Download presentation
Presentation is loading. Please wait.

1
APIC IC Challenges in Dialysis
Danilo B. Concepcion,CBNT, CCHT-A Operations Manager, Renal Service The views and opinions are those of the author and does not reflect those of St. Joseph Hospital or any other organization.

2
Infections: A Major Patient Safety Problem in Dialysis – 2nd Leading Cause Of Death
UM-KECC, 2009 Approximately 15,000 dialysis patients die annually due to infections

3
IC Challenges in Dialysis
Temporal and spatial issues Water and dialysate Staffing matrix

9
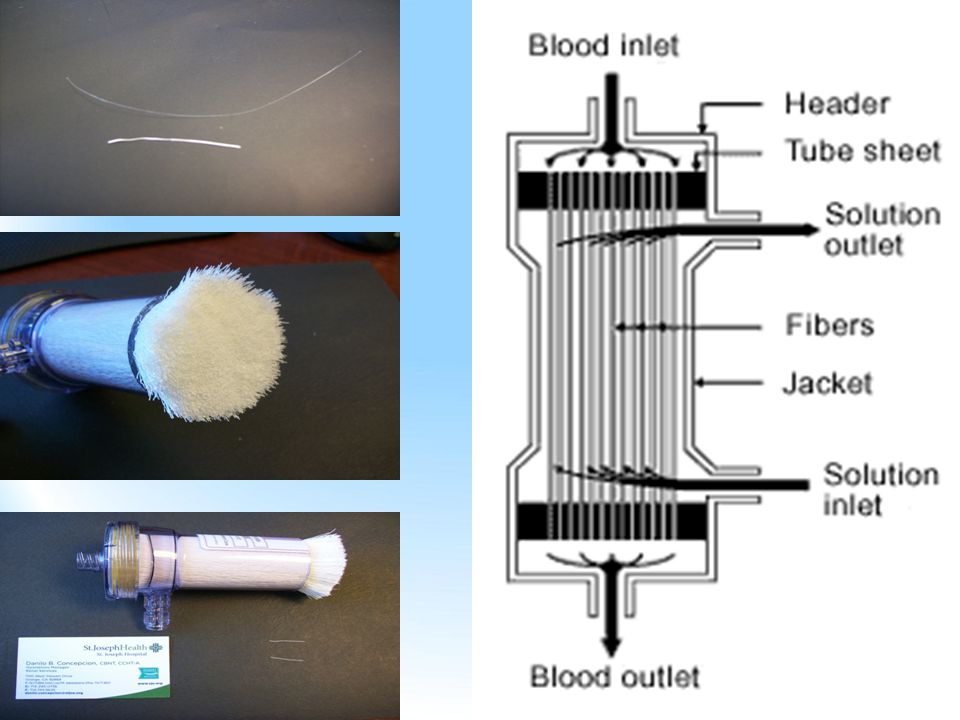
HOLLOW FIBERS Hollow fiber Fiber wall

11
DIFFUSION IN THE DIALYZER
Dissolved particles can move either way across the membrane. From blood to the dialysate. From dialysate to the blood. They will move from area of higher to lower concentration. Very important that precise electrolyte level of dialysate is known. This will determine what is removed or given to the patient.

12
MMWR Vol. 50/No.RR-5, page 23 “Hemodialysis in Acute-Care Settings” states: For patients with acute renal failure who receive hemodialysis in acute-care settings, Standard Precautions as applied in all health-care settings are sufficient to prevent transmission of bloodborne viruses. However, when chronic hemodialysis patients receive maintenance hemodialysis while hospitalized, infection control precautions specifically designed for chronic hemodialysis units should be applied to these patients. If both acute and chronic renal failure patients receive hemodialysis in the same unit, these infection control precautions should be applied to all patients

13
Why Is Infection Prevention Such a Challenge in Dialysis?
The in-center hemodialysis patient treatment reality: High risk for spread of blood-borne and other pathogens Staff caring for multiple patients w/short “changeover” times No physical separation of individual treatment stations Lots of potential blood exposure immunosuppressed dialysis patients compounded by…

14
Organisms remain viable on surfaces for prolonged periods
Recent Studies Illustrate How the Dialysis Facility Can Become a “Box of Bugs” Organisms remain viable on surfaces for prolonged periods Hepatitis B >1 week Influenza days MRSA days to 7 months VRE days to 4 months C. difficile spore months Kramer A, Schwebke I, Kampf G. BMC Infect Dis 6:130, 2006 Healthcare workers touch as many as 7 surfaces after touching a contaminated one! McLaughlin AC, Walsh F. Am J Infect Control 39(6): , 2011
: ,")
15
How Are Infections Spread in Dialysis?
Five main sources of pathogen transmission: 1. On the hands of staff going between patients & between common areas and patients 2. From ineffectively disinfected equipment & environmental surfaces 3. From contaminated supplies & medications 4. From inadequate vascular access care 5. From virulent pathogens (e.g. hepatitis B)
")
16
Dialysis Patient Infections Can Be Prevented by:
Following good infection prevention and control practices The Centers for Disease Control and Prevention (CDC) has guidelines for these practices in dialysis facilities
 has guidelines for these practices in dialysis facilities.")
17
Remember the lesson from the Patient Safety Movement…
The CDC Guidelines Address general practices (wash hands, clean & disinfect equipment, etc.) Do not include details for application of the guidelines (what parts of the equipment need to be disinfected, etc.) Remember the lesson from the Patient Safety Movement… Staff need clear directions in what is expected of them in their duties…
 Do not include details for application of the guidelines (what parts of the equipment need to be disinfected, etc.) Remember the lesson from the Patient Safety Movement… Staff need clear directions in what is expected of them in their duties…")
18
NOTICE! National Opportunity To Improve Infection Control In ESRD
The NOTICE Initiative is funded by the Department of Health and Human Services to support the renal community in improving infection control We are VERY excited to tell you about the NOTICE Initiative. It is a truly collaborative endeavor involving dialysis providers, networks, and government agencies. The goal of the initiative is to reduce infections in dialysis patients through improved direct care delivery practices.

19
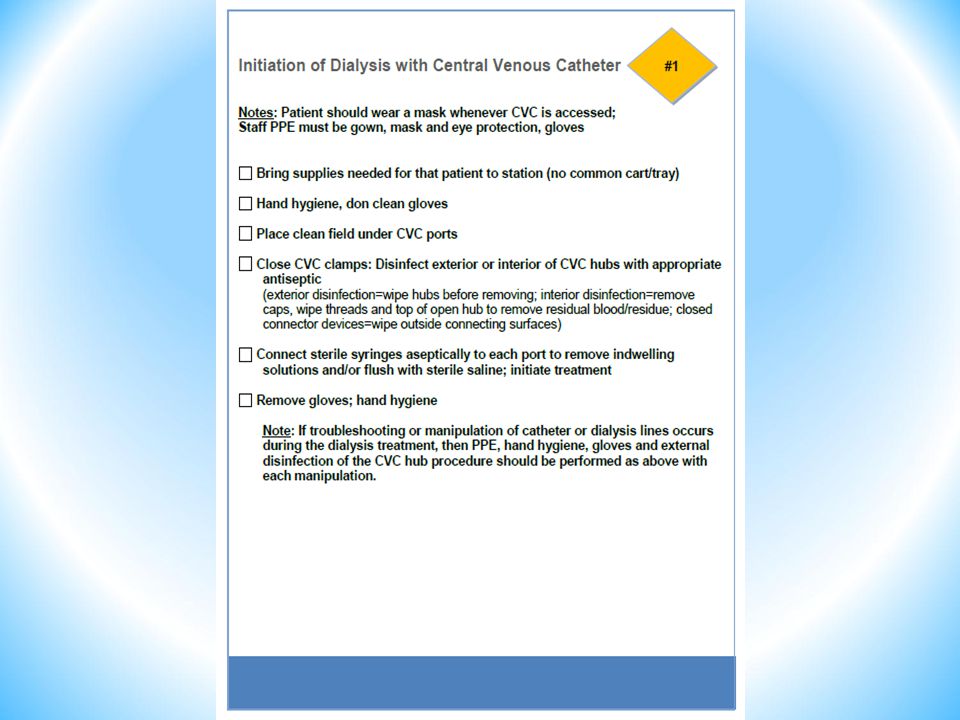
Infection Control Checklists for Dialysis
Initiation of Dialysis with CVC CVC Exit Site Care Discontinuation of Dialysis and Post Care of CVC Initiation of Dialysis with AVF/G Discontinuation of Dialysis and Post Care of AVF/G Parenteral Medication Preparation/Administration Cleaning & Disinfection of the Dialysis Station Supply Management & Contamination Prevention

28
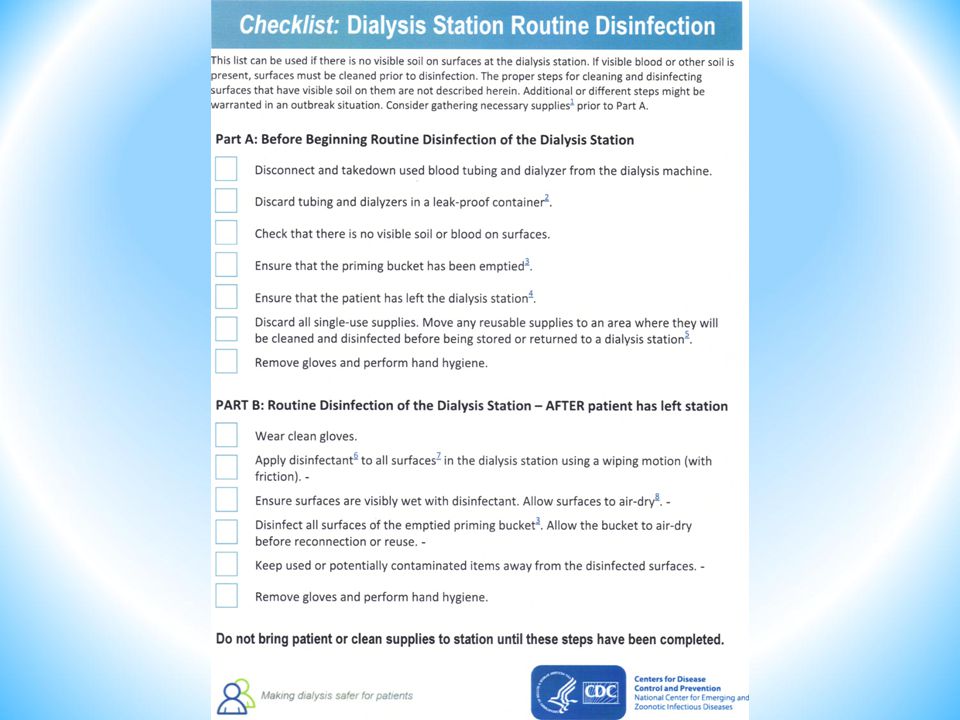
Note: It is not required that the patient has vacated the dialysis station before disinfection and preparation of the machine can be conducted. If the patient remains in the chair during disinfection, strictly adhere to separation b/t the patient and the disinfected/prepared machine.

32
The Infection Control Checklists Don’t Address Everything on How to Protect Patients from HAI…

33
V120 Blood Contaminating a Pressure Transducer Filter

34
V128 Isolation of HBV+ Patients
Separate isolation room February 9, 2009 all new facilities must have a separate isolation room (waiver)… Separate isolation area If there are current HBV+ patients on census, the isolation area/room can not be used for HBV- patients on other shifts or days due to the risk of cross-contamination.
… Separate isolation area. If there are current HBV+ patients on census, the isolation area/room can not be used for HBV- patients on other shifts or days due to the risk of cross-contamination.")
35
V130 Separate dedicated supplies and equipment, including blood glucose monitors. Labeled “isolation” Concentrate containers

36
V131 Staff members caring for HBsAg positive patients should not care for HBV susceptible patients at the same time, including during the period when dialysis is terminated on one patient and initiated on another (e.g., during the same shift or during patient change-over). If a staff member assigned to care for an HVB+ patient must concurrently care for someone other than another HBV+ patient, the additional patient must be HBV immune
. If a staff member assigned to care for an HVB+ patient must concurrently care for someone other than another HBV+ patient, the additional patient must be HBV immune.")
37
Dialysate is the largest contact material a patient’s blood touches
The more pure and endotoxin free the water and dialysate, the fewer Chronic Inflammatory Disease (CID) processes seen in patients over time
 processes seen in patients over time.")
39
Definitions of Quality for Dialysis
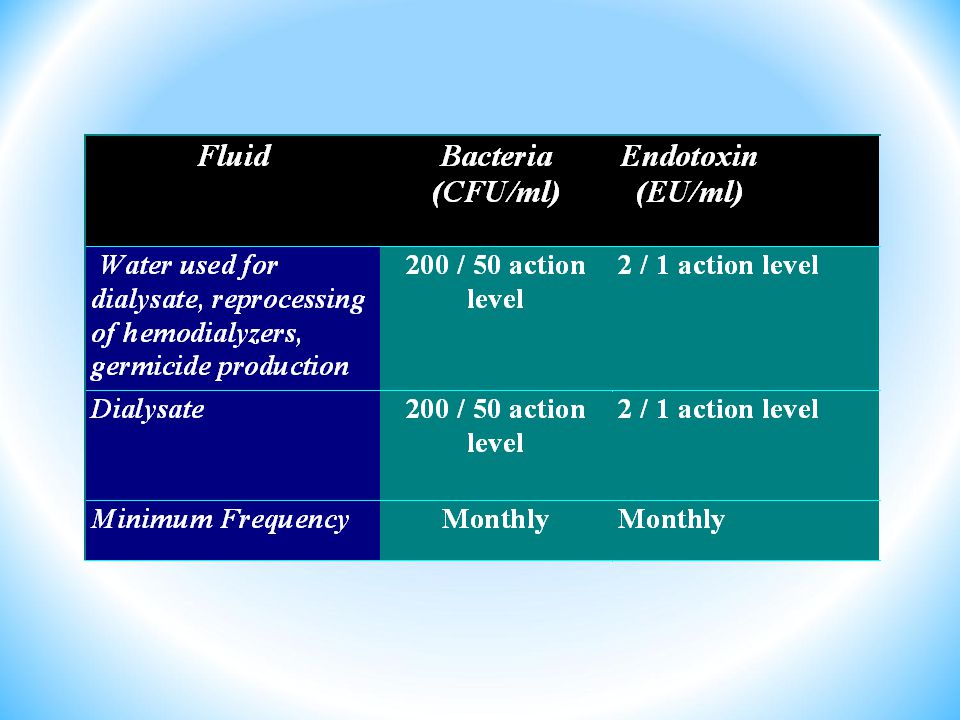
Reference Allowable water TVC Action level water TVC Allowable Level water EU Action Level water EU RD52:2004 <200 <2 2 1 ANSI/AAMI/ISO 13959 <100 50 <0.25 0.125 ANSI/AAMI/ISO 23500 ANSI/AAMI/ISO 11663 Ultrapure <0.1 <0.03 Infusable (Sterile) Not listed in the standards Reference Allowable dialysate TVC Action level dialysate TVC Allowable Level dialysate EU Action Level dialysate EU RD52:2004 <200 <2 50 1 ANSI/AAMI/ISO 13959 <100 <0.5 0.25 ANSI/AAMI/ISO 23500 ANSI/AAMI/ISO 11663 Ultrapure <0.1 <0.03 Infusable (Sterile) 10-6 Chemical Contaminant maximum allowable levels equal in all references.
 Not listed in the standards. Reference. Allowable dialysate TVC. Action level dialysate TVC. Allowable Level dialysate EU. Action Level dialysate EU. RD52:2004. <200. < ANSI/AAMI/ISO <100. < ANSI/AAMI/ISO ANSI/AAMI/ISO Ultrapure. <0.1. <0.03. Infusable (Sterile) Chemical Contaminant maximum allowable levels equal in all references.")
40
Disinfection Frequency
Distribution/Loop System Central systems at least once a month Disinfects water inlet line to hemodialysis machines Portables Dialysis Machines Daily OP Acute setting Bicarbonate mixing systems daily rinse Weekly disinfect Individual bicarbonate concentrate containers should rinsed and inverted to drain at end of each day disinfected weekly

41
Bacteria Testing Methods
Culture media should be trypticase soy agar (TSA) or equivalent No blood or chocolate agar Incubate at 35-37o C for 48 hours May want to go to 72 hours Count colonies with a magnifying device Shall not exceed 200 cfu/ml / 50 cfu action level
 or equivalent. No blood or chocolate agar. Incubate at 35-37o C for 48 hours. May want to go to 72 hours. Count colonies with a magnifying device. Shall not exceed 200 cfu/ml / 50 cfu action level.")
42
Bacteriology of the Dialysate
Collected during or at the termination of dialysis at or beyond the point where the dialysate leaves the hemodialyzer. AAMI: Two machines per month Each machine at least once annually The total viable bacteria count shall not exceed 200 cfu/ml.

43
Bacteriology of water V178 IG: the final decision of whether to discontinue dialysis rests with the medical director of a facility. V179 IG: “Promptly” would be met if action is taken within 48 hours of receiving the results of testing.”

44
Endotoxins By-products of water-borne gram negative bacteria
Reside in the cell wall Released when the bacteria dies Enter bloodstream Build-up in Reprocessed Hemodialyzers Back Diffusion* Back Filtration* Sense Bacteria/Endotoxin

45
Limulus Amebocyte Lysate (LAL) Assay
Do disinfect the ports with LAL testing <2 EU > 1EU action level Current testing can be done in-center Perform a control with each batch of tests Outside labs usually require freezing or refrigerated specimen and have better sensitivities Frequency monthly If suspected endotoxin reaction

46
Long-term Effects Attributed to Chronic Micro-Inflammation
Malnutrition Low albumin Muscle protein wasting Protein catabolism Increased CRP Atherosclerosis Low cholesterol synthesis Increased ferritinlevels Resistance to EPO therapy Bone disease, cysts, fractures Sleep disorders Anti- endotoxinantibodies

47
Causes That Contribute to Growth
Improper water treatment system design Loop Holding tanks UV/Ultrafilters Improper maintenance of water treatment system and delivery system (dialysis machine) Disinfection schedule Improper disinfectant
 Disinfection schedule. Improper disinfectant.")
48
Disinfection A key concept in ensuring compliance with the bacteriological control requirements is that disinfection schedules should be designed to prevent bacterial proliferation, rather than being designed to eliminate bacteria once they have proliferated to an unacceptable level.

Similar presentations














 Gloves Gown* Mask* Individuals in Contact Precautions do not require PPE when leaving their.>")













 AGENT SUSCEPTIBLE HOST RESERVOIR.>")


 Diagnostic testing at or near the site of patient care Uses portable handheld.>")

