Download presentation
Presentation is loading. Please wait.

1
Autism Spectrum Disorder

2
DSM-V Criteria Criterion A: Persistent deficits in social communication and interaction Can include social-emotional reciprocity, nonverbal communicative behaviors, developing/maintaining relationships Criterion B: Restricted, repetitive patterns of behavior Repetitive motor movements (rocking), ecolalia, insistence on sameness and a routine, highly restricted, fixated interests, unusual interest in sensory aspects of the environment Symptoms must be present in early developmental period and cannot be better explained by intellectual disability or global developmental disability 3 levels of severity Viewed as a dimensional disorder Specifiers for each criterion Behaviors fitting criterion A: problems w/back and forth conversation, sharing emotion, responding to social interaction, poor nonverbal communication, problems maintaining or understanding eye contact and other body language, difficulty in imaginary play, making friends, absence of interest in peers Specify with or without intellectual disability (often with, not always) Needing support, substantial support, or very substantial support (high/medium/low functioning) There’s been some work to subtype kids, but anything meaningful is explained by IQ Dimensionality helps linking with biology Relationship b/t IQ and symptom severity,
, ecolalia, insistence on sameness and a routine, highly restricted, fixated interests, unusual interest in sensory aspects of the environment. Symptoms must be present in early developmental period and cannot be better explained by intellectual disability or global developmental disability. 3 levels of severity. Viewed as a dimensional disorder. Specifiers for each criterion. Behaviors fitting criterion A: problems w/back and forth conversation, sharing emotion, responding to social interaction, poor nonverbal communication, problems maintaining or understanding eye contact and other body language, difficulty in imaginary play, making friends, absence of interest in peers. Specify with or without intellectual disability (often with, not always) Needing support, substantial support, or very substantial support (high/medium/low functioning) There’s been some work to subtype kids, but anything meaningful is explained by IQ. Dimensionality helps linking with biology. Relationship b/t IQ and symptom severity,")
3
Secondary Features Intellectual disability Motor disabilities
Often large discrepancies in abilities in high functioning kids Motor disabilities Odd gait, clumsiness, walking on tiptoes Self-injury Inattention Disruptive behavior Catatonia Possible, not particularly common Most likely during adolescent years

4
Controversy DSM-IV included categories for Autism, Pervasive Development Disorder NOS, High Functioning Autism, and Asperger’s Syndrome Sevin et al (1995) studied 34 kids with autism and PDD-NOS. Did not find discrete categories. Categories were collapsed into Autism Spectrum – PDD-NOS, HFA, and AS now “on the spectrum” Concern about retaining diagnoses, receiving services, stigma PDD-NOS – like autism but don’t clearly fit into the old category. Atypical or subthreshold symptoms HFA – not with intellectual disability or requiring substantial support. Just odd social behavior and repetitive behaviors, can function alone. No cognitive issues, really, but they do have delayed motor milestones Asperger’s Syndrome – even higher than HFA kid, just “socially awkward.” Facial expression, prosody, social gestures deficient but nothing else
 studied 34 kids with autism and PDD-NOS. Did not find discrete categories. Categories were collapsed into Autism Spectrum – PDD-NOS, HFA, and AS now on the spectrum Concern about retaining diagnoses, receiving services, stigma. PDD-NOS – like autism but don’t clearly fit into the old category. Atypical or subthreshold symptoms. HFA – not with intellectual disability or requiring substantial support. Just odd social behavior and repetitive behaviors, can function alone. No cognitive issues, really, but they do have delayed motor milestones. Asperger’s Syndrome – even higher than HFA kid, just socially awkward. Facial expression, prosody, social gestures deficient but nothing else.")
5
Controversy Intent was NOT to remove anyone’s diagnosis
Will actually help some higher functioning kids get services Everyone should convert to Autism Spectrum with specifications if criteria used correctly DSM-IV included category for communication difficulty This is covered by DSM-V criteria A and B. Separate category was not needed

6
DSM-V Schematic Genetics Core Symptoms Biological Substrate
Unknown Core Symptoms Social Deficits Restricted, repetitive behaviors Biological Substrate Unknown Secondary Symptoms Intellectual, motor disabilities Self-injury Inattention/Disruptive Behavior Catatonia

7
Assessment – ADI-R Gold Standards are Autism Diagnostic Interview – Revised (ADI-R) and Autism Diagnostic Observation Scale (ADOS) ADI-R is semi-structured interview for caregivers 93 items, about 2 hours Based on DSM-IV criteria (Communication difficulties, social reciprocity, restricted, repetitive behaviors) Chakrabarti and Fombonne (2001) found that interrater reliability was excellent on those subscales
 Chakrabarti and Fombonne (2001) found that interrater reliability was excellent on those subscales.")
8
Assessment - ADOS Observational
Can be used in nonverbal 2-year-olds – verbal adults and all between 4 Modules: Pre-Verbal-Single Words Phrase speech Fluent Speech Activities for daily living, plans, hopes

9
Psychometric Issues in Diagnosis
Low test-retest reliability on many instruments Little investigation of specificity or validity of screening measures Lack sensitivity and specificity Severity scores quantifying social deficits needed Sometimes alternative thresholds are suggested for research vs clinical diagnoses Children of color or of less-educated parents less likely to receive ASD diagnosis than Caucasian kids or kids with well-educated parents (Mandell et al 2009)
")
10
Psychometric Issues in Diagnosis
In a study of children with language disorder, both the ADOS and ADI-R were administered to children Studied 21 children ages 6-9 Correlation between instruments low (Bishop 2011) Χ^2 (4) = 1.86, p= .762 ----- Meeting Notes (10/28/14 20:06) ----- Chi squared - distributions of categorical data sig different or not? (ASD diagnosis or not)
 Χ^2 (4) = 1.86, p= Meeting Notes (10/28/14 20:06) Chi squared - distributions of categorical data sig different or not (ASD diagnosis or not)")
11
Social Problems Most universal, specific characteristic of ASD
Consistent and replicated across studies Lack joint attention, theory of mind Cannot correctly assign motives, understand someone’s goals, difficulty participating in spontaneous symbolic play Other groups show problems with theory of mind but may not show same deficits in joint attention Down Syndrome, severe hearing impairment Pay proportionately less attention to people than objects Spend less time than TD kids doing something that shows intent Children are attached to mothers as much as age- and IQ-matched TD kids (Rogers et al., 1991) Tend not to point, show objects – attention-sharing behaviors (Sigman et al., 1986) Do not seem to recognize emotions (facial expression, gesture, nonverbal vocalizations of emotion) Range from aloofness, active and odd behavior, passivity, just not at all interested *Toddler who doesn’t want to play with other kids *Adult who’s never had a significant other *Trouble understanding workplace roles, back and forth conversation, etc. Will likely develop language but are never good at back-and-forth communication Hobson 1986 Some people think they don’t form attachments, but they do Joint Attention = person w/autism, another person, and object/event. TOM = people have minds which differ from one’s own, one can learn from others by reading social signals and listening (Lord & MaGill-Evans, 1995) There is a DSM category for people with JUST these, no RRB’s – social communication disorder
 Tend not to point, show objects – attention-sharing behaviors (Sigman et al., 1986) Do not seem to recognize emotions (facial expression, gesture, nonverbal vocalizations of emotion) Range from aloofness, active and odd behavior, passivity, just not at all interested. *Toddler who doesn’t want to play with other kids. *Adult who’s never had a significant other. *Trouble understanding workplace roles, back and forth conversation, etc. Will likely develop language but are never good at back-and-forth communication. Hobson Some people think they don’t form attachments, but they do. Joint Attention = person w/autism, another person, and object/event. TOM = people have minds which differ from one’s own, one can learn from others by reading social signals and listening. (Lord & MaGill-Evans, 1995) There is a DSM category for people with JUST these, no RRB’s – social communication disorder.")
12
Restricted, Repetitive Behaviors
Verbal and nonverbal repetitive, stereotyped behaviors More heterogeneous and context-dependent than social deficits Including them on diagnostic instruments increases specificity with little change in sensitivity One study showed only 9 of 2700 children with ASD diagnosis did not show any RRB’s (Lord et al., 2012) Interests – Heidi’s Charlie Brown kid. Symptoms must be present in childhood Same thing to eat every day, certain activity only certain day a week, Number and intensity at age 2 predictor of ASD diagnosis at age 9 (Lord et al 2006) Predictive of parental stress, academic achievement Longitudinal studies show that neither social deficits nor RRB’s account for each other, but they are correlated (about .5) - There may be something higher-level that accounts for both
 Interests – Heidi’s Charlie Brown kid. Symptoms must be present in childhood. Same thing to eat every day, certain activity only certain day a week, Number and intensity at age 2 predictor of ASD diagnosis at age 9 (Lord et al 2006) Predictive of parental stress, academic achievement. Longitudinal studies show that neither social deficits nor RRB’s account for each other, but they are correlated (about .5) - There may be something higher-level that accounts for both.")
13
Restricted, Repetitive Behaviors
Four subdomains: Motor stereotypies – lining things up, flipping things, step counting, unusual responses to sensory input, rocking Some of these may be common in young children – clinicians must look at the number and intensity of behaviors to discriminate TD from ASD Tend to emerge early in life but are somewhat malleable Most common subdomain Rituals and sameness – like Rain Man’s pancake Tuesday Prevalent in about 25% of ASD population Develop later than motor type, stable throughout life Circumscribed interests – highly fixated or unusual interests A particular movie, cartoon character, topic, the phone book, shoe size Self-injurious behavior – hand flapping, hitting Present in other disorders More common in ASD than general population Subdomains show different trajectories *found the trajectories noted but I don’t know much about them

14
Language Delay Language delay is not specific to ASD
Delays in receptive language may be specific to ASD as opposed to other communication disorders (Philofsky, Hepburn, Hayes, Hageran, & Rogers 2004) Not yet connected to specific neurobiological problem Language (particularly receptive language) scores correlate with IQ (specifically verbal) (Luyster et al., 2008)
 Not yet connected to specific neurobiological problem. Language (particularly receptive language) scores correlate with IQ (specifically verbal) (Luyster et al., 2008)")
15
Prevalence In 1990’s it was 1 per 2,000, including Asperger’s Syndrome 1 per 1,000 (Tanguay 2000) Current prevalence rates around 1/150 to 1/100 for ASDs (Croen et al., 2002, Rice, 2009) True increase in milder cases True increase of all case types More awareness Problems with diagnostic instruments Incorrect diagnoses Studies differ in screening methods, diagnostic instruments, diagnostic criteria Diagnosed 4x as often in males than females We don’t know why – probably combination of listed reasons for increase in prevalence
 True increase in milder cases. True increase of all case types. More awareness. Problems with diagnostic instruments. Incorrect diagnoses. Studies differ in screening methods, diagnostic instruments, diagnostic criteria. Diagnosed 4x as often in males than females. We don’t know why – probably combination of listed reasons for increase in prevalence.")
16
Diagnostic Criteria Projects using ICD-10 criteria show prevalence around 1/2,000 (Autism) and 1/600 (Autism plus other pervasive developmental disorders) Studies using less strict criteria show much higher prevalence rates Bryson et al., 1988, 1/1,000 Used ABC (checklist) Sugiyama and Abe (1989) used DSM-III and noted 1/760 Ehlers and Gillberg (1993) set of criteria specifically designed to diagnose ASD found 1/143 ASD = autism spectrum disorder
 and 1/600 (Autism plus other pervasive developmental disorders) Studies using less strict criteria show much higher prevalence rates. Bryson et al., 1988, 1/1,000 Used ABC (checklist) Sugiyama and Abe (1989) used DSM-III and noted 1/760. Ehlers and Gillberg (1993) set of criteria specifically designed to diagnose ASD found 1/143. ASD = autism spectrum disorder.")
17
Onset and Course Symptoms are usually noted first in months of a child’s life Delayed language, odd play patterns, lack of social interaction Pay attention to type, frequency, intensity of symptoms Can experience developmental plateaus or regression Rarely a severe regression after 2 years of normal development Onset must occur by age 3 Individuals generally improve throughout lives Robust diagnosis Sensitivity of .82 and specificity of .87 (Volkmar et al 1994) Earlier if severe, later if subtle Lack of interest in social interaction may come about in first year Sensitivity = true positive (82% of autistic group diagnosed). Not many false negatives. Not missing many. Specificity = true negative (don’t diagnose 87% of healthy group) Not many false positives
 Earlier if severe, later if subtle. Lack of interest in social interaction may come about in first year. Sensitivity = true positive (82% of autistic group diagnosed). Not many false negatives. Not missing many. Specificity = true negative (don’t diagnose 87% of healthy group) Not many false positives.")
18
Common Comorbidities 70% of ASD individuals have one comorbid disorder, up to 40% may have 2 or more (DSM-V) Medical conditions such as epilepsy and sleep problems somewhat common Comorbid diagnoses of ADHD, anxiety and depressive disorders, and developmental coordination disorder seen First degree relatives have higher incidence of major depression and social phobia than the rest of the population (Bolton et al., 1998) Relatives have 20% frequency of social phobia (Smalley et al., 1995) 10 times higher than controls Over half (64%) had first episode before the birth of autistic child
 Relatives have 20% frequency of social phobia (Smalley et al., 1995) 10 times higher than controls. Over half (64%) had first episode before the birth of autistic child.")
19
Common Comorbidities? Posited that autism shared genetic cause and thus comorbidities with: Fragile X (no more than 2-5% have FRA-X mutation, Bailey et al., 1993) Tuberous sclerosis (mostly seen in autistic people with severe deficits, Guiterrez et al., 1998) Celiac disease (Pavone et al., 1997 study of 120 people with celiac disease showed none with diagnosis of autism based on DSM-III, nor celiac disease in the 11 patients with autism)
 Tuberous sclerosis (mostly seen in autistic people with severe deficits, Guiterrez et al., 1998) Celiac disease (Pavone et al., 1997 study of 120 people with celiac disease showed none with diagnosis of autism based on DSM-III, nor celiac disease in the 11 patients with autism)")
20
Biological Contributions
?
21
Genetics Concordance rates in monozygotic versus dizygotic twins range from 60-91% (MZ), 0-10% (DZ) (Folstein and Rutter, 1977, Steffenburg et al., 1989, Bailey et al., 1995.) Variation in behavioral and cognitive deficits as great within MZ pairs as between pairs These findings suggest that autism is highly heritable (broad cognitive and social impairment) Different sets of genes do not act to produce different symptoms Tuberous sclerosis – root-shaped growth in the brain, number correlated w/degree of intellectual disability If so, MZ pairs would be almost identical (identical genes)
, 0-10% (DZ) (Folstein and Rutter, 1977, Steffenburg et al., 1989, Bailey et al., 1995.) Variation in behavioral and cognitive deficits as great within MZ pairs as between pairs. These findings suggest that autism is highly heritable (broad cognitive and social impairment) Different sets of genes do not act to produce different symptoms. Tuberous sclerosis – root-shaped growth in the brain, number correlated w/degree of intellectual disability. If so, MZ pairs would be almost identical (identical genes)")
22
Genetics Gender disparity led some researchers to wonder if ASD linked to X chromosome Hallmayer et al (1996) found no major gene effect on X chromosome causing autism International Molecular Genetic Study of Autism Consortium (1998) found possible connections for regions on chromosomes 7 and 16 Significance is not yet known Found most often in those with severe language delays Normal on the right, abnormal on left (inverted)
 found no major gene effect on X chromosome causing autism. International Molecular Genetic Study of Autism Consortium (1998) found possible connections for regions on chromosomes 7 and 16. Significance is not yet known. Found most often in those with severe language delays. Normal on the right, abnormal on left (inverted)")
23
Neuroligins and Neurexins
Neuroligins and neurexins are the “building blocks” of synapses Small percentage of those with ASD have mutations which can cause neurexin deletions This affects synaptic formation and function May increase risk for developing ASD Neurexins and neuroligins “shake hands” and form the synapse, crucial for function and connectivity. Presynaptic, generally. Building blocks for synapse Neurexin – presynaptic protein, helps “glue together” neuron at synapse Variability of genetic profiles in ASD kids tells us maybe there are distinct genetic disorders with overlapping phenotypes

24
Neuropharmacological Studies
Cook and Leventhan (1996) noted that serotonin may be involved in many of the symptoms of autism This is neither surprising nor particularly helpful One study found people with ASD have autoantibodies to brain serotonin receptors (Todd and Ciaranello, 1985) Two studies failed to confirm findings People with ASD may have increased 5-HT on blood platelets Found increased serotonin levels on blood platelets
 noted that serotonin may be involved in many of the symptoms of autism. This is neither surprising nor particularly helpful. One study found people with ASD have autoantibodies to brain serotonin receptors (Todd and Ciaranello, 1985) Two studies failed to confirm findings. People with ASD may have increased 5-HT on blood platelets. Found increased serotonin levels on blood platelets.")
25
Electroencephalography
ASD people unlikely to show more EEG abnormalities than the normal population This is nonspecific and not particularly helpful

26
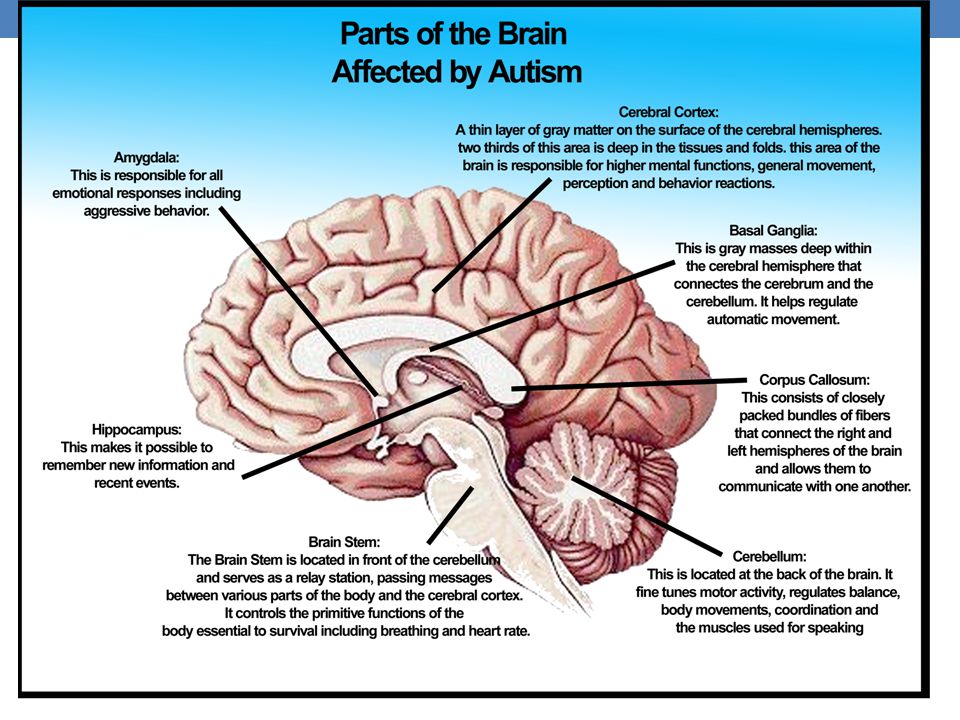
Neuroimaging and Neuropathological Studies
General difficulty confirming neuroimaging findings Different measures used to correlate with brain function, generally weak measures Future studies will probably add comparisons of ADHD or language impairments to ASD Increased volume in amygdala, hippocampus, and limbic system, decreased Purkinje cells We don’t know how high functioning these individuals were Harris et al. (2006) claimed to find abnormal patterns of activity in the brains of those with ASD and claimed near-perfect identification This has not been replicated Ongoing NIMH effort to form neurobiologically based dimensions to help diagnose ASD, but no published data yet I could not access the Harris 2006 study. Been super difficult to link any biological findings with symptoms due to only a small percentage of ASD pop with any given abnormality One solution is to turn behavior (like criteria A and B) into dimensions and connect those with biological findings Purkinje cells – GABA-ergic neurons
 claimed to find abnormal patterns of activity in the brains of those with ASD and claimed near-perfect identification. This has not been replicated. Ongoing NIMH effort to form neurobiologically based dimensions to help diagnose ASD, but no published data yet. I could not access the Harris 2006 study. Been super difficult to link any biological findings with symptoms due to only a small percentage of ASD pop with any given abnormality. One solution is to turn behavior (like criteria A and B) into dimensions and connect those with biological findings. Purkinje cells – GABA-ergic neurons.")
27
Macroencephaly 14-30% of ASD people have increase in head circumference (Fombonne et al., 1999) Developed in early/middle childhood (Lainhart et al), but this finding relies on retrospective data Increase is in temporal, parietal, and occipital lobes (not frontal) Cause and effects of increase unknown Not correlated with IQ, verbal ability, seizure, other mental illness ----- Meeting Notes (10/28/14 20:06) ----- Lack of appropriate pruning?
, but this finding relies on retrospective data. Increase is in temporal, parietal, and occipital lobes (not frontal) Cause and effects of increase unknown. Not correlated with IQ, verbal ability, seizure, other mental illness Meeting Notes (10/28/14 20:06) Lack of appropriate pruning")
28
Yellow – white matter, enlarged in ASD

29
Red – smaller in ASD, Grey matter

30
Neuropsychological Patterns
Compared to normal controls, ASD people have intact or superior performance in attention, simple memory, simple language, and visual-spatial domains Impaired in skilled motor tasks, complex memory, complex language, and reasoning While interesting, not helpful in understanding much more about autism than is already known Minshew et al 1997 33 participants – autistic w/normal intelligence and normal controls

31
Neuropsychological patterns
Executive functioning deficits Impairments in cognitive flexibility and set-shifting Nonspecific to autism May underlie theory of mind deficits Price et al., (1990) study of 2 individuals with widespread frontal damage (early in developmental process) Both showed severe impairment in role-taking, also seen in ASD and is part of theory of mind Flexibility = Cog set shift =
 study of 2 individuals with widespread frontal damage (early in developmental process) Both showed severe impairment in role-taking, also seen in ASD and is part of theory of mind. Flexibility = Cog set shift =")
32
Neuropsychological Patterns
20 ASD, 19 Down’s Syndrome kids, 20 TD kids Two tasks: Delayed Non-Matching to Sample Rule-learning ability, visual recognition memory Amygdala and hippocampus Delayed Response Working memory and response inhibition Dorsolateral PFC Social and nonsocial stimuli task Actually Autistic and PDD-NOS, back w/DSM-III criteria, now would be ASD Diagnosed w/CARS – Non_Matching to Sample: Shown a sample object, rewarded when they reached for it (reward underneath) Waited 5 seconds. Did again but w/second object there too. Rewarded when they reached for that one Established criterion performance (5 in a row right, 15 max) DV’s - # of errors made, # of trial required until reached criterion performance Delayed Response Experimenter hid a toy in a container at midline, then moved right or left 5 second delay, screen lowered, identical container put on opposite side (now 2 containers) Side hidden reversed after 2 correct. Continued until 3 reversals or 14 trials DV – % correct in reverse trials No diff in average # of reversal trials Social – calling name or clapping hands Nonsocial – rattle, jack in the box
 Waited 5 seconds. Did again but w/second object there too. Rewarded when they reached for that one Established criterion performance (5 in a row right, 15 max) DV’s - # of errors made, # of trial required until reached criterion performance. Delayed Response. Experimenter hid a toy in a container at midline, then moved right or left. 5 second delay, screen lowered, identical container put on opposite side (now 2 containers) Side hidden reversed after 2 correct. Continued until 3 reversals or 14 trials. DV – % correct in reverse trials. No diff in average # of reversal trials. Social – calling name or clapping hands Nonsocial – rattle, jack in the box.")
33
This shows 1st task Autistic kids sig worse than other groups – took more trials Less time attending to social things than other groups Suggests the structures tested implicated in autism (amygdala, hippocampus, dorsolateral PFC)
")
35
Vaccines

36
Vaccines One study published in a medical journal concluded a link between vaccines (MMR) and autism Article was fully retracted in 2010 Lead author Andrew Wakefield had many undeclared conflicts of interest and manipulated some of his data Found guilty of serious medical misconduct and no longer allowed to practice medicine Study has been disproved many times since its original publication in 1998

37
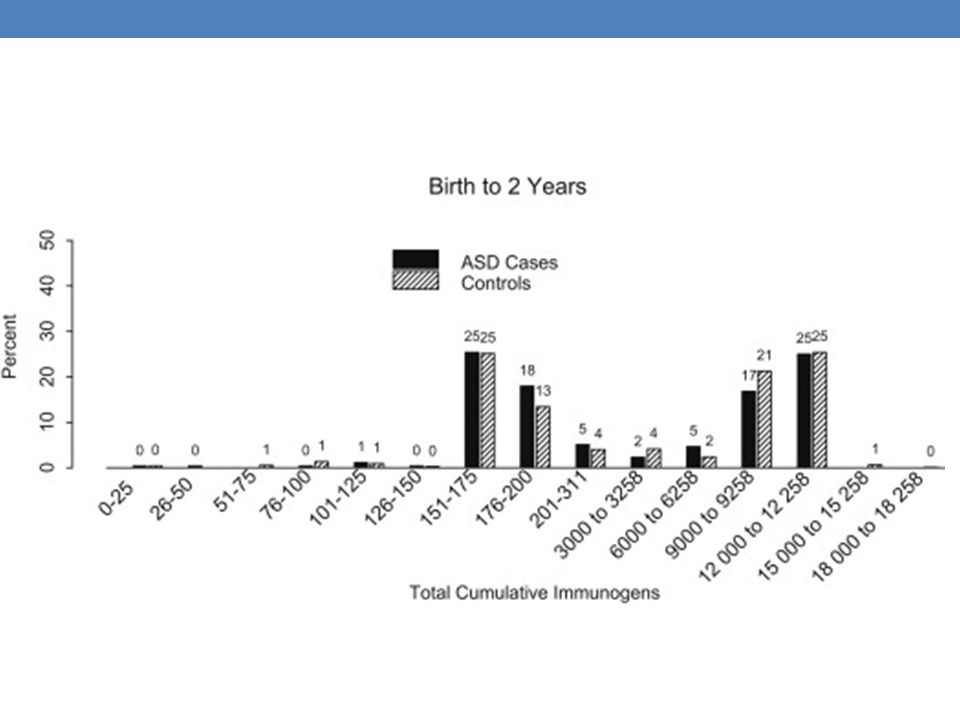
Vaccines DeStefano et al (2013) evaluated 256 ASD kids and 752 TD kids matched on birth year and sex, ages 6-13 Confirmed diagnoses via ADI-R and ADOS Study inclusion criteria required elevated scores on both assessments and onset before 36 months Obtained vaccination histories, Looked at total antigen exposure, amount per day No significant differences Birth-3 months, 7-months, 2-years Latest published study disproving connection b/t vaccines and autism

38
Bimodal because of different vaccines

40
Environmental Factors
Mouridsen et al. studied 328 children with autism, “autism-like conditions,” or “borderline child psychosis” Children with autism had greater incidence of births in March or August Children with autistic-like conditions most often born in May and November Essentially, this means nothing. DSM-III criteria

41
Environmental Factors
Rutter 1998 study looked at institutionalized children in Romania sent to the UK Experienced horrible living conditions 7/165 met criteria for autism based on a screening questionnaire Severe social deprivation may lead to autistic-like social and emotional difficulties Could less severe social deprivation interact with genes to cause autism in some kids or worsen symptoms?

42
Treatment

43
Medication Tricyclics and SSRI’s seem to decrease hyperactivity, anger, and compulsive behaviors (Gordon et al., 1993, Brodkin et al., 1997) Neuroleptics may be effective in reducing hyperactivity, impulsivity, aggressiveness (Potenza et al., 1999) (Obviously) Pharmacological interventions have a limited role
 (Obviously) Pharmacological interventions have a limited role.")
44
Medication Double-blind study of 40 kids, given placebo or haloperidol
Given semistructured interviews, rated by teachers on Connors Parent-Teach Questionnaire While on haloperidol, kids showed significant decreases in withdrawl, hyperacitvity, abnormal object relationships, fidgetiness, negativeism, angry affect, and lability of affect as compared to baseline or placebo Ages years 2 weeks placebo for baseline Then either haloperidol/placebo/H or Placebo/H/P for four weeks each Rating scale Doses ranged from mg/day, started low and stopped when started seeing either positive or negative effects ----- Meeting Notes (10/24/14 21:25) ----- Again, talking about kids 2-6 getting neuroleptic!
 Again, talking about kids 2-6 getting neuroleptic!")
45
Therapy The key is early intervention! Two types
This means developing specific measures is crucially important Two types Traditional behavior learning (ABA) Focus is on adult control and child compliance, uses positive reinforcement Social-pragmatic teaching (child-centered therapy, incidental teaching) Focuses mainly on social skills Focus of therapy is on increasing independence and quality of life ----- Meeting Notes (10/24/14 21:25) ----- Measures not sensitive nor specific, nor do they correlate with each other, and they can have different thresholds for research vs clinical When kids are 18 months, key predictors of diagnosis of autism in later life are two or more: Lack of pretend play Lack of protodeclarative pointing Lack of social interest/play Lack of joint attention
 Focus is on adult control and child compliance, uses positive reinforcement. Social-pragmatic teaching (child-centered therapy, incidental teaching) Focuses mainly on social skills. Focus of therapy is on increasing independence and quality of life Meeting Notes (10/24/14 21:25) Measures not sensitive nor specific, nor do they correlate with each other, and they can have different thresholds for research vs clinical. When kids are 18 months, key predictors of diagnosis of autism in later life are two or more: Lack of pretend play. Lack of protodeclarative pointing. Lack of social interest/play. Lack of joint attention.")
46
Applied Behavior Analysis
Gold standard Based on behaviorism Uses positive reinforcement to decrease maladaptive and unwanted behaviors, increase adaptive behaviors Uses negative reinforcement/negative punishment when necessary (rarely) Treatment can begin when children are as young as 3 In severe cases, focus is on compliance Intensive (20-40 hours/week), one-on-one format Targets a wide range of skills Includes parents (and important others when possible – siblings, teachers, etc.)
 Treatment can begin when children are as young as 3. In severe cases, focus is on compliance. Intensive (20-40 hours/week), one-on-one format. Targets a wide range of skills. Includes parents (and important others when possible – siblings, teachers, etc.)")
47
ABA Effect Size Metrics
Meta-Analysis of 22 studies (Virués-Ortega 2010) Different outcome reported: full-scale IQ (18 studies), nonverbal IQ (9), receptive language (10), expressive language (9), language composite (5), adaptive behavior-communication (10), adaptive behavior – daily living skills (10), adaptive behavior – socialization (10), adaptive behavior – motor skills (3), overall composite adaptive behavior (14) Mean age ranged from months Some studies included PDD-NOS Because: Participants, actual therapy highly variable, studies use different metrics when reporting outcomes Often single-subject design Because so many outcome instruments were used they “Used effect sizes to obtain standardized measurements of the effect of the intervention on the outcome variable” Effect sizes were corrected for sample size Pooled correlational coefficient was estimated from studies in which data available to calculate pre-post correlation coefficients for a given outcome Those were then applied to all studies reporting the outcome For each outcome, pooled estimates and 95% confidence intervals of effect sizes calculated 2 or more studies available, sensitivity analysis done by restricting the analysis to control group designs Separate for intervention model (general ABA vs UCLA, don’t know diff), and format (clinic based or parent managed) Only effect sizes over .5 reported for brevity” Rank ordered by length of intervention (hours), dose-response meta then done
 Different outcome reported: full-scale IQ (18 studies), nonverbal IQ (9), receptive language (10), expressive language (9), language composite (5), adaptive behavior-communication (10), adaptive behavior – daily living skills (10), adaptive behavior – socialization (10), adaptive behavior – motor skills (3), overall composite adaptive behavior (14) Mean age ranged from months. Some studies included PDD-NOS. Because: Participants, actual therapy highly variable, studies use different metrics when reporting outcomes. Often single-subject design. Because so many outcome instruments were used they Used effect sizes to obtain standardized measurements of the effect of the intervention on the outcome variable Effect sizes were corrected for sample size. Pooled correlational coefficient was estimated from studies in which data available to calculate pre-post correlation coefficients for a given outcome. Those were then applied to all studies reporting the outcome. For each outcome, pooled estimates and 95% confidence intervals of effect sizes calculated. 2 or more studies available, sensitivity analysis done by restricting the analysis to control group designs. Separate for intervention model (general ABA vs UCLA, don’t know diff), and format (clinic based or parent managed) Only effect sizes over .5 reported for brevity Rank ordered by length of intervention (hours), dose-response meta then done.")
48
ABA ABA positively impacted:
IQ – 1.19 no evidence of effect from intensity/duration Nonverbal IQ – 0.67 Receptive language – 1.48 Expressive language – 1.47 General language skills – 1.07 Communication – 1.45 Daily living skills – 0.62 Socialization Motor skills – 0.71 Adaptive behavior (composite score) – 1.09 ABA leads to long-term medium to high positive effect sizes for adaptive behaviors Social support (siblings) moderate response (Hastings, 2003) 95% CI’s IQ – , p<.001 Nonverbal IQ – p = .008 Receptive language – , p<0.001 Expressive language p<0.001 General language – , p = 0.004 Communication p<0.001 Daily living skills – , p < 0.001 Socialization – p<0.001 Motor skills p =0.008 Adaptive behavior composite – p<0.001
 – ABA leads to long-term medium to high positive effect sizes for adaptive behaviors. Social support (siblings) moderate response (Hastings, 2003) 95% CI’s. IQ – , p<.001. Nonverbal IQ – p = Receptive language – , p< Expressive language p<0.001 General language – , p = Communication p< Daily living skills – , p < Socialization – p< Motor skills p = Adaptive behavior composite – p<")
49
CBT CBT has been modified for ASD kids presenting with anxiety
Goal is to remediate social skills in the hopes that this will translate to decreased anxiety Random assignment to 16 sessions of CBT or 3-month waitlist CBT model emphasized adaptive behavior, parental training, school consultation 78% of CBT group had reductions in anxiety on Clinical Global Impressions-Improvement scale compared to 8.7% of waitlist CBT did not reduce self-reports of anxiety ----- Meeting Notes (10/28/14 20:06) ----- Where we might come in as they'll go to ABA therapist probably, but we might do this and it's possible.
 Where we might come in as they ll go to ABA therapist probably, but we might do this and it s possible.")
50
Virtual Interactive Environments
Used for teaching social skills, theory of mind Practical situations, such as taking the bus, going to the grocery store Some studies use robots (can play games with kids) Interactions (eye gaze, tough, contact time) increase Not yet known if this generalizes to real life Opposite effect – more complacent/happy to stay with computer? Allows children to role-play, practice skills in a safe environment, may promote greater insight into minds of others Designed as part of larger problem – with an instructor working on skills
 Interactions (eye gaze, tough, contact time) increase. Not yet known if this generalizes to real life. Opposite effect – more complacent/happy to stay with computer Allows children to role-play, practice skills in a safe environment, may promote greater insight into minds of others. Designed as part of larger problem – with an instructor working on skills.")
51
AIT – 10 hours of music to decrease irritability/hyperactivity
Complimentary and Alternative Medicine Therapies (Mostly pseudoscience) Auditory integration Training Facilitated communication Nonverbal/severely handicapped people are suddenly writing emotional, grammatically correct messages This is due to the facilitator (Bomba et al 1996) Viamin B6 and Magnesium 30% of children showed improvement in Martineau (1998) study. Other studies show no improvement Changes in nutrition All are ineffective AIT – 10 hours of music to decrease irritability/hyperactivity Facilitated communication – therapist guides hand to keyboard to type messages (removing food additives, sugar, increasing certain fats, yoga and massage, herbal remedies) all disproven Of course can be useful for certain problems (yoga for sleep or anxiety, diet for GI problems) but not ASD itself Fenfluramine Decreases blood serotonin levels May decrease hyperactivity but nothing else (Campbell 1988) Naltrexone Clonidine Doesn’t work for social behaviors Secretin Endogenous gastroinestinal polypeptide, ineffective Corticosteroids
 Auditory integration Training. Facilitated communication. Nonverbal/severely handicapped people are suddenly writing emotional, grammatically correct messages. This is due to the facilitator (Bomba et al 1996) Viamin B6 and Magnesium. 30% of children showed improvement in Martineau (1998) study. Other studies show no improvement. Changes in nutrition. All are ineffective. AIT – 10 hours of music to decrease irritability/hyperactivity. Facilitated communication – therapist guides hand to keyboard to type messages. (removing food additives, sugar, increasing certain fats, yoga and massage, herbal remedies) all disproven. Of course can be useful for certain problems (yoga for sleep or anxiety, diet for GI problems) but not ASD itself. Fenfluramine. Decreases blood serotonin levels. May decrease hyperactivity but nothing else (Campbell 1988) Naltrexone. Clonidine. Doesn’t work for social behaviors. Secretin. Endogenous gastroinestinal polypeptide, ineffective. Corticosteroids.")
52
Therapy Core Features Genetics Biological Substrate Genetics
ABA Genetics Some combination of: Neurexin and neuroligin abnormality Chromosome 16 abnormality Chromosome 7 inversion Core Features Social difficulties Restricted, repetitive behaviors Biological Substrate Some combination of: Enlarged amygdala, hippocampus Abnormal fusiform gyrus Macroencephaly Decreased Purkinje cells Increased 5-HT Genetics Some combination of: Neurexin and neuroligin abnormality Chromosome 16 abnormality Chromosome 7 inversion Biological Substrate Some combination of: Enlarged amygdala, hippocampus Abnormal fusiform gyrus Macroencephaly Decreased Purkinje cells Increased 5-HT Secondary Features Intellectual disability Inattention Motor problems Environment Abuse Social support Genetics: Combinations of 7, 16, possible X-chromosomal abnormalities, neurexin and neuroligin abnormalities Biological substrate: Increased levels of serotonin, macroencephaly, larger amygdala and hippocampus Core and Secondary features the same as DSM specifies, no catatonia Genetics Some combination of: Neurexin and neuroligin abnormality Chromosome 16 abnormality Chromosome 7 inversion Medication SSRI’s Antipsychotics

53
References Anderson, D.K., Oti, r.s>, Lord, C., & Welch, K. (2009). Patterns of growth in adaptive social abilities among children with autism spectrum disorders. Journal of Abnormal Child Psychology, 37(7), Baron-Cohen, S. (2009). The short life of a diagnosis. The New York Times. Available from Anderson, L.W., Campbell, M., Grega, D.M., Perry, R., Small, A.M., & Green, W.H. (1984). Haloperidol in the treatment of infantile autism, American Journal of Psychiatry, 141(10), Baron-Choen, S., Leslie, A.M., & Frith, U. (1985). Does the autistic child have a “Theory of mine”? Cognition, 21(1), Bertrand, J., Mars, A., Boyle, C., Bove, F., Yeargin-Allsopp, M., & Decoufle, P. (2001). Prevalence of autism in a United States population: The Brick Township, New Jersey, investigation, Pediatrics, 108(5), Bishop, D.V. (1989). Autism, Asperger’s syndrome, and semantic-pragmatic disorder: Where are the boundaries? British Journal of Disordered Communication, 24(2), Bishop, D. (2011). How common is autism? Notes & Theories blog on guardian.co.uk (7 June 2011). Available from: Bishop, S.L., Richler, J., & Lord, C. (2006). Association between restricted and repetitive behaviors and nonverbal IQ in children with autism spectrum disorders. Child Neuropsychology, 12(4-5), Bowler, D.M. (1992). “Theory of mind” in Asperger’s Syndrome. Journal of Child Psychology and Psychiatry, 33(5), Brieber, S., Neufang, S., Bruning, N., Kamp-Becker, I., Remschmidt, H., Herpertz-Dahlmann, B., … & Konrad, D. (2007). Structural brain abnormalities in adolescents with autism spectrum disorder and patients with attention deficit/hyperactivity disorder. Journal fo Child Psychology and Psychiatry, 48(12), Carey, B. (2012). New definition of autism may exclude many, study suggests. The New York Times, A1. Charman, T., Baird, G., Simonoff, E., Loucas, T., Chandler, S., Meldrum, D., & Pickles, A. (2007). Efficacy of three screening instruments in the identification of autistic-spectrum disorders. British Journal of Psychiatry, Charman, T., Jones, C.R., Pickles, A., Simonoff, E., Baird, G., & Happe, F. (2011). Defining the cognitive phenotype of autism. Brain 1380,
. Patterns of growth in adaptive social abilities among children with autism spectrum disorders. Journal of Abnormal Child Psychology, 37(7), Baron-Cohen, S. (2009). The short life of a diagnosis. The New York Times. Available from Anderson, L.W., Campbell, M., Grega, D.M., Perry, R., Small, A.M., & Green, W.H. (1984). Haloperidol in the treatment of infantile autism, American Journal of Psychiatry, 141(10), Baron-Choen, S., Leslie, A.M., & Frith, U. (1985). Does the autistic child have a Theory of mine Cognition, 21(1), Bertrand, J., Mars, A., Boyle, C., Bove, F., Yeargin-Allsopp, M., & Decoufle, P. (2001). Prevalence of autism in a United States population: The Brick Township, New Jersey, investigation, Pediatrics, 108(5), Bishop, D.V. (1989). Autism, Asperger’s syndrome, and semantic-pragmatic disorder: Where are the boundaries British Journal of Disordered Communication, 24(2), Bishop, D. (2011). How common is autism Notes & Theories blog on guardian.co.uk (7 June 2011). Available from: Bishop, S.L., Richler, J., & Lord, C. (2006). Association between restricted and repetitive behaviors and nonverbal IQ in children with autism spectrum disorders. Child Neuropsychology, 12(4-5), Bowler, D.M. (1992). Theory of mind in Asperger’s Syndrome. Journal of Child Psychology and Psychiatry, 33(5), Brieber, S., Neufang, S., Bruning, N., Kamp-Becker, I., Remschmidt, H., Herpertz-Dahlmann, B., … & Konrad, D. (2007). Structural brain abnormalities in adolescents with autism spectrum disorder and patients with attention deficit/hyperactivity disorder. Journal fo Child Psychology and Psychiatry, 48(12), Carey, B. (2012). New definition of autism may exclude many, study suggests. The New York Times, A1. Charman, T., Baird, G., Simonoff, E., Loucas, T., Chandler, S., Meldrum, D., & Pickles, A. (2007). Efficacy of three screening instruments in the identification of autistic-spectrum disorders. British Journal of Psychiatry, Charman, T., Jones, C.R., Pickles, A., Simonoff, E., Baird, G., & Happe, F. (2011). Defining the cognitive phenotype of autism. Brain 1380,")
54
References Cicchetti, D.V., Koenig, K., Klin, A., Volkman, F.R., Paul, R., & Sparrow, S. (2011). From Bayes through marginal utility to effect sizes: A guide to understanding the clinical and statistical significant of the results of autism research findings. Journal of Autism Developmental Disorders, 41(2), Constantino, J.N., & Gruber, C.P. (2005). Social Responsiveness Scale Manual. Los Angeles: Western Psychological Services Croen, L.A., Grether, J.K., Hoogstrate, J., & Selvin, S. (2002). The changing prevalence of autism in California. Journal of Autism Developmental Disorders, 32(3), Dautenhahn, K., & Werry, I. (2004). Toward interactive robots in autism therapy, Pragmatics and Cognitions, 12(1), 1-35. Dawson, G., Webb, S.J., & McPartland, J. (2005). Understanding the nature of face processing impairment in autism: Insights from behavioral and electrophysiological studies. Developmental Neuropsychology, 27(3), Dominick, K.C., Davis, N.O., Lainhart, J., Tager-Flusberg, H., & Folstein, S. (2007). Atypical behaviors in children with autism and children with a history of language impairment. Developmental Disabilities, 29(2), Ecker, C., Marquand, A., Mourao-Miranda, J., Jonston, P, Daly, E.M., Brammer, M.J., … & Murphy, D.G. (2010). Describing the brain in autism in five dimensions-magnetic resonance imaging-assisted diagnosis of autism spectrum disorder using a multiparameter classification approach. Journal of Neuroscience, 30(32) Elsabbagh, M., Mercure, E., Hudry, K., Chandler, S., Pasco, G., Charman, T., … & Johnson, M.H. (2012). Infant neural sensitivity to dynamic eye gaze is associated with later emerging autism. Current Biology, 22, 1-5. Folstein, S., & Rutter, M. (1977). Infantile autism: A genetic study of 21 twin pairs. Journal of Child Psychology and Psychiatry, 18(4), Fombone, E. (2002). Prevalence of childhood disintegrative disorder. Autism, 6(2), Fombonne, E. (2003). Epidemiological surveys of autism and other pervasive developmental disorders: An update. Journal of Autism and Developmental Disorders, 33(4), Geschwind, D.H. (2011). Genetics of autism spectrum disorders. Trends in Cognitive Science, 15(9),
. From Bayes through marginal utility to effect sizes: A guide to understanding the clinical and statistical significant of the results of autism research findings. Journal of Autism Developmental Disorders, 41(2), Constantino, J.N., & Gruber, C.P. (2005). Social Responsiveness Scale Manual. Los Angeles: Western Psychological Services. Croen, L.A., Grether, J.K., Hoogstrate, J., & Selvin, S. (2002). The changing prevalence of autism in California. Journal of Autism Developmental Disorders, 32(3), Dautenhahn, K., & Werry, I. (2004). Toward interactive robots in autism therapy, Pragmatics and Cognitions, 12(1), Dawson, G., Webb, S.J., & McPartland, J. (2005). Understanding the nature of face processing impairment in autism: Insights from behavioral and electrophysiological studies. Developmental Neuropsychology, 27(3), Dominick, K.C., Davis, N.O., Lainhart, J., Tager-Flusberg, H., & Folstein, S. (2007). Atypical behaviors in children with autism and children with a history of language impairment. Developmental Disabilities, 29(2), Ecker, C., Marquand, A., Mourao-Miranda, J., Jonston, P, Daly, E.M., Brammer, M.J., … & Murphy, D.G. (2010). Describing the brain in autism in five dimensions-magnetic resonance imaging-assisted diagnosis of autism spectrum disorder using a multiparameter classification approach. Journal of Neuroscience, 30(32) Elsabbagh, M., Mercure, E., Hudry, K., Chandler, S., Pasco, G., Charman, T., … & Johnson, M.H. (2012). Infant neural sensitivity to dynamic eye gaze is associated with later emerging autism. Current Biology, 22, 1-5. Folstein, S., & Rutter, M. (1977). Infantile autism: A genetic study of 21 twin pairs. Journal of Child Psychology and Psychiatry, 18(4), Fombone, E. (2002). Prevalence of childhood disintegrative disorder. Autism, 6(2), Fombonne, E. (2003). Epidemiological surveys of autism and other pervasive developmental disorders: An update. Journal of Autism and Developmental Disorders, 33(4), Geschwind, D.H. (2011). Genetics of autism spectrum disorders. Trends in Cognitive Science, 15(9),")
55
References Gillespie-Lynch, K., Sepeta, L., Wang, Y., Marshall, S., Gomez, L., Sigman, M., & Hutman, T. (2012). Early childhood predictors of the social competence adults with autism. Journal of Autism Developmental Disorders, 42(2), Gotham, K., Risi, S., Pickles, A., & Lord, C. (2007). The Autism Diagnostic Observation Schedule: Revised algorithms for improved diagnos validity. Journal of Autism Developmental Disorders, 37(4), Harris, G.J., Chabris, C.F., Clark, J., Urban, T., Aharon, I., Steele, S. … & Tager-Flusberg, H. (2006). Brain activation during semantic processing in autism spectrum disorders via functional magnetic resonance imaging. Brain Cognition, 61(1), Hazlett, H.C., Poe, M.D., Gerig, G., Styner, M., Chappell, C., Smit, R.G., & Piven, J. (2011). Early brain overgrowth in autism associated with an increase in cortical surface area before age 2 years. Archives of General Psychiatry, 68(5), Insel, T.R., & Cuthbert, B.N. (2009). Endophenotypes: Bridging genomic complexity and disorder heterogeneity, Biological Psychiatry, 66(11), Jones, W., Carr, K., & Klin, A. (2008). Absence of preferential looking to the eyes of approaching adults predicts level of social desirability in 2-year-old toddlers with autism spectrum disorder. Archives of General Psychiatry, 65(8), Juranek, J., Filipek, P.A., Berenji, G.R., Modahl, C., Osann, K., & Spench, M.aA. (2006). Association between amygdala volume and anxiety level: Magnetic resonance imaging (MRI) study in autistic children. Journal of Child Neurology, 21(12), Kaiser, M.D>, Hudac, C.M., Shultz, S., Lee, S.M., Cheung, C., Berken, A.M., … & Pelphrey, K.A. (2010). Neural signatures of autism. National Academy of Science, 107(49), Kim, S.H., & Lord, C. (2010). Restricted and repetitive behaviors in toddlers and preschoolers with autism spectrum disorders based on the Autism Diagnostic Observation Schedules (ADOS). Autism, 3(4), Kleinhans, N.M., Richards, T., Weaver, K., Johnson, L.C., Greenson, J., Dawson, G., & Aylward, E. (2010). Association between amygdala response to emotional faces and social anxiety in autism spectrum disroders. Neuropsychologia, 48(12), Lee, H., Marvin, A.R., Watson, T., Piggot, J., Law, J.K., Law, P.A., … & Nelson, S.F. (2010). Accuracy of phenotyping of autistic children based on Internet implemented parent report. American Journal of Medicine, 153B(6), Leekam, S. Tandos, j., McConachie, H., Meins, E., Parkinson, K., Wright, C., … & Le Couteur, A. (2007). Repetitive behaviours in typically developing 2-year-olds. Journal of Child Psychology and Psychiatry, 48(11), Lord, C., & Bishop, S.L. (2010). Autism spectrum disorders: Diagnosis, prevalence, and services for children and families, Social Policy Report. Society for Research in Child Development, 24(2), 1-21.
. Early childhood predictors of the social competence adults with autism. Journal of Autism Developmental Disorders, 42(2), Gotham, K., Risi, S., Pickles, A., & Lord, C. (2007). The Autism Diagnostic Observation Schedule: Revised algorithms for improved diagnos validity. Journal of Autism Developmental Disorders, 37(4), Harris, G.J., Chabris, C.F., Clark, J., Urban, T., Aharon, I., Steele, S. … & Tager-Flusberg, H. (2006). Brain activation during semantic processing in autism spectrum disorders via functional magnetic resonance imaging. Brain Cognition, 61(1), Hazlett, H.C., Poe, M.D., Gerig, G., Styner, M., Chappell, C., Smit, R.G., & Piven, J. (2011). Early brain overgrowth in autism associated with an increase in cortical surface area before age 2 years. Archives of General Psychiatry, 68(5), Insel, T.R., & Cuthbert, B.N. (2009). Endophenotypes: Bridging genomic complexity and disorder heterogeneity, Biological Psychiatry, 66(11), Jones, W., Carr, K., & Klin, A. (2008). Absence of preferential looking to the eyes of approaching adults predicts level of social desirability in 2-year-old toddlers with autism spectrum disorder. Archives of General Psychiatry, 65(8), Juranek, J., Filipek, P.A., Berenji, G.R., Modahl, C., Osann, K., & Spench, M.aA. (2006). Association between amygdala volume and anxiety level: Magnetic resonance imaging (MRI) study in autistic children. Journal of Child Neurology, 21(12), Kaiser, M.D>, Hudac, C.M., Shultz, S., Lee, S.M., Cheung, C., Berken, A.M., … & Pelphrey, K.A. (2010). Neural signatures of autism. National Academy of Science, 107(49), Kim, S.H., & Lord, C. (2010). Restricted and repetitive behaviors in toddlers and preschoolers with autism spectrum disorders based on the Autism Diagnostic Observation Schedules (ADOS). Autism, 3(4), Kleinhans, N.M., Richards, T., Weaver, K., Johnson, L.C., Greenson, J., Dawson, G., & Aylward, E. (2010). Association between amygdala response to emotional faces and social anxiety in autism spectrum disroders. Neuropsychologia, 48(12), Lee, H., Marvin, A.R., Watson, T., Piggot, J., Law, J.K., Law, P.A., … & Nelson, S.F. (2010). Accuracy of phenotyping of autistic children based on Internet implemented parent report. American Journal of Medicine, 153B(6), Leekam, S. Tandos, j., McConachie, H., Meins, E., Parkinson, K., Wright, C., … & Le Couteur, A. (2007). Repetitive behaviours in typically developing 2-year-olds. Journal of Child Psychology and Psychiatry, 48(11), Lord, C., & Bishop, S.L. (2010). Autism spectrum disorders: Diagnosis, prevalence, and services for children and families, Social Policy Report. Society for Research in Child Development, 24(2),")
56
References Lord, C., Luyster, R., Ruthrie, W., & Pickles, A. (2012). Patterns of Developmental trajectories in toddlers with autism spectrum disorders. Journal of Consulting and Clinical Psychology. Lord, C., Petkova, E., Hus, V., Gan, W., Lu, F., Martin, D.M., … & Risi, S. (2012). A Multivariate Study of the Clinical Diagnosis of Different Autism Spectrum Disorders. Archives of General Psychiatry, 69(3), Lord, C., Risi, S., DiLavore, P.S., Shulman, C., Thurm, A., & Pickles, A. (2006). Autism from 2 to 9 years of age. Archives of General Psychiatry, 63(6), Luyster, R., Gotham, K., Guthrie, W., Coffing, M., Petrak, R., Pierce, K., & Lord, C. (2009). The Autism Diagnostic Observation Schedule – toddler module: A new module of a standardized diagnostic measure for autism spectrum disorders. Journal of Developmental Disorders39(9), Parsons, S., & Mitchell, S. (2002). The potential of virtual reality in social skills training for people with autistic spectrum disorders, Journal of Intellectual Disability Research, 46(5), Pelphrey, K.A., Shultz, S., Hudac, C.M., & Vander, B.C. (2011). Research review: Constraining heterogeneity: The social brain and its development in autism spectrum disorder. Journal of Child Psychologica Psychiatry, 52(6), Piven, J., Arndt., Bailey, J., & Andreasen, N. (1996). Regional brain enlargement in autism: A magnetic resonance imaging study. Journal of the American Academy of Child and Adolescent Psychiatry, 35(4), Piven, J., Gayle, J., Landa, R., Wzorek, M., & Folstein, S. (1911). The prevalence of fragile X in a sample of autistic invididuals diagnosed using a standardized interview. Journal of the American Academy of Child and Adolescent Psychiatry, 30(5), Regier, D.A.E., Narrow, W.E.E., Kuhl, E.A.E., & Kupfer, D.J.E. (2011). The conceptual evolution of DSM-5. Washington DC: American Psychiatric Publishing Inc. Richler, J., Huerta, M., Bishop, S.L., & Lord, C. (2010). Developmental trajectories of restricted and repetitive behaviors and interests in children with autism spectrum disorders. Developmental Psychopathology, 22(1), Sanders, S.J., Ercan-Sencicek, A.G>, Hus, V., Luo, R., Murtha, M.T., Moreno-De_Luca, D., … & State, M.W> (2011). Multiple recurrent de novo CNVs, including duplications of the 7q11.23 Williams syndrome region, are strongly associated with autism. Neurology, 70(5), Sparks, B.F., Friedman, S.D>, Shaw, D.W., Aylward, E.H., Echelard, D., Artru, A.A. … & Dager, S.R. (2002). Brain structural abnormalities in young children with autism spectrum disorders. Neurology, 59(2), Tanguay, P.E. (2000). Pervasive developmental disorders: A 10-year review, Journal of American Academy of Child Adolescent Psychiatry, 39(9), Veenstra-Vanderweele, J., Christian, S.L., & Cook, E.H., JR. (2004). Autism as a paradigmatic complex genetic disorder. Annual Review of Genomics Human Genetics, 5, Virtues-Ortega, J. (2010). Applied behavior analytic intervention for autism ine arly childhood: Meta-analysis, meta-regression, and dose-response meta-analysis of multiple outcomes, Clinical Psychology Review, 30, Walker, D.R., Thompson, A., Zwaigenbaum, L., Goldberg, J., Bryson, S.E., Mahoney, W.J., … & Szatmari, P. (2004). Specifying PDD-NOS: A comparison of PDD-NOS, Asperger syndrome and autism. Journal of American Academy of Cild and Adolescent Psyciatry, 42(2), Wood, J., Drahota, A., Sze, K., Har, K., Chiu, A., & Langer, D.A. (2009). Cognitive behavioral therapy for anxiety in children with autism spectrum disorders: a randomized, controlled trial, Journal of Psychology and Psychiatry, 50(3),
. Patterns of Developmental trajectories in toddlers with autism spectrum disorders. Journal of Consulting and Clinical Psychology. Lord, C., Petkova, E., Hus, V., Gan, W., Lu, F., Martin, D.M., … & Risi, S. (2012). A Multivariate Study of the Clinical Diagnosis of Different Autism Spectrum Disorders. Archives of General Psychiatry, 69(3), Lord, C., Risi, S., DiLavore, P.S., Shulman, C., Thurm, A., & Pickles, A. (2006). Autism from 2 to 9 years of age. Archives of General Psychiatry, 63(6), Luyster, R., Gotham, K., Guthrie, W., Coffing, M., Petrak, R., Pierce, K., & Lord, C. (2009). The Autism Diagnostic Observation Schedule – toddler module: A new module of a standardized diagnostic measure for autism spectrum disorders. Journal of Developmental Disorders39(9), Parsons, S., & Mitchell, S. (2002). The potential of virtual reality in social skills training for people with autistic spectrum disorders, Journal of Intellectual Disability Research, 46(5), Pelphrey, K.A., Shultz, S., Hudac, C.M., & Vander, B.C. (2011). Research review: Constraining heterogeneity: The social brain and its development in autism spectrum disorder. Journal of Child Psychologica Psychiatry, 52(6), Piven, J., Arndt., Bailey, J., & Andreasen, N. (1996). Regional brain enlargement in autism: A magnetic resonance imaging study. Journal of the American Academy of Child and Adolescent Psychiatry, 35(4), Piven, J., Gayle, J., Landa, R., Wzorek, M., & Folstein, S. (1911). The prevalence of fragile X in a sample of autistic invididuals diagnosed using a standardized interview. Journal of the American Academy of Child and Adolescent Psychiatry, 30(5), Regier, D.A.E., Narrow, W.E.E., Kuhl, E.A.E., & Kupfer, D.J.E. (2011). The conceptual evolution of DSM-5. Washington DC: American Psychiatric Publishing Inc. Richler, J., Huerta, M., Bishop, S.L., & Lord, C. (2010). Developmental trajectories of restricted and repetitive behaviors and interests in children with autism spectrum disorders. Developmental Psychopathology, 22(1), Sanders, S.J., Ercan-Sencicek, A.G>, Hus, V., Luo, R., Murtha, M.T., Moreno-De_Luca, D., … & State, M.W> (2011). Multiple recurrent de novo CNVs, including duplications of the 7q11.23 Williams syndrome region, are strongly associated with autism. Neurology, 70(5), Sparks, B.F., Friedman, S.D>, Shaw, D.W., Aylward, E.H., Echelard, D., Artru, A.A. … & Dager, S.R. (2002). Brain structural abnormalities in young children with autism spectrum disorders. Neurology, 59(2), Tanguay, P.E. (2000). Pervasive developmental disorders: A 10-year review, Journal of American Academy of Child Adolescent Psychiatry, 39(9), Veenstra-Vanderweele, J., Christian, S.L., & Cook, E.H., JR. (2004). Autism as a paradigmatic complex genetic disorder. Annual Review of Genomics Human Genetics, 5, Virtues-Ortega, J. (2010). Applied behavior analytic intervention for autism ine arly childhood: Meta-analysis, meta-regression, and dose-response meta-analysis of multiple outcomes, Clinical Psychology Review, 30, Walker, D.R., Thompson, A., Zwaigenbaum, L., Goldberg, J., Bryson, S.E., Mahoney, W.J., … & Szatmari, P. (2004). Specifying PDD-NOS: A comparison of PDD-NOS, Asperger syndrome and autism. Journal of American Academy of Cild and Adolescent Psyciatry, 42(2), Wood, J., Drahota, A., Sze, K., Har, K., Chiu, A., & Langer, D.A. (2009). Cognitive behavioral therapy for anxiety in children with autism spectrum disorders: a randomized, controlled trial, Journal of Psychology and Psychiatry, 50(3),")
Similar presentations



 a. Joint attention b. Verbal.>")












 Rhonda Landwehr PESS 369-Adapted Aquatics 6/20/2006.>")


