Download presentation
Presentation is loading. Please wait.

1
Morals, Money, and Medical Citizenship
Nancy Olivieri, MD, FRCPC, Professor, Pediatrics, Medicine and Public Health Sciences, University of Toronto, Canada

2
“Riveting…a horror story on the involvement of corporations in university research”
But whatever their ultimate goals I would urge all of you to read “The Olivieri Report.” Now, you may think it may be rather self-absorbed behaviour to be recommending reading with my picture all over it, but in my defense I need to tell you that this volume – I should say this FIRST volume -- of this experience has been summed up as “reading like a horror story on the involvement of corporations in university research” Thompson J, Baird P, Downie J. The Olivieri Report: The complete text of the report of the independent committee of inquiry commissioned by the Canadian Association of University Teachers. Toronto: James Lorimer & Co. Publishers, 2001.

3
Thompson J, Baird P, Downie J. The Olivieri Report
“[The Olivieri case] raised issues of research ethics and academic freedom so important to the public interest that it has attracted national and international attention” “Unless the lessons are learned and changes made, there will be repetitions”

4
The outline of this story
Identification of potential risks in a clinical trial of children The backlash: administrative, legal, regulatory, scientific, professional, personal A nasty, destructive, no-one-wins story “Non- scientific” Issues arising: Conflicts of interest Medical citizenship and loyalty Academic “mobbing” The costs of “doing the right thing”

5
What the story is really about
An erosion of scientific integrity Obfuscation of medical evidence A failure to protect patients Repeatedly triumphant conflicts-of-interests A lost war on undeserved privilege No bending of arc toward justice Personal devastation, and professional ruin

6
Constraints on discussion
Apotex v Olivieri, December 2008 caut.ca search “Olivieri”

7
Where I was 1996 Clinician and researcher at HSC (1986- )
Research funded through MRC Completing 2nd term ( ) as Career Scientist, Ontario MOH Director, Clinical/Research Hemoglobin program Involved in international thalassemia work May 1996 Elected to ASCI Obtained MRC Scientist Award ( ) Promoted to Professor, Pediatrics & Medicine
 as Career Scientist, Ontario MOH. Director, Clinical/Research Hemoglobin program. Involved in international thalassemia work. May Elected to ASCI. Obtained MRC Scientist Award ( ) Promoted to Professor, Pediatrics & Medicine.")
8
Three trials of an iron chelator
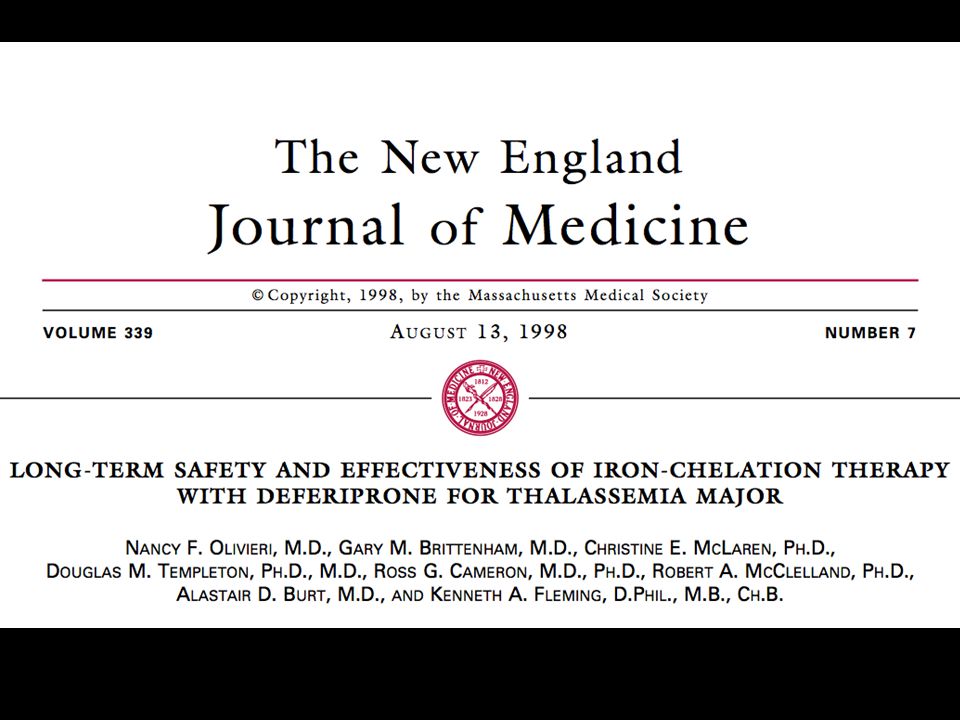
Long-term open-label trial 1989- PI Olivieri [Koren “pharmacokinetic studies”) RCT, deferiprone vs deferoxamine 1993- European “toxicity” trial Scientific Chairs Olivieri & Brittenham (CWRU)
 RCT, deferiprone vs deferoxamine European toxicity trial. Scientific Chairs Olivieri & Brittenham (CWRU)")
9
First potential risk identified in 1st (long-term) Toronto trial
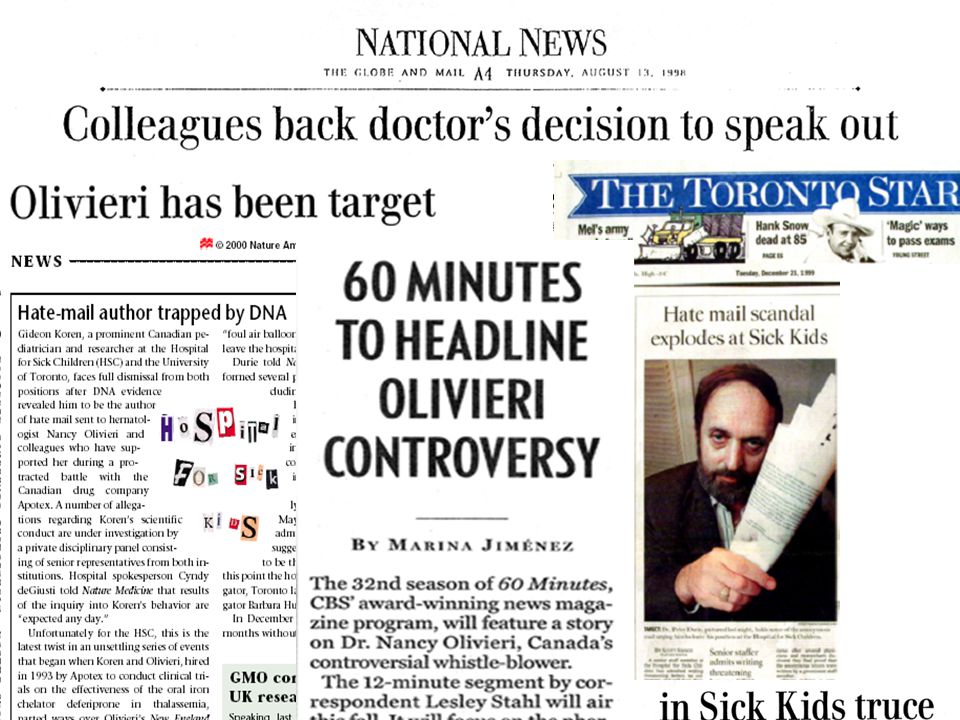
Potential lack of sustained efficacy: evidence from increasing/static [iron] in liver biopsies “Apotex disputed the risk, and the need to inform patients” Thompson et al, 2001 “Ax issued warnings of legal consequences to Dr. Olivieri should she inform patients or anyone else of the risk” Thompson et al, 2001 HSC REB Chair decreed revised consent forms May 20, 1996: revised forms sent to company May 24, 1996: termination of both trials:

10
Immediate outcomes Premature termination of trials
“All legal remedies” in writing and letters Overnight removal of drug from pharmacy Successful recruitment of “experts”, “expert panels”, and “key” experts to “dispute” findings Discreditation begins : ‘The picture painted … was of a scientist of almost breathtaking incompetence’ Successful engagement of patient organizations

11
Continuing drug administration
Abrupt termination left some patients unwilling to return to standard treatment “Apotex refused to re-instate the trials” Thompson et al, 2001 EDR : drug provided to informed patients Such patients were no longer in a trial* Dean decreed “very substantial research funding to Dr. Koren [continued]”

12
How could clinical trials be terminated?
“…no contractual basis for legal warnings” [legal distinction not appreciated] “Each of the two contracts specified … the right to terminate the corresponding trial at any time” MRC: no prohibition of confidentiality Any industrial sponsor could unilaterally terminate a (MRC co-sponsored) trial No (MRC) requirement to ensure patients not adversely affected
 trial. No (MRC) requirement to ensure patients not adversely affected.")
13
The [Olivieri/Koren/Apotex] “contract”
The University claimed widely (including in 12-point statement for Naimark) that Dr. Olivieri the author of her own misfortune by signing “the contract” University did not discuss Koren signature/ REB study approval/obtain legal opinion University’s Logic[?]: once the contract signed, it should have been honoured
![The [Olivieri/Koren/Apotex] contract](http://slideplayer.com/slide/3552912/12/images/13/The+%5BOlivieri%2FKoren%2FApotex%5D+contract.jpg "The University claimed widely (including in 12-point statement for Naimark) that Dr. Olivieri the author of her own misfortune by signing the contract University did not discuss Koren signature/ REB study approval/obtain legal opinion. University’s Logic[ ]: once the contract signed, it should have been honoured.")
14
Was this contract enforceable under common law?
“A physician is under a legal duty to disclose material or significant risks; failure may well amount to the tort of negligence” “Any term in a contract that prohibits disclosure that would amount to the commission of a tort is, to the extent that it does so, illegal and void” DA Soberman, Professor of Law Emeritus, Queen’s University

15
Was this contract enforceable under common law?
“The patient must be given the opportunity to decide whether to continue with treatment. The researcher does not have to establish the complete accuracy of her concern -- a risk is a risk, not a certainty -- but only that it was not an unreasonable concern” DA Soberman, Professor of Law Emeritus, Queen’s University

16
A second risk identified in 1st trial
Risk of progressive hepatic fibrosis Associated potential safety implications Followed by more legal warnings Led to return of all patients to standard Rx Only effective support was CMPA* “…not always effective” Thompson et al, 2001

17
Two risks First risk, 1996: increase in hepatic iron concentration -> possible inadequate sustained effectiveness Second risk, 1997: accelerated progression of hepatic fibrosis -> possible liver damage

18
Ongoing threats to disclosure
Malta 1997 meeting ; new opportunity for disclosure “[An attempt] through legal warnings to suppress information” Thompson et al, 2001 Our data taken and “re-interpreted” without knowledge Led to first substantive aggressive action by University: “Freidland committee”

19
A first “investigation”: The “Friedland Committee”
“Friedland Committee” evaluated complaint about data published without knowledge, attribution, or citation Friedland: “….no misconduct or serious scientific error was committed …” “Dr. Olivieri used poor judgment in bringing these very serious charges…”

20
“Some of the findings of the Friedland Committee are difficult to understand.” Thompson et al, “The [F] Committee reached the conclusion that ‘the authors committed no serious scientific error’ without … appropriate investigation” Thompson et al, 2001
![Some of the findings of the Friedland Committee are difficult to understand. Thompson et al, 2001 The [F] Committee reached the conclusion that ‘the authors committed no serious scientific error’ without … appropriate investigation Thompson et al, 2001](http://slideplayer.com/slide/3552912/12/images/20/Some+of+the+findings+of+the+Friedland+Committee+are+difficult+to+understand.+Thompson+et+al%2C+2001+The+%5BF%5D+Committee+reached+the+conclusion+that+%E2%80%98the+authors+committed+no+serious+scientific+error%E2%80%99+without+%E2%80%A6+appropriate+investigation+Thompson+et+al%2C+2001.jpg "Some of the findings of the Friedland Committee are difficult to understand. Thompson et al, 2001 The [F] Committee reached the conclusion that ‘the authors committed no serious scientific error’ without … appropriate investigation Thompson et al, 2001")
21
Subsequent actions by administration
“HSC and the University did not provide effective support to Dr. Olivieri during the first two and a half years of the controversy” “After the controversy became public, the University claimed that it had provided support, but this was not true.” Thompson et al, 2001

22
The Response of the Academic Institutions: Sick Kids and The University of Toronto
June 1996: Dean of Medicine:“It’s OK for company to stop the studies; it is paying. Don’t you think this will just blow over?” July 1996: Chairman of Pediatrics:“Not a matter in which the Hospital wishes to involve itself … this is a scientific controversy.” 1996 and 1997: Written legal threats copied to all

23
The academic institutions “did not provide effective support”
Research Accusations of sloppiness, incompetence, research misconduct HSC Executive: public circulation of allegations made by company against the quality of work Pressure to provide clinical data to company Harassment, marginalization of students and fellows: evicted; s, pagers, phones cut Delays in approval of research proposals Removal of research space Closure of lab

24
The institutions “did not provide effective support”
Clinical Clinic co-worker “replaced” by Chief’s “friend” Private “interviews” with nurses, students and fellows Patient encouraged to sue [HSC eventually pays] “Citizenship” graded as “0.5”: annual bonuses refused Successive “removals” from Directorship: ‘96, ‘98, ‘99 Erosion of resources for SCD patients Attempt to move office away to vacant, Q-fever-infected wing -- > Evacuation to lower floor -> Evacuation to TGH

25
The academic institutions “did not provide effective support”
Personal Whisper campaign: medical errors, stealing money from grants, misconduct, promiscuity Shunned at work by “friends” & co-workers Private s published front page, Nat /Post Documents about Olivieri circulated by HSC lawyer to OHA “by mistake” Twelve Clinical Chiefs “vote” to ‘remove’ Olivieri after SCD program cuts made public

28
Repeated appeals Approached: Eaton Professor of Medicine Philipson
Director, Research HSC, Buchwald Dean of Medicine, Aberman University Vice-President (Research), Munroe-Blum Provost, Sedra CAUT UTFA
, Munroe-Blum. Provost, Sedra. CAUT. UTFA.")
30
Donation discussions

31
Donation discussions “[This] controversy was linked to a much larger university-industry project” “Since the early 1990s, the University … had been engaged in discussions for a multimillion-dollar donation toward a new research centre” Thompson et al, 2001
![Donation discussions [This] controversy was linked to a much larger university-industry project](http://slideplayer.com/slide/3552912/12/images/31/Donation+discussions+%5BThis%5D+controversy+was+linked+to+a+much+larger+university-industry+project.jpg "Since the early 1990s, the University … had been engaged in discussions for a multimillion-dollar donation toward a new research centre Thompson et al,")
32
Donation discussions In 1998 “agreement in principle reached on … the largest donation University had ever received”, to be “matched to provide ≈$92 million” “After the controversy in media, donation discussions suspended, until matters ….resolved” Thompson et al, 2001

34
So for those who might think that this sounds like a long series of personal injuries, I take solace from the observation of Edison who noted that “you cannot have a sense of justice without a sense of injustice.” Universities, science and industry all play important roles in modern society. I would like to conclude by emphasizing that if universities are to add “innovation” to their three traditional roles of teaching, research and service to the community, this must be interpreted in a way which is supportive, not destructive, of the other three. It is common to talk of the responsibility of industry to make a profit for its shareholders. But industry concerned with health care, must recognise a responsibility to a broader public interest. Science, is now inextricably bound up with industry in many of its activities. The scientific community must take seriously what can properly be termed the corruption of its integrity where it involves suppression of unpalatable results and failure to declare a financial interest. I am immensely grateful for the support that I personally received from many members of the scientific community, and hope that it has moral resources to put its house in order.

35
A “public” inquiry gone wrong
HSC had no effective grievance procedure for staff (as of 2001, still no procedure in place) CEO rejects inquiry: “over my dead body” CEO appoints Dr. Arnold Naimark “[As president of U of M] Naimark had successfully lobbied Apotex for … just under $1 million … and was on the CIBC Board chaired by a member of the Hospital’s Board.” Thompson et al, 2001
 CEO rejects inquiry: over my dead body CEO appoints Dr. Arnold Naimark. [As president of U of M] Naimark had successfully lobbied Apotex for … just under $1 million … and was on the CIBC Board chaired by a member of the Hospital’s Board. Thompson et al,")
36
A “public” inquiry gone wrong
Public outrage expressed, but “Instead of recusing himself, Naimark accepted … in final 10 days joined by two academics” [Lowy and Knoppers] Naimark paid $150K for 10 weeks work

37
Assisting Naimark: Chairman of Peds Hugh O’Brodovich (“HOB”)
HOB “put forward incorrect allegations and testimony, to Naimark” …“used information from and with Dr. Koren” …“was seriously neglectful in not checking validity of testimony” Thompson et al, 2001

38
Assisting Naimark: REB chair Dr Aideen Moore
Dr Moore [REB Chair appointed shortly after trials terminated] “put forward incorrect testimony … [although] correct information was available to her….[Moore’s] information cited by Koren to bolster referrals to MAC and CPSO” Thompson et al, 2001

39
Assisting Naimark: Dr Gideon Koren
Koren, one of “primary submitters …” “forwarded allegations and testimony which he knew to be incorrect … cited ‘information’ he knew was mistaken” “Koren’s false allegations and testimony were believed” Thompson et al, 2001 Led to referral to Medical Advisory Committee Used to defend drug in legal proceedings

40
Naimarked: The Shadow of an “Independent” Inquiry
Olivieri entirely blameworthy, Hospital entirely innocent Empowerment of mobbers Imposition of “gag orders” Imposition of punitive financial and academic actions Another firing (#3) Libel in international press False accusations provided in Naimark led to Allegations of research misconduct: to University’s highest investigative Committee Allegations of medical misconduct: to licensing authority (CPSO) Allegations of research misconduct referred to University’s highest committee: dismissed Allegations of medical misconduct referred to highest medical licensing authority (CPSO): dismissed Hate mail : author identified through DNA & found guilty of professional and research misconduct “Gag orders” issued to all supporters: withdrawn Dismissed from position: re-instated Libel: CBS; international press: some damages awarded $20 million COUNTERSUIT for defamation and breach of contract: ongoing
 Libel in international press. False accusations provided in Naimark led to. Allegations of research misconduct: to University’s highest investigative Committee. Allegations of medical misconduct: to licensing authority (CPSO) Allegations of research misconduct referred to University’s highest committee: dismissed. Allegations of medical misconduct referred to highest medical licensing authority (CPSO): dismissed. Hate mail : author identified through DNA & found guilty of professional and research misconduct. Gag orders issued to all supporters: withdrawn. Dismissed from position: re-instated. Libel: CBS; international press: some damages awarded. $20 million COUNTERSUIT for defamation and breach of contract: ongoing.")
41
What Naimark et al “found”
After risks identified in data from liver biopsy, biopsy alleged to be unnecessary, risky, and obtained only for research purposes (“after similar criticisms of procedure by company” Thompson et al, 2001) “Concerns” that Dr. O had not notified REB, patients* Arising from Koren /HOB/ Moore/* / testimony All false Olivieri referred to MAC then CPSO
 Concerns that Dr. O had not notified REB, patients* Arising from Koren /HOB/ Moore/* / testimony. All false. Olivieri referred to MAC then CPSO.")
42
Proceeding from Naimark
Allegations & testimony {“concerns”} made in secret After spirited legal defense hired (and paid for) by Olivieri, most of the false testimony disclosed HSC abruptly announced [press conference] referral to CPSO - two weeks after compelled to acknowledge Koren’s misconduct For 18 months, HSC posted unfounded Olivieri accusations on a university-hospital web site Dean Naylor referred Koren’s accusations of research misconduct v Olivieri to Univ committee
 by Olivieri, most of the false testimony disclosed. HSC abruptly announced [press conference] referral to CPSO - two weeks after compelled to acknowledge Koren’s misconduct. For 18 months, HSC posted unfounded Olivieri accusations on a university-hospital web site. Dean Naylor referred Koren’s accusations of research misconduct v Olivieri to Univ committee.")
43
“The key organizational strategy is to transform [resistance] from an issue of policy and principle, into one of private disobedience and psychological disturbance” CF Alford. Whistleblowers: Broken lives and organizational power Cornell University Press
![The key organizational strategy is to transform [resistance] from an issue of policy and principle, into one of private disobedience and psychological disturbance CF Alford.](http://slideplayer.com/slide/3552912/12/images/43/The+key+organizational+strategy+is+to+transform+%5Bresistance%5D+from+an+issue+of+policy+and+principle%2C+into+one+of+private+disobedience+and+psychological+disturbance+CF+Alford..jpg "Whistleblowers: Broken lives and organizational power Cornell University Press.")
44
“This ain't the shop for justice.” Dickens

45
In the midst of Naimark, a series of anonymous letters….
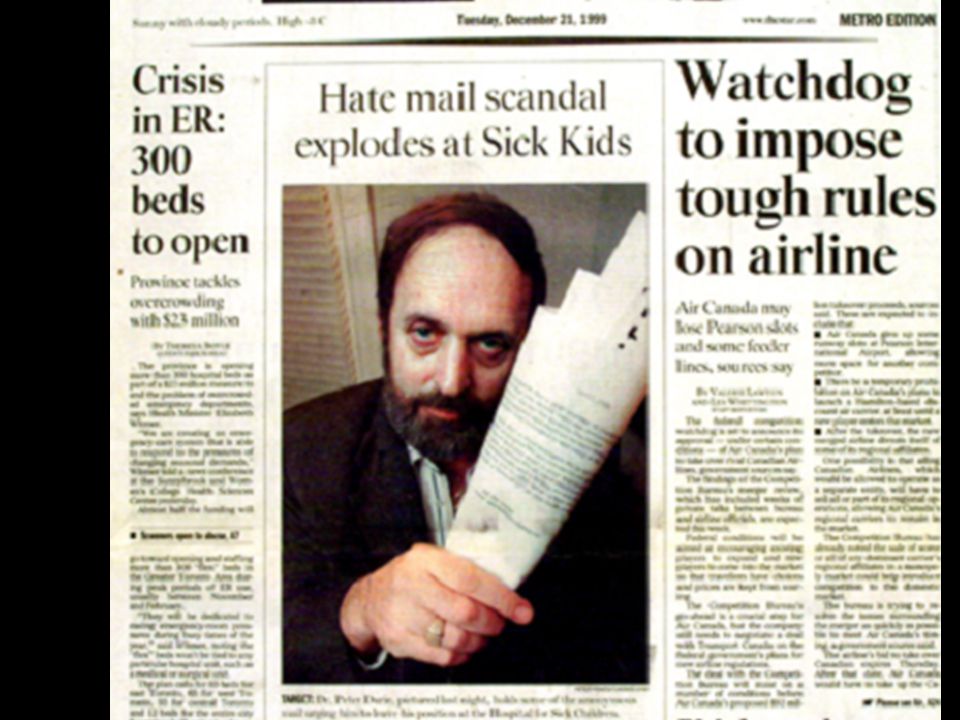
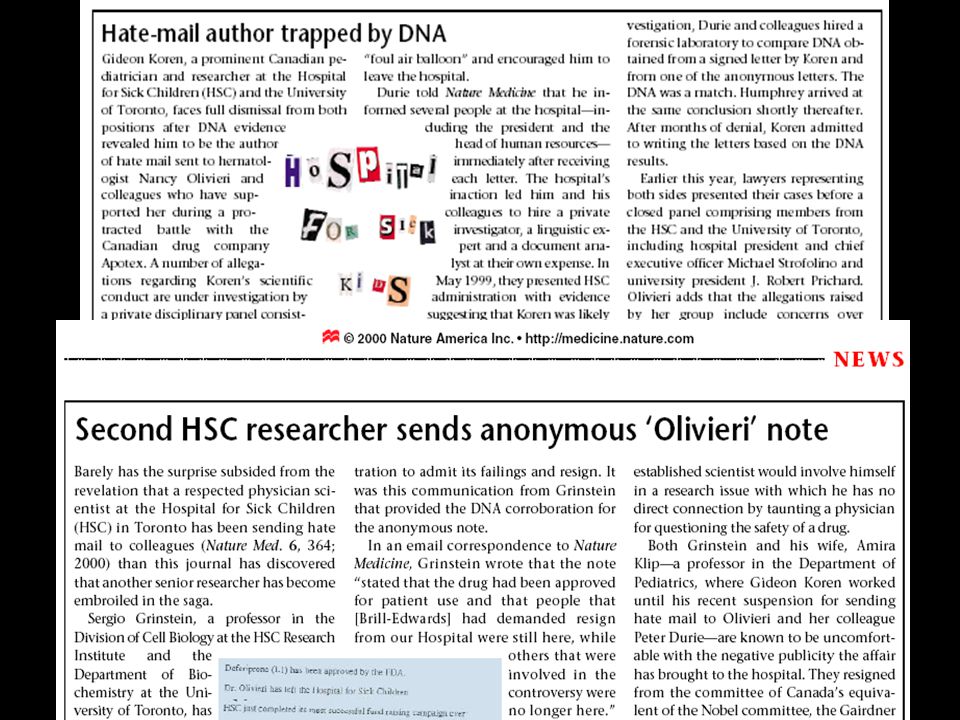
Seven months of harassing hate mail received by media and MDs at HSC A public inquiry for hate letters stalled “by lying” Finally author identified … by DNA on a licked stamp!

48
More familiar responses
HSC Chairman Aird: “unwanted letters” U of T & HSC President & CEO: “mitigating factors” “research accomplishments;” “recent MRC Scientist Award”; “outpouring of sympathy” Acquitted by CPSO On appeal to CPSO citizens’ panel, ruled guilty Suspended for five months: two without pay

49
Response to Koren hate mail
“Humphrey” hate mail investigation characterized by lying, blaming “secretaries”, institutional defensiveness Humphrey claimed x 7 months to be “stalled”; but “declined to accept” DNA evidence Humphrey recommended “mediation” with Koren as his targets bore responsibility for a “web of conflict in which Koren had become enmeshed”

50
“No dismissal for hate mail author” Nat Med June 2000

51
“I came to realize that, by comparison with reality, my story was as tame as a holiday postcard.”
John Le Carre

52
{Final CPSO decision on Koren issued by board of citizens on appeal}
“It defies belief that an individual of professed integrity could author such vicious [childish, vindictive, and dishonest] diatribes” “…only when confronted with irrefutable scientific evidence of guilt, did Koren admit as perpetrator” “Though claimed ‘extreme remorse’ …we are constrained to point out that Dr. Koren’s statement was silent on this issue”

53
Koren's proven misconduct “confided” by Dean Naylor to Faculty Council
Doctors for Research Integrity: April 22, 2002 : “HATE MAIL DOCTOR ESCAPES PENALTY FOR LATEST RESEARCH MISCONDUCT” Koren revealed guilty of research misconduct in studies published w/o knowledge of colleagues Announced penalty: withdrawal of offending article (*) made to “apologize” no discipline Koren's proven misconduct “confided” by Dean Naylor to Faculty Council
 made to apologize no discipline. Koren s proven misconduct confided by Dean Naylor to Faculty Council.")
54
Koren rehab program Awarded prizes by CDN Pharma societies, all widely trumpeted in CMAJ Awarded The Richard Ivey Foundation Chair at University of Western Ontario The “Local Hero of the Week”, Star The “hero of Shuchman’s book”

55
Yet more donation discussions…
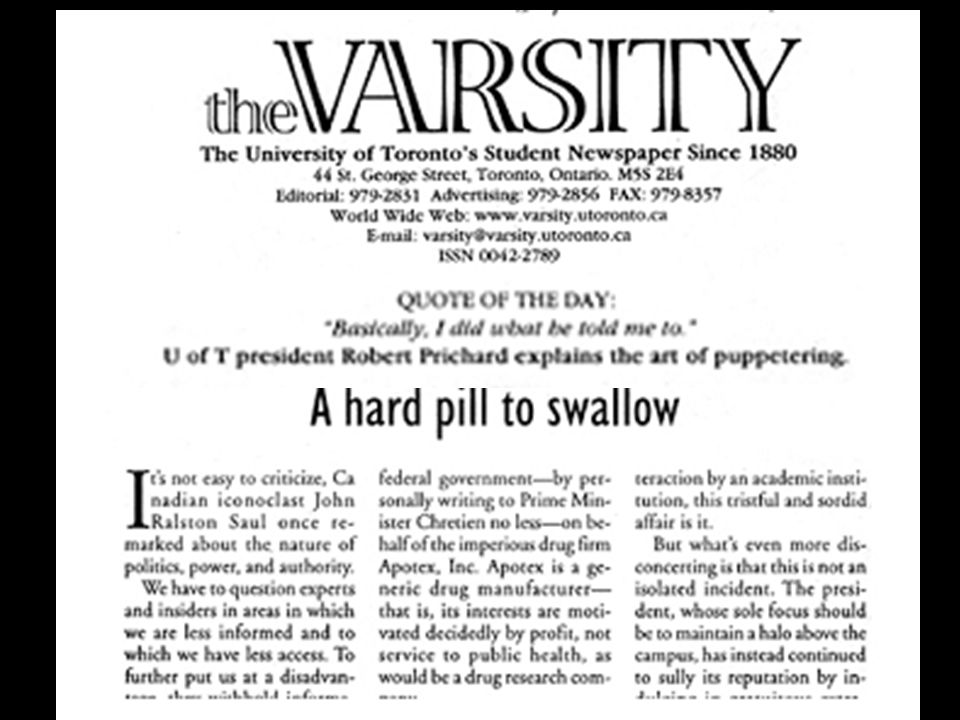
In 1999, company asked President Prichard to lobby Government against proposed changes to patent regulations that were adverse to company’s revenues Prichard wrote to PM Chretien, claiming that the proposed patent regulations “could jeopardize” funding of U of T’s building

57
End* of donation discussions
President P apologizes: “inappropriately” Lobbying against regulations unsuccessful 1999: company withdraws from agreement ‘donation-on-principle’ Smaller donation

58
J Med Ethics 2004;30:8-24. doi: 10.1136/jme.2003.005702
“Some were led to speculate that the University’s failure to recognise and support Olivieri’s academic freedom might not have been unconnected to its eagerness to secure financial support for the university’s proposed molecular medicine building project.” A Schafer. Biomedical conflicts of interest: a defence of the sequestration thesis: learning from the cases of Nancy Olivieri and David Healy J Med Ethics 2004;30:8-24. doi: /jme

59
Naimark’s last stand October 26, 2001: The Olivieri Report
December 18, 2001: Naimark/Lowy/Knoppers release new, false public accusations in their: “commentary on Report of the CAUT Committee” December 19, 2001: CPSO’s complete acquittal: “[O]judgement not only reasonable: commendable” January 2002: HSC “decides” not to appeal acquittal; Dean “decides” to drop “charges” of “misconduct”

60
“Five years after Apotex terminated the Toronto trials and issued its first legal warnings … the controversy continues, widened and intensified” Thompson et al, 2001

61
Pushback after acquittals:
Olivieri et al lodge grievances, multiple lawsuits, against University and Hospital HSC initiates action to quash summonses for documents in grievance. They lose. November 2002: Mediated settlement with Hospital and University L: Nader

62
Legal threats, claims and counterclaims arising from the controversy
(Threats) company vs Dr Olivieri, Gideon Koren vs Dr Brenda Gallie The Hospital for Sick Children vs Olivieri Deans Aberman, Naylor vs Arthur Schafer, D4R Olivieri vs Ax Ax vs Olivieri = countersuits Ax vs CBS (60 minutes) – dropped Olivieri et al vs The Hospital for Sick Children Olivieri v The Hospital for Sick Children Olivieri et al vs University of Toronto Olivieri v WmCarter, Borden Ladner [HSC lawyer] Olivieri v National Post Olivieri v CBC Olivieri v Stuart MacLeod (Koren mentor) Olivieri v Random House Canada, Shuchman Ax v Olivieri (2008) Olivieri vs The Commission of the European Communities, European Agency for the Evaluation of Medicinal Products and Apotex Europe Lehrer was asking Nader what he would do in and with the office of the presidency in the unlikely event that he won the election. How could Nader possibly appreciate the complex workings of all those vast and complex government agencies in Washington? Nader paused for a moment, as if he couldn't quite believe what he'd just heard. Then he laughed and said, "Well, I don't know anybody who has sued more of them."
 company vs Dr Olivieri, Gideon Koren vs Dr Brenda Gallie. The Hospital for Sick Children vs Olivieri. Deans Aberman, Naylor vs Arthur Schafer, D4R. Olivieri vs Ax. Ax vs Olivieri = countersuits. Ax vs CBS (60 minutes) – dropped. Olivieri et al vs The Hospital for Sick Children. Olivieri v The Hospital for Sick Children. Olivieri et al vs University of Toronto. Olivieri v WmCarter, Borden Ladner [HSC lawyer] Olivieri v National Post. Olivieri v CBC. Olivieri v Stuart MacLeod (Koren mentor) Olivieri v Random House Canada, Shuchman. Ax v Olivieri (2008) Olivieri vs The Commission of the European Communities, European Agency for the Evaluation of Medicinal Products and Apotex Europe. Lehrer was asking Nader what he would do in and with the office of the presidency in the unlikely event that he won the election. How could Nader possibly appreciate the complex workings of all those vast and complex government agencies in Washington Nader paused for a moment, as if he couldn t quite believe what he d just heard. Then he laughed and said, Well, I don t know anybody who has sued more of them.")
63
Where I am now : international research (Sri Lanka, Bangladesh, India) : Research outside of Asia [NIH] 2001: Sabbatical, MA Medical Ethics and Law 2003: Executive Director, Hemoglobal® 2006: Settlement with HSC; now at TGH 2009: UNI440 “Health and Pharmaceuticals”
![Where I am now : international research (Sri Lanka, Bangladesh, India) : Research outside of Asia [NIH]](http://slideplayer.com/slide/3552912/12/images/63/Where+I+am+now+%3A+international+research+%28Sri+Lanka%2C+Bangladesh%2C+India%29+%3A+Research+outside+of+Asia+%5BNIH%5D.jpg "2001: Sabbatical, MA Medical Ethics and Law. 2003: Executive Director, Hemoglobal® 2006: Settlement with HSC; now at TGH. 2009: UNI440 Health and Pharmaceuticals")
64
2009-2013 “Corporate UHN thinks you’re trouble”
Painful professional existence Groundswell of support at UHN retired TGH Admin refuse clinical care, impede research program, suggest resignation Hematologist “donates” $1M, hires MD Aggressive campaign against staff

65
Academic marginalization
“Pretty soon, you realize it’s not just the things you know you’re not getting that you’re not getting, you’re also not getting the things you don’t know you’re not getting” Healy D, in: review of The Drug Trial Monash Bioethics Review 2005; (24) 4
 4.")
66
Who helped? Who didn’t? “Gang of Four” One ethicist UTFA CAUT
Some colleagues, citizens, patients Most “friends”, “colleagues”, “public intellectuals” and patients CMAJ CBC Anonymous sources

67
What I still hear “This is such a complicated story.”
“You did the right thing, the wrong way.” “I did a lot behind the scenes.” “I’m so glad everything turned out OK.” “At least you appeared on 60 minutes.”

68
“We blew it, big.” An unidentified administrator at the Hospital for Sick Children, 2005

69
The last years (2001-2013) Settlements
2002: Olivieri et al, University & Hospital 2004: Olivieri, CBC 2004: Olivieri, company 2006: Olivieri, Hospital for Sick Children 2012: Olivieri Random House/Shuchman

70
If you have God, the facts, the law, and the press on your side, you have a 50:50 chance of defeating the bureaucracy

71
Dr. David Kern: “When Medical Science meets an Amoral Administration”
Founder and Director, Occupational Med, Brown Observed interstitial lung disease in workers at nearby industrial plant Published relationship between occupational exposure and disease Threatened with legal action by company Dismissed by Brown U The first example is that of Dr David Kern who was an occupational health physician at a hospital affiliated to Brown University, in Rhode Island when he observed a pattern of increased frequency of interstitial lung disease associated in workers at a nearby plant called Microfibres. Dr Kern submitted an abstract for a scientific meeting in which he detailed his perceived relationship between occupational exposure on the one hand and interstitial lung disease on the other. He was immediately threatened with legal action by Microfibres. The basis was that, at one of his visits as an occupational physician to the Rhode Island plant, he had signed a routine form on entry, agreeing not to reveal “trade secrets” which might be learned on the visit. Kern presented his findings to the American Thoracic Society and, a week later, was informed by the Hospital and the University that when his fixed-term contract of employment expired, it would not be renewed. The occupational health department at Brown, of which Kern was founder and Director, was closed. Kern has pointed out that Microfibres, Inc. was a donor to the hospital and that several members of the company owner’s family serve as members of the Memorial Hospital Corporation. After having relocated to another State, he published his findings in full in the Annals of Internal Medicine in 1998.

72
Dr. Aubrey Blumsohn, University of Sheffield “We are losing the battle over what it means to be an academic, and the raison d’etre of a university.” P & G repeatedly refused to provide raw data to academic “collaborators” to verify “ghost written” publications Data provided (3 years later, following press exposure) showed “fair” analysis would not have yielded findings desired by the sponsor Intriguing attempts made to prevent problem from being raised or discussed (See:
 showed fair analysis would not have yielded findings desired by the sponsor. Intriguing attempts made to prevent problem from being raised or discussed (See:")
73
Citizenship Noun: a legally recognized subject or national of a state or commonwealth …an inhabitant of a particular town or city

74
Medical Citizenship? Collegiality? Leadership? Professsionalism?
Resistance?

75
“Citizenship” “A tough occupation, which obliges the citizen to make his own informed opinion and stand by it” Martha Gellhorn

76
Medical Citizenship = Resistance?
One who raises concerns in the face of unethical, unsafe practices in medicine One who is [truly] “loyal to the profession of medicine, and just and generous to its members” “I represented the real organization. They said I was disloyal, but they’re the real traitors. They forgot who we were working for.” Quoted in Alford 2001

77
Problem is, nobody likes a whistleblower
“They invite snide remarks about their competency and their twisted motives. One man or woman against the medical establishment … is a minnow waiting to be crushed, shamed, and thrashed out of the medical profession. “We don't protect whistleblowers; we persecute them” Kamran Abbasi. A way forward for whistleblowing. J R Soc Med. 2011; 104: 275

78
Whistleblowing in medicine
Romanticized Rarely supported Most who attempt, become targets of career-ending retaliation

79
Workplace Mobbing Leymann (1980s): “impassioned, collective campaign to exclude, punish, and humiliate a target” observed in “ostensibly rational” workplaces Universities among most highly represented Shunning, gossip, ridicule, bureaucratic hassles, withholding of deserved rewards Loaded, stigmatizing term Well recognized; illegal in Europe [Quebec 2004] Ken Westhues
: impassioned, collective campaign to exclude, punish, and humiliate a target observed in ostensibly rational workplaces. Universities among most highly represented. Shunning, gossip, ridicule, bureaucratic hassles, withholding of deserved rewards. Loaded, stigmatizing term. Well recognized; illegal in Europe [Quebec 2004] Ken Westhues")
80
An erosion of citizenship in medicine?

81
Is academic medicine for sale?
M Angell, NEJM 2000;342:1516 No. The current owner is very happy with it. TJ Ruane, NEJM 2000;343:510

82
The Funding of Medical Research
Moses et al JAMA 2005; 294: Biomedical research funding increased from $37.1 billion in 1994 to $94.3 billion in 2003, a doubling when adjusted for inflation. Principal research sponsors were industry (57%) {BLUE} and the National Institutes of Health {GREY} (28%). in real terms Industry sponsorship of clinical trials more than tripled from $4 to $14 billion while NIH proportions were unchanged. 1 of 4 of academic investigators receive industry money 1 of 3 have personal financial ties with industry 50,000 U.S. clinical investigators received funding for one or more clinical trial in 2002 1/4 of investigators were found to have industry affiliations, and roughly 2/3 of academic institutions were found to hold equity in start-ups that sponsor research performed at the same institution. 60% of medical school adminisrators had personal relationships with industry including : consultancy arrangements, stock, equity in the companies doing research at their institutions, see Campbell 2007
 {BLUE} and the National Institutes of Health {GREY} (28%). in real terms Industry sponsorship of clinical trials more than tripled from $4 to $14 billion while NIH proportions were unchanged. 1 of 4 of academic investigators receive industry money. 1 of 3 have personal financial ties with industry. 50,000 U.S. clinical investigators received funding for one or more clinical trial in /4 of investigators were found to have industry affiliations, and roughly 2/3 of academic institutions were found to hold equity in start-ups that sponsor research performed at the same institution. 60% of medical school adminisrators had personal relationships with industry including : consultancy arrangements, stock, equity in the companies doing research at their institutions, see Campbell")
83
Medical researchers today find themselves in a conflict-of-interest
“A person is in a conflict-of-interest situation if she is in a relationship with another in which she has a moral obligation to exercise her judgment in that other’s service …and, at the same time, has an interest tending to interfere with the proper exercise of judgment in that relationship.” A Schafer But why look just at Big Pharma? Medical researchers face a conflict every day, while conducting research for an industry that pays them, that wants an answer that may or may not be true. researchers have a moral and legal obligation to patients in clinical studies, and in practice -- not the same as interest - it might be clearer if we called “working to develop drugs with the PI the way it is currently configured” a “conflict of obligation and interest.” Most of them will deny that this is a coi at all.

84
Conclusions of industry-sponsored randomized trials favour industry drugs
The finding that industry sponsored research produces results favorable to industry, is no surprise. He who pays the piper calls the tune. What this study by Bekelman did was to synthesize and summarize the increasing body of evidence for this statement from 8 studies which analyzed data from 1140 artciles over a period of approximately two decades ( ). This is another odds ratio -- you can see how far over to the right was the likelihood that conclusions from indsutry studies, vs nonindustry studies, will be favorable to the drug studied. Drug industry trials report favorably OVERWHELMINGLY on drug company drugs, THIS influences the findings of biomedical research in important ways.
. This is another odds ratio -- you can see how far over to the right was the likelihood that conclusions from indsutry studies, vs nonindustry studies, will be favorable to the drug studied. Drug industry trials report favorably OVERWHELMINGLY on drug company drugs, THIS influences the findings of biomedical research in important ways.")
85
“The privatization of profits and the socialization of losses” Ralph Nader
Research in publicly-funded institutions (=expertise, infrastructure) “partnered” by private industry (=profits) ‘Currency’ = publication A premium on ‘new’, ‘positive’ results
 partnered by private industry (=profits) ‘Currency’ = publication. A premium on ‘new’, ‘positive’ results.")
86
What Medical Schools Accept in Clinical Trial Agreements with Industry
Asked whether the industry sponsor may: Yes (%) No Unsure Decide whether results should not be published? 1 93 6 Make revisions to manuscript written by investigator? 89 Prohibit sharing raw data after trial over? 41 34 24 Write up results but investigator can “review and make suggestions”? 50 40 11 Own data? 80 16 5 Alter study design after agreement executed? 62 27 Mello et al. NEJM 2005;352:
 No. Unsure. Decide whether results should not be published Make revisions to manuscript written by investigator 89. Prohibit sharing raw data after trial over Write up results but investigator can review and make suggestions Own data Alter study design after agreement executed Mello et al. NEJM 2005;352:")
87
Why should doctors act as citizens?
The social /personal relationships once encountered eroded in one generation Shared backgrounds, interests, experiences are rare Manager CEOs are the new chiefs Apprentice-trainee relationships {“I trained with…”} have disappeared There is no common country

88
Why should doctors act as citizens?
Medicine is no longer “a calling” No sanctions for ‘making it’ with industry; rather, academic and personal rewards Endowed chairs are named for industrial giants, not admired physicians Doctors compete for: academic kudos; salaries; protected time; recognition Clinical/research tensions and hierarchy complicate collegiality

89
Reform?

90
Reform of academic research
The research agenda is dictated by a corporate imperative Research results follow industry funding across all studies The “evidence base” of medicine has been distorted Most scrutinised are the relationships that entail corporate funding of academic research: a recent review of the evidence found financial conflicts of interest to be "pervasive and problematic" in biomedical research. Strong and consistent evidence shows that industry sponsored research tends to draw conclusions favourable to industry and industry sponsored studies were much more likely to reach conclusions that were favourable to the sponsor than were non-industry studies. The explanations for the "systematic bias" in results is not that sponsored science is bad science but rather that the scientific questions being asked reflect the self interest of the sponsor.The concern is that the evidence base of healthcare is being distorted fundamentally.

91
Reform Return to public funding (“The sequestration package”, Schafer, 2004): tax corporations for profit from university research Establish individual and institutional policies to prevent entanglement with industry Scrutinize clinical trial agreements Establish a public data base (Rxisk.org) Improve internal complaint procedures Provide financial support for litigation Honor policies to preserve academic freedom, freedom of speech and publication
 Improve internal complaint procedures. Provide financial support for litigation. Honor policies to preserve academic freedom, freedom of speech and publication.")
92
CMA Policy Medical Professionalism http://policybase. cma
“The profession needs to meet [these] challenge[s] by demonstrating its ability to uphold its values and its commitment to doing so. Supporting strong and transparent self-regulatory systems will be a key component of this endeavour…”

93
Can citizenship be promoted?
“The world is a dangerous place, not because of those who do evil but because of those who look on and do nothing” Albert Einstein “The hottest places in hell are reserved for those who, in times of moral crisis, maintain their neutrality” Dante Aligheri

94
“There is no kingdom too small for a doctor to be king of”
John Green, Royal Society of Medicine

95
So for those who might think that this sounds like a long series of personal injuries, I take solace from the observation of Edison who noted that “you cannot have a sense of justice without a sense of injustice.” Universities, science and industry all play important roles in modern society. I would like to conclude by emphasizing that if universities are to add “innovation” to their three traditional roles of teaching, research and service to the community, this must be interpreted in a way which is supportive, not destructive, of the other three. It is common to talk of the responsibility of industry to make a profit for its shareholders. But industry concerned with health care, must recognise a responsibility to a broader public interest. Science, is now inextricably bound up with industry in many of its activities. The scientific community must take seriously what can properly be termed the corruption of its integrity where it involves suppression of unpalatable results and failure to declare a financial interest. I am immensely grateful for the support that I personally received from many members of the scientific community, and hope that it has moral resources to put its house in order.

96
What might help Systemic solutions: Clinical trials registry; industry-academic contract reform; regulatory reform Protection from scientific suicide: standing committee to appoint those w/o CsOI to assess “controversial” data: scientists & statisticians from “both sides” data anonymized opinions signed publish dissenting/minority opinions Sanctions for research misconduct Democratize the debate: level the playing field! offer legal fund for those attacked from within Increase awareness: Education. Un-purchase ethicists. Celebration of role models. Education!

97
Recommended Elliott, Carl White Coat, Black Hat. Adventures on the Dark Side of Medicine. Boston: Beacon Press. Healy, David Pharmageddon. University of California Press Abramson, John Overdosed America: The Broken Promise of American Medicine. New York: Harper. Angell, Marcia The Truth about the Drug Companies: How they Deceive us and what we can do about it. Random House Press
![]()
98
Recommended CF Alford, Whistleblowers: Broken lives and organizational power. Cornell University Press Westheus Ken Eliminating Professors: A Guide to the Dismissal Process. T Devine The Whistleblower’s Survival Guide: Courage without Martyrdom. Government Accountability Project: Washington

99
Recommended Schafer, A. Biomedical conflicts of interest: a defence of the sequestration thesis-learning from the cases of Nancy Olivieri and David Healy. J Med Ethics 2004; 30:8-24 Blumsohn A. While Rome burns: collusion with pharmaceutical scientific fraud and the prognosis for dispassionate academic discourse. CAFAS 2006 Young, T Death By Prescription: A father takes on his daughter's killer. Key Porter Books

Similar presentations
 is a review committee established to help protect the rights and welfare of human research subjects.>")



 Director, Center for Ethics Saint Joseph’s Health System, Atlanta,>")


 in Business by Simon Rogerson IMIS Journal May 1998.>")











