Download presentation
Presentation is loading. Please wait.

1
California STD/HIV Prevention Training Center
Diseases without Borders: Best Practices for Sexually Transmitted Diseases Care and Prevention Linda Creegan, MS, FNP California STD/HIV Prevention Training Center Border Conference El Centro, CA June 2014

2
I do not have any financial arrangements or affiliations with commercial sponsors which have direct interest in the subject matter:

3
Sexually Transmitted Diseases
Chlamydia Chancroid HPV Gonorrhea Trichomonas Genital herpes Syphilis Granuloma inguinale Lice HIV / AIDS Scabies LGV Hepatitis B BV? M. genitalium Hepatitis C Others…..

4
Complications of STDs Infection Chlamydia Gonorrhea HPV Hepatitis B
PID Infertility Ectopic pregnancy Chronic pain Cancer Perinatal Congenital infection Low birth weight Stillbirth HIV Brain/organ damage Chlamydia Gonorrhea HPV Hepatitis B Trichomonas HSV Syphilis

5
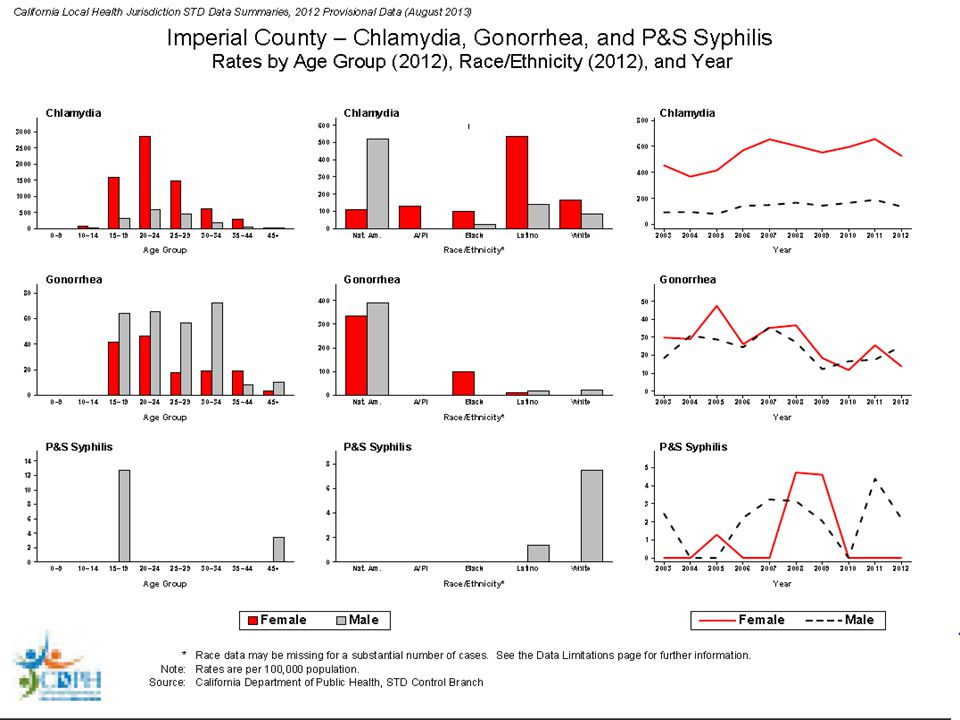
CA STD Data and Statistics

7
Priority Populations Teens & young people Pregnant women
Gay/Bi men (MSM) People of color
 People of color.")
8
Testing in STD Care Testing applications Types of tests Case finding
Asymptomatic (screening) Symptomatic (diagnostic) Follow-up Guide treatment (HIV resistance testing) Surveillance Types of tests Culture (susceptibility testing) Serologic tests (antibodies in the blood) Molecular-based tests (NAAT) Combo tests CT/GC HIV/syphilis Non-treponemal and treponemal
 Symptomatic (diagnostic) Follow-up. Guide treatment (HIV resistance testing) Surveillance. Types of tests. Culture (susceptibility testing) Serologic tests (antibodies in the blood) Molecular-based tests (NAAT) Combo tests. CT/GC. HIV/syphilis. Non-treponemal and treponemal.")
9
Testing Approaches In clinic Outside the clinic Clinician-collected
Self-collected Outside the clinic Collected at lab Field-based program Home testing

10
Provide Those Free Sexual Health Services!
Essential Health Benefits related to STD/HIV prevention and care Must be included in all health plans at no cost-sharing to patient Annual Wellness visit STD and HIV screening STD and HIV care HPV and Hep B Immunizations Risk Reduction counseling Pap smears Essential health benefits must be included in all insurance packages available in the state insurance exchanges, so these will be benefits that all patients can receive. And of course these are billable services, so when these reproductive health services are provided to patients in your practice, they will be reimbursable.

11
1. Ask three essential sexual history questions
WHO are your partners? WHAT are your sexual and drug use practices? HOW do you try to prevent STDs/HIV? It all begins with a sexual history or risk assessment. A very brief risk assessment can give you a pretty good idea of the level of this patient’s risk for STIs. With all patients, hit just 3 topics as a screen Any current protocol/ practice re: sexual risk assessment? Including self-administered forms that pts fill out? Adolescent and adult history forms both on paper that patients complete and electronic history in EHR. Risk assessment important since many STDs are asymptomatic

12
2. Screen for Chlamydia and Gonorrhea
ALL sexually active adolescent and young women ≤ 25 years Pregnant women Men who have sex with men (MSM) Persons living with HIV Others according to risk CDC 2010 STD Tx Guidelines.
 Persons living with HIV. Others according to risk. CDC 2010 STD Tx Guidelines.")
13
Why screen? Highly prevalent Frequently asymptomatic
Reduces transmission Prevents complications HEDIS measure: chlamydia screening in females under 25 years old Standard of care

14
STD Screening for Women
Sexually Active adolescents & up to age 25 Routine chlamydia and gonorrhea screening Others STDs and HIV based on risk Women over 25 years of age STD/HIV testing based on risk Pregnant women Chlamydia Gonorrhea (<25 years of age or risk) HIV Syphilis serology HepB sAg Hep C (if high risk) CDC 2010 STD Tx Guidelines
 HIV Syphilis serology HepB sAg Hep C (if high risk) CDC 2010 STD Tx Guidelines")
15
Estimated Chlamydia Screening Coverage (HEDIS), Females Age 15–24, USA and California, 1999–2010
National California Source: National Committee on Quality Assurance; California DHCS Division of Medi-Cal Managed Care; Kaiser Permanente Northern CA; California DPH Office of Family Planning Rev. 4/2012

16
Who is falling through the cracks?
Visits that do not require an exam Pregnancy test only Emergency contraception Contraception method follow-up Refills Depo-provera injection So who are we missing, who is falling thru the cracks? Well, women who come for a clinic visit that does not require an exam. CT screening is pretty much routine at annual exams, but many women come for other types of visits which may be the only time we see them for care. And for these women, we’re much less likely to remember to do a CT test.

17
A pelvic exams is not necessary to obtain a chlamydia test
Nucleic acid amplification tests (NAATs) Highest sensitivity Noninvasive samples Urine Self-collected vaginal swabs A pelvic exam isn’t necessary to obtain the sample for a CT test. NAAT tests using urine or vaginal swab samples are in widespread use now. So the urine we get for that pregnancy test can be sent for a CT test as well.
 Highest sensitivity. Noninvasive samples. Urine. Self-collected vaginal swabs. A pelvic exam isn’t necessary to obtain the sample for a CT test. NAAT tests using urine or vaginal swab samples are in widespread use now. So the urine we get for that pregnancy test can be sent for a CT test as well.")
18
Major conclusions NAATs recommended for detection of genital tract infections in men and women – with and without symptoms Optimal specimen types are: First catch urine for men Self collected vaginal swabs from women NAATs recommended for: detection of rectal and oropharyngeal infections

19
CT Test Volume & Prevalence among Females by Age
What about Women over age 25? CT Test Volume & Prevalence among Females by Age 50% Test Volume This slide graphically depicts the problem we face in CA – namely the over-screening that is occurring within the low prevalence population of FP women over age 25. This graph shows 2006 CT test volume and prevalence data by age group for women tested for CT via CA’s F-PACT program (F-PACT, or “Family PACT”, is a CA entitlement program which provides comprehensive reproductive health care to low income female and male residents of the state). The red line in this graph represents a CT prevalence of 3%, the state’s cost-effective cut-off for universal screening, which was chosen based on research of the 1) literature, 2) statewide surveillance data, and 3) our current level of resources in CA. . CT prevalence drops below this line in the groups of women age 25 and older. Yet, the CT test volume remains quite high across these older age groups, with 50% of all Family-PACT chlamydia testing occurring in the population of women over age 25. This practice of screening older adult women with a CT prevalence lower than the cost-effective level is not an effective use of the limited resources we have in CA. CA FPACT Data, 2006 *Quest Diagnostics/Unilab: West Hills/Tarzana, Sacramento, San Jose
. The red line in this graph represents a CT prevalence of 3%, the state’s cost-effective cut-off for universal screening, which was chosen based on research of the 1) literature, 2) statewide surveillance data, and 3) our current level of resources in CA. . CT prevalence drops below this line in the groups of women age 25 and older. Yet, the CT test volume remains quite high across these older age groups, with 50% of all Family-PACT chlamydia testing occurring in the population of women over age 25. This practice of screening older adult women with a CT prevalence lower than the cost-effective level is not an effective use of the limited resources we have in CA. CA FPACT Data, *Quest Diagnostics/Unilab: West Hills/Tarzana, Sacramento, San Jose.")
20
Which women over age 25 should be screened?
Based on risk: Infection with CT or GC in past 2 years > 1 sex partner in past 12 months New partner in past 3 months Belief that a partner in the past 12 months may have had other sex partners at the same time Other indications: Pregnancy Contact to STD New STD diagnosis CA CT Screening Guidelines Draft; Howard et al. Over 20. In prep.

21
STI Screening Recommendations: HIV-positive Men & Women
Anatomic Site Chlamydia Genital, rectal if exposed Gonorrhea Genital, rectal & oral if exposed Syphilis Serology Trichomoniasis Women only HSV-2 Hep B sAg Hep C * * Screen at least annually; repeat screening every 3-6 months as indicated by risk. MSM- Consider anal Pap screening Women-Cervical Pap screening; Consider anal Pap if hx of dysplasia. Primary Care Guidelines for the Management of Persons Infected with HIV: 2009 Update by the HIVMA of the IDSA. Clin Infect Dis 2009;49,

22
STD Screening for MSM * HIV Syphilis Urethral GC and CT
Rectal GC and CT (if RAI) Pharyngeal GC (if oral sex) HSV-2 serology (consider) Hepatitis B (HBsAg) Anal Pap (consider for HIV+) * * At least annually, more frequent (3-6 months) if at high risk (multiple/anonymous partners, drug use, high risk partners) CDC 2010 STD Tx Guidelines
 Pharyngeal GC (if oral sex) HSV-2 serology (consider) Hepatitis B (HBsAg) Anal Pap (consider for HIV+) * * At least annually, more frequent (3-6 months) if at high risk (multiple/anonymous partners, drug use, high risk partners) CDC 2010 STD Tx Guidelines")
23
Majority of Rectal Infections in MSM are Asymptomatic
86% 84% Chlamydia Gonorrhea n=316 n=264 Asymptomatic Urethral Infections Symptomatic 10% 42% Chlamydia Gonorrhea n=315 n=364 Kent, CK et al, Clin Infect Dis July 2005

24
Proportion of CT and GC infections MISSED among 3398 asymptomatic MSM if screening only urine/urethral sites, San Francisco, Chlamydia Gonorrhea Marcus et al, STD Oct 2011; 38: 922-4

25
Chlamydia and Gonorrhea NAA Testing
…not FDA-cleared for rectal or pharyngeal specimens but now the preferred testing method over culture Validation procedures can be done by labs to allow use of a non-FDA-cleared test or application Quest & LabCorp currently provide GC/CT NAAT for rectal/pharyngeal specimens

26
NAAT Laboratory Ordering and Billing Codes
For information on specimen collection and transportation, clinicians should contact the local reference laboratory representative. *CDC does not endorse these laboratories, however, they represent the largest laboratories nationally. There may be other private laboratories that have verified rectal and pharyngeal testing with NAATs. Many PHLs have also verified rectal and pharyngeal testing. Bolan, CDC webinar March 2011

27
Case Scenario 22 year old female Asymptomatic, no prior STDs
STD Screening done on intake No known drug allergies GC positive CT negative

28
What regimen would you use to treat Gonorrhea?
Ceftriaxone 250 mg IM Azithromycin 2 gm PO Ceftriaxone 250 mg IM plus azithromycin 1 gm PO Ceftriaxone 125 mg IM plus azithromycin 1gm PO

29
Development of GC Resistance
1930s-1970s 1980s 1990s 2000s 2010s 1976: Pen-R NG first identified in US (in CA) 2002: Fluoroquinolones no longer recommended for TX by CA 1945: Penicillin first used widely for TX 2001: First cephalosporin TX failures in Japan 1986: GISP started by CDC 1991: QRNG first identified in US (in HI) 2010: Dual TX recommended for TX by CDC 1936: Sulfanilamides introduced as TX 1989: Penicillin no longer recommended for TX by CDC 2007: Fluoroquinolones no longer recommended for TX by CDC
 2002: Fluoroquinolones no longer recommended. for TX by CA. 1945: Penicillin first used widely for TX. 2001: First cephalosporin TX failures in Japan. 1986: GISP started by CDC. 1991: QRNG. first identified. in US (in HI) 2010: Dual TX. recommended. for TX by CDC. 1936: Sulfanilamides introduced as TX. 1989: Penicillin no longer recommended for TX by CDC. 2007: Fluoroquinolones no longer recommended for TX by CDC.")
30
Who is most likely to be affected by cephalosporin-resistant GC?
Men who have sex with men California 30

31
3. Use Current Treatment for Gonorrhea
[Insert Lecture Name Here] 3. Use Current Treatment for Gonorrhea Gonorrhea Treatment: Uncomplicated Genital/Rectal/Pharyngeal Infections Azithromycin 1 g orally ** or Doxycycline 100 mg BID x 7 days Ceftriaxone 250 mg IM in a single dose PLUS* * Regardless of CT test result **Azithromycin preferred as 2nd antimicrobial MMWR Weekly August 10, 2012 MMWR updates CDC 2010 Guidelines Slide 31

32
Do you have ceftriaxone and azithromycin available onsite?
Yes No

33
Gonorrhea Treatment Alternatives Anogenital Infections
ALTERNATIVE CEPHALOSPORINS: Cefixime 400 mg orally once PLUS Dual treatment with azithromycin 1 g (preferred) or doxycycline 100 mg BID x 7 days, regardless of CT test result IN CASE OF SEVERE ALLERGY: Azithromycin 2 g orally once (Caution: GI intolerance, emerging resistance) Proposed in case of allergy: gentamicin 240 mg IM + azithromycin 2g orally or gemifloxacin 320 mg orally + azithromycin 2g orally MMWR / 61(31);
 or doxycycline 100 mg BID x 7 days, regardless of CT test result. IN CASE OF SEVERE ALLERGY: Azithromycin 2 g orally once. (Caution: GI intolerance, emerging resistance) Proposed in case of allergy: gentamicin 240 mg IM + azithromycin 2g orally or gemifloxacin 320 mg orally + azithromycin 2g orally. MMWR 2012 / 61(31);")
34
Test of Cure Current TOC recommendation: Test of cure in 1 week for anyone treated w/ alternative regimens Routine TOC poses implementation challenges No data on TOC positivity rates in absence of symptoms Proposed: Limit TOC only to pharyngeal GC treated with alternative regimen, may extend interval to 14 days

35
How to slow the spread of A-R Gonorrhea
New antibiotics Multiple antibiotics Surveillance Rapid response plans Resistance testing of isolates

36
Suspected GC Treatment Failure What should I do? CDPH Recommendations
CULTURE: if GC culture not available on-site, call CA STD Control Branch for resources REPEAT TREATMENT: Ceftriaxone 500 mg IM PLUS Azithromycin 2 g orally in a single dose* REPORT: To your local health department within 24 hours; call STD Control Branch if consult desired TREAT PARTNERS: All partners in last 60 days should be treated with CTX 500 mg + AZ 2g TEST OF CURE (TOC): Patient returns in 1 week for TOC with culture (if culture not avail, with NAAT) * If reinfection suspected instead of treatment failure, OK to repeat treatment with CTX AZ 1g
: Patient returns in 1 week for TOC with culture (if culture not avail, with NAAT) * If reinfection suspected instead of treatment failure, OK to repeat treatment with CTX AZ 1g.")
37
4. Ensure Partner Management
Patient referral Ask patient to notify partner and ensure treatment Suggest patient bring partner to clinic for concurrent treatment (“BYOP”) Internet-based anonymous notification Expedited partner treatment (EPT) Patient-delivered partner treatment (PDPT) Health department field-delivered treatment Pharmacy-based Provider or clinic-based referral Health department referral
 Internet-based anonymous notification. Expedited partner treatment (EPT) Patient-delivered partner treatment (PDPT) Health department field-delivered treatment. Pharmacy-based. Provider or clinic-based referral. Health department referral.")
38
Legal Status of EPT in the U.S.
PERMISSIBLE 32 states UNCERTAIN 11 states PROHIBITED 7 states CDC EPT Legal Status Updated August 2012

39
Online Partner Referral
Patients use website to notify partners - anonymous - free - referrals for testing inspot.org sotheycanknow.org

40
Nadine 28 y/o non-pregnant female treated for CT
Nadine 28 y/o non-pregnant female treated for CT. When should you schedule her follow-up? 1 week for a TOC 3 weeks for a TOC 3 months for a test for reinfection 1 year for her annual exam Not sure

41
5. Retest for CT and GC at three months following treatment
Retesting Recommendations: Retest all women and men with CT or GC months after treatment* “Opportunistic” testing Retest whenever possible, 1-12 mo *CDC 2010 STD Tx Guidelines,

42
Repeat Chlamydial Infection is Common
Typical Screening Prevalence Retesting Hosenfeld C, et al. Sex Transm Dis Aug;36(8):478-89
:")
43
Repeat Infection is Dangerous
Repeat CT infection leads to higher risk of complications: PID, ectopic pregnancy, infertility Most infections are asymptomatic Relative Risk Hillis SD, et al. (1997). Am J Obstet Gynecol 176(1 Pt 1):
. Am J Obstet Gynecol 176(1 Pt 1):")
44
Chlamydia Care Continuum: Family PACT females age ≤25 years (N=686,327)
Total Est Cases Cases detected Cases treated 78% 92% Pt returns 1-6 mo. retested 60% Pos at Restest 59% Source: Family PACT Annual Report FY

45
Getting clients back in for retesting:
Counseling at treatment visit Written materials Advance appointments Traditional reminder systems (telephone and postcards) Text message and/or reminders Downer SR et al Aust Health Rev 2006;30:389; Leong KC et al. Fam Pract 2006; 23:699.
 Text message and/or reminders. Downer SR et al Aust Health Rev 2006;30:389; Leong KC et al. Fam Pract 2006; 23:699.")
46
Appointment and STI Retest Reminders
For more information:

47
6. Recommend the HPV Vaccine
Population ACIP Recommendation Gender Age Females 11-12 (as young as 9) Routine vaccination with either HPV4 or HPV2 13-26 Routine catch-up vaccination either HPV4 or HPV2* Males Routine vaccination w HPV4 13-21 Routine catch-up vaccination HPV4 22-26 Permissive recommendation HPV 4 MSM & HIV+ Males Routine catch-up vaccination HPV 4 Available now? At all of our many clinic sites. b. What funding sources (VFC, various insurance, private pay) VFC and/or coverage for CHDP-approved and managed Medi-Cal programs. Utilization of the Merck program for many of our clients in our community clinic setting when not covered and with insufficient income. c. Any idea of uptake? When offered and covered, the general acceptance, especially when framed as a cancer-preventative vaccine, is encouragingly high, even among children of relatively conservative parents presenting during CHDP physicals, which was not always the case. d. Any problems they have encountered? I am unaware of any problems with stock availability or reported adverse effects other than localized site tenderness * Irrespective of history of abnormal Pap, HPV, genital warts MMWR, May ; 59(20): , MMWR , December ; 60(50);
 Routine vaccination with either HPV4 or HPV Routine catch-up vaccination either HPV4 or HPV2* Males. Routine vaccination w HPV Routine catch-up vaccination HPV Permissive recommendation HPV 4. MSM & HIV+ Males. Routine catch-up vaccination HPV 4. Available now At all of our many clinic sites. b. What funding sources (VFC, various insurance, private pay) VFC and/or coverage for CHDP-approved and managed Medi-Cal programs. Utilization of the Merck program for many of our clients in our community clinic setting when not covered and with insufficient income. c. Any idea of uptake When offered and covered, the general acceptance, especially when framed as a cancer-preventative vaccine, is encouragingly high, even among children of relatively conservative parents presenting during CHDP physicals, which was not always the case. d. Any problems they have encountered I am unaware of any problems with stock availability or reported adverse effects other than localized site tenderness. * Irrespective of history of abnormal Pap, HPV, genital warts. MMWR, May ; 59(20): , MMWR , December ; 60(50);")
48
The HPV Family Mucosal HPVs (~40 types) Dermal HPVs Common skin warts
I’ll start by providing an overview of human papillomavirus family. Currently, there are over 100 types of HPV. These HPVs can be separated into those that infected skin, also called dermal types, that cause common skin warts, and those that infect mucosal tissue, including genital and oral areas. Mucosal HPVs are transmitted through intimate and sexual contact. The genital HPV types can be further subdivided into high-risk types and low-risk types depending on their ability to cause cancer. “Low-risk” Wart types “High-risk” Cancer types

49
Incidence of Cervical HPV Detection in Women from the Time of Sexual Debut
0% 10% 20% 30% 40% 50% 60% 70% 6 12 18 24 30 36 42 48 Cervical HPV Detection Cohort study of 242 women with <= 1 lifetime partner followed for 48 months to assess incident HPV infection (PCR) Cervical HPV infection was assessed using highly sensitive PCR tests. By 4 years post sexual debut, over 60% of women were infected with HPV, demonstrating just how common HPV is. The median time from the first sexual experience to HPV detection was only 3 months. Time since first intercourse (months) Collins et al. Br J Obstet Gynecol 2002;109:96
 Cervical HPV infection was assessed using highly sensitive PCR tests. By 4 years post sexual debut, over 60% of women were infected with HPV, demonstrating just how common HPV is. The median time from the first sexual experience to HPV detection was only 3 months. Time since first intercourse (months) Collins et al. Br J Obstet Gynecol 2002;109:96.")
50
Clearance of HPV Infections Over 2 Years
Percent HPV Infected On this graph you can see how quickly HPV infection goes away on its own without treatment. The line follows the clearance of HPV infections over 2 years. These data are from a study of young women infected with HPV who were tested multiple times for about 24 months. As you can see, by 2 years, 90% of women infected with HPV, completely cleared their infection. The median persistence of any specific HPV type was only about 6 months. HPV infection clears as a result of a healthy immune response which then provides type-specific protection from reinfection for at least 10 years. Time from HPV infection (months) Adapted from Brown et al. JID 2005:191;182
 Adapted from Brown et al. JID 2005:191;182.")
51
Low Risk Mucosal HPVs TYPES Most common: 6, 11
Others: 40, 42, 43, 44, 54, etc DISEASES Genital and oral warts Respiratory papillomatosis Low grade cervical Pap abnormalities The most common low risk mucosal HPV types are 6 and 11, which account for about 90% of genital warts. These HPVs can cause genital and oral warts, respiratory papillomatosis, an infection of the vocal cords in infants exposed at birth, and low grade cervical abnormalities on Pap tests. I’ll let you know here that the next 2 slides contain graphic pictures of the some of the diseases caused by low risk HPV types.

52
Anogenital Warts Source: DOIA Website, 2000

53
HPV Vaccine Efficacy in Preventing Precancer and Warts
HPV Disease HPV 4 HPV 2 FEMALES CIN 2+ 98% Genital Warts 100% --- VIN/VaIN 2+ MALES Genital warts 90% AIN 78% CIN = Cervical Intraepithelial Neoplasia AIN = Anal Intraepithelial Neoplasia VIN = Vulvar Intraepithelial Neoplasia VaIN = Vaginal Intraepithelial Neoplasia Future II Study Group. N Engl J Med 2007;356(19): Garland SM et al. NEJM 2007;356(19): Paavonen et al. Lancet. 2009;374(9686):301-14 Giuliano et al. NEJM 2011; 364:401-11 Palefsky et al. NEJM 2011; 365:
: Garland SM et al. NEJM 2007;356(19): Paavonen et al. Lancet. 2009;374(9686): Giuliano et al. NEJM 2011; 364: Palefsky et al. NEJM 2011; 365:")
54
ACIP Recommendations: Administration, Precautions and Contraindications
Synchronized dosing: 3-dose schedule, second dose at 1-2 months after first dose, third dose 6 months after first dose Minimum intervals: Minimum time b/w 1st & 2nd = 4 wks Minimum time b/w 2nd & 3rd = 12 wks Minimum time b/w 1st & 3rd = 24 wks If schedule is interrupted, the series does not need to be restarted HPV vaccines can be given simultaneously/before/after other vaccines If possible, the same product should be used for all doses in the series No change in cervical cancer screening recommendations MMWR, May 28, 2010; 59(20): ,
: ,")
55
ACIP Recommendations: Administration, Precautions and Contraindications
Pregnancy: HPV vaccines are not recommended for use in pregnant women; however pregnancy testing is not needed before vaccination. Any exposure to vaccine during pregnancy should be reported to the appropriate vaccine pregnancy registry: Pregnancy Registry: (Merck) or (GSK vaccine) Contraindications: allergy to vaccine component, severe illness Quadrivalent HPV vaccine contains yeast antigens Bivalent HPV vaccine in prefilled syringes contraindicated for persons with anaphylactic latex allergy Adverse reactions should be reported to VAERS: or MMWR, May 28, 2010; 59(20): ,
 or (GSK vaccine) Contraindications: allergy to vaccine component, severe illness. Quadrivalent HPV vaccine contains yeast antigens. Bivalent HPV vaccine in prefilled syringes contraindicated for persons with anaphylactic latex allergy. Adverse reactions should be reported to VAERS: or MMWR, May 28, 2010; 59(20): ,")
56
Vaccine Funding Programs
Vaccines for Children Program Up to age 18, Medicaid eligible, uninsured or underinsured Receiving immunizations through a Federally Qualified Health Center or Rural Health Clinic, or Native American or Alaska Native Merck Vaccine Assistance Program Age ≥ 19, low income, and no health insurance coverage Phone number (8a-8p EST) Merck Dose Replacement Program Vaccine doses provided but not reimbursed GSK Vaccines Access Program Age 19-25, income eligible, and no heath insurance
 Merck Dose Replacement Program. Vaccine doses provided but not reimbursed. GSK Vaccines Access Program. Age 19-25, income eligible, and no heath insurance.")
57
HPV Vaccine Uptake, Girls Ages 13-17
National Immunization Survey, 49% 44% 37% 25% MMWR 2008 / 57(40):1100-3; MMWR 2009 / 58(36): ; MMWR 2010 / 59(32): ; MMWR 2011 / 60(33):
:1100-3; MMWR 2009 / 58(36): ; MMWR 2010 / 59(32): ; MMWR 2011 / 60(33):")
58
7. Offer Management for Recurrent/Persistent Vaginitis
Challenges in Managing Vaginitis Patient factors Self-treatment may preclude diagnosis Clients seek help from multiple providers Provider factors Under-utilization of available tests Insensitive clinic-based tests Dependent on provider skills

59
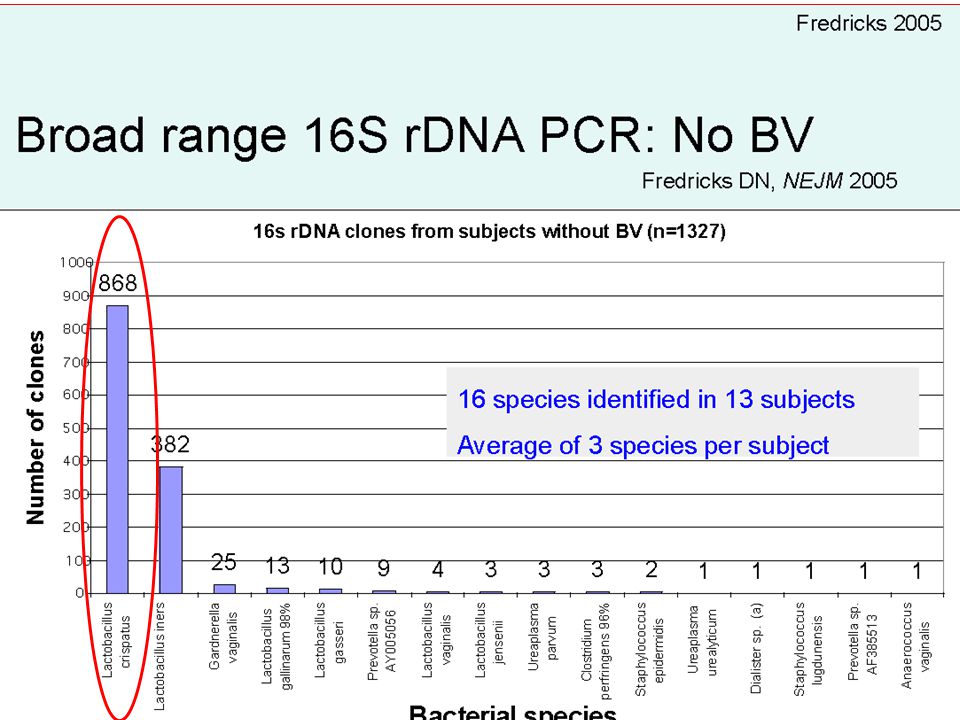
Bacterial Vaginosis Decrease in lactobacilli
Polymicrobial overgrowth Enzymes degrade the protective effects of cervical mucus and immune factors Most common cause of vaginitis Sequelae SAb, PROM, PTL, PTD Increases susceptibility to HIV, HSV, trich Pathogenesis is unclear; Recurrence is common Is BV an infection? What is the microbial cause? What is the association with sexual activity? Photo: Seattle PTC

62
Bev….. “I have BV again!” Recurrence rates as high as 30% at 3 months and 80% at 9 months Etiology unclear Resistance? Re-infection? Unrecognized trigger? Failure of lactobacilli to recolonize? Management Confirm diagnosis Condoms No douching Intermittent metronidazole gel (twice a week intravaginally)
")
63
Recurrent BV: Success with Suppressive Treatment
Recurrence MTNZ Placebo P value Prophylactic phase (4 mo) Clinical 13/51 (26%) 26/44 (59%) <.001 Gram Stain 8/45 (18%) 14/35 (40%) .03 Observation phase (3 mo) Clinical 26/51 (51%) 33/44 (75%) .02 Gram Stain 17/45 (38%) 17/35 (49%) .33 Sobel JD et al, Am J ObGyn. May 2006
 Clinical. 13/51 (26%) 26/44 (59%) <.001. Gram Stain. 8/45 (18%) 14/35 (40%) .03. Observation phase (3 mo) Clinical. 26/51 (51%) 33/44 (75%) .02. Gram Stain. 17/45 (38%) 17/35 (49%) .33. Sobel JD et al, Am J ObGyn. May")
64
Candice……. Majority of women have no predisposing or underlying conditions Non-albicans more common Pathogenesis is unclear Deficient host response? Overactive host response? Relapse/reinfection? Photos; Mosby STD Atlas 1997 and Seattle STD/HIV PTC Initial Treatment Longer regimen of topical therapy (7-10 d) Fluconazole (100 mg, 150 mg, or 200 mg) p.o. every 3rd d x 3 Maintenance Regimens Fluconazole (100 mg, 150 mg, 200 mg) qw x 6 m OR if not feasible Topical antifungals used intermittently
 Fluconazole (100 mg, 150 mg, or 200 mg) p.o. every 3rd d x 3. Maintenance Regimens. Fluconazole (100 mg, 150 mg, 200 mg) qw x 6 m. OR if not feasible. Topical antifungals used intermittently.")
65
Trixie….. CDC Consult & T. vaginalis susceptibility (404-718-4141)
First treatment failure, re-treat with: Metronidazole 500 mg PO BID x 7 days If repeat failure, treat with: Metronidazole 2 g PO x 5 days Tinidazole 2 g PO x 5 days Susceptibility testing: send isolate to CDC CDC Consult & T. vaginalis susceptibility ( )
")
66
Diagnostic tests for Trichomonas
BioMed Diagnostics Needs incubator Read at 3 and 5 days Sekisui Diagnostics CLIA-waived Results in 10 minutes 83% sensitive compared to culture Gen-Probe APTIMA Trichomonas vaginalis Assay Same specimen types as for other APTIMA tests Close to 100% sensitive; Slightly less sensitive using urine Over 99% specific

67
Trich in HIV + Women Screen on entry to care
Retest at 3 months after treatment Consider metronidazole 500 mg p.o. bid x 7d instead of stat dose

68
OH, NO!! She’s allergic to metronidazole!

69
Treatment Options with “Azole” Allergy
Consult with specialist Metronidazole desensitization Helms et al, Am J Obstet Gynecol 2008 Perlman et al, Am J Obstet Gynecol, 1996 Kurohara et al, j Allergy Clin Immunol, 1991 Paramomycin vaginal inserts not as effective

70
8. Encourage Good Old Condoms!
And last but certainly not least, good old condoms!!

71
Openers for a Conversation about Condoms
Tell me about your experience with condoms. Some men take condoms almost for granted, and other men really dislike them. What about you? How willing have you found guys to be about using condoms?

72
Making the Change Goal: to improve patient care by improving medical practice What can you do on your own? What can you realistically influence? What can you advocate for?

73
THANK YOU!!!! Questions?

74
A bit more info…..

75
Online STD Resources CDC Treatment Guidelines
California STD/HIV Prevention Training Center California Department of Public Health STD Control Branch

76
California Laws and Regulations

77
STD Reporting to Public Health
Which diseases? Syphilis within 1 day HIV/AIDS Chlamydia, including LGV Gonorrhea Chancroid Pelvic Inflammatory Disease (PID) By whom? Provider and Laboratory To whom? The jurisdiction where patient resides How? CMR to be completed by the provider Within 7 days
 By whom Provider and Laboratory. To whom The jurisdiction where patient resides. How CMR to be completed by the provider. Within. 7 days.")
78
Partner Management Provider Responsibility
The clinician should: Attempt to determine the source of infection Determine the intimate and sexual contacts of the infected patient Make an effort with patient to bring in those contacts for exam and treatment Persons determined as source of infection but not under treatment within 10 days of infection should be reported to the health officer EPT is allowable for CT, GC, and trichomoniasis CCR Title 17 §2636

79
Minor’s Rights to STD Care in California
Minors age 12 and above are able to consent to STD and reproductive health care without parental permission As of January 1, 2012, minors may also consent to medical care related to prevention of STD (e.g., HPV vaccine) Minors have a right to confidentiality Parents are not liable for costs of STD care Reporting requirements for non-consensual (and “unlawful”) sexual activity CA Family Code §6926
 Minors have a right to confidentiality. Parents are not liable for costs of STD care. Reporting requirements for non-consensual (and unlawful ) sexual activity. CA Family Code §6926.")
80
Valacyclovir Group (N=743)
Transmission of HSV-2 to Susceptible Partners is Reduced with Once-Daily Suppression 1484 heterosexual couples randomized to 500 mg of valacyclovir vs placebo once daily for 8 months Monthly serum samples collected from susceptible partners Valacyclovir group showed decreased transmission lower frequency of shedding fewer copies of HSV-2 DNA when shedding occurred Valacyclovir Group (N=743) Control Group (N=741) Corey et al, NEJM 2004; 350(1):11-20.
 Control Group (N=741) Corey et al, NEJM 2004; 350(1):")
81
Gardasil or Cervarix: Which is better?
BOTH HPV Vaccines: Effective in preventing 16/18-related cervical dysplasia Good safety profile High cost Gardasil advantages: Protects against 6/11-related genital warts Licensed for males Indications vulvar/vaginal dysplasia Cervarix advantages: Higher titer levels May give greater cross-protection against other oncogenic HPV types Effectiveness data for preventing persistent re-infection

Similar presentations







 Adopted from : IPPF MEDICAL AND SERVICE DELIVERY GUIDELINES FOR SEXUAL AND REPRODUCTIVE HEALTH.>")








 and two non->")


>")
