Download presentation
Presentation is loading. Please wait.

1
HYPONATREMIA AND THE EMERGING ROLE OF TOLVAPTAN IN CARDIOLOGY
DR SHREETAL RAJAN NAIR

2
Hyponatremia Hyponatremia, defined as a serum sodium <135 mEq/L, is the most common electrolyte disorder encountered in hospitalized patients. Is a significant independent predictor of medical prognosis and costs.

3
Prevalence of hyponatremia
Prevalence of hyponatremia ([Na+] <135 mEq/L): 28% in hospitalized patients 21% in hospital clinics and 7% in outpatient community care clinics Clin Chim Acta. 2003;337(1-2):
: 28% in hospitalized patients. 21% in hospital clinics and. 7% in outpatient community care clinics. Clin Chim Acta. 2003;337(1-2):")
4
Prevalence of hyponatremia in hospitalized patients with heart failure or cirrhosis
Gheorghiade M, Rossi JS, Cotts W et al. Arch Intern Med. 2007;167(18): , Angeli P, Wong F, Watson H, Gines P. Hepatology. 2006;44(6):
: , Angeli P, Wong F, Watson H, Gines P. Hepatology. 2006;44(6):")
5
Classification of hyponatremia
Hypervolemic hyponatremia, Euvolemic hyponatremia, Hypovolemic hyponatremia

6
Hypervolemic hyponatremia
Dilutional form of hyponatremia, occurs when there is an increase in total body water but a relatively smaller increase in the total serum sodium. 3 primary causes of hypervolemic hyponatremia: HF, Cirrhosis of the liver, and Renal disease. Clinical signs evidence of volume expansion, such as the presence of clinically evident edema, ascites, and pulmonary edema

7
Euvolemic hyponatremia
It occurs when there is an increase in total body water without a corresponding increase in total serum sodium, though the increase in body water is not sufficient to promote clinically evident edema. Causes: Syndrome of inappropriate antidiuretic hormone (SIADH) Patients with euvolemic hyponatremia have no signs of volume depletion or volume expansion.
 Patients with euvolemic hyponatremia have no signs of volume depletion or volume expansion.")
8
Hypovolemic hyponatremia
Depletional form of hyponatremia, occurs when there is a decrease in both total body water and total serum sodium, with a disproportionately greater decrease in serum sodium. Hypovolemic hyponatremia is usually due to an excess of fluid loss. It is commonly caused by fluid loss through vomiting or diarrhea or is due to the use of diuretic therapy. Clinical signs of volume depletion include orthostatic decreases in blood pressure, increases in pulse rate, dry mucus membranes, and decreased skin turgor

9
Description of hyponatremia
Dilutional hyponatremia Depletional hyponatremia Hypervolemic Euvolemic Hypovolemic Increase in total body water with a relatively smaller increase in the total serum sodium; presence of clinically evident edema Mild to moderate increase in total body water with normal or near normal sodium levels; absence of clinically evident edema Decrease in total body water with a disproportionately greater decrease in total serum sodium; presence of clinically evident volume depletion

10
Causes of hyponatremia
Dilutional hyponatremia Depletional hyponatremia Hypervolemic Euvolemic Hypovolemic Heart failure (HF) Cirrhosis Renal disease (nephrotic syndrome and renal failure) Glucocorticoid deficiency Hypothyroidism SIADH, resulting from the following: Neurologic or CNS disorders such as mass lesions, inflammatory diseases,degenerative demyelinative diseases A range of cancers, including lung, pancreatic, prostate/ureteral, uterine, throat, and leukemia Pulmonary diseases, such as infections, respiratory failure, or chronic obstructive pulmonary disease (COPD) AIDS and AIDS-related complex Drug-induced Diuretic therapy Cerebral salt wasting Mineralocorticoid deficiency Salt-wasting nephropathy Bicarbonaturia, glucosuria, ketonuria Gastrointestinal losses, including vomiting and diarrhea Third-space losses such as bowel obstruction, pancreatitis, muscle trauma, and burns Sweat losses
 Cirrhosis. Renal disease. (nephrotic syndrome. and renal failure) Glucocorticoid deficiency. Hypothyroidism. SIADH, resulting from the following: Neurologic or CNS disorders such as mass lesions, inflammatory diseases,degenerative demyelinative diseases. A range of cancers, including lung, pancreatic, prostate/ureteral, uterine, throat, and leukemia. Pulmonary diseases, such as infections, respiratory failure, or chronic obstructive pulmonary disease (COPD) AIDS and AIDS-related complex. Drug-induced. Diuretic therapy. Cerebral salt wasting. Mineralocorticoid. deficiency. Salt-wasting nephropathy. Bicarbonaturia, glucosuria, ketonuria. Gastrointestinal losses, including. vomiting and diarrhea. Third-space losses such. as bowel obstruction, pancreatitis, muscle trauma, and burns. Sweat losses.")
11
Signs, symptoms, and consequences of hyponatremia
Serum [Na+] mEq/L Serum [Na+] mEq/L Serum [Na+] <120 mEq/L • Malaise • Unsteadiness • Headache • Nausea • Vomiting • Fatigue • Confusion • Muscle cramps •Asymptomatic • Headache • Nausea • Vomiting • Fatigue • Confusion • Muscle cramps • Depressed reflexes • Headache • Restlessness • Lethargy • Seizures • Brain-stem herniation • Respiratory arrest • Death .

12
Pathophysiology of hyponatremia

13
Physiology of water homeostasis

14
Vasopressin Is a nine-amino-acid peptide synthesized in the neurosecretory cells of the supraoptic and paraventricular nuclei of the hypothalamus and is stored in the posterior pituitary gland. Upon its release, vasopressin binds to and activates V2-receptors in the renal collecting duct, leading to the insertion of water channels into the wall of the collecting duct by a cAMP-dependent mechanism. This series of events stimulates water reabsorption. Thus, increased vasopressin promotes an increase in electrolyte-free water reabsorption and more concentrated urine as water passively diffuses out of the renal tubule. Circulating vasopressin can also cause vasoconstriction by activating V1a-receptors on smooth muscle cells in blood vessels. V1b-receptors are found on corticotropes, and they contribute to increased ACTH secretion.

15
Vasopressin The primary role of vasopressin is
to control total body water, electrolyte balance, and blood pressure by regulating vascular tone and water excretion by the kidney. Increased vasopressin levels due to nonosmotic hemodynamic stimuli is the mechanism responsible for water retention and hyponatremia in edema-forming disorders such as HF and cirrhosis.

16
Heart failure: HF patients may have increased vasopressin secretion
in response to decreases in arterial blood pressure and circulating blood volume. Decrease in blood volume or blood pressure of approximately 8% to 10% - stimulates vasopressin secretion. The underloading of arterial baroreceptors is responsible for the stimulation of vasopressin secretion. Vasopressin increases the passive reabsorption of electrolyte-free water in the kidney in an attempt to restore perfusion pressure- may result in hypervolemic hyponatremia.

17
MOA OF V1 RECEPTOR ACTIVATION

18
MOA OF V2 RECEPTOR ACTIVATION

19
Receptor subtypes that mediate the actions of vasopressin

20
Factors stimulating the release of vasopressin
The 2 key mechanisms regulating fluid/electrolyte balance are Renal water reabsorption, due to vasopressin, and Drinking behavior driven by thirst perception. Vasopressin increases passive water reabsorption in the kidney and results in more concentrated urine, which is reflected by increased urine osmolality. Hyponatremia may result from sodium loss, excessive fluid intake, or, more frequently, water retention.

21
Factors stimulating the release of vasopressin
Osmotic stimuli Nonosmotic stimuli of vasopressin release: These stimuli include decreased effective arterial blood volume or blood pressure, pain, nausea, stress, and a variety of drugs. Decreases of approximately 8% to 10% in arterial blood pressure and circulating blood volume may activate baroreceptors in the carotid sinus, aortic arch, cardiac atria, and pulmonary venous system, which stimulate the release of vasopressin. Vasopressin release due to nonosmotic stimuli is responsible for the predominance of euvolemic and hypervolemic hyponatremia (e.g., SIADH, HF, or Cirrhosis).
.")
22
Why recognising and treating hyponatremia is important ?

24
Hyponatremia - HF The Organized Program to Initiate Life Saving Treatment in Patients Hospitalized for Heart Failure (OPTIMIZE-HF) registry recorded that 25.3% of 47,647 heart failure patients had hyponatremia on admission. In this registry, patients with hyponatremia had increased in-hospital and postdischarge mortality and longer median hospital stay compared with those with higher sodium levels. . OPTIMIZE-HF registry, Eur Heart J, 2007;28(8):980–88.
 registry recorded that 25.3% of 47,647 heart failure patients had hyponatremia on admission. In this registry, patients with hyponatremia had increased in-hospital and postdischarge mortality and longer median hospital stay compared with those with higher sodium levels. . OPTIMIZE-HF registry, Eur Heart J, 2007;28(8):980–88.")
25
Hyponatremia Is Associated with Higher Mortality
Lancet. 1982;2(8289):101-2. Clin Sci. 1939;4:73-7. Br Med J. 1983;286(6366):671-3. Br Med J. 1979;1(6173):
: Clin Sci. 1939;4:73-7. Br Med J. 1983;286(6366): Br Med J. 1979;1(6173):")
26
Hyponatremia - HF Currently, there are no guidelines for the appropriate way to deal with low serum sodium levels in heart failure patients; Treatment generally consists of fluid restriction, which has not been clinically examined in this setting. Vasopressin receptor antagonists that selectively increase solute-free water excretion by the kidneys are showing evidence of being effective for the treatment of hyponatremia in heart failure.

27
Rationale of present therapies
Increase the amount of sodium in the body Decrease intake of water Prevent water reabsorption into the body and prevent dilution

28
Current therapies of hyponatremia
Isotonic and hypertonic saline for short-term use, and fluid restriction, demeclocycline, salt tablets, and rarely mineralocorticoids and urea for long-term use. All of these therapies work in specific circumstances, but none are ideal and all have limitations for a variety of different reasons, including variable efficacy, slow responses, intolerable side effects such as thirst, and dangerous toxicities such as ODS.

29
Current therapies of hyponatremia
Fluid restriction Is that fluid restriction usually cannot be sustained Because it produces intolerable dehydration and thirst. Secondly, fluid restriction works very slowly—generally 1 to 2 mEq/L per day even under a severe fluid restriction of <500 mL/d. Consequently, this method can take many days to correct a low serum [Na+]. Fluid restriction, long the mainstay of treating chronic hyponatremia, is arguably the least expensive and potentially the safest treatment. But its major drawback, reported as early as in the initial description of SIADH in 1957, is that fluid restriction usually cannot be sustained because it produces intolerable dehydration and thirst. Secondly, fluid restriction works very slowly—generally 1 to 2 mEq/L per day even under a severe fluid restriction of <500 mL/d. Consequently, this method can take many days to correct a low serum [Na+]. Am J Med. 1957;23(4):
:")
30
Current therapies of hyponatremia
All treatments other than demeclocycline and the vaptans fail to attack the mechanistic cause of dilutional hyponatremia, which is inappropriately elevated plasma AVP levels.

31
Treatments for Hyponatremia
Therapy Limitations Isotonic saline Ineffective in dilutional hyponatremias; can’t be used in edema-forming disorders; no controlled safety database Hypertonic saline No consensus re appropriate infusion rates; overcorrection can cause osmotic demyelination; can’t be used in edema-forming disorders; no controlled safety database Fluid restriction Slow to correct over many days; poorly tolerated due to thirst; unsuccessful with high AVP levels and urine osmolalities Demeclocycline Not FDA approved for hyponatremia; slow to correct; nephrotoxic in cirrhosis and CHF

32
Treatments for Hyponatremia
Therapy Limitations Mineralocorticoid Only one report in elderly patients with SIADH; no safety database; can’t be used in edema-forming disorders Urea No USP formulation; not FDA approved for hyponatremia; poor palatability

33
Aquaretic therapies The newest addition in hyponatremia treatment

34
rationale for aquaretic therapies
The appropriate method of treating hyponatremia in HF is by removing excess total body water That is the objective of fluid restriction that decreases body water via insensible losses of water, but very inefficiently and very slowly. A better therapy would be blocking the process of urinary concentration, which originates from AVP binding to the V2 receptor in the kidney and would prevent all the downstream intracellular consequences of V2 receptor activation including the insertion of the aquaporin water channels into the apical membrane of the collecting duct cells.

35
The VAPTANS

37
Tolvaptan

38
Was approved by US FDA in february 19,2009
Tolvaptan (INN), also known as OPC-41061, is a selective, Competitive vasopressin receptor 2 antagonist used to treat hyponatremia (low blood sodium levels) associated with congestive heart failure, cirrhosis, and the syndrome of inappropriate antidiuretic hormone (SIADH).
, also known as OPC-41061, is a selective, Competitive vasopressin receptor 2 antagonist used to treat hyponatremia (low blood sodium levels) associated with congestive heart failure, cirrhosis, and the syndrome of inappropriate antidiuretic hormone (SIADH).")
39
Tolvaptan Mechanism of action of the Tolvaptan: stimulate increased water excretion from the kidney. Importantly, blocking the V2 receptor has no effect on sodium or potassium excretion; it simply causes increased excretion of water without increased solute. Therefore, vaptans are electrolyte-sparing, and it is more appropriate to call their effect “aquaresis” or increased urinary water excretion rather than diuresis, which classically has been defined as increased urinary water and solute (particularly sodium and potassium) excretion.
 excretion.")
40
Mechanism of action Tolvaptan is a selective vasopressin V2-receptor antagonist with an affinity for the human V2-receptor 1.8 times that of native vasopressin. Tolvaptan affinity for the V2-receptors is approximately 29 times that for the V1a-receptor. Urinary excretion of sodium and potassium, and plasma potassium concentrations are not significantly changed. When taken orally, 15- to 60-mg doses of tolvaptan antagonize the effect of vasopressin and cause an increase in urine water excretion that results in an increase in free water clearance (aquaresis), a decrease in urine osmolality, and a resulting increase in serum sodium. Am J Med. 2007;120(suppl 11A):S1-S21
, a decrease in urine osmolality, and a resulting increase in serum sodium. Am J Med. 2007;120(suppl 11A):S1-S21.")
41
Targeted MOA: Vasopressin V2-receptor antagonism
Tolvaptan N Engl J Med. 2005;352(18):
:")
42
Targeted MOA: Vasopressin V2-receptor antagonism
Binding of a V2-receptor antagonist, such as tolvaptan, blocks the activation of the receptor by endogenous vasopressin. The resulting increase in urine output produced by a V2-receptor antagonist is quantitatively similar to diuretics such as loop diuretics, but qualitatively different in that electrolyte-free water is excreted without a significant increase in urine solute excretion, including sodium and potassium. For this reason, the renal effects produced by V2-receptor antagonists are termed aquaresis, to distinguish them from the renal effects produced by some diuretic agents, which include not only increased water excretion but also natriuresis and kaliuresis

43
Dosing and titration The usual starting dose for (tolvaptan) is 15 mg administered once daily without regard to meals. The dose of Tolvaptan may be increased to 30 mg once daily, after at least 24 hours, to a maximum of 60 mg once daily, as needed to achieve the desired level of serum sodium. During initiation and titration, frequently monitor for changes in serum electrolytes and volume to prevent overcorrection of serum sodium

44
Dosage and administration
Route of administration: Oral Initial dose (hospitalization: mg required) Dose range (titrated to : –60 mg response) Frequency of administration Once daily
 Dose range (titrated to : 15–60 mg. response) Frequency of administration Once daily.")
45
Pharmacokinetic profile
Peak plasma concentration: (mean) [ng/mL] Time to achieve peak plasma: concentration (median) [h] Area under the plasma concentration-time curve over the 24-hour dosage interval (mean) [ng • h/mL] Elimination half-life (mean) [h]
 [ng/mL] Time to achieve peak plasma: 2.0. concentration (median) [h] Area under the plasma concentration-time curve over. the 24-hour dosage interval. (mean) [ng • h/mL] Elimination half-life (mean) [h] 9.4.")
46
Tolvaptan is contraindicated in the following conditions:
Urgent need to raise serum sodium acutely Inability of the patient to sense or appropriately respond to thirst Hypovolemic hyponatremia Concomitant use of strong CYP 3A inhibitors Anuric patients

47
Adverse effects Problems with speech or muscle control, trouble swallowing, trouble moving your arms and legs, mood changes, and seizure (convulsions) – may be osmotic demyelination syndrome due to rapid correction of sodium weakness or fainting; melaena; Hemoptysis,hemetemesis; Less serious side effects may include: dry mouth; increased thirst abnormal frequent urination (pollakiuria) constipation; or loss of appetite, fruity breath odor, drowsiness, dry skin, nausea, vomiting.
 – may be osmotic demyelination syndrome due to rapid correction of sodium. weakness or fainting; melaena; Hemoptysis,hemetemesis; Less serious side effects may include: dry mouth; increased thirst. abnormal frequent urination (pollakiuria) constipation; or. loss of appetite, fruity breath odor, drowsiness, dry skin, nausea, vomiting.")
48
TOLVAPTAN Trials

49
Study of Ascending Levels of Tolvaptan in Hyponatremia
SALT 1 & 2 Study of Ascending Levels of Tolvaptan in Hyponatremia

50
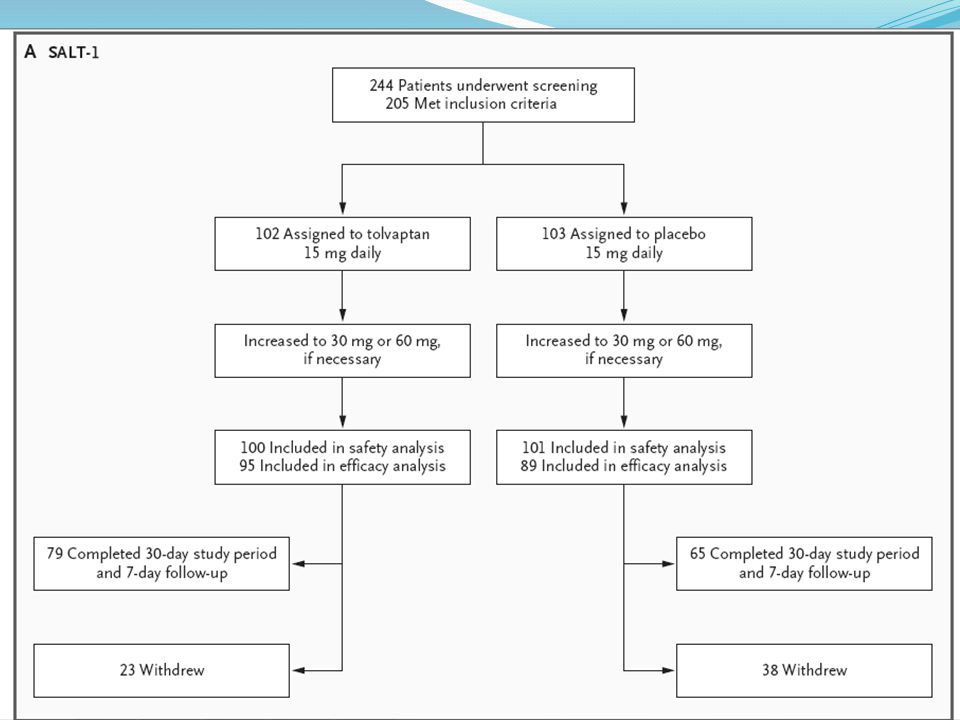
SALT-1 and SALT-2 Multicenter, randomized, double-blind, placebo-controlled trials, the efficacy of tolvaptan was evaluated in patients with euvolemic and hypervolemic hyponatremia. N= 448 patients Hypervolemic or euvolemic hyponatremia resulting from (HF, cirrhosis, or SIADH) Oral placebo (n=223) or Oral Tolvaptan (n=225) in a titrated regimen of 15 to 60 mg once daily. N Engl J Med 2006;355:
 Oral placebo (n=223) or. Oral Tolvaptan (n=225) in a titrated regimen of 15 to 60 mg once daily. N Engl J Med 2006;355:")
51
Inclusion Sodium (mEq/L) Mean Sodium (mEq/L): 129.1 mEq/L 128.9 mEq/L
 Mean Sodium (mEq/L): mEq/L mEq/L")
52
Inclusion/exclusion criteria
Inclusion criteria: Exclusion criteria: 18 years of age or older Had hypervolemic or euvolemic hyponatremia (serum sodium <135 mEq/L) associated with HF, cirrhosis, or SIADH Psychogenic polydipsia Head trauma Postoperative conditions Uncontrolled hypothyroidism or adrenal insufficiency Hyponatremic conditions associated with the use of medications that could have been safely withdrawn Clinically evident hypovolemic hyponatremia
 associated with HF, cirrhosis, or SIADH. Psychogenic polydipsia. Head trauma. Postoperative conditions. Uncontrolled hypothyroidism or adrenal insufficiency. Hyponatremic conditions associated with the use of medications that could have been safely withdrawn. Clinically evident hypovolemic hyponatremia.")
53
Study Assessments Patients were evaluated at baseline, 8 hours after
the first administration of the study drug (tolvaptan or placebo), and on days 2, 3, 4, 11, 18, 25, 30, and 37. Study drugs were withheld after day 30,and the effect of discontinuation of the study drug was assessed on day 37
, and on days 2, 3, 4, 11, 18, 25, 30, and 37. Study drugs were withheld after day 30,and the effect of discontinuation of the study drug was assessed on day 37.")
54
Primary end points The change in the average daily area under the curve (AUC) for the serum sodium concentration from baseline to day 4 from baseline to day 30

55
Secondary end points the change in the AUC for the serum sodium concentration in patients with marked hyponatremia, the absolute serum sodium concentration at each visit, the time to normalization of the serum sodium concentration, the percentages of patients with serum sodium concentrations that had normalized at day 4 and day 30, and the categorical serum sodium concentration on day 4 and day 30 (normal value >135 mmol per liter; mild hyponatremia, 130 to 135 mmol per liter as conservatively extended for the analysis of categorical change; or marked hyponatremia <130 mmol per liter) for patients with mild or marked hyponatremia at baseline. Other secondary end points were fluid intake and output on day 1, change in body weight in patients with hypervolemic hyponatremia on day 1, fluid restriction or use of intravenous saline as rescue therapy,
 for patients with mild or marked hyponatremia at baseline. Other secondary end points were fluid intake and output on day 1, change in body weight in patients with hypervolemic hyponatremia on day 1, fluid restriction or use of intravenous saline as rescue therapy,")
58
RESULTS P = <0.001 FO ALL COMPARISONS

59
RESULTS P = <0.001 FO ALL COMPARISONS

60
Subjects with serum sodium <135 mEq/L (ITT population)
Results Tolvaptan 15–60 mg/day Placebo Estimated effect Subjects with serum sodium <135 mEq/L (ITT population) Change in average daily serum [Na+] AUC: baseline to day 4 (mEq/L) mean (SD) (n) 4.0 (2.8) (213) 0.4 (2.4) (203) 3.7 ( ) P<0.0001 Change in average daily serum [Na+] AUC:baseline to day 30 (mEq/L) mean (SD) 6.2 (4.0) 1.8 (3.7) 4.6 ( )
 Change in average daily serum [Na+] AUC: baseline to day 4 (mEq/L) mean (SD) (n) 4.0 (2.8) (213) 0.4 (2.4) (203) 3.7 ( ) P< Change in average daily serum [Na+] AUC:baseline to day 30 (mEq/L) mean (SD) 6.2 (4.0) 1.8 (3.7) 4.6 ( )")
61
Subgroup with serum sodium <130 mEq/L
Results Tolvaptan 15–60 mg/day Placebo Estimated effect Subgroup with serum sodium <130 mEq/L Change in average daily serum [Na+] AUC: baseline to day 4 (mEq/L) mean (SD) (n) 4.8 (3.0) (110) 0.7 (2.5) (105) 4.2 ( ) P<0.0001 Change in average daily serum [Na+] AUC: baseline to day 30 (mEq/L) mean (SD) 7.9 (4.1) 2.6 (4.2) 5.5 ( )
 mean (SD) (n) 4.8 (3.0) (110) 0.7 (2.5) (105) 4.2 ( ) P< Change in average daily serum [Na+] AUC: baseline to day 30 (mEq/L) mean (SD) 7.9 (4.1) 2.6 (4.2) 5.5 ( )")
62
Subgroup with serum sodium <125 mEq/L
Results Tolvaptan 15–60 mg/day Placebo Estimated effect Subgroup with serum sodium <125 mEq/L Change in average daily serum [Na+] AUC: baseline to day 4 (mEq/L) mean (SD) (n) 5.7 (3.8) (26) 1.0 (1.8) (30) 5.3 ( ) P<0.0001 Change in average daily serum [Na+] AUC:baseline to day 30 (mEq/L) mean (SD) 10.0 (4.8) 4.1 (4.5) 5.7 ( )
 mean (SD) (n) 5.7 (3.8) (26) 1.0 (1.8) (30) 5.3 ( ) P< Change in average daily serum [Na+] AUC:baseline to day 30 (mEq/L) mean (SD) 10.0 (4.8) 4.1 (4.5) 5.7 ( )")
65
RESULTS

68
Summary – SALT 1 and SALT -2
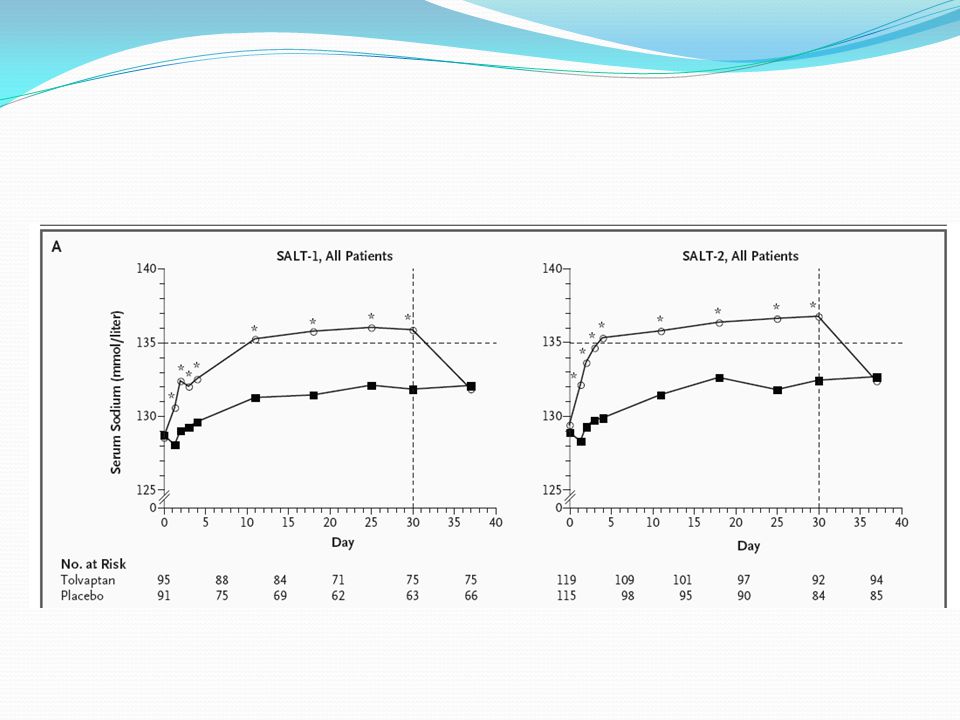
A total of 424 patients with euvolemic and hypervolemic hyponatremia (serum sodium <135 mEq/L) were treated for 30 days with tolvaptan or oral placebo, then followed for an additional 7 days after withdrawal. The primary end point for these studies was the average daily AUC for change in serum sodium from baseline to day 4 (tolvaptan, 4.0 mEq/L vs placebo, 0.4 mEq/L) and baseline to day 30 (tolvaptan, 6.2 mEq/L vs placebo, 1.8 mEq/L) in patients with a serum sodium <135 mEq/L.
 were treated for 30 days with tolvaptan or oral placebo, then followed for an additional 7 days after withdrawal. The primary end point for these studies was the average daily AUC for change in serum sodium from baseline to day 4 (tolvaptan, 4.0 mEq/L vs placebo, 0.4 mEq/L) and baseline to day 30 (tolvaptan, 6.2 mEq/L vs placebo, 1.8 mEq/L) in patients with a serum sodium <135 mEq/L.")
69
Summary – SALT 1 & 2 Patients received either tolvaptan or placebo, at a starting dose of 15 mg. The dosage of tolvaptan or placebo was increased to 30 mg or 60 mg, if necessary. During the 7-day discontinuation/follow-up period, serum sodium concentrations in patients treated with tolvaptan declined to placebo-like levels. In patients with euvolemic or hypervolemic hyponatremia, tolvaptan, an oral vasopressin V2-receptor antagonist, was effective in increasing serum sodium concentrations at day 4 and day 30.

70
Extension study of the SALT trials
SALTWATER Extension study of the SALT trials

71
SALTWATER was a multicenter, open-label extension of the Study of Ascending Levels of Tolvaptan in Hyponatremia (SALT-1 and SALT-2). In total, 111 patients with hyponatremia received oral tolvaptan for a mean follow-up of 701 days, providing 77,369 patient-days of exposure. All patients had hyponatremia at randomization in SALT-1 and SALT-2 J Am Soc Nephrol 2010, 21(4):
:")
74
Serum sodium levels during SALT -1 ,SALT -2 and SALTWATER

75
SALTWATER Trial: Analysis of Mean Serum Sodium (± SE, mEq/L) by Visit
 by Visit")
77
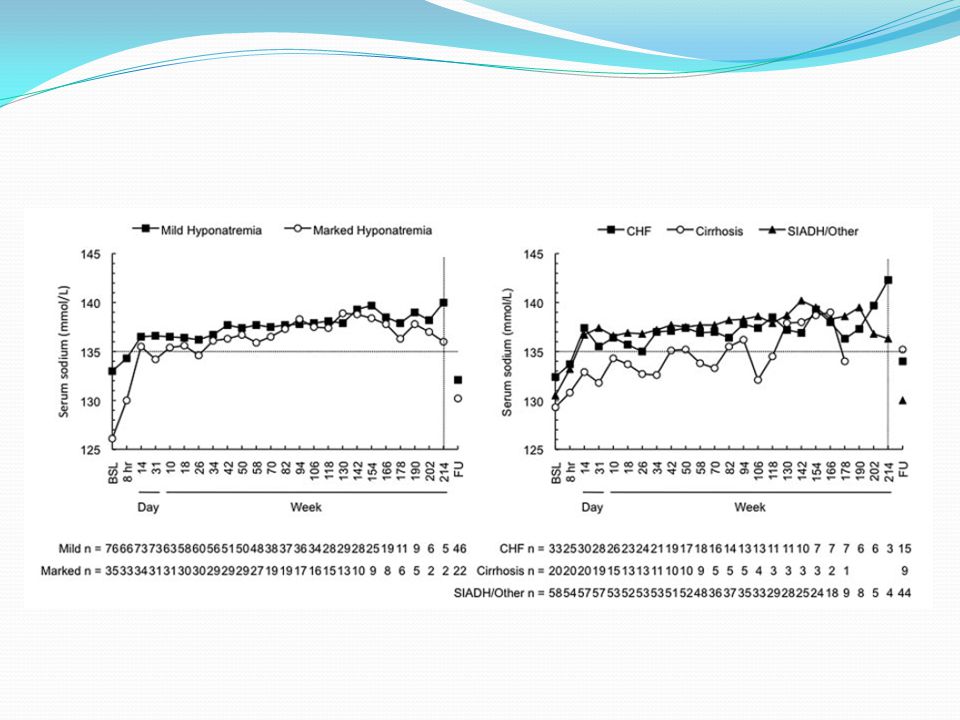
Percentage of patients who normalized their serum sodium according to severity of hyponatremia

78
Percentage of patients who normalized their serum sodium according to etiology

80
Results & conclusion- SALTWATER
Mean serum sodium increased from mmol/L at baseline to 135 mmol/L throughout the observation period (P versus baseline at most points). Conclusion: Prolonged administration of tolvaptan maintains an increased serum sodium with an acceptable margin of safety.
. Conclusion: Prolonged administration of tolvaptan maintains an increased serum sodium with an acceptable margin of safety.")
81
EVEREST Efficacy of Vasopressin Antagonism in Heart Failure Outcome Study With Tolvaptan

83
Inclusion criteria Patients 18 years of age or older with
reduced left ventricular ejection fraction (40%), signs of volume expansion, New York Heart Association class III/IV symptoms, and Hospitalization for exacerbation of chronic HF no more than 48 hours earlier were eligible for the study.
, signs of volume expansion, New York Heart Association class III/IV symptoms, and. Hospitalization for exacerbation of chronic HF no more than 48 hours earlier were eligible for the study.")
84
Exclusion criteria Cardiac surgery within 60 days of enrollment,
cardiac mechanical support, biventricular pacemaker placement within the last 60 days, comorbid conditions with an expected survival of less than 6 months, acute myocardial infarction at the time of hospitalization, hemodynamically significant uncorrected primary cardiac valvular disease, refractory end-stage HF, hemofiltration or dialysis, supine systolic arterial blood pressure less than 90 mm Hg, serum creatinine level greater than 3.5 mg/dL (309 μmol/L), serum potassium level greater than 5.5 mEq/L, and hemoglobin level less than 9 g/dL.
, serum potassium level greater than 5.5 mEq/L, and. hemoglobin level less than 9 g/dL.")
85
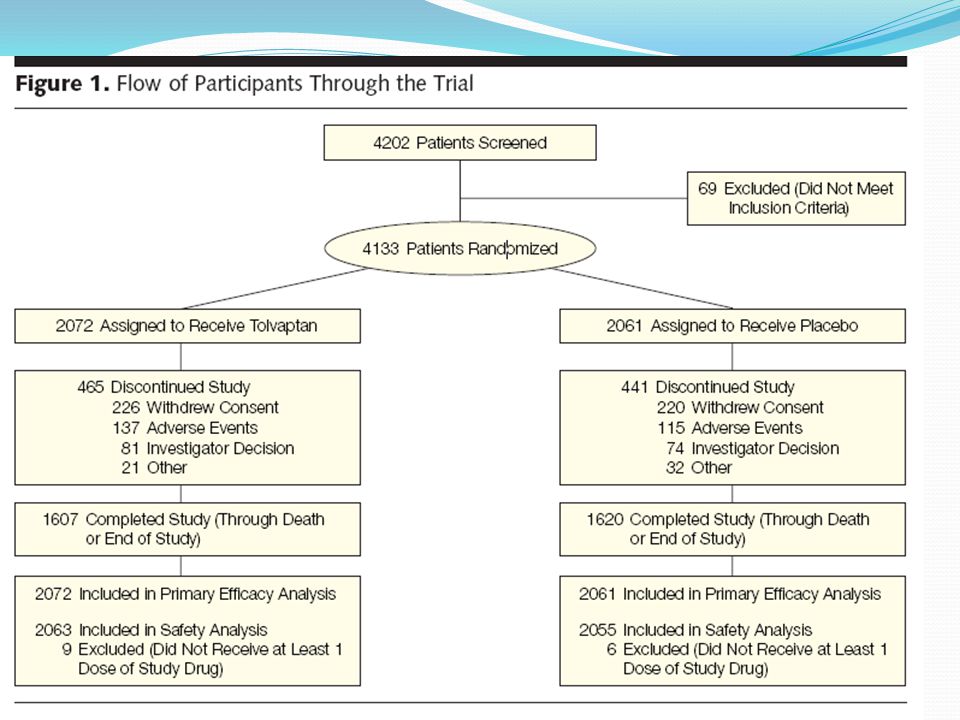
STUDY POPULATION A total of 2072 patients in tolvaptan group and patients in placebo group hospitalized with heart failure

86
Intervention Patients were randomized to receive either tolvaptan (30 mg/d) or matching placebo, within 48 hours of admission
 or matching placebo, within 48 hours of admission.")
87
Primary end points The outcome study had 2 primary end points:
all-cause mortality and the composite of cardiovascular death or hospitalization for HF

88
Secondary end points the composite of cardiovascular mortality or cardiovascular hospitalization; incidence of cardiovascular mortality; and incidence of clinical worsening of HF (death, hospitalization for HF, or unscheduled visit for HF)
")
89
Additional secondary end points
included changes from baseline in body weight at day 1, serum sodium level at day 7 or discharge in patients with a baseline serum sodium level of less than 134 mEq/L, edema score at day 7 or discharge for those with edema at baseline, patient-assessed dyspnea at day 1 for those with dyspnea at baseline,

95
Patient-assessed dyspnoea status at inpatient Day 1 in the combined EVEREST trial population

97
Conclusion : EVEREST Tolvaptan modestly improves dyspnoea compared with standard therapy alone, regardless if given early or relatively late after hospitalization, and also across major pre-specified subgroups

98
ECLIPSE: EffeCt of toLvaptan on hemodynamIc Parameters
in Subjects with hEart failure

100
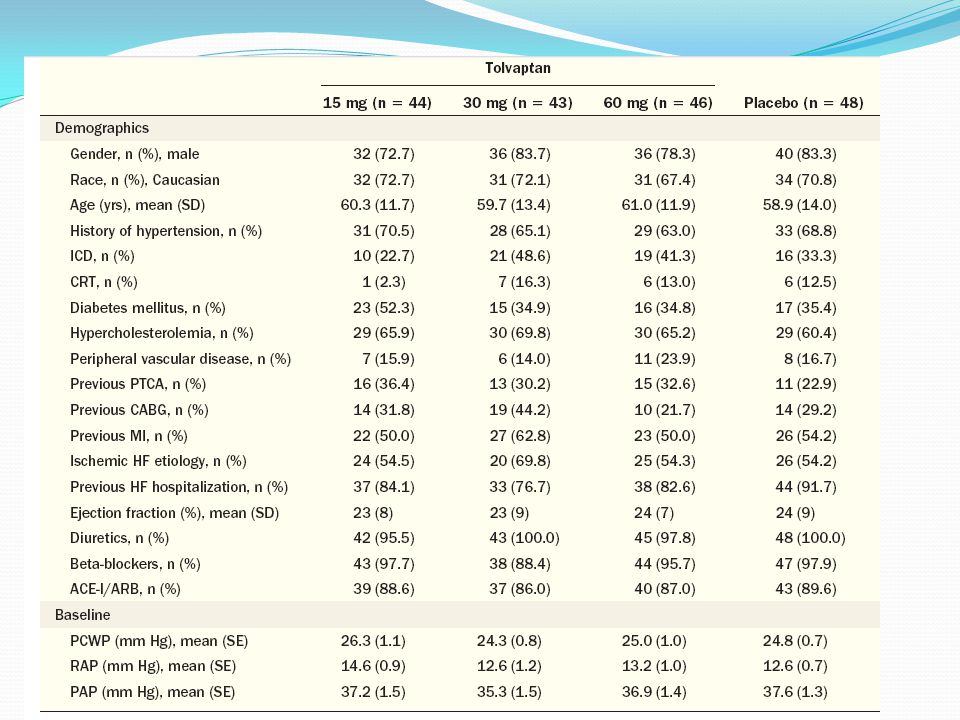
Study groups- 4 groups Tolvaptan 15 mg Tolvaptan 30 mg Tolvaptan 60 mg
placebo

103
Mean Change from Baseline in PCWP and RAP

104
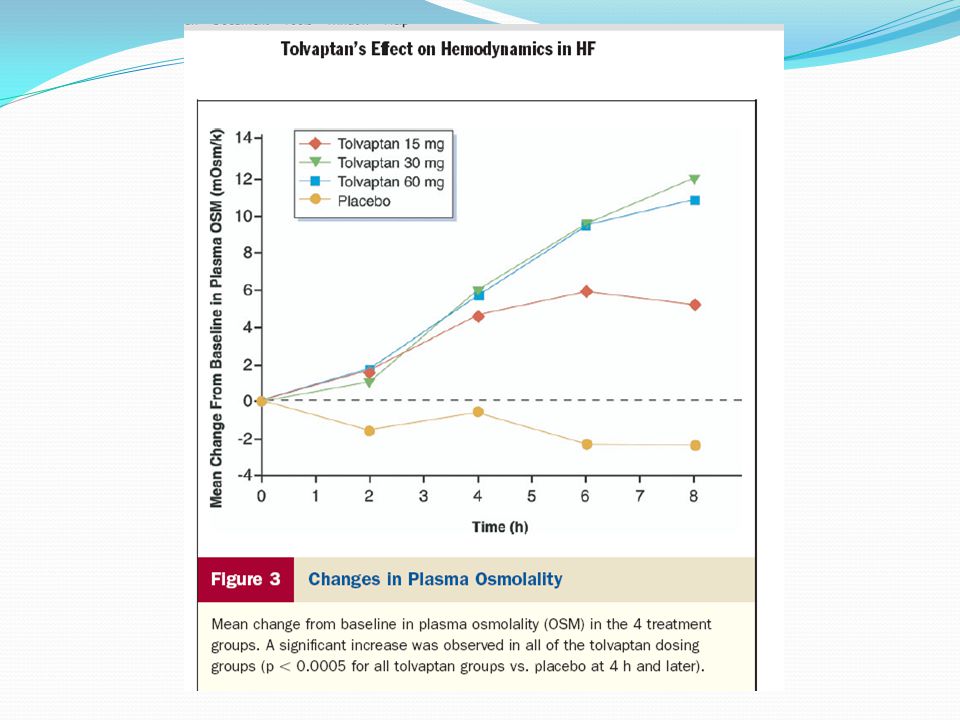
Mean Change From Baseline in Urine Volume and Osmolality

107
QUEST

109
End points The primary endpoint of the current study was body weight change from the baseline at the end of treatment. The secondary endpoints were changes in congestive symptoms, including lower limb edema, pulmonary congestion, jugular venous distention hepatomegaly, pulmonary rales and third heart sound induced with fluid retention

110
Patient disposition

116
Improvements in congestive symptoms

117
Time-course of change in daily urine volume

118
Plasma AVP (a), plasma BNP (b)
, plasma BNP (b)")
119
serum osmolality (c) and plasma renin activity (d)
 and plasma renin activity (d)")
120
Time-course of serum Na+ levels in patients with serum Na+ ≥135 mEq/L (a) or <135 mEq/L (b) at baseline
 or <135 mEq/L (b) at baseline")
121
Quest Study Results: Compared with placebo, tolvaptan administered for 7 days significantly reduced body weight and improved symptoms associated with volume overload. The safety profile of tolvaptan was considered acceptable for clinical use with minimal adverse effects. Conclusion: Tolvaptan reduced volume overload and improved congestive symptoms associated with HF by a potent water diuresis (aquaresis).
.")
122
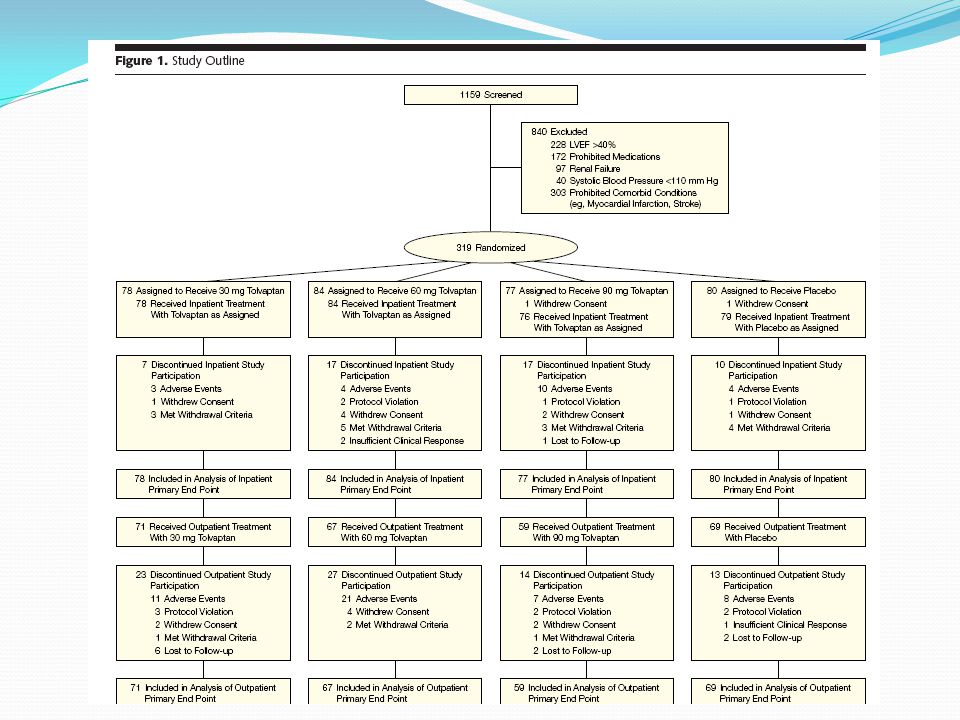
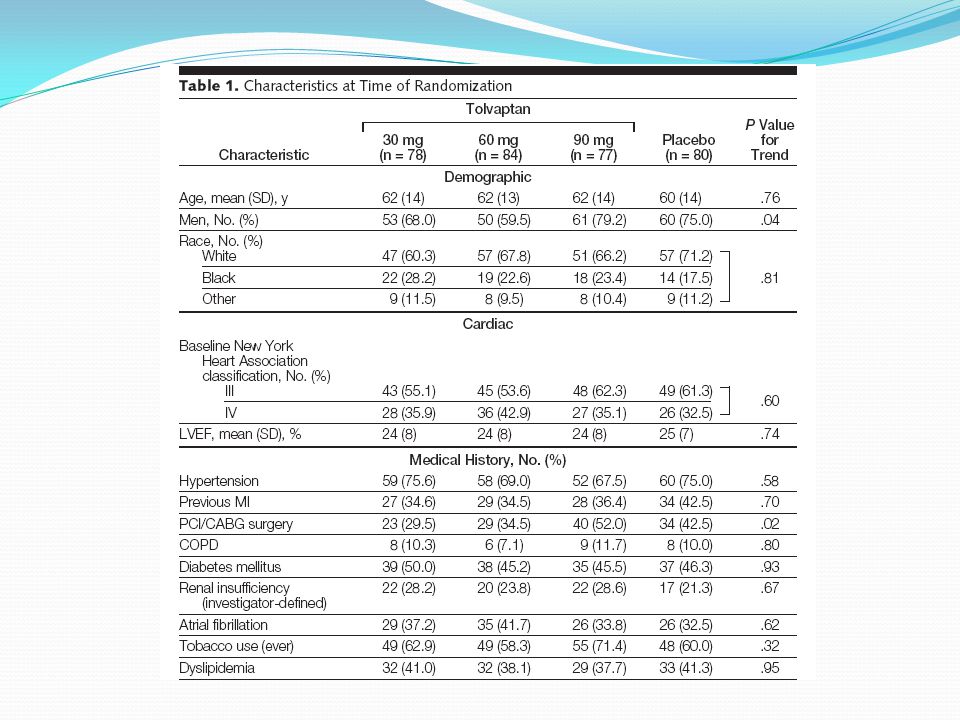
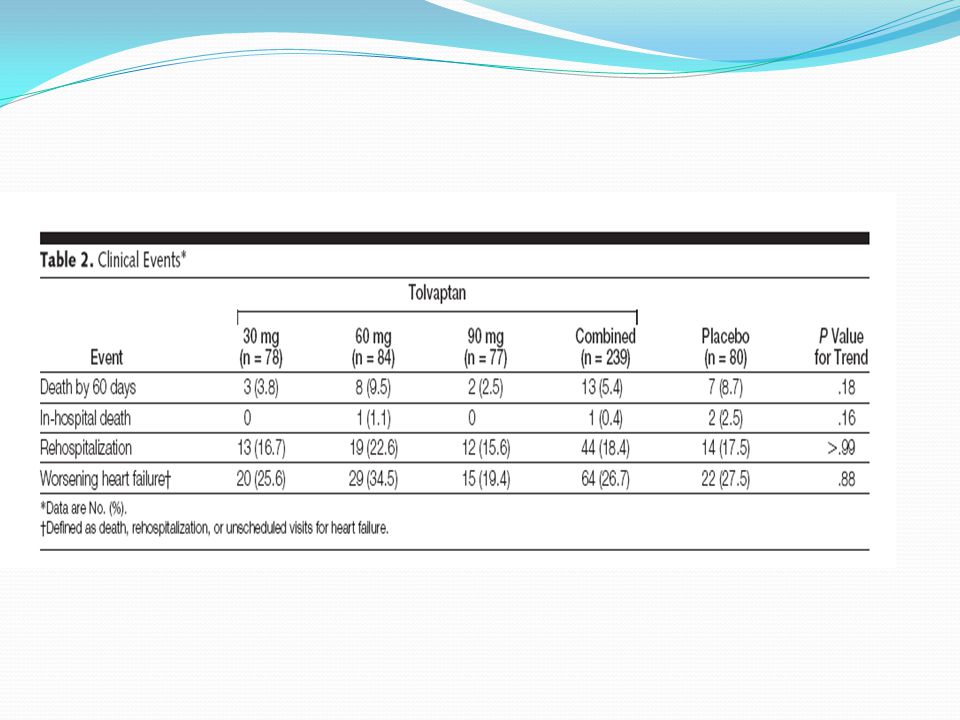
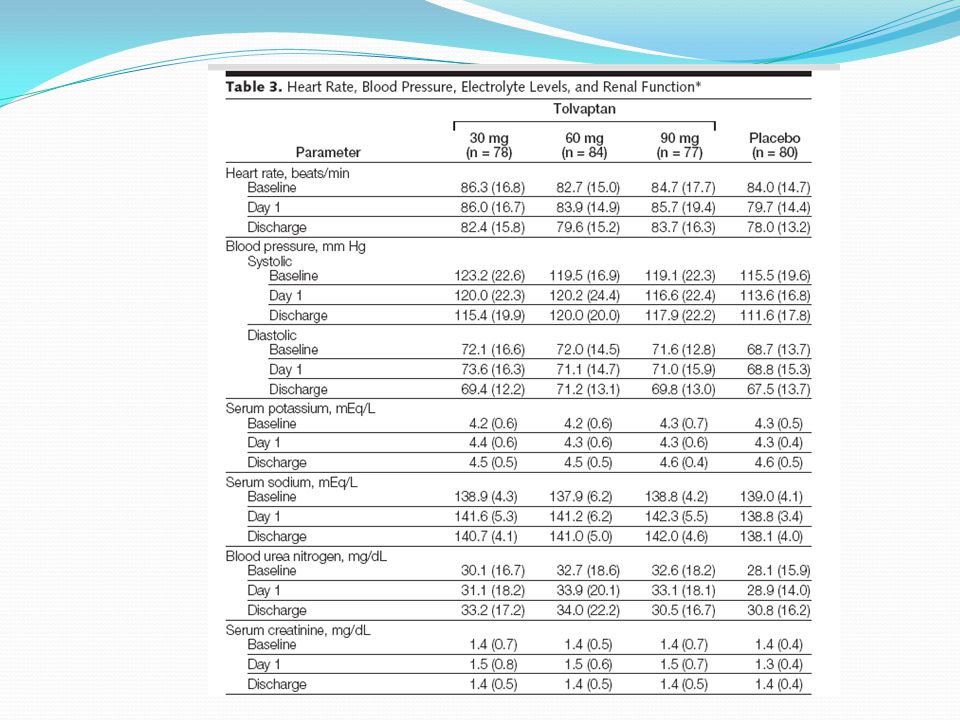
ACTIV in CHF trial: Effects of Tolvaptan, Vasopressin Antagonist, in Patients Hospitalized With Worsening Heart Failure delete

123
JAMA, April 28, 2004—Vol 291, No. 16

124
End points The study had 2 primary end points designed
to assess the acute (in-hospital) and the intermediate-term (outpatient ,after hospital discharge) effects of the study drug. The in-hospital end point was change in body weight at 24 hours after the administration of the first dose of study drug The outpatient end point was worsening heart failure at 60 days after randomization
 and the intermediate-term (outpatient ,after hospital discharge) effects of the study drug. The in-hospital end point was change in body weight at 24 hours after the administration of the first dose of study drug. The outpatient end point was worsening heart failure at 60 days after randomization.")
125
Secondary end points Secondary end points included
changes in dyspnea, JVD, rales, edema,body weight (at discharge and in the outpatient setting) urine output (in patient) serum electrolyte levels length of hospital stay after randomization use of diuretics patient and physician-assessed symptom scales
 urine output (in patient) serum electrolyte levels. length of hospital stay after randomization. use of diuretics. patient and physician-assessed symptom scales.")
129
Median Changes in Body Weight Over Time
*Indicates P=.002; †, P=.009; ‡, P=.006; and §, P=.008 for comparisons with placebo group. Error bars indicate interquartile range.

131
Signs and Symptoms of Heart Failure at Day 1 and at Hospital Discharge
P>0.05 for all comparisons of tolvaptan vs placebo except for dyspnea at discharge, for which P=.04. JVD indicates jugular venous distention.

136
Adverse reaction trial data
In a subgroup of patients with hyponatremia (N = 475, serum sodium < 135 mEq/L) mortality (42% tolvaptan, 38% placebo), nausea (21% tolvaptan, 16% placebo), thirst (12% tolvaptan, 2% placebo), dry mouth (7% tolvaptan, 2% placebo) and polyuria or pollakiuria (4% tolvaptan, 1% placebo).
 mortality (42% tolvaptan, 38% placebo), nausea (21% tolvaptan, 16% placebo), thirst (12% tolvaptan, 2% placebo), dry mouth (7% tolvaptan, 2% placebo) and. polyuria or pollakiuria (4% tolvaptan, 1% placebo).")
139
Trials involving tolvaptan

140
Thank you

Similar presentations


































 Na+ Positively charged counterions Rinse in buffer, add ionic compounds. Positive charges (triangles) stick.>")

 Dr Steve Hyer.>")










![Hyponatremia. Definition Serum [Na] < 135 meq/L Serum [Na] < 135 meq/L - incidence is 1%-4% Serum [Na] < 130meq/L - incidence is 15%-30% (represents a.](/39/11037667/big_thumb.jpg "Hyponatremia. Definition Serum [Na] < 135 meq/L Serum [Na] < 135 meq/L - incidence is 1%-4% Serum [Na] < 130meq/L - incidence is 15%-30% (represents a.>")