Download presentation
Presentation is loading. Please wait.

1
Practical Neuroimmunology: An update on Multiple Sclerosis Diagnosis and Treatments
Aaron Boster M.D. Assistant Professor of Neurology Division of Immunology The Ohio State University 1

2
Objectives 1. Learn to diagnosis MS
2. Learn to assess the risk of developing MS after a Clinically Isolated Syndrome 3. Become more familiar with MS therapeutics and treatment algorithms

3
Questions: 1. When faced with a clinically isolated syndrome, which tests can help delineate the risk to develop MS? 2. True or False: Starting MS therapies early improves long term outcome. 3. True or False: MS patients have high risk pregnancies.

4
What Is MS? An chronic inflammatory demyelinating disorder of the CNS of uncertain etiology, likely autoimmune, associated with destruction of myelin sheaths and axons Immuno-fluorescent confocal micrographs showing segmental demylination and axonal swelling in acute MS lesion. Trapp, 1998 4

5
MS Signs and Symptoms Fatigue Heat intolerance Visual symptoms
Numbness, tingling, loss of sensation Weakness Imbalance Urinary and sexual dysfunction Cognitive deficits

6
Epidemiology Peak age 15 to 45 Women : Men 2.5 : 1
Geographic variation USA prevalence 0.1% Approx ½ million MS patients in USA Life expectancy essentially normal Total lifetime cost > $2,200,000 6

7
Natural History of Multiple Sclerosis
Relapses and impairment cMRI activity (T2, T1+Gd) Axonal loss Measures of brain volume Secondary progressive Preclinical Relapsing-remitting Adapted from Goodkin DE. UCSF MS Curriculum. January 1999.
 Axonal loss. Measures of brain volume. Secondary progressive. Preclinical. Relapsing-remitting. Adapted from Goodkin DE. UCSF MS Curriculum. January")
8
Natural History of RRMS and PPMS
22 years from onset 5 years 50% need a cane 50% bed bound 15% PPMS 85% RRMS 26 years from onset 50% SPMS and 50% need a cane 90% SPMS 11-15 years Not completely ascertained cohort. from longitudinal natural history studies that have been done 50% (majority) will require assistance to walk in 10 years 20-25yrs is important because you are talking about a person who is maybe years old. 30 years from onset 83% need cane ~ 34% bed bound Weinshenker, 1989
 will require assistance to walk in 10 years yrs is important because you are talking about a person who is maybe years old. 30 years from onset. 83% need cane. ~ 34% bed bound. Weinshenker,")
9
CLINICALLY Pathologically Radiographically Rx Response
Isolated Syndrome Relapsing- Remitting Pre- Clinical Secondary Progressive INFLAMMATORY ACTIVITY Relapses Atrophy Active WML Poor Rx effect Rx effect No New WMLs Inflam dam occurs in early RRMS Brain dam by recur bouts of inflam even during ‘remission’ Accum disability at least in part 2/2 early active inflam dz We can treat inflam, At later dz stage, Rx not as effective PROGRESSION NEURODEGENERATION Time (Years)
")
10
CASE 1 30yo Science Teacher

11
CASE 1 30yo WF science teacher
1year ago, 3 week history of urinary urgency & frequency, one episode of fecal incontinence and bilateral foot numbness with frequent tripping 6 months ago, 2 week history of clumsy gait and poor balance, tremors of the right hand 1 month history of blurry vision with right gaze only 11

12
CASE 1 EXAM Left intranuclear ophthalmoplegia
Hyper-reflexia of the bilateral legs Bilateral upgoing toes (+ babinski) Absent vibration, poor proprioception in feet Mildly dysmetric finger-nose-finger and ataxic fine finger movements R>L + Romberg Ataxic gait 12
 Absent vibration, poor proprioception in feet. Mildly dysmetric finger-nose-finger and ataxic fine finger movements R>L. + Romberg. Ataxic gait. 12.")
13
CASE 1 Does she have MS? How do we diagnose MS?

14
MS Diagnosis “Dissemination in space and time”
14

15
Diagnostic Criteria Dawson criteria: 1916 Schumacher criteria: 1965
Poser criteria: 1983 McDonald criteria: 2001 Revised McDonald criteria: 2005 All criteria require dissemination in time and space

16
Summarized Diagnostic Criteria
1. Dissemination in space: Objective evidence of neurological deficits localized to two separate parts of the CNS 2. Dissemination in Time: Onset of neurological deficits separated by at least one month 3. Rule out other explanations! August November 16

17
New Diagnostic Criteria
Incorporate use of MRI Clinically Isolated Syndrom + MRI Dissemination in space + MRI Dissemination on time = Earlier MS Diagnosis DIS August November DIT 17

18
MRI - Dissemination in Space
3 of the following: 9 T2 or 1 Gd+ 3 Periventricular 1 Infratentorial 1 Juxtacortical lesion 18

19
MRI - Dissemination in Time
Gd Gd > 3 months T2 T2 > 1 month > 1 month CIS Polman, 2005 19

20
DIAGNOSTIC WORK UP History & Physical Exam Brain and Spinal Cord MRI
Labs: rule out mimics of MS Connective tissue diseases, infections, metabolic disorders Cerebrospinal Fluid (when clinical and MRI evidence inconclusive) Evoked Potentials: Identify damage to visual, auditory, & touch perception systems Less sensitive than MRI or cerebrospinal fluid 20
 Evoked Potentials: Identify damage to visual, auditory, & touch perception systems. Less sensitive than MRI or cerebrospinal fluid. 20.")
21
CSF Analysis • Most helpful for suggesting an alternative Dx
-high protein, marked pleocytosis, PMNs Elevated IgG Index >0.7 Increased CNS IgG synthesis, with normal serum IgG consistent with MS Oligoclonal Bands Presence of 2 distinct bands in CSF is consistent with MS 21

22
CSF OCB are not specific to MS!
Lupus 25% Sarcoidosis 51% Behcet’s dz 8% Syphillis CJD Whipple’s disease Lyme disease Vaculitidies Devic’s disease Healthy siblings of MS patients adapted from a lecture by Peter Riskind MD PhD 11/19/05 22

23
Differential Diagnosis
Metabolic: SCD (B12 def), Adrenomyeloneuropathy Connective Tissue Diseases: Sjogren’s, SLE Infectious: HIV, HTLV1, Lyme disease, Syphillis Structural: Chiari malformation, spinal cord compression Genetic: ataxias, paraplegias, mitochondrial Neoplastic: CNS lyphoma, paraneoplastic “MS variants”: ON, TM, ADEM, NMO Other: Neurosarcoidosis, CNS vasculitis Psychiatric 23
, Adrenomyeloneuropathy. Connective Tissue Diseases: Sjogren’s, SLE. Infectious: HIV, HTLV1, Lyme disease, Syphillis. Structural: Chiari malformation, spinal cord compression. Genetic: ataxias, paraplegias, mitochondrial. Neoplastic: CNS lyphoma, paraneoplastic. MS variants : ON, TM, ADEM, NMO. Other: Neurosarcoidosis, CNS vasculitis. Psychiatric. 23.")
24
CASE 1 NEWLY DIAGNOSED RRMS
> 2 historical events with objective findings on examination MRI consistent with MS Normal “rule out labs” CXR normal 24

25
Disease Modifying Therapies: 1993-2002
Glatiramer Acetate (Copaxone®) 1997 IFN -1b (Betaseron®) 1993 IFN -1a (Rebif®) 2002 IFN -1a (Avonex®) 1996 Type Polypeptide Recombinant Recombinant Recombinant mixture protein protein protein Indication Reduce freq. Reduce freq. Reduce freq. Slow prog. of relapses of relapses of relapses in relapsing in RRMS Slow Delay forms disability in disability in Prevent 2nd relapsing forms relapsing forms attack in CIS Injection SC SC SC IM Administration Daily Every other day 3x/week Weekly Dosage 20 mg 250 g (8 MIU) 44 g 30 g Immunomodulatory Treatments The long-term data that was published on glatiramer acetate1 involves a 6-year interim analysis of the ongoing 10-year open-label study. Some 8-year data are available. An extension of the pivotal North American study of IFN -1b (Betaseron®) provided placebo-controlled data for up to 5 years (median treatment period, 48.0 months).2 More recently, data from the 4-year extension of the PRISMS trial suggest that IFN -1a SC (Rebif®) may be efficacious for up to 4 years.3 No long-term studies (>2 years) have been published describing neurologic outcomes following the long-term use of IFN -1a IM (Avonex®). 1. Johnson KP, Brooks BR, Ford CC, et al. Sustained clinical benefits of glatiramer acetate in relapsing multiple sclerosis patients observed for 6 years. Mult Scler. 2000;6: 2. The IFNB Multiple Sclerosis Study Group and the University of British Columbia MS/MRI Analysis Group. Interferon beta-1b in the treatment of multiple sclerosis: final outcome of the randomized controlled trial. Neurology. 1995;45: 3. The PRISMS (Prevention of Relapses and Disability by Interferon--1a Subcutaneously in Multiple Sclerosis) Study Group. PRISMS-4: long-term efficacy of interferon--1a in relapsing MS. Neurology. 2001;56:
 IFN -1b. (Betaseron®) IFN -1a. (Rebif®) IFN -1a. (Avonex®) Type Polypeptide Recombinant Recombinant Recombinant. mixture protein protein protein. Indication Reduce freq. Reduce freq. Reduce freq. Slow prog. of relapses of relapses of relapses in relapsing. in RRMS Slow Delay forms. disability in disability in Prevent 2nd. relapsing forms relapsing forms attack in CIS. Injection SC SC SC IM. Administration Daily Every other day 3x/week Weekly. Dosage 20 mg 250 g (8 MIU) 44 g 30 g. Immunomodulatory Treatments. The long-term data that was published on glatiramer acetate1 involves a 6-year interim analysis of the ongoing 10-year open-label study. Some 8-year data are available. An extension of the pivotal North American study of IFN -1b (Betaseron®) provided placebo-controlled data for up to 5 years (median treatment period, 48.0 months).2 More recently, data from the 4-year extension of the PRISMS trial suggest that IFN -1a SC (Rebif®) may be efficacious for up to 4 years.3 No long-term studies (>2 years) have been published describing neurologic outcomes following the long-term use of IFN -1a IM (Avonex®). 1. Johnson KP, Brooks BR, Ford CC, et al. Sustained clinical benefits of glatiramer acetate in relapsing multiple sclerosis patients observed for 6 years. Mult Scler. 2000;6: The IFNB Multiple Sclerosis Study Group and the University of British Columbia MS/MRI Analysis Group. Interferon beta-1b in the treatment of multiple sclerosis: final outcome of the randomized controlled trial. Neurology. 1995;45: The PRISMS (Prevention of Relapses and Disability by Interferon--1a Subcutaneously in Multiple Sclerosis) Study Group. PRISMS-4: long-term efficacy of interferon--1a in relapsing MS. Neurology. 2001;56:")
26
Reduction in Relapse Rate:
2 year data from Phase III Studies 70 60 50 40 32 % Reduction vs Placebo 29 30 28 Reduction in Relapse Rate: Phase III Studies Glatiramer Acetate The effect of SC administration of glatiramer acetate (20 mg daily) on decreasing the primary endpoint of relapse rate in glatiramer acetate patients (n = 125) and placebo patients (n = 126) was evaluated in a randomized, placebo-controlled trial of RRMS patients. Data were analyzed at 3-month intervals using an ITT analyses using ANCOVA with tests for study-drug-by-center interaction and including the a priori–defined covariates: gender, disease duration (years), prior 2-year relapse rate, and baseline EDSS. The beneficial treatment effect of glatiramer acetate compared to placebo on decreasing relapse rate at month 3 was 17%, P = NS; at month 6 was 27%, P = 0.074; at month 9 was 25%, P = 0.047; at month 12 was 27%, P = 0.018; at month 15 was 24%, P = 0.034; at month 18 was 27%, P = 0.014; at month 24 was 29%, P = 0.007; and at approximately 30 months was 32%, P = IFN -1a IM Number of patients and P values given below are for ITT analyses using the likelihood ratio test done by CBER statistical review. 3-month 6.7% reduction stated in the summary basis for approval for Avonex 1995, on file at FDA, p.18. Annualized relapse rates for placebo patients (n = 142) = 1.04, for IFN-1a IM patients (n = 157) = 0.97, NS. 12-month 9.6% reduction stated in the OWIMS trial paper (Figure 3) by the OWIMS Study group.2 Original source: summary basis for approval for Avonex 1995, on file at FDA, p.18. Annualized exacerbation rates for placebo patients = 0.94, for IFN -1a IM patients = 0.85, so ( )/.94 = 9.57% reduction, NS. 24-month 18.3% reduction is derived from annualized relapse rates of all placebo (0.82) and all IFN -1a patients (0.67) as stated in Table 5 of the Jacobs et al.3: ( )/0.82 = 18.29% reduction, P = Summary basis for approval shows a similar 17.4% reduction (IFN -1a patients 0.673; n = 158; placebo patients 0.815; n = 143, P = 0.039). Jacobs et al. results were analyzed using ITT data assessment with likelihood ratio test.3 Note: Avonex advertises 32% reduction. That comes from a subgroup analysis of the data. Subgroup analysis data (placebo = 0.90 and IFN -1a = 0.61 annualized relapse rate, 32% reduction P = 0.002) includes only patients who completed the 104 weeks of the trial before it was stopped. IFN -1b Analyses of 12- and 24-month data comes from IFNB MS study group article in Neurology Analyses included a modified intent-to-treat analysis in which all data available for any given patient to the point of study completion or dropout was used. 12-month reduction of 33% comes from Table 1 of the IFNB MS study group article in Neurology Annual exacerbation rates for year 1 listed as 1.44 for Placebo (n = 123) and .96 for IFN-1b patients on 8 MIU (n = 124), P < 24-month reduction of 28% comes from Table 1 of the IFNB MS study group article in Neurology Annual exacerbation rates for year 2 listed as 1.18 for placebo (n = 110) and .85 for IFNB patients on 8 MIU (n=107), P < 0.03. Note: IFNB MS study group paper in Neurology 1993 (43 p. 657) lists a 33.8% reduction in relapse rate for 24 months (exacerbation rate for placebo patients = 1.27 and for IFN-1b patients 8 MIU = .84, P = ). IFN-1a SC 3-month reduction: in promotional materials the following is stated, “32% reduction in relapse frequency seen as early as Month 3 and continuing through Year 2 (1.73 vs 2.56; P < )” Information listed in promotional material as data on file. 12-month reduction of 37% for patients taking 44 ug of Rebif comes from page 1502 of the PRISMS report in Lancet 1998; 352: , P < 24-month reduction reduction of 32% for patients taking 44 ug of Rebif comes from Table 2 on page 1501 of the PRISMS report in Lancet 1998; 352: , P < Note: keep in mind, the percent value for mean relapses per patient listed in promotion material as stated as starting in month 3 is the same as that for 24 months as stated in PRISMs report. 1. Johnson KP, Brooks BR, Ford CC, et al. Onset of benefit of glatiramer acetate (Copaxone®) in patients with relapsing remitting multiple sclerosis (RRMS). ACRTIMS/ECTRIMS, September 2002, abstract 22. 2. The OWIMS (Once-Weekly Interferon for MS) Study Group. Evidence of Interferon B-1a dose response in relapsing-remitting MS: The OWIMS study. Neurology. 1999; 53: 3. Jacobs LD, Cookfair DL, Rudick RA, et al. Intramuscular interferon beta-1a for disease progression in relapsing multiple sclerosis. Ann Neurol. 1996;39: 4. The IFNB Multiple Sclerosis Study Group and the University of British Columbia MS/MRI Analysis Group. Interferon beta-1b in the treatment of multiple sclerosis: final outcome of the randomized controlled trial. Neurology. 1995;45: 18 20 10 Copxone Avonex Betaseron Rebif
 on decreasing the primary endpoint of relapse rate in glatiramer acetate patients (n = 125) and placebo patients (n = 126) was evaluated in a randomized, placebo-controlled trial of RRMS patients. Data were analyzed at 3-month intervals using an ITT analyses using ANCOVA with tests for study-drug-by-center interaction and including the a priori–defined covariates: gender, disease duration (years), prior 2-year relapse rate, and baseline EDSS. The beneficial treatment effect of glatiramer acetate compared to placebo on decreasing relapse rate at month 3 was 17%, P = NS; at month 6 was 27%, P = 0.074; at month 9 was 25%, P = 0.047; at month 12 was 27%, P = 0.018; at month 15 was 24%, P = 0.034; at month 18 was 27%, P = 0.014; at month 24 was 29%, P = 0.007; and at approximately 30 months was 32%, P = IFN -1a IM. Number of patients and P values given below are for ITT analyses using the likelihood ratio test done by CBER statistical review. 3-month 6.7% reduction stated in the summary basis for approval for Avonex 1995, on file at FDA, p.18. Annualized relapse rates for placebo patients (n = 142) = 1.04, for IFN-1a IM patients (n = 157) = 0.97, NS. 12-month 9.6% reduction stated in the OWIMS trial paper (Figure 3) by the OWIMS Study group.2 Original source: summary basis for approval for Avonex 1995, on file at FDA, p.18. Annualized exacerbation rates for placebo patients = 0.94, for IFN -1a IM patients = 0.85, so ( )/.94 = 9.57% reduction, NS. 24-month 18.3% reduction is derived from annualized relapse rates of all placebo (0.82) and all IFN -1a patients (0.67) as stated in Table 5 of the Jacobs et al.3: ( )/0.82 = 18.29% reduction, P = Summary basis for approval shows a similar 17.4% reduction (IFN -1a patients 0.673; n = 158; placebo patients 0.815; n = 143, P = 0.039). Jacobs et al. results were analyzed using ITT data assessment with likelihood ratio test.3. Note: Avonex advertises 32% reduction. That comes from a subgroup analysis of the data. Subgroup analysis data (placebo = 0.90 and IFN -1a = 0.61 annualized relapse rate, 32% reduction P = 0.002) includes only patients who completed the 104 weeks of the trial before it was stopped. IFN -1b. Analyses of 12- and 24-month data comes from IFNB MS study group article in Neurology Analyses included a modified intent-to-treat analysis in which all data available for any given patient to the point of study completion or dropout was used. 12-month reduction of 33% comes from Table 1 of the IFNB MS study group article in Neurology Annual exacerbation rates for year 1 listed as 1.44 for Placebo (n = 123) and .96 for IFN-1b patients on 8 MIU (n = 124), P < month reduction of 28% comes from Table 1 of the IFNB MS study group article in Neurology Annual exacerbation rates for year 2 listed as 1.18 for placebo (n = 110) and .85 for IFNB patients on 8 MIU (n=107), P < Note: IFNB MS study group paper in Neurology 1993 (43 p. 657) lists a 33.8% reduction in relapse rate for 24 months (exacerbation rate for placebo patients = 1.27 and for IFN-1b patients 8 MIU = .84, P = ). IFN-1a SC. 3-month reduction: in promotional materials the following is stated, 32% reduction in relapse frequency seen as early as Month 3 and continuing through Year 2 (1.73 vs 2.56; P < ) Information listed in promotional material as data on file. 12-month reduction of 37% for patients taking 44 ug of Rebif comes from page 1502 of the PRISMS report in Lancet 1998; 352: , P < month reduction reduction of 32% for patients taking 44 ug of Rebif comes from Table 2 on page 1501 of the PRISMS report in Lancet 1998; 352: , P < Note: keep in mind, the percent value for mean relapses per patient listed in promotion material as stated as starting in month 3 is the same as that for 24 months as stated in PRISMs report. 1. Johnson KP, Brooks BR, Ford CC, et al. Onset of benefit of glatiramer acetate (Copaxone®) in patients with relapsing remitting multiple sclerosis (RRMS). ACRTIMS/ECTRIMS, September 2002, abstract The OWIMS (Once-Weekly Interferon for MS) Study Group. Evidence of Interferon B-1a dose response in relapsing-remitting MS: The OWIMS study. Neurology. 1999; 53: Jacobs LD, Cookfair DL, Rudick RA, et al. Intramuscular interferon beta-1a for disease progression in relapsing multiple sclerosis. Ann Neurol. 1996;39: The IFNB Multiple Sclerosis Study Group and the University of British Columbia MS/MRI Analysis Group. Interferon beta-1b in the treatment of multiple sclerosis: final outcome of the randomized controlled trial. Neurology. 1995;45: Copxone. Avonex. Betaseron. Rebif.")
27
DMT Side Effects Glatiramer Acetate Interferons Flu-like symptoms
Injection Site Reactions Idiopathic Injection Reactions Interferons Flu-like symptoms Liver dysfunction Bone marrow Endocrine abnormalities Other: Depression Spasticity Headaches

28
Natalizumab Humanized monoclonal Antibody against 41 integrin
Selective adhesion-molecule inhibitor (SAM) Prevents transendothelial migration of activated leukocytes from small venules into CNS
 Prevents transendothelial migration of activated leukocytes from small venules into CNS.")
29
“68% relative reduction in the annualized
rate of relapse produced by natalizumab was maintained at two years (P<0.001)”
")
30
Kleinschmidt-DeMasters, 2005
3 patients with confirmed PML : 2 of 1171 MS patients (SENTINEL study: Natalizumab and INFβ-1a IM) 1 of 248 Crohn’s disease patients Incidence ~1:1000 for PML with Natalizumab Kleinschmidt-DeMasters, 2005
 1 of 248 Crohn’s disease patients. Incidence ~1:1000 for PML with Natalizumab. Kleinschmidt-DeMasters,")
31
Second Line Agents Tysabri IVIG
When a patient has failed or is otherwise unable to tolerate IFN and GA Tysabri IVIG

32
High School Football Star
CASE 2 High School Football Star

33
CASE 2 - 16yo AAM, High school Football star
Optic Neuritis, a Clinical Isolated Syndrome History: Woke blind in left eye, complains of pain with extra occular movements Exam: Va OD 20/20, OS 20/200. Left disk pallor, Left Afferent pupillary defect.

34
CASE 2 “Yes” “We need an MRI and LP” “Can I still play football?”
“What is my son’s risk of developing Multiple Sclerosis?” “Yes” “We need an MRI and LP”

35
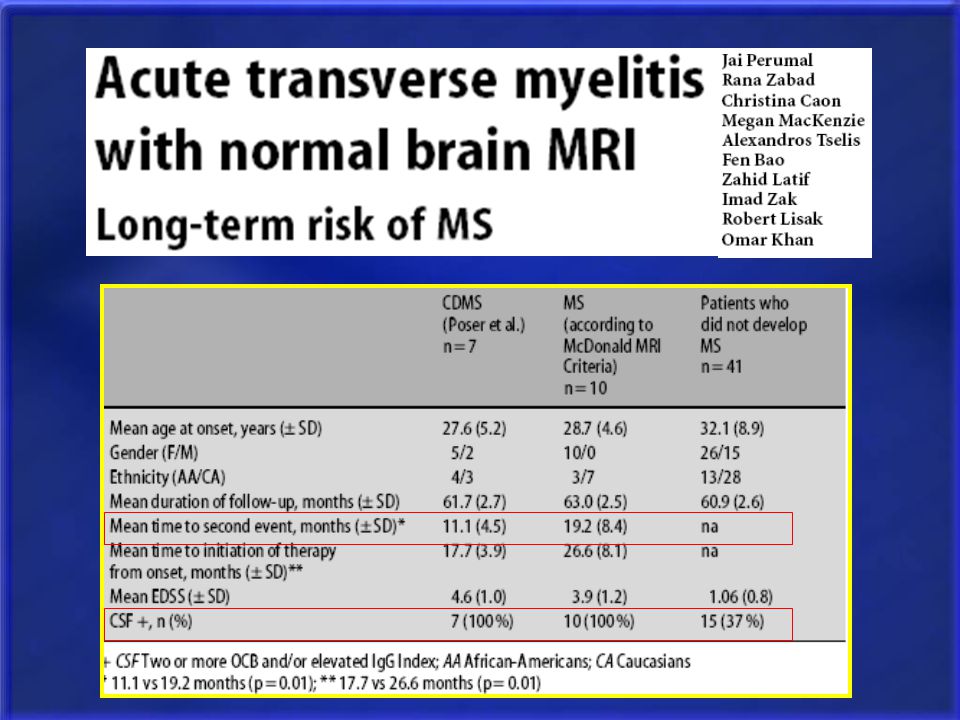
CASE 2

39
415 CIS pts with MRI & CSF and 50 month follow-up
+OBC doubled conversion risk to CDMS, independent of MRI findings 1a=reference category; N1=#pts developing CDMS; N2=#pts fulfilling baseline criteria; HR=hazard ratio adjusted by age, time on Rx, presence of OCB).
.")
40
Optic Neuritis, CIS WHAT ABOUT EARLY DMT? MRI Brain & C spine
CSF: IgGI, OCB, W,R,G,P IVMP 1gm daily x 5 days WHAT ABOUT EARLY DMT?

41
Avonex, Rebif, Betaseron, or Copaxone
CHAMPS, ETOMS, BENEFIT, PRECISE STUDIES First ever attack Second attack placebo Avonex, Rebif, Betaseron, or Copaxone Time to Second Attack Delayed with Treatment

44
CASE 3 26yo IRS agent

45
CASE 3 26yo LH WF with RRMS diagnosed 2yrs ago
3 day history of difficulty writing, clumsy and numb left hand No signs/symptoms of infection No prior history of similar symptoms

46
CASE 3 ACUTE MS RELAPSE IO & FE 4/5 on left hand
Hyper reflexia of left arm Ataxic FFM & dysmetric FNF on left Decreased LT on left face, arm, leg

47
CASE 3 Expanded Disability Status Scale EDSS=0 last 3 visits

48
CASE 3 Acute MS Relapse Expanded Disability Status Scale
Current EDSS=3

49
HOW TO IDENTIFY A RELAPSE?
CRITICAL, compare with previous examinations (history and examination), when ever possible Relapses can be precipitated by infections and fever Check U/A for occult UTI
, when ever possible. Relapses can be precipitated by infections and fever. Check U/A for occult UTI.")
50
TREATMENT OF RELAPSE INPATIENT OUTPATIENT Severe deficits
Risk of fall or other injury Poor social support OUTPATIENT All other relapses

51
TREATMENT OF RELAPSE: IV Solumedrol one gram daily for 5 days
Severe cases: up to 2 grams qd x 7d Oral Prednisone for special circumstances poor veins, insurance issues, travel, etc…

52
TREATMENT OF RELAPSE: PLASMAPHERESIS
Severe relapses not responding to steroids 5 to 7 courses done on alternate days for 2 weeks One course takes place over 3 to 4 hours

53
CASE 4 27yo Apartment Manager

54
CASE 4 Rapidly Worsening MS 27yo F diagnosed with RRMS 5 years ago
DMT with Rebif since diagnosis Suffered 3 MS relapses in past 15 months each treated with Solumedrol Incomplete recovery of cerebellar and pyramidal function EDSS 1 year ago was 2.5, now 5.5

55
Rapidly Worsening MS Treatment: Intense Immunosuppression
Documented worsening corresponding to >3 point EDSS increase in previous 12 months despite at least 6 months of IMT and at least 2 courses of IVMP Treatment: Intense Immunosuppression

56
Rationale for Intense Immunosuppression in Rapidly Worsening MS
Inflammatory damage occurs during early RRMS Permanent tissue damaged from recurrent bouts of inflammation, even during the silent periods of so-called remission Accumulated disability is at least in part secondary to early active inflammatory disease We can treat inflammation During later disease stages, there is no / less inflammation and our treatments are not effective

57
Boster, Lancet Neurology, 2008
GOOD IIS CANIDATE Active progression over past several months or frequent severe relapses 2. Age < 40 3. Ambulatory 4. Earlier disease course (RRMS or early SPMS) 5. Incomplete recovery from relapses 6. Frequent relapses leading to disability 7. Persistence of multiple Gd+ MRI lesions Boster, Lancet Neurology, 2008
 5. Incomplete recovery from relapses. 6. Frequent relapses leading to disability. 7. Persistence of multiple Gd+ MRI lesions. Boster, Lancet Neurology,")
58
Boster, Lancet Neurology, 2008
POOR IIS CANIDATE 1. Age > 50 2. Long-standing, stable disability -Predominantly motor or cerebellar deficits -Non-ambulatory status 3. Significant spinal cord atrophy 4. Significant other medical problems Boster, Lancet Neurology, 2008

59
Pulsed IVMP May attempt to “stabilize” disease course
1gram IVMP q15-30 days x 3-6 months CRITICAL to have close follow-up and document objective changes on exam

60
MITOXANTRONE Chemotherapy drug used to treat a variety of cancers since 1987 FDA approved for progressive forms of MS or worsening RRMS 12 mg/m2 q 3 months, many other regimens

61
CYCLOPHOSPHAMIDE Chemotherapy agent
Also used in other autoimmune disease Monthly IV infusion as an outpatient

62
Adverse RXN and Complications
CTX MITO Nausea / Alopecia + Myelosuppression Amenorrhea Hemorrhagic Cystitis - Remote Cancer + * Treatment Related Acute Leukemia ~ 0.23% Cardiotoxicity Amenorrhea: reversible in 1/3 women. Perm: 7% women < 35yo; 14% women >35yo Remote CA: not reported in MS but in Rx of CA and other AI d/o Cardio: max lifetime dose 140mg/m2. MUGA/ECHO before each infusion.

63
Natalizumab Not been studied in rapidly worsening MS
Extrapolate data from Phase II and AFFIRM trials Risk of PML

64
45yo Automotive Executive
CASE 5 45yo Automotive Executive

65
CASE 5 SPMS 45yo RH M with 13yr history of MS
DMT with Glatiramer Acetate Last MS relapse 7 years ago Ambulation: Cane 4 years ago Walker 3 years ago Wheelchair 1 year ago

66
Natural History of RRMS and SPMS
50% SPMS and 50% need a cane 85% RRMS 11-15 years 26 years from onset 90% SPMS 30 years from onset Not completely ascertained cohort. from longitudinal natural history studies that have been done 50% (majority) will require assistance to walk in 10 years 20-25yrs is important because you are talking about a person who is maybe years old. 83% need cane ~ 34% bed bound Weinshenker, 1989 66
 will require assistance to walk in 10 years yrs is important because you are talking about a person who is maybe years old. 83% need cane. ~ 34% bed bound. Weinshenker,")
67
Treating SPMS No treatment has been shown to be helpful UNLESS the patient still has superimposed relapses

69
Treating PPMS PROMiSe trial post hoc analysis Glatiramer Acetate slowed progression of disease in men with earlier disease IVIG Delayed progression by 12 wks vs PCB (Pohlau, 2007) Results need to be confirmed Consider challenge with steroids or IIS if relatively rapid decline in ADLs
 Results need to be confirmed. Consider challenge with steroids or IIS if relatively rapid decline in ADLs.")
70
CASE 6 36yo Physician

71
CASE 6 Wants to become pregnant 36yo WF with 4yr history of RRMS
Betaseron for past 3.5 years Last MS relapse 1 year ago EDSS 2, unchanged for past year Wants to become pregnant

72
Pre-pregnancy Counseling
MS not worsened by pregnancy Pregnancy not worsened by MS No differences in Prenatal Care MS has no known effect on fertility “High Risk” should be determined on obstetrical status and disease activity Little evidence to support increased risk of relapse with anesthesia administration Closely monitor for urinary tract infections

73
Pre-pregnancy Counseling
Lifetime Risk of MS (%) General population F 0.5 ; M 0.3 Child of MS patient 3-5 Sibling of MS patient 3 Monozygotic twin of MS patient 25-30 Only 10-15% of MS is familial
 General population. F 0.5 ; M 0.3. Child of MS patient Sibling of MS patient. 3. Monozygotic twin of MS patient Only 10-15% of MS is familial.")
74
Pregnancy and Relapse Rate
Pre-Pregnancy Post Partum PRIMS, n=254

75
Pre-Pregnancy Planning
Planned Pregnancy Discontinue DMT 1-2 menstrual cycles before planned conception Brain MRI Scan Unplanned Pregnancy First Trimester: Discontinue DMT Second Trimester: Review safety data

76
Relapses During Pregnancy
Risk-Benefit Assessment: severe motor, sensory or cerebellar deficits that affect ambulation IV Solumedrol (Cat C) Plasmapheresis IVIG (Cat C)
 Plasmapheresis. IVIG (Cat C)")
77
DMT During Pregnancy Insufficient data to support use of DMT
Interferons (Cat C, Abortifactant) Glatiramer acetate (Cat B) IVIG? (Cat C)
 Glatiramer acetate (Cat B) IVIG (Cat C)")
78
Post-Partum Management
Post-Partum DMT Resume soon after delivery or after breastfeeding Breastfeeding Not contraindicated But DMT pass into breast-milk May decrease relapse rate Post-Partum Relapses (~30%) Treat with IVMP (PE or IVIG) IVMP may impair wound healing ? Prophylaxis with IVIG
 Treat with IVMP (PE or IVIG) IVMP may impair wound healing. Prophylaxis with IVIG.")
79
Therapeutic Agents Under Investigation
MECHANISM ROUTE PHASE Rituxan Anti CD20 IV (2 x year) Phase II Campath Anti CD52 IV (1 x year) Daclizumab Anti CD25 IV or SC (q mo) Anti IL-12 SC (qw or qow) Statins immunomodulator oral Teriflunomide Phase III Anti VLA-4 SAM inhibitor FTY 720 Oral Cladribine immunosuppressant Minocycline Estriol MBP 8292 IV (q month)
 Phase II. Campath. Anti CD52. IV (1 x year) Daclizumab. Anti CD25. IV or SC (q mo) Anti IL-12. SC (qw or qow) Statins. immunomodulator. oral. Teriflunomide. Phase III. Anti VLA-4. SAM inhibitor. FTY 720. Oral Cladribine. immunosuppressant. Minocycline. Estriol. MBP IV (q month)")
80
Questions?

Similar presentations





 (MND) are a group of neurological disorders that selectively affect motor neurons.>")

 LaTasha Wilson Nate Jr.. Pathophysiology of MS In MS, the body’s own defense system attacks myelin, the fatty substance that surrounds.>")
>")





 is an inflammatory disease of the Central Nervous System (CNS) - that's the brain and spinal cord. Predominantly,>")
 & Multiple Sclerosis>")







, MRCP (UK)(Neurology), PhD February 12th 2015 First Fit Pathway & Multiple Sclerosis.>")
 By: Morgan Farr Biology 1010.>")