Download presentation
Presentation is loading. Please wait.

1
DRUGS ACTING ON RAAS DR SHREETAL RAJAN NAIR

2
The Renin Angiotensin Aldosterone System (RAAS)
Most important neurohormonal system that maintains vascular tone and fluid-electrolyte balance in our body Is involved in the pathophysiology of most cardiovascular diseases and hence its importance Works through a negative feedback loop in our body

3
Pathophysiology of RAS

5
Factors stimulating renin release
Low arterial blood pressure Decreased sodium concentration in the distal tubule Decreased blood volume Increased beta -1 sympathetic activity

7
Drugs influencing PRA Increasing PRA ACEI ARBs Vasodilators Diuretics
Decreasing PRA Adrenergic blockers Renin inhibitors

10
DRUGS ACTING ON RAAS ACE Inhibitors Angiotensin receptor blockers
Aldosterone antagonists Renin inhibitors New therapeutic pathways

11
ACE Inhibitors

12
Historical aspects ACE was initially discovered from the venom of pit viper and named bradykinin potentiating factor and later it was found that this kininase and ACE were the same. Teprotide was the first ACEI to be synthezised But it had limitations Later , captopril was developed as the first ACEI in 1977

13
ACEI ACE inhibitors differ
in the chemical structure of their active moieties, in potency, in bioavailability, in plasma half-life, in route of elimination, in their distribution and affinity for tissue-bound ACE, and in whether they are administered as prodrugs.

14
ACE Inhibitors CLASSIFICATION Class I : Containing a sulfhydryl group
- Captopril ( proline derivative) Class II : Prodrugs Class III : Water soluble - Lisinopril ( Lysine derivative )
 Class II : Prodrugs. Class III : Water soluble. - Lisinopril ( Lysine derivative )")
15
ACEI Captopril is the prototype of the sulfhydryl-containing ACE inhibitors; others are fentiapril, pivalopril, zofenopril, and alacepril. In vitro studies suggest that the presence of the sulfhydryl group may confer properties other than ACE inhibition to these drugs, such as free-radical scavenging and effects on prostaglandins In vivo no much benefit has been found

16
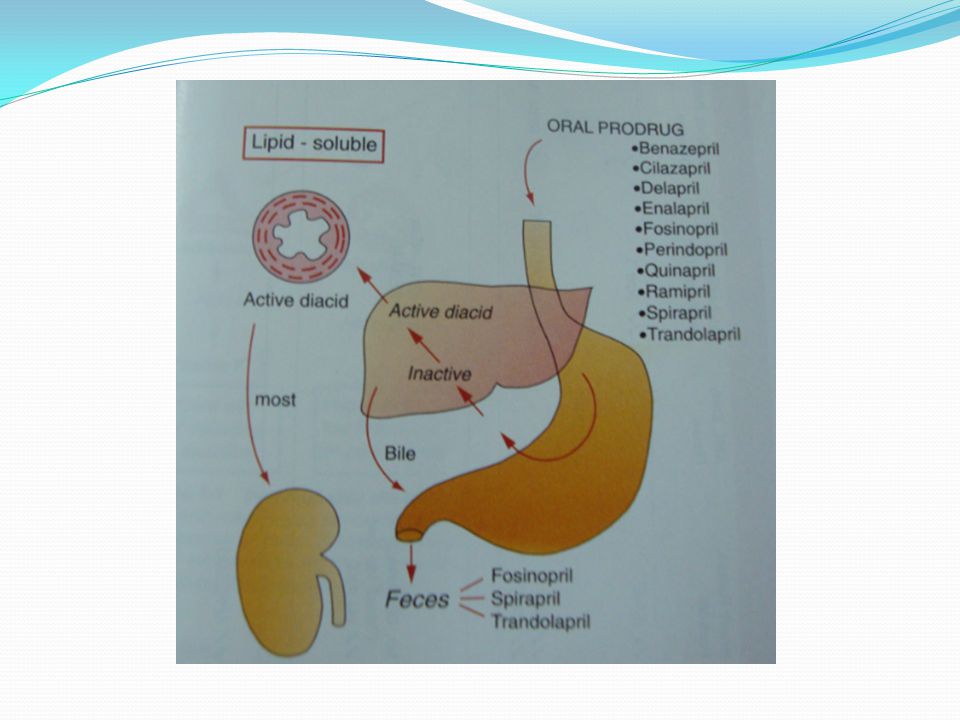
ACEI – salient features
Captopril by itself is active and its metabolites are also active Prodrugs by itself are not active and need to be converted to the active diacids in the liver and prodrugs have better bioavailability Lisinopril is active and is not metabolised and excreted unchanged All ACEI are excreted exclusively via renal system except fosinopril,spirapril and trandolapril which are excreted via the biliiary system and feces.

18
ACEI – salient features
Bioavailability : highest – captopril; least – perindopril Most prodrugs are carboxyl derivatives except fosinopril Time to peak action – fastest captopril ( 1 hr) Elimination t ½ - longest with ramipril (8-48 hrs) ACEI with duration of action > 24 hrs : enalapril,lisinopril,ramipril and perindopril Captopril is the only ACEI to cross BBB but its clinical significance is unknown
 Elimination t ½ - longest with ramipril (8-48 hrs) ACEI with duration of action > 24 hrs : enalapril,lisinopril,ramipril and perindopril. Captopril is the only ACEI to cross BBB but its clinical significance is unknown.")
19
ACEI – pharmacokinetics in a nut shell
Nancy J. Brown, MD; Douglas E. Vaughan, MD Circulation. 1998;97:

21
ACEI- hemodynamic effects
ACEI are beneficial in many ways Prevents generation of angiotensin II Useful in conditions in which the renin angiotensin system is dysregulated like essential hypertension and renovascular hypertension Decreases the peripheral vascular resistance Fall in systolic and diastolic BP No effect on cardiac output

22
INDICATIONS OF ACEI 1. Heart failure
Chronic heart failure due to any cause 2. AMI Early phase AMI with HF 3. Hypertension 4. Chronic Renal Disease 5. Diabetic nephropathy 6. Risk prevention

23
ACEI – other indications
Non – cardiovascular Diabetic and non- diabetic nephropathy Scleroderma crisis ( captopril test to diagnose renovascular hypertension )
")
25
Adverse effects

26
Adverse effects First dose hypotension more in diuretic treated patients Hyperkalemia more in patients with impaired renal function and those taking potassium sparing diuretics and NSAIDs Cough : occurs in patients within 1-8 weeks ; subsides in 7-21 days after discontinuation ;not dose related- earlier it was believed to be due to inhibition of bradykinin degradation; now it is believed to be mediated by substance P as kininase II is also believed to be degrade substance P. More in women

27
Adverse effects Angioedema: the pathogenesis is found to be similar to the cough; cough and angioedema found in higher incidence in those concomitantly using DPP IV inhibitors as DPP is also responsible for substance P breakdown. Rashes,urticaria: do not need drug stoppage Dysguesia is a reversible alteration in the taste sensation – found in captopril treated patients and believed to be due to the sulfhydryl moiety

28
ADAPTED from www./spo.escardio.org/eslides

29
Adverse effects Granulocytopenia and proteinuria very rare but warrant withdrawal Headache,dizziness ,nausea and bowel upset- in 1-4 % ARF in bilateral RAS due to dilatation of efferent arterioles and fall in GFR and hence contraindicated Fetopathic effects- 1st trimester produces cardiovascular malformations ( PDA ) and 2nd and 3rd trimester responsible for oligohydramnios, fetal calvarial hypoplasia, fetal pulmonary hypoplasia, fetal growth retardation, fetal death, neonatal anuria, and neonatal death and hence contraindicated in pregnancy.
 and 2nd and 3rd trimester responsible for oligohydramnios, fetal calvarial hypoplasia, fetal pulmonary hypoplasia, fetal growth retardation, fetal death, neonatal anuria, and neonatal death and hence contraindicated in pregnancy.")
30
Interactions NSAIDs especially in elderly, taking diuretics and ACEI
Potassium sparing diuretics/ on K+ supplements Antacids decrease absorption Reduce Lithium clearance and predispose to toxicity in those taking lithium Caution in Impaired renal function, hypovolemia or dehydration

31
Contraindications Bilateral RAS Pregnancy Hyperkalemia
Known allergy or hypersensitivity Serum creatinine (>2.5 – 3.0 mg/dl ) arbitrary cut off in patients with heart failure
 arbitrary cut off in patients with heart failure.")
32
Pharmacogenomics Found to be less effective in young and elderly blacks because are found to have less PRA. Adding drugs which increase PRA like diuretics have found to increase response to therapy An insertion (I)/deletion (D) polymorphism in the ACE gene that correlates with ACE activity such that ACE levels are highest in patients who are homozygous for the ACE D allele, lowest in patients homozygous for the ACE I allele, and intermediate in those who are heterozygous . Persons with the D/D phenotype had subdued response to the ACEI Angioedema more in whites.
/deletion (D) polymorphism in the ACE gene that correlates with ACE activity such that ACE levels are highest in patients who are homozygous for the ACE D allele, lowest in patients homozygous for the ACE I allele, and intermediate in those who are heterozygous . Persons with the D/D phenotype had subdued response to the ACEI. Angioedema more in whites.")
33
Some new concepts in ACE inhibition
ACE inhibitors have also been shown to cause a central enhancement of parasympathetic nervous system activity in healthy volunteers and patients with heart failure. This action may reduce the prevalence of malignant cardiac arrhythmias, and the reduction in sudden death . The ACE inhibitor enalapril has also been shown to reduce cardiac cachexia in patients with chronic heart failure. Cachexia is a poor prognostic sign in patients with chronic heart failure

34
Some new concepts in ACE inhibition
ACE inhibitors are under early investigation for the treatment of frailty and muscle wasting (sarcopenia) in elderly patients without heart failure The lactotripeptides Val-Pro-Pro and Ile-Pro-Pro produced by the probiotic Lactobacillus helveticus or derived from casein have been shown to have ACE-inhibiting and antihypertensive functions ( discovered in Japan IN 1991)
 in elderly patients without heart failure. The lactotripeptides Val-Pro-Pro and Ile-Pro-Pro produced by the probiotic Lactobacillus helveticus or derived from casein have been shown to have ACE-inhibiting and antihypertensive functions ( discovered in Japan IN 1991)")
36
ACEI in heart failure Panel A- ACEI in HF with depressed EF in a post AMI metaanalysis Panel B – ACEI in HF with depressed EF including postinfarction trials (metaanalysis) Benefit from therapy is seen very early and persisted long term
 Benefit from therapy is seen very early and persisted long term.")
37
Omapatrilat Omapatrilat was a novel antihypertensive agent that inhibits both neutral endopeptidase (NEP) and angiotensin converting enzyme (ACE). NEP inhibition results in elevated natriureticpeptide levels, promoting natriuresis, diuresis, vasodilation, and reductions in preload and ventricular remodeling. This was being promoted for CHF but was not approved by the FDA due to angioedema safety concerns

38
Omapatrilat - trials The OVERTURE (Omapatrilat Versus Enalapril Randomized Trial of Utility in Reducing Events) study: Omapatrilat was as good as enalapril but not better In the OCTAVE (Omapatrilat Cardiovascular Treatment Assessment Versus Enalapril) study 25,267 hypertensives were randomised to Omapatrilat or enalapril and a difference of approximately 3 mmHg in favour of Omapatrilat was seen. Significantly more cases of angioedema were seen with Omapatrilat in both trials.
 study 25,267 hypertensives were randomised to Omapatrilat or enalapril and a difference of approximately 3 mmHg in favour of Omapatrilat was seen. Significantly more cases of angioedema were seen with Omapatrilat in both trials.")
39
IMPRESS randomised trial
Comparison of vasopeptidase inhibitor, omapatrilat, and lisinopril on exercise tolerance and morbidity in patients with heart failure Showed a trend in favour of omapatrilat

40
Angiotensin receptor blockers (ARBs)
")
41
ARBs The ARBs act on the next step in RAAS and they block the angiotensin II receptor through which angiotensin II exerts its effects Why the need of ARBs arose after ACEI ? Clinical and experimental studies showed the initial suppression of angiotensin II after the administration of angiotensin-converting enzyme (ACE) inhibitors is later reversed and returns almost to pretreatment levels. The ESCAPE phenomenon was hypothesized which was strengthened by the discovery that angiotensin II can also be generated through non-ACEs Increased incidence of adverse effects with ACEI therapy
 inhibitors is later reversed and returns almost to pretreatment levels. The ESCAPE phenomenon was hypothesized which was strengthened by the discovery that angiotensin II can also be generated through non-ACEs. 2. Increased incidence of adverse effects with ACEI therapy.")
42
Advantages of ARBs over ACEI
Do not interfere with degradation of bradykinin and other ACE substrates More complete inhibition of AT1 receptor activation Indirect activation of AT2 receptor Other molecular effects apart from the receptor action

43
Losartan was the first ARB to be synthezised and it was a imidazole derivative
All ARBs expect for losartan are highly selective for the AT1 receptor. In fact, ARBs show 10,000–30,000 times greater affinity for the AT1 receptor than for the AT2 receptor The majority of ARBs produce insurmountable antagonism ( non competitive inhibition )
")
44
What is the advantage of AT1 receptor specificity ?
AT2 receptor may be exposed to a higher concentration of Ang II It increases the Ang II-induced AT2 receptor stimulation which may cause anti-cell proliferation and vasodilation

45
Other effects of ARBs Inverse agonism of AT1 receptor
Anti platelet effects Anti – inflammatory effects Reduction in serum uric acid levels

47
Benefits of Inverse agonism
1. Sometimes AT1 receptors are mutated and have constitutive activity which means the receptors can get activated in the absence of its ligand Constitutive has also been found in wild type receptors Losartan,valsartan,olmesartan and candesartan have significant inverse agonism

48
Benefits of inverse agonism
2. AT1 receptor mRNA levels are upregulated by myocyte stretching over time Studies have demonstrated that the AT1 receptor is activated by the mechanical stretching of cultured rat myocytes and constriction of the transverse aorta in angiotensinogen knockout mice without the involvement of Ang II, and these adverse effects were suppressed by an inverse agonist

49
Anti platelet effects Losartan has some degree of antagonistic action on the thromboxane A2 receptor which is responsible for the platelet antiaggregatory effects

50
Anti inflammatory effects
Ang II induces inflammation in vasculature and vascular remodeling, and subsequently promotes atherosclerosis. Ang II stimulates monocyte chemoattractant protein-1 (MCP-1), interleukin (IL)-8, tumor necrosis factor-a and IL-6 production Decrease in MCP-1 levels seen with irbesartan and losartan Increase in adiponectin expression seen with irbesartan,losartan,candesartan and telmisartan
, interleukin (IL)-8, tumor necrosis factor-a and IL-6 production. Decrease in MCP-1 levels seen with irbesartan and losartan. Increase in adiponectin expression seen with irbesartan,losartan,candesartan and telmisartan.")
51
Anti inflammatory effects
PPAR gamma activation with eprosartan – may be one reason of preventing New Onset Diabetes(NOD), the other being increased adiponectin levels Irbesartan and olmesartan act as antagonists of chemokine receptors Actions are independent of actions on the AT1 and AT2 receptors and suggest a molecular level of action for the ARBs
, the other being increased adiponectin levels. Irbesartan and olmesartan act as antagonists of chemokine receptors. Actions are independent of actions on the AT1 and AT2 receptors and suggest a molecular level of action for the ARBs.")
52
Decrease in uric acid levels
Compared with other ARBs, losartan, telmisartan and irbesartan have been shown to reduce serum uric acid. These effects are believed to be mediated at the molecular levels independent of action on the AT1 receptor

53
In a nut shell Angiotensin II type 1 receptor blockers: class effects versus molecular effects Shin-ichiro Miura, Sadashiva S. Karnik and Keijiro Saku -Journal ofthe Renin-Angiotensin-Aldosterone System (Including other Peptidergic systems) March 2011 Volume 12 Number 1
 March 2011 Volume 12 Number 1.")
54
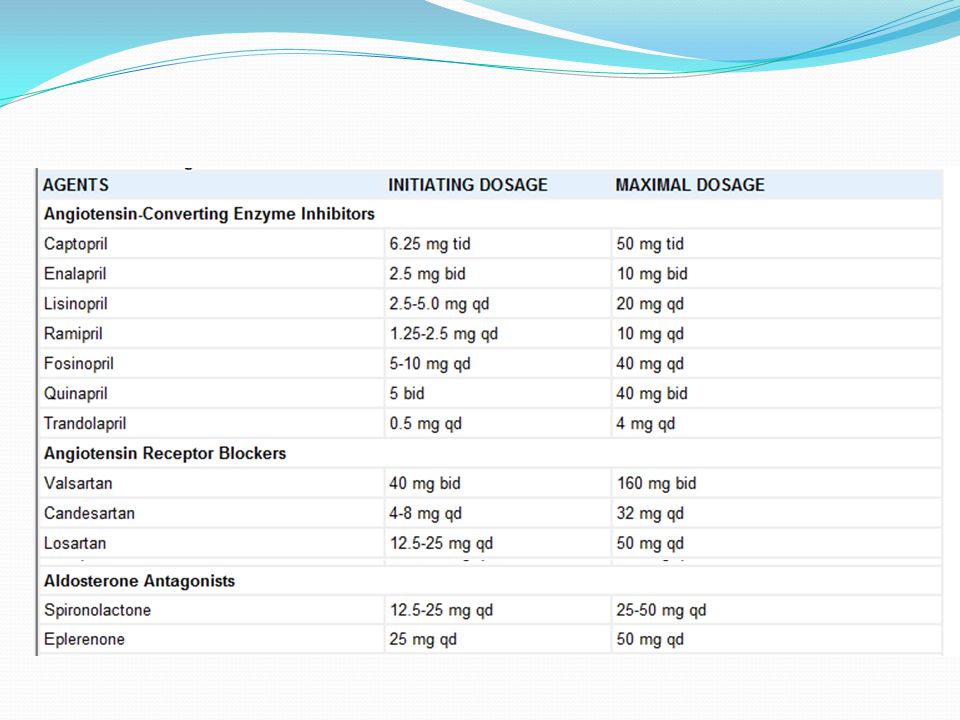
ARB in hypertension

56
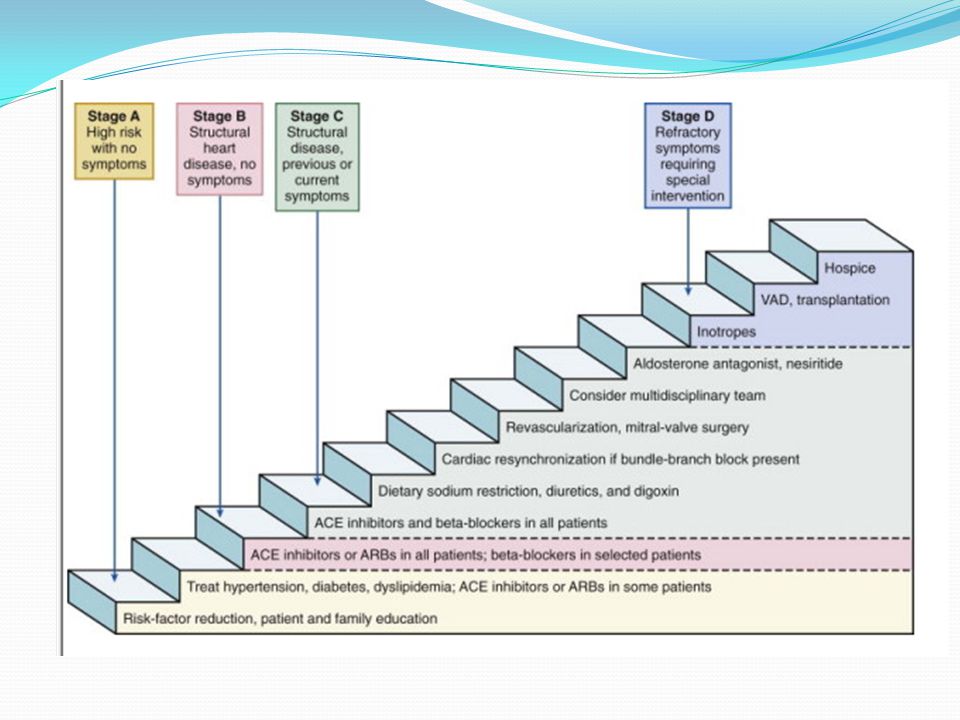
ACC/AHA recommendations (2005)
")
58
The concept of dual RAAS blockade with ACEI and ARB
Arose because of the phenomenon of escape phenomenon with ACEI To achieve complete and more effective blockade of Angotensin action It was combining ACEI and ARB would be of benefit but studies did not give promising results Now dual ACEI and ARB therapy not recommended except in non- diabetic renal disease -(COOPERATE,2003 trial showed progression of non diabetic renal disease retarded to a greater extent than with monotherapy.

59
Some salient features of ARBs
Highest affinity for AT1 receptor – candesartan Longest duration of action - telmisartan All ARBs need dose reduction in liver diseases

60
Adverse effects Similar to ACEI except
Less incidence of first dose hypotension Cough , angioedema , dysguesia incidence less

61
Interactions Similar to that with ACEI

62
T cells and angiotensin II induced hypertension
T cells, which express AT1 receptors and NADPH oxidase, may play an important role in the genesis of A II–dependent hypertension, particularly obesity-related hypertension, as the activated T cells are selectively sequestered in adipose tissue. Homing of activated T cells to perivascular fat promotes vasoconstriction and vascular remodeling. Homing of activated T cells to perinephric fat promotes renal dysfunction and sodium retention

63
The ARB- MI paradox – a controversy unresolved
The major ARB trials in high-risk patients have thus far demonstrated almost a complete lack of reduction in MI and mortality despite significant reductions in blood pressure. Paradoxically, rates of MI in some trials have actually increased with ARBs, which suggests that ARBs and ACEIs may exert distinctive effects on both the coronary circulation and atherosclerotic plaque stability This unexpected relationship of ARBs with MI may be aptly described as the “ARB-MI paradox.” Martin H. Strauss and Alistair S. Hall: Angiotensin Receptor Blockers May Increase Risk of Myocardial Infarction : Unraveling the ARB-MI paradox ; Circulation. 2006;114: ; LIONEL H. OPIE and BERNARD J GERSH : DRUGS FOR THE HEART ; 7 Edition 2009

64
Aldosterone antagonists

65
Role of aldosterone in CV disease
Direct correlation of aldosterone levels and mortality in heart failure Increase in myocardial fibrosis Inhibition of the release of NO Increased incidence of arrhythmias Increased response to vasoconstrictor doses of angiotensin I Critical mediator of early angiotensin II induced experimental myocardial injury

66
Deleterious effects of aldosterone

67
Aldosterone antagonists
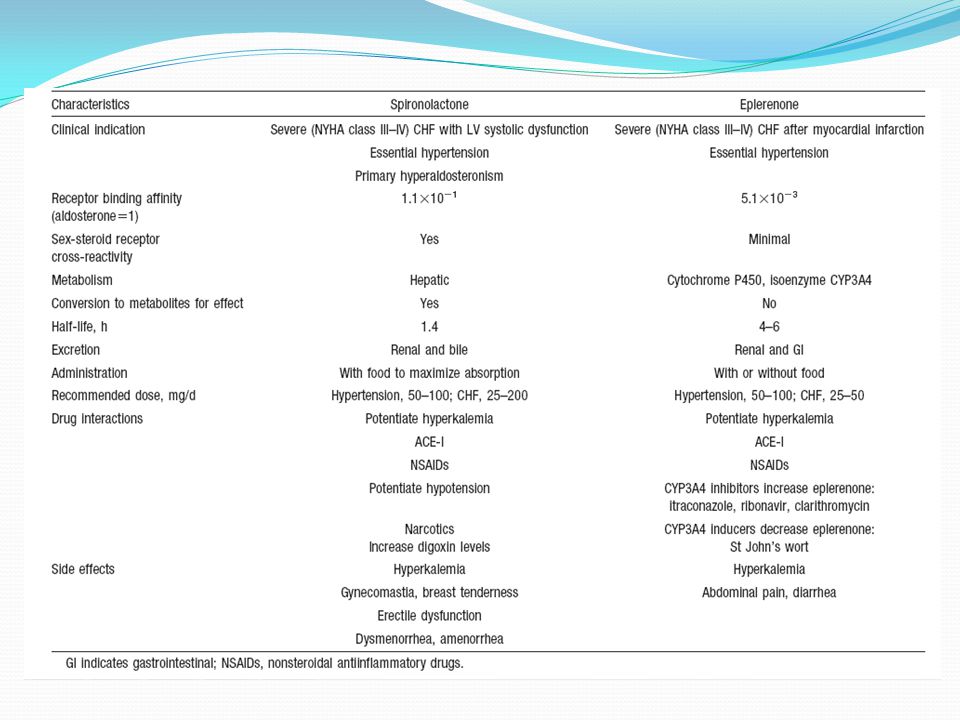
Spironolactone Eplerenone Canrenone ( available only in europe)
")
68
What do they do? Decrease extracellular markers of fibrosis
Decreases the release of cardiac norepinephrine Vasodilator effects

69
Spironolactone- mechanism of action
It is a steroid chemically related to aldosterone Competitive inhibition of the mineralocorticoid receptor from the interstitial side of the tubular cell Inhibits formation of (Aldosterone induced proteins) AIPs
 AIPs.")
71
Spironolactone Spironolactone acts as an antagonist and/or agonist at the following sites: Antagonism Mineralocorticoid receptor Androgen receptor Agonism Progesterone receptor Glucocorticoid receptor

72
Spironolactone bodies
Long-term administration of spironolactone gives the histologic characteristic of spironolactone bodies in the adrenal cortex. Spironolactone bodies are eosinophilic, round, concentrically laminated cytoplasmic inclusions surrounded by clear halos in preparations stained with hematoxylin and eosin

73
Contraindications Hyperkalemic states
Pregnancy - high risk of feminisation of female fetuses

74
Pharmacokinetics 75% oral bioavailability
Highly bound to plasma proteins Completely metabolised in the liver Active metabolite canrenone ( ½ - 2/3rd of action in vivo is due to this metabolite) Half life of spironolactone is 1-2 hours; canrenone is 18 hours
 Half life of spironolactone is 1-2 hours; canrenone is 18 hours.")
75
Indications Hypertension
To improve survival of stable patients with LV systolic dysfunction ( EF </= 40% ) Clinical evidence of CHF after AMI Refractory edema in cirrhosis and renal disease – helps to breakdown resistance to thiazide diuretics due to secondary hyperaldosteronism To counteract K+ loss due to thiazide and loop diuretics
 Clinical evidence of CHF after AMI. Refractory edema in cirrhosis and renal disease – helps to breakdown resistance to thiazide diuretics due to secondary hyperaldosteronism. To counteract K+ loss due to thiazide and loop diuretics.")
76
Interactions Dangerous hyperkalemia can occur if given with K+ supplements or drugs causing hyperkalemia ( ACEI or ARBs) Aspirin blocks action of spironolactone by inhibiting tubular secretion of canrenone Spironolactone increases plasma digoxin concentration

77
Adverse effects Drowsiness , confusion and abdominal discomfort
Hirsutism,gynecomastia,impotence and menstrual irregularities Hyperkalemia especially in renal disease Risk of acidosis in cirrhotics

78
Eplerenone More selective aldosterone antagonist
Less likely to cause hormonal disturbances like gynecomastia,impotence and menstrual irregularities

79
EPLERENONE Starting dose 25 mg daily increased to 50 mg daily if serum potassium < 5.0 mEq/L If serum K+ is > 5.5 mEq/L then the dose must be decreased or discontinued Specific warning in T2DM with hypertension and microalbuminuria because of the risk of hyperkalemia Dose for hypertension ; mg once daily Equally effective in white and black patients.

81
Trial data – aldosterone antagonists
Aldosterone antagonists (or mineralocorticoid receptor antagonists [MRAs]) are guideline-recommended therapy for patients with moderate to severe heart failure (HF) symptoms and reduced left ventricular ejection fraction (LVEF), and in postmyocardial infarction patients with HF.
 are guideline-recommended therapy for patients with moderate to severe heart failure (HF) symptoms and reduced left ventricular ejection fraction (LVEF), and in postmyocardial infarction patients with HF.")
82
Trial data RALES,TOPCAT ( spironolactone)
EPHESUS ; EMPHASIS-HF ; 4E ( eplerenone) AREA IN CHF ( canrenone )
 AREA IN CHF ( canrenone )")
83
The Eplerenone in Mild Patients Hospitalization and Survival Study in Heart Failure (EMPHASIS-HF)
Eplerenone reduced the risk of the primary endpoint of cardiovascular death or HF hospitalization (hazard ratio [HR] 0.63, 95% confidence interval [CI] , P < .001) and all-cause mortality (adjusted HR 0.76, 95% CI , P < .008) after a median of 21 months
 and all-cause mortality (adjusted HR 0.76, 95% CI , P < .008) after a median of 21 months.")
84
The Randomized Aldactone Evaluation Study(RALES)
Eplerenone Post-Acute Myocardial Infarction Heart Failure Efficacy and Survival Study (EPHESUS) established that spironolactone and eplerenone, respectively, increased survival in patients with severe CHF symptoms from LV systolic dysfunction occurring with minimal exertion or at rest (New York Heart Association [NYHA] class III or IV) or CHF after an acute myocardial infarction
 established that spironolactone and eplerenone, respectively, increased survival in patients with severe CHF symptoms from LV systolic dysfunction occurring with minimal exertion or at rest (New York Heart Association [NYHA] class III or IV) or CHF after an acute myocardial infarction.")
85
THE 4E STUDY The 4E Study (Eplerenone,Enalapril, and Eplerenone/Enalapril Combination Therapy in Patients with Left Ventricular Hypertrophy) compared the effects of 9-month treatment with eplerenone 200 mg/d (n=64), enalapril 40 mg/d (n=71), or eplerenone 200 mg/d plus enalapril 10 mg/d (n= 67) on LV mass, systolic and diastolic blood pressures, and urinary albumin-creatinine ratio (UACR) in patients with mild-to-moderate hypertension and echocardiographic evidence of LVH. Combination therapy with eplerenone and enalapril significantly reduced LV mass
 compared the effects of 9-month treatment with eplerenone 200 mg/d (n=64), enalapril 40 mg/d (n=71), or eplerenone 200 mg/d plus enalapril 10 mg/d (n= 67) on LV mass, systolic and diastolic blood pressures, and urinary albumin-creatinine ratio (UACR) in patients with mild-to-moderate hypertension and echocardiographic evidence of LVH. Combination therapy with eplerenone and enalapril significantly reduced LV mass.")
86
Ongoing trial TOPCAT study (Treatment of Preserved Cardiac
Function Heart Failure With an Aldosterone Antagonist)- is ongoing At this time, however, there are insufficient clinical data to recommend the use of aldosterone antagonist therapy for the treatment of diastolic dysfunction.
- is ongoing. At this time, however, there are insufficient clinical data to recommend the use of aldosterone antagonist therapy for the treatment of diastolic dysfunction.")
87
Anti-remodelling effect of canrenone in patients with mild chronic heart failure (AREA IN-CHF study): To test whether canrenone, an aldosterone receptor antagonist, improves left ventricular (LV) remodelling in NYHA class II heart failure (HF). Aldosterone receptor antagonists improve outcome in severe HF, but no information is available in NYHA class II. Canrenone on top of optimal treatment for HF did not have additional effects on LVEDV, but it increased EF, and reduced left atrial size and circulating BNP, with potential beneficial effects on outcome
 remodelling in NYHA class II heart failure (HF). Aldosterone receptor antagonists improve outcome in severe HF, but no information is available in NYHA class II. Canrenone on top of optimal treatment for HF did not have additional effects on LVEDV, but it increased EF, and reduced left atrial size and circulating BNP, with potential beneficial effects on outcome.")
88
Direct renin inhibitors

89
DRI- Historical aspects
The concept of blocking the RAAS at its origin by inhibiting renin has existed for at least 50 years. The first synthetic renin inhibitor was pepstatin, which was followed by first-generation agents that were active but required parenteral administration Oral agents that were subsequently developed, such as enalkiren,remikiren, and zankiren, had limited clinical use because they demonstrated poor bioavailability (< 2%), short half-lives, and weak antihypertensive activity
, short half-lives, and weak antihypertensive activity.")
90
Aliskiren Aliskiren is the first synthetic non peptide direct renin inhibitor (DRI) to be approved by the U.S. Food and Drug Administration and the European Medicines Agency for treating hypertension in 2007. Aliskiren binds to the active site (S1/S3 hydrophobic binding pocket) of renin, preventing the conversion of angiotensinogen to angiotensin I
 to be approved by the U.S. Food and Drug Administration and the European Medicines Agency for treating hypertension in Aliskiren binds to the active site (S1/S3 hydrophobic binding pocket) of renin, preventing the conversion of angiotensinogen to angiotensin I.")
91
Aliskiren Binding to Renin
Aliskiren bound to Active site Wood et al. BBRC 2003.

92
ALISKIREN named after ALICE HUXLEY

93
Aliskiren - pharmacokinetics
Direct renin inhibitor 50 – 80 % decrease plasma renin activity Pharmacokinetics Accumulation Half-life of ~ 24 hours Oral bioavailability of 2.6% 7 – 8 days to achieve steady state levels Elimination Half-life of ~ 48 hours 25 % excreted by kidneys Metabolized by CYP 450-3A4 Does not induce or suppress CYP 450 No effect on QT interval

94
Aliskiren – pharmacokinetics
Pathway of elimination for aliskiren is via biliary excretion as unmetabolized drug. Less than 1% of an orally administered dose is excreted in urine. Not metabolized by, and does not induce or inhibit, cytochrome P450 enzymes and shows no clinically relevant pharmacokinetic interactions with warfarin, lovastatin, atenolol,celecoxib,cimetidine,amlodipine,valsartan,hydrochlorothiazide (HCTZ), or ramipril. The pharmacokinetics of aliskiren remain unaffected by ethnicity, age, gender, hepatic impairment, renal impairment, and diabetes.
, or ramipril. The pharmacokinetics of aliskiren remain unaffected by ethnicity, age, gender, hepatic impairment, renal impairment, and diabetes.")
95
Drug interactions It reduces furosemide blood concentration.
Atorvastatin may increase blood concentration, but no dose adjustment is needed. Due to possible interaction with ciclosporin, the concomitant use of ciclosporin and aliskiren is contraindicated. Aliskiren is a minor substrate of CYP3A4 and, more important, P-glycoprotein Caution should be exercised when aliskiren is administered with ketoconazole or other moderate P-gp inhibitors (itraconazole, clarithromycin, telithromycin, erythromycin, or amiodarone). Doctors should stop prescribing aliskiren-containing medicines to patients with diabetes (type 1 or type 2) or with moderate to severe kidney impairment who are also taking an ACE inhibitor or ARB, and should consider alternative antihypertensive treatment as necessary
. Doctors should stop prescribing aliskiren-containing medicines to patients with diabetes (type 1 or type 2) or with moderate to severe kidney impairment who are also taking an ACE inhibitor or ARB, and should consider alternative antihypertensive treatment as necessary.")
96
Adverse effects Angioedema
Hyperkalemia (particularly when used with ACE inhibitors in diabetic patients) Hypotension (particularly in volume-depleted patients) Diarrhea and other GI symptoms Headache, Dizziness Cough Rash Elevated uric acid, gout, and renal stones
 Hypotension (particularly in volume-depleted patients) Diarrhea and other GI symptoms. Headache, Dizziness. Cough. Rash. Elevated uric acid, gout, and renal stones.")
97
Potential therapeutic roles of aliskiren
Monotherapy for hypertension Component of combination therapy for hypertension, with a diuretic, a CCB, an ACEI, and/or an ARB Alternative to ACEIs or ARBs in the management of hypertension and the prevention of organ damage Alternative to ACEIs in patients with diabetic nephropathy or cardiovascular disease Use in patients with diabetic nephropathy or in African American hypertensive patients, in whom intrarenal angiotensin II formation occurs via ACE or non–ACE-dependent pathways

98
ali

99
ATMOSPHERE (Efficacy and Safety of Aliskiren and Aliskiren/Enalapril Combination on Morbi-mortality in Patients With Chronic Heart Failure) study Aliskiren is currently being evaluated in a phase III study that will evaluate the efficacy and safety of both aliskiren monotherapy and aliskiren-enalapril combination therapy as compared with enalapril monotherapy in regard to cardiovascular death and heart failure hospitalizations in NYHA Classes II to IV HF patients

101
Aldosterone antagonists

102
Role of aldosterone in CV disease
Direct correlation of aldosterone levels and mortality in heart failure Increase in myocardial fibrosis Inhibition of the release of NO Increased incidence of arrhythmias Increased response to vasoconstrictor doses of angiotensin I Critical mediator of early angiotensin II induced experimental myocardial injury

103
Deleterious effects of aldosterone

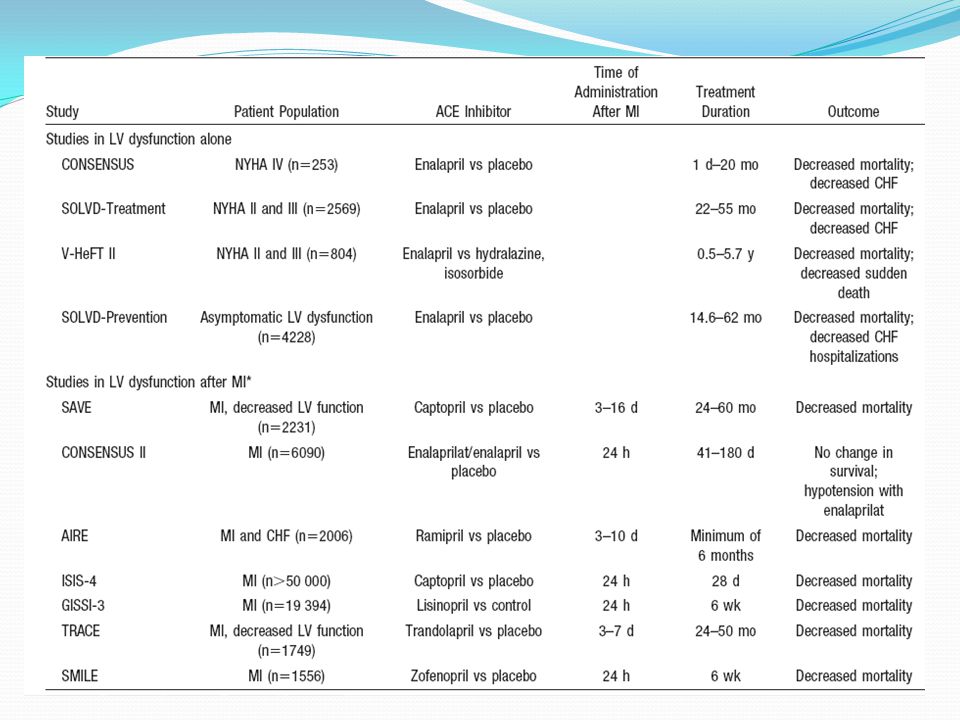
104
Major outcome trials of RAAS inhibitors with favourable evidence
Trials in post MI HF ACEI – SAVE (Captopril), AIRE (Ramipril ), TRACE (Trandolapril) ARB – VALIANT (Valsartan ) Aldosterone antagonists ( EPHESUS)
, AIRE (Ramipril ), TRACE (Trandolapril) ARB – VALIANT (Valsartan ) Aldosterone antagonists ( EPHESUS)")
105
Major outcome trials of RAAS inhibitors with favourable evidence
Trial in AMI – Early phase GISSI – lisinopril. Trials in cardiovascular risk prevention ACEI : EUROPA (perindopril), HOPE( ramipril), PEACE( trandolapril) ARBs : ONTARGET ( Telmisartan)
, HOPE( ramipril), PEACE( trandolapril) ARBs : ONTARGET ( Telmisartan)")
106
New therapeutic pathways in ACE inhibition

107
Biased AT1 receptor blockade
A very novel development in the field of ARBs is the concept of “biased” AT1-receptor blockade. Biased ARBs block AT1-receptor-coupled G-protein signalling in the “traditional” way, while simultaneously stimulating β-arrestin-coupled signalling which, for example, results in improved cardiac function. TRV is the first biased ARB in clinical development and is currently being evaluated in a phase II clinical study for the treatment of heart failure.

108
AT1-receptor blockade combined with neutral endopeptidase inhibition
NEP is responsible for the degradation of atrial and brain natriuretic factor, which both have cardioprotective properties. Consequently, inhibition of NEP increases plasma levels of these protective molecules. LCZ696, which may become the first in class ARNI (AT1-receptor and NEP inhibitor) lowered blood-pressure more effectively than valsartan monotherapy in a phase II clinical trial. Phase III clinical trials are currently ongoing to test LCZ696 for the treatment of heart failure. Outcomes of these studies and data about long-term safety (potential risks for obesity, Alzheimer’s disease and angioedema have been discussed) have to be awaited
 lowered blood-pressure more effectively than valsartan monotherapy in a phase II clinical trial. Phase III clinical trials are currently ongoing to test LCZ696 for the treatment of heart failure. Outcomes of these studies and data about long-term safety (potential risks for obesity, Alzheimer’s disease and angioedema have been discussed) have to be awaited.")
109
Novel therapies AT1-receptor blockade combined with endothelin A receptor blockade RE-021 is a dual AT1-receptor and endothelin-A receptor (ETA) antagonist which was successfully taken through a phase IIb study in patients in hypertension . It has potential for use in FSGS AT1-receptor blockade combined with nitric oxide (NO) release is in the pipeline
 antagonist which was successfully taken through a phase IIb study in patients in hypertension . It has potential for use in FSGS. AT1-receptor blockade combined with nitric oxide (NO) release is in the pipeline.")
110
Novel therapies AT2 RECEPTOR AGONISTS
potential use in post-myocardial infarction (MI) cardiac function,hypertension-induced vascular remodelling, pulmonary hypertension), neurological (e.g. stroke, spinal cord injury, Alzheimer’s disease) and immunological (e.g. multiple sclerosis, rheumatoid arthritis) diseases AT2 RECEPTOR ANTAGONISTS in post herpetic pain ANGIOTENSIN 1-7 analogues and special formulations in hypertension, post-MI cardiac failure, metabolic syndrome, diabetes, renal disease and RA Recombinant ACE2 and ACE2 formulations
 cardiac function,hypertension-induced vascular remodelling, pulmonary hypertension), neurological (e.g. stroke, spinal cord injury, Alzheimer’s disease) and immunological (e.g. multiple sclerosis, rheumatoid arthritis) diseases. AT2 RECEPTOR ANTAGONISTS in post herpetic pain. ANGIOTENSIN 1-7 analogues and special formulations in hypertension, post-MI cardiac failure, metabolic syndrome, diabetes, renal disease and RA. Recombinant ACE2 and ACE2 formulations.")
Similar presentations















 Garrett J. Gross, Ph.D. Drugs Used In the Treatment of Congestive Heart Failure(Cont) Garrett.>")
 Renin-Angiotensin System Important for its role in hypertrophy, inflammation, remodelling and apoptosis Binding of renin or pro-renin to.>")











