’t find the right words) Communication severely impaired. May not recognize family members or self in mirror. Loss of most or all self-care abilities. Cognition severely impaired. Immune system depressed. GMHCS.")
117
Dementia – What to Watch For
Confabulation - making up the story or details as they go along Minimizing and denying losses Rambling speech Perseveration - changing the subject continually to something in particular Difficulty with nouns Difficulty with abstract word finding Generally normal mood – can be “pleasantly confused” or can become irritable when asked too many questions they can’t answer May be very suspicious as to why they are being asked questions “Mind your own business!”, “I’m not going to tell you” “Yes, I know my age, but I’m not going to tell you” GMHCS

118
Risk Factors for Alzheimer’s Disease
Age – with age comes a decline in the body’s ability to repair any damage. This decline occurs at different rates in different people. Genetic risk factors – everyone has two sets of genes, one from each parent. If a person gets one “Alzheimer’s gene”, they are three times more likely to develop Alzheimer’s. If they carry both A. genes, they are ten times more likely to develop Alzheimer’s. - Alzheimer’s Society of Canada, 2006

119
Risk Factors for Alzheimer’s Disease
Diabetes – likely due to the blood vessel and heart disorders, and sometimes obesity, that accompany Type II diabetes. Also, glucose utilization is impaired in the Alzheimer brain. Current research is looking at new anti-diabetic drugs used by those with Type II diabetes to help their bodies respond to insulin, to see if they could also be helpful in reducing the malfunctioning of the brain in those people with Alzheimer’s disease who do not have diabetes. There are encouraging indications that memory and cognition could be enhanced. - Alzheimer’s Society of Canada, 2006

120
Risk Factors for Alzheimer’s Disease
Mild cognitive impairment Being female – twice as many women than men get Alzheimer’s (live longer, more prone to diabetes and decline in estrogen post-menopause) Down’s syndrome (almost all who live into their 40’s will develop Alzheimer’s) Chronic inflammatory conditions History of clinical depression Head injury High cholesterol levels Strokes or “ministrokes” High blood pressure Stress Lack of physical exercise Inadequate exercising of the brain Unhealthy eating habits Obesity Low level of formal education Low socio-economic status (these last two may be indicative of other risk factors in their environment that have not yet been identified) - Alzheimer’s Society of Canada, 2006
 Down’s syndrome (almost all who live into their 40’s will develop Alzheimer’s) Chronic inflammatory conditions. History of clinical depression. Head injury. High cholesterol levels. Strokes or ministrokes High blood pressure. Stress. Lack of physical exercise. Inadequate exercising of the brain. Unhealthy eating habits. Obesity. Low level of formal education. Low socio-economic status (these last two may be indicative of other risk factors in their environment that have not yet been identified) - Alzheimer’s Society of Canada,")
121
- Alzheimer’s Society of Canada, 2006
The Good News Research indicates that adopting a healthy lifestyle is the best way to lower the chances of developing Alzheimer’s. Studies of identical twins have shown that around 60% of the overall risk of developing Alzheimer’s disease comes from lifestyle, rather than genetic susceptibility. - Alzheimer’s Society of Canada, 2006

122
Recent research indicates that the frequent consumption of fruit and vegetable juices may significantly reduce the risk of Alzheimer’s disease Seniors who consumed three or more glasses of fruit or vegetable juice per week were 76% less likely to develop Alzheimer’s disease than those who drank less than one glass per week Scientists believe that antioxidants, found in high concentration in the skin and peel of fruits and vegetables, may act to protect the brain from other chemicals that can cause damage Another study showed that drinking two glasses of apple juice per day improves memory and prevents cognitive decline Vitamins and minerals protect blood vessels from deterioration, ensuring optimal blood flow to the brain (Alzheimer’s has been linked to poor blood flow) - Oct/07 issue of Alive Magazine
 - Oct/07 issue of Alive Magazine.")
123
Why is it so important to get accurate diagnosis of dementia as soon as someone exhibits possible signs and symptoms? The sooner someone is diagnosed, the sooner treatment can begin ↓ The sooner treatment can begin, the greater the likelihood that cognitive and memory decline can be slowed Also, accurate diagnosis means that the most appropriate treatment plan can be developed Early diagnosis and treatment = ↑ quality of life

124
Treatment of Alzheimer’s Dementia
Aricept™ (donezipel) (cholinesterase inhibitor) Exelon™ (rivastigmine) (cholinesterase inhibitor) Reminyl™ (galantamine) (cholinesterase inhibitor) Ebixa® (memantine hydrochloride) Basically, these medications help messages to be conveyed from one nerve cell to the next, so that messages have a better chance of getting through to the right place
 (cholinesterase inhibitor) Exelon™ (rivastigmine) (cholinesterase inhibitor) Reminyl™ (galantamine) (cholinesterase inhibitor) Ebixa® (memantine hydrochloride) Basically, these medications help messages to be conveyed from one nerve cell to the next, so that messages have a better chance of getting through to the right place.")
125
DIFFERENTIATING BETWEEN DEMENTIA, DEPRESSION AND DELIRIUM

126
Is it depression or dementia?
Common disorders in the elderly They may co-exist Alzheimer’s disease – up to 25% experience depression Vascular dementia – an even higher prevalence of depression than AD Many symptoms overlap, making them difficult to distinguish Depression may cause reversible dementia GMHCS

127
Is It Depression Or Dementia – Common Symptoms
Eating changes Dementia – usually gradual weight loss over years, but may be a large weight increase due to inactivity, hyperorality (frontotemporal dementia), medications, etc. Depression – subacute changes over weeks to months, weight may increase or decrease GMHCS
, medications, etc. Depression – subacute changes over weeks to months, weight may increase or decrease. GMHCS.")
128
Is It Depression Or Dementia – Common Symptoms
Sleep disturbance Dementia – gradual loss of diurnal pattern over years Depression – subacute changes over weeks to months Often middle night awakening or early morning awakening May be excessive sleep GMHCS

129
Is It Depression Or Dementia – Common Symptoms
Mood Dementia – may have early depressive mood; later, mood fluctuates according to circumstances Irritability fairly common Depression – pervasive changes over weeks, nearly every day Sadness Irritability Loss of pleasure GMHCS

130
Is It Depression Or Dementia – Common Symptoms
Mood lability Dementia – increases with time, often unrelated to circumstances (laughing or crying anappropriately) Depression – more crying, congruent with sadness Apathy Dementia – loss of interest and initiative without sadness Depression – subacute onset with sadness and feelings of helplessness GMHCS
 Depression – more crying, congruent with sadness. Apathy. Dementia – loss of interest and initiative without sadness. Depression – subacute onset with sadness and feelings of helplessness. GMHCS.")
131
Is It Depression Or Dementia – Common Symptoms
Concentration Dementia – usually intact until the late stages slowly progressive changes Person often unaware and unconcerned Depression – subacute changes often a major concern for the person “Do I have dementia?” Many “I don’t know” answers on testing Give up easily GMHCS

132
Is it depression or dementia?
Depressed senior exagger-ates their disabilities: “I can’t”, “I don’t know” Tests better than anticipated Inability to concentrate Insomnia, difficulty with sleep onset/early morning waking, hypersomnia Slow, sluggish speech Commonly have feelings of guilt, worthlessness Ruminations common Suicidal ideation much more common Dementia: Senior with dementia confabulates, minimizes and denies losses Rambling speech, difficulty with nouns Difficulty with abstract word finding Generally normal mood Sleep is fragmented, often awakens at night GMHCS

133
Is it depression or delirium?
Symptoms of depression may occur in delirium, but depression cannot be diagnosed until the delirium has cleared One study showed that 42% of elderly people sent to a psychiatric service for treatment of depressive symptoms actually had delirium GMHCS

134
What to Look for/Notice
Appearance body frame Size personal hygiene Dress Psychomotor behaviour Speech Affect Mood Eye contact Thought content Perceptual disturbances Person’s description/percep-tion of the problem Cognitive state (MMSE) GMHCS
 GMHCS.")
135
Differentiating Between the 3 D’s
Delirium Dementia Depression Onset Sudden/abrupt; depends on cause; often at twilight or in darkness Insidious/slow and often unrecognized; depends on cause Coincides with major life changes; often abrupt, but can be gradual Duration Hours to weeks Months to years At least 2 weeks, but can be months to years Alertness Fluctuates, lethargic or hypervigilant Generally normal Normal Memory Recent and immediate impaired Recent and remote impaired Selective or patchy impairment, islands of intact memory Thinking Disorganized, distorted, fragment-ed, slow or acceler-ated, incoherent Difficulty with abstraction, thoughts impoverished, poor judgements, word finding difficulty Intact, but with themes of hopelessness, helplessness or self-deprecation Perception Distorted, delusions, hallucinations, difficulty distinguishing between reality & misperceptions Misperceptions uncommon Intact RNAO, 2003

136
MMSE (Mental Status Exam)
Needs to be administered and scored properly When done on a regular basis, can indicate progression of dementia If there is a drastic change in a short period of time and the person has not had a CVA, poor score can indicate delirium GMHCS

137
MMSE (Mental Status Exam)
Orientation: what is the year, season, month, date, day of week, country, province, city, name of building, room number Registration/attention & short-term memory: remember three words, spell “world” backwards Language/spatial orientation & coordination: name a pen and watch, repeat phrase, read a sentence, write a sentence, copy a design, 3-part instruction Molloy, 1989

138
MoCA (Montreal Cognitive Assessment)
Better assessment tool for mild dementia or dementias such as frontotemporal, where confusion and poor memory are not an issue Picks up more subtle changes in cognition May score 30/30 on the MMSE, yet score poorly on the MoCA GMHCS

139
WHAT ELSE DO WE NEED TO KEEP IN MIND?

140
Sensory Loss Gradual sensory loss is a “normal” part of aging
Loss of vision, hearing, taste, smell and touch can adversely affect a senior’s quality of life Orzech, Social Work Today

141
Sensory Loss Smell and taste play a key role in food enjoyment and trigger feelings of hunger Loss of smell and taste, and therefore motivation to eat a variety of foods, contributes to poor nutrition in the elderly As a result of sensory loss, many seniors add more salt and sugar to their food in order to try to make the food taste better Orzech, Social Work Today

142
Sensory Loss Macular degeneration is the most common age-related vision disorder affecting seniors. People with macular degeneration are unable to see things in the centre of their vision field Diabetic retinopaty (blurry and fluctuating vision) affects the sight of many seniors Poor vision often leads to social isolation and boredom, as it becomes impossible to read or perform usual tasks Orzech, Social Work Today
 affects the sight of many seniors. Poor vision often leads to social isolation and boredom, as it becomes impossible to read or perform usual tasks. Orzech, Social Work Today.")
143
Sensory Loss More than 25% of seniors over the age of 75 report problems with their eyesight, even when wearing glasses Poor vision often leads to social isolation and boredom, as it becomes impossible to read or perform usual tasks Orzech, Social Work Today

144
Sensory Loss Around 30% of seniors have significant hearing loss
As with poor vision, hearing loss can result in social isolation and boredom, as communication with others, in person or over the telephone, is so difficult Some studies show a relationship between hearing loss and depression, although not as strong a connection as with vision loss Orzech, Social Work Today

145
Sensory Loss Many of those in the helping professions, including social workers, are unaware of the problems faced by seniors as a result of sensory loss. Social workers need to pay attention when a client has a precursor such as diabetes so that appropriate resource information can be provided to the client Orzech, Social Work Today

146
Sensory Loss “Nor are many social workers aware of the connection between vision loss in older adults and depression. Older people with vision impairment are anywhere from two to five times more likely to suffer from depression than someone without vision impairment. Between ¼ and 1/3 of visually impaired elders report a significant number of depressive symptoms.” Orzech, Social Work Today, p. 21

147
Pain Pain issues are reported by 25-50% of seniors living in the community and 45-80% of long-term care residents Diagnosis of pain in the frail elderly can be complicated by cognitive impairment due to delirium or dementia, cultural barriers, vision and hearing loss, and inaccurate beliefs (“pain is an inevitable part of aging”) Feldt, 2005
 Feldt,")
148
Pain Diagnosis in cognitively-impaired adults is further complicated by the fact that when they are sitting quietly, they may forget they have pain and appear to be “just fine” Seniors with cognitive impairment (dementia or delirium) are often unable to recognize or describe their discomfort – in other words, they are unable to recognize their discomposure as pain and, therefore, may deny having pain or discomfort if asked, or they may describe their discomfort as “I hurt all over” Feldt, 2005
 are often unable to recognize or describe their discomfort – in other words, they are unable to recognize their discomposure as pain and, therefore, may deny having pain or discomfort if asked, or they may describe their discomfort as I hurt all over Feldt,")
149
Pain Studies have shown that, with cognitively impaired seniors, aggression, agitation or resistance to care can be related to untreated or poorly managed pain issues New behaviours such as aggression or agitation in seniors with dementia may indication an underlying infection or other medical imbalance which is causing discomfort (i.e., urinary tract infection, constipation, cardiac changes or prolonged discomfort from a fracture) Feldt, 2005
 Feldt,")
150
Pain The cognitively-impaired senior may deny discomfort and present with non-verbal symptoms such as: facial movements (grimacing, frowning, raising cheeks) Body movements (bracing, guarding, rubbing, touching) Vocalizations (moans, groans, yelling, shouting) Poor appetite Sleep disturbance Depressed mood Agitated behaviour Withdrawn Weepy Feldt, 2005
 Body movements (bracing, guarding, rubbing, touching) Vocalizations (moans, groans, yelling, shouting) Poor appetite. Sleep disturbance. Depressed mood. Agitated behaviour. Withdrawn. Weepy. Feldt,")
151
Pain If left untreated, pain issues can have serious consequences, including depression, isolation, sleep disturbance, impaired ambulation and slowed healing Treatment includes treating underlying medical issues, finding the right analgesic for the type of pain and the correct dosage Feldt, 2005

152
Sleep Issues Sleep issues are a common complaint amongst seniors, yet they are rarely diagnosed or treated, even by geriatric specialists – despite the fact that sleep disorders can have harmful effects on healthy aging “Sleep disturbances among the elderly are associated with significant morbidity and mortality and increase the risk for nursing home placement” McCall, 2004, p. 9

153
Sleep Issues “Sleep disturbances in the elderly, and the subsequent disruption of caregivers’ sleep, exact a toll on family support. Insomnia has been cited as a primary factor in caregivers’ decisions to institutionalize an elder, with … 52% of admissions to long-term care directly attributable to elderly sleep disturbance.” “A survey of 1855 elderly urban residents found that insomnia was the strongest predictor among males for both mortality and nursing home placement” McCall, 2004, p. 10

154
Sleep Issues Sleep disturbance can contribute to cognitive decline and, if unrecognized, becomes another factor that can impair accurate diagnosis of dementia (i.e., person gets a diagnosis of dementia, rather than insomnia and the sleep disorder goes unrecognized and untreated) Staying asleep is more of an issue with older adults than falling asleep McCall, 2004
 Staying asleep is more of an issue with older adults than falling asleep. McCall,")
155
Sleep Issues There are no guidelines regarding how much sleep is appropriate for older adults Even healthy seniors tend to spend more time resting in bed then younger adults, with no more time spent sleeping Studies show that older adults often spend more time in light sleep and less time in deep sleep than younger adults McCall, 2004

156
Sleep Issues Insomnia is often a “side effect” of chronic disease, poor physical health or psychosocial issues Sleep disturbance in the elderly is strongly correlated with depression McCall, 2004

157
Common Causes of Sleep Disturbance
Caffeine Nicotine Perscription drugs (beta blockers, decongestants, thyroid medications, corticosteroids, antidepressants, chemotherapy, benzodiazepenes Sleep disorders (sleep apnea, periodic limb movement disorder, nocturnal myoclonus, restless legs syndrome, circadian rhythm sleep disorder, rapid eye movement behavioural disorder)
")
158
Common Causes of Sleep Disturbance
Pain Neurological disease (Parkinson’s, Alzheimer’s) Chronic medical illness (arthritis, cardiovascular disease, gastrointestinal disease, asthma, COPD) Thyrotoxicosis Daytime napping Depression Anxiety Life stressors Bedtime worrying Mania or hypomania Environmental causes Noise Eating or exercise before bedtime
 Chronic medical illness (arthritis, cardiovascular disease, gastrointestinal disease, asthma, COPD) Thyrotoxicosis. Daytime napping. Depression. Anxiety. Life stressors. Bedtime worrying. Mania or hypomania. Environmental causes. Noise. Eating or exercise before bedtime.")
159
Treatment of Sleep Disturbance
Studies have shown that the use of sleep medications could be reduced by 74% if non-pharmacological sleep protocols are used on a regular basis, such as: back rubs warm drink relaxation tapes, etc. CHR

160
SAMPLE CASES

161
Case #1: A 78-year-old widow presents with insomnia
Case #1: A 78-year-old widow presents with insomnia. Her medical history includes hypertension, diabetes, possible Crohn’s disease, recurrent urinary tract infections, cataracts and bilateral knee replacement surgery a number of years ago. She denies any psychiatric history. Mrs. Smith lives alone in her own home. For the past five years, she has cared for her ailing husband, until his death one month ago. She admits that looking after him was a strain and, at times, she “could hardly stand it”. Since her husband’s death, she has stopped going to church and no longer socializes with friends. She is alert and oriented, but appears to be stressed. Her MMSE score is 25/30; she lost points on orientation and concentration. She denies feeling depressed, but scored 15/30 on the Geriatric Depression Scale Gall, Clinical Geriatrics

162
Case #2: Mr. Johnson is a 90-year old gentleman who lives at home with his wife. Mrs. Johnson has had health problems for many years and he has been her main caregiver. Mr. Johnson was admitted to hospital for further investigations following a fall. While in hospital, he was confused, resistive to care, rambling incoherently and did not recognize family members. Family were reassured that this was his “dementia”. Family were perplexed, as they had not noticed much confusion or serious cognitive impairment prior to his hospitalization. They were reassured that he had probably been “covering up” his deficits for some time. Family were told that Mr. Johnson was not safe to look after his wife. Therefore, the decision was made for long term care.

163
Case #3: An 82-year-old widow presents with memory problems and symptoms consistent with major depressive disorder. She is having difficulties with independent functioning, so admission to hospital is arranged for further work-up and treatment. Her medical issues include arthritis, hypothyroidism, glaucoma and NIDDM. Two months ago, she had a fall, resulting in a compression fracture, so Tylenol #3 is started for pain. Other medications include Synthroid, multivitamin and Pilocarpine eye drops. To treat the depressive features, an anti-depressant is also started. Not long after admission, she begins to complain of hearing music. Confusion and distress is evident – she claims she is about to give birth, blood is everywhere, the head is crowning. She appears to be restless and is awake throughout the night GMHCS

164
Case #4: Mr. Jones is an 87-year-old gentleman with mild dementia
Case #4: Mr. Jones is an 87-year-old gentleman with mild dementia. He had been through a difficult period of adjustment since his admission to the nursing home several months earlier. He wa critical of staff, impatient with his roommate and plagued by insomnia. One night at 3:00 am, he woke up, put his clothes on over his pajamas and went to the dining room for breakfast. When staff tried to orient him, he exploded in anger and accused them of trying to make him look like a fool. He refused to go back to bed and paced the halls until morning. Staff who changed his sheets noticed that, for the first time since admission, he had been incontinent of urine. On reviewing his chart, it was noted he had been started on Oxazepam for insomnia 5 days earlier. He was not cooperative with a physical exam and refused to answer mental status questions, complaining bitterly that this was an infringement of his rights. The oxazepam was discontinued. Two weeks later, however, Mr. Jones had deteriorated further. He appeared disheveled, swore at staff and shook his fist at them whenever they tried to approach him. During the afternoon he slept for hours and was difficult to rouse. He started complaining of bugs in his room GMHCS

165
CONCLUSIONS – WHAT TO KEEP IN MIND WHEN YOUR CLIENT IS A SENIOR

166
“Age is an issue of mind over matter
“Age is an issue of mind over matter. If you don’t mind, it doesn’t matter.” Mark Twain

167
It is extremely important to obtain an accurate picture
You need to get an accurate sense of what this senior was like before you met them so that you can determine whether there has been a sudden change While respecting privacy and confidentiality issues: gather collateral information from as many sources as possible (i.e., medical history – do they have a history of delirium, depression, UTI’s, etc.) Talk to different sources - the client, family members, supports in the community, etc. If possible, visit their home to get a better idea of what their day-to-day functioning is like
 Talk to different sources - the client, family members, supports in the community, etc. If possible, visit their home to get a better idea of what their day-to-day functioning is like.")
168
It is extremely important to obtain an accurate picture
Be aware of the potential for adverse cognitive effects/change in behaviour from many medications, infection, other medical imbalance, pain, constipation, poor nutrition, etc. Consider the signs and symptoms you are seeing in context with the senior’s history Don’t jump to conclusions!

169
Create opportunities for honest, sincere dialogue
Ask appropriate questions Be aware of your biases and society’s biases

170
Create opportunities for honest, sincere dialogue
Ask appropriate questions Be aware of your biases and society’s biases

171
They’re from a generation that never asked for help for anything
Most seniors – and their families – don’t know where to go for help, who to talk to or how to ask for help They’re from a generation that never asked for help for anything They’re also ashamed to admit they have a “problem”

172
Assess the capabilities of their existing support system
Refer to an appropriate professional for more thorough assessment, supportive counselling, etc.

173
Provide opportunities to discuss the benefits and risks of choices
Social workers can provide appropriate and accurate information to seniors and their family so they can make informed choices Provide opportunities to discuss the benefits and risks of choices

174
It may be necessary to have a competency assessment done.
You may encounter situations where a senior obviously needs help, yet refuses any type of support In such a situation, risk of harm (to self and others) needs to be properly assessed. It may be necessary to have a competency assessment done.
 needs to be properly assessed. It may be necessary to have a competency assessment done.")
175
If unsure what to do, discuss the case with other qualified personnel Health regions have ethics boards and most are more than willing to discuss a case If risk of harm to self or others is apparent, it may be necessary to complete a Form 1 to have the person committed to hospital or psychiatric service for assessment

176
Find out what resources are available for seniors in your community
Local Health Authority - Seniors’ Health Family physician (should know who to refer to for assessment, physician referral usually necessary for geriatric &/or psychiatric assessment) Alzheimer’s Society Community support agencies Grief support programs Competency assessment teams
 Alzheimer’s Society. Community support agencies. Grief support programs. Competency assessment teams.")
177
Local Health Authority - Seniors’ Health
Family physician (should know who to refer to for assessment, physician referral usually necessary for geriatric &/or Specialized Geriatric Services There are a number of geriatric services available. Clients seen within these services are typically frail, complex older adults who present with deterioration in their functional status. This deterioration may either be on a physical, cognitive or a mental health basis, or a combination of the three. These individuals generally have a number of underlying chronic conditions. The client’s family and support system are often included in the services offered. Components to the services include both inpatient and outpatient geriatric services. Referrals to any of the following services is centralized though a One Line Referral Service. Family physicians, Home Care Coordinators and others use a common referral form to access any one of these services. Referrals are triaged by Seniors Health professional staff. General information about these services is obtained by calling or Geriatric Consultation Services Substance Abuse in Later Life (SAILL) Mental Health Geriatric Team Alzheimer and Dementia Resource Clinic (ADRC) Calgary Fall Prevention Clinic Cognitive Assessment Clinic Carewest Day Hospital Carewest Comprehensive Community Care (C3) Inpatient geriatric assessment and rehabilitation units Inpatient geriatric consultation services Alzheimer’s Society Community support agencies Grief support programs
 Mental Health Geriatric Team. Alzheimer and Dementia Resource Clinic (ADRC) Calgary Fall Prevention Clinic. Cognitive Assessment Clinic. Carewest Day Hospital. Carewest Comprehensive Community Care (C3) Inpatient geriatric assessment and rehabilitation units. Inpatient geriatric consultation services. Alzheimer’s Society. Community support agencies. Grief support programs.")
178
Mental Health & Addictions Services
Geriatric Programs & Services Access Mental Health Calgary Health Region at Sunridge Mall Community Geriatric Mental Health Services Geriatric Mental Health Acute Inpatient, Unit 48 RGH Geriatric Mental Health Consulting Service Geriatric Mental Health Outreach Team Geriatric Rehabilitation & Recovery Unit South Calgary Health Centre Geriatric Services Educational Series For information on any of the services listed call Access Mental

179
Mental Health & Addictions Services
Rural Programs & Services Access Mental Health Airdrie Mental Health Clinic Black Diamond Mental Health Clinic Bow Valley Mental Health Clinic Chestermere Mental Health Clinic Claresholm Centre for Mental Health & Addictions Claresholm Mental Health Clinic Cochrane Mental Health Clinic Didsbury Mental Health Clinic High River Mental Health Clinic Nanton Mental Health Clinic Okotoks Mental Health Clinic Shared Mental Health Care, Rural South Strathmore Mental Health Clinic Vulcan Mental Health Clinic Rural South Community Mental Health Workshops For information on any services listed call Access Mental

180
Especially for Seniors Programs & Services
Capital Health has published a guide listing the programs and services it provides for seniors. For a copy of this pdf click here As well, we've gathered resources and links relating to the health information needs of seniors and their caregivers. Use the topic links below to browse for health information that interests you. Or find out about programs and services of interest to seniors by using the link to the right. Information is available on topics such as keeping fit, eating to stay healthy, and living safely at home. Additionally, there is information about some disorders and conditions that you might have questions about. Community Care Services provides an integrated system of health and personal support services to clients based on assessed need. Our services are provided in clients' homes, and through a variety of supportive living environments and continuing care facilities. Community Care Access The first point of contact is to call Community Care Access (known formerly as Information and Intake) at Community Care Access provides telephone screening and needs assessment 24 hours a day, seven days a week.
 at Community Care Access provides telephone screening and needs assessment 24 hours a day, seven days a week.")
181
Ensure you’re part of the solution, not part of the problem:
Deal with any issues presented by a senior, rather than ignoring them Be aware that seniors often feel disenfranchised, ignored and of little value in today’s society Talk about seniors and their plight whenever possible, in order to battle society’s general lack of awareness, lack of understanding, apathy, ambivalence and tendency to “put blinders on” whenever the issues of the elderly are mentioned

182
They also have the right to take risks
Remember: The elderly, like all other human beings, deserve the opportunity to live as comfortably and contentedly as possible They also have the right to take risks Even those seniors with advanced dementia can have their quality of life improved by proper care and attention Unlike younger adults, seniors are much more likely to need your help to ensure their needs are met

183
Therapies, etc. Reminiscence therapy Cognitive behavioural
Motivational interviewing Solution-focused

184
Bibliography Alexopoulos, G.B., et. al., Cornell Scare for Depression in Dementia, Biological Psychiatry, Vol. 23, 1988, pp Brink, T.L., et. al., Screening Test for Geriatric Depression, Clinical Gerontologist, Vol. 1, No. 1, 1982, pp Caine & Grossman, Neuropsychiatric Assessment, in Birren, Sloane & Cohen, eds., Handbook of Mental Health and Aging, 1992 Gallo, J.J., et. al., Handbook of Geriatric Assessment, Gaithersburg, MD: Aspecn Publications, 1995 Inouye, S.K., et. al., Clarifying Confusion: The Confusion Assessment Method – a New Method for Detection of Delirium, Annual of Internal Medicine, Vol. 113, pp McCall, W.V., Sleep Disturbance in the Elderly: Burden, Diagnosis, and Treatment, Primary Care Companion, Journal of Clinical Psychiatry, Vol. 6, No. 1, 2004, pp Molloy, W., Standardized Mini Mental State Examination, Ontario: New Grange Press, 1989 Orzech, D., Sensory Loss in Aging, Social Work Today, Vol. 7, No. 1, p. 20

185
Bibliography www.aafp.org American Academy of Family Physicians
Gallo, J.J. & Rabins, P.V., Depression Without Sadness: Alternative Presentations of Depression in Late Life, American Family Physician, September 1999 www. ajgponline.org American Journal of Geriatric Psychiatry wilkins, C.H., et. al., Vitamin D Deficiency is Associated with Low Mood and Worse Cognitive Performance in Older Adults, Vol. 14, December 2006, pp Alive Magazine (October 2007) Alzheimer’s Society of Canada A Report on Alzheimer’s Disease and Current Research (2006)
 Alzheimer’s Society of Canada A Report on Alzheimer’s Disease and Current Research (2006)")
186
Bibliography www.calgaryhealthregion.ca Calgary Health Region website
Mental Status Exam – learning module Clinical Geriatric Journal Gall, J.S. & Szwabo, P., Psychosocial Aspects of Aging Harvard Medical School Harvard Men’s Health Watch, Vol. 10, No. 10 (May 2006) Montreal Cognitive Assessment Tool (MoCA)
 Montreal Cognitive Assessment Tool (MoCA)")
187
Bibliography Public Health Agency of Canada, Aging and Seniors Statistics re seniors Healthy Aging in Canada: A New Vision, A Vital Investment, From Evidence to Action – A Background Paper Prepared for the Federal, Provincial and Territorial Committee of Officials (Seniors) Advance Online Editions for Directors in Rehabilitation Feldt, K.S., Pain in the Elderly, Issue date 10/3/2005 Registered Nurses Association of Ontario Screening for Delirium, Dementia and Depression in Older Adults, Nursing Best Practice Guidelines, November 2003 Caregiving Strategies for Older Adults with Delirium, Dementia and Depression in Older Adults, Nursing Best Practice Guidelines, November 2003
 Advance Online Editions for Directors in Rehabilitation. Feldt, K.S., Pain in the Elderly, Issue date 10/3/ Registered Nurses Association of Ontario. Screening for Delirium, Dementia and Depression in Older. Adults, Nursing Best Practice Guidelines, November Caregiving Strategies for Older Adults with Delirium, Dementia and Depression in Older Adults, Nursing Best. Practice Guidelines, November")
Similar presentations