Download presentation
Presentation is loading. Please wait.

1
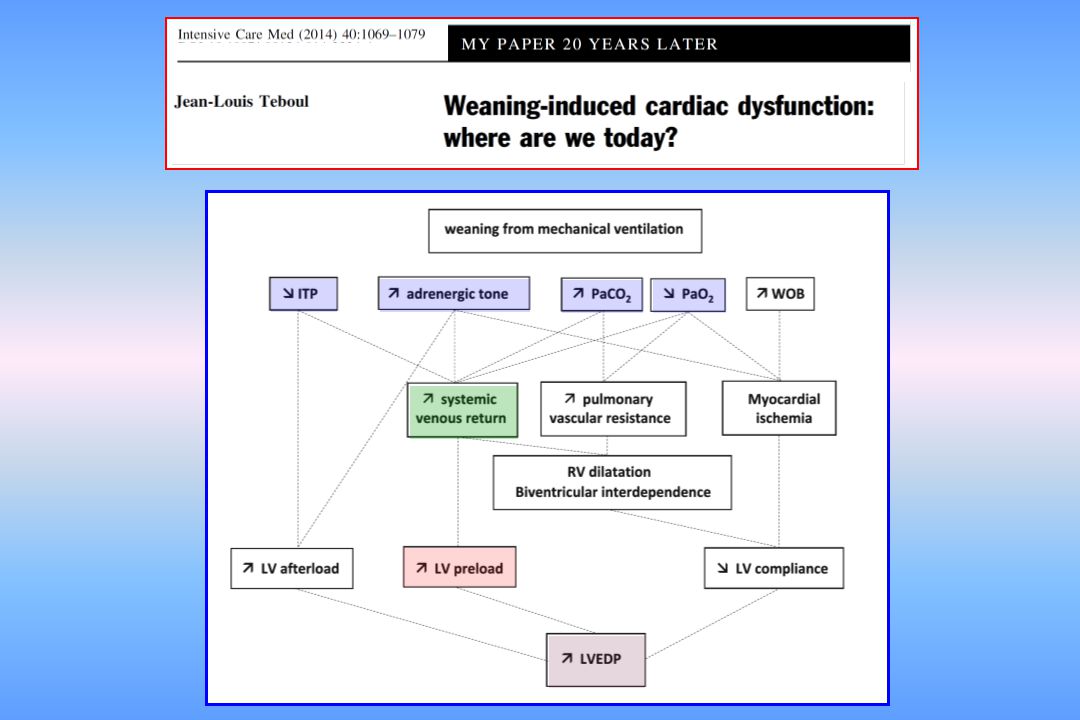
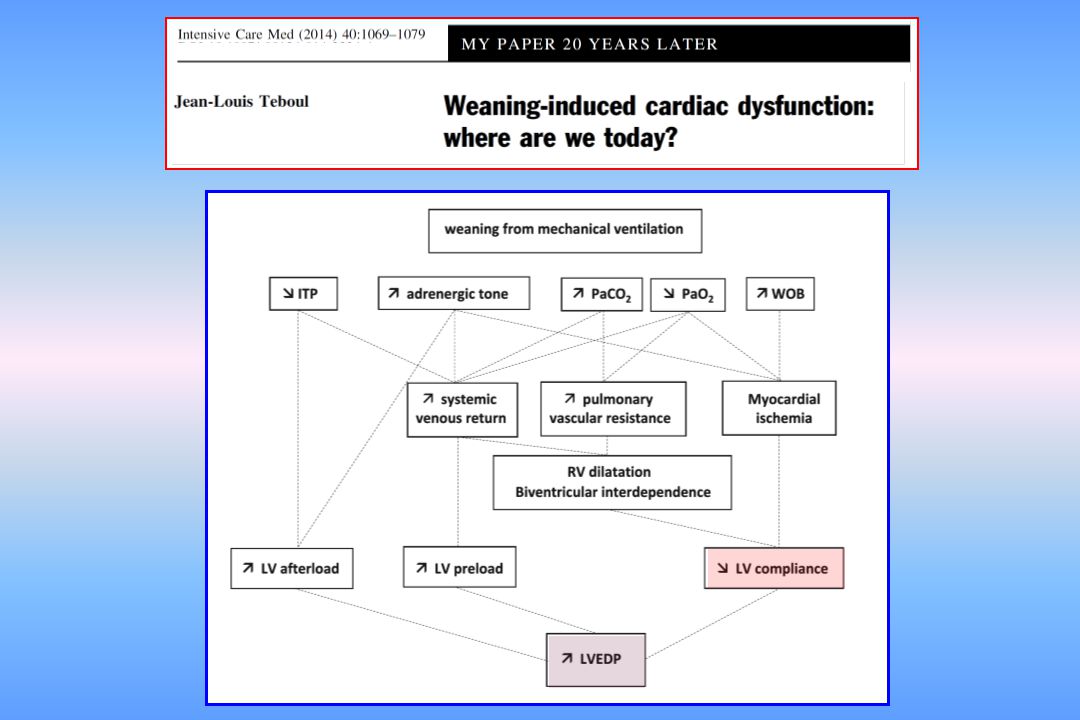
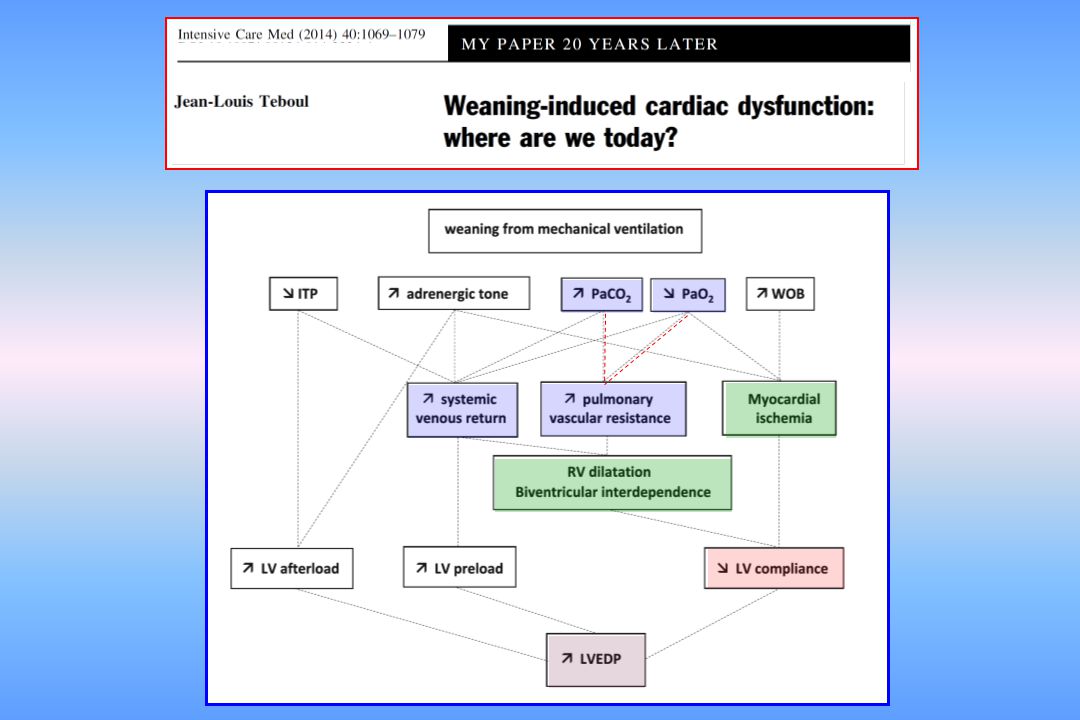
Weaning failure of cardiac origin
Prof. Jean-Louis TEBOUL Medical ICU Bicetre Hospital University Paris-South France

2
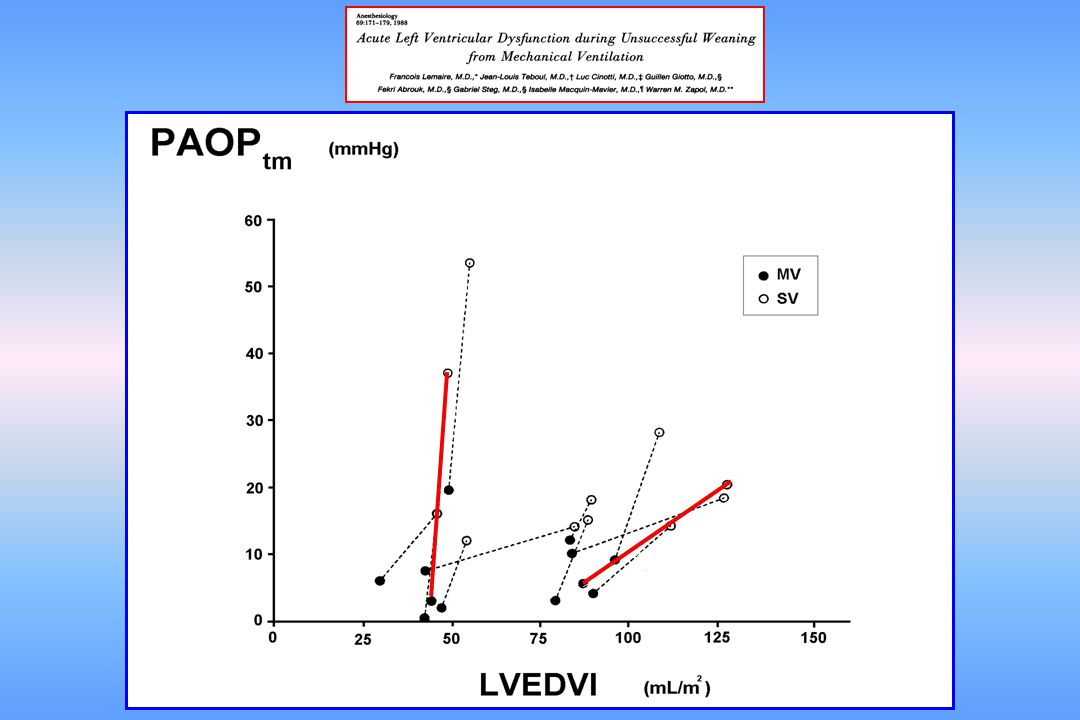
Weaning-induced pulmonary edema may develop
Invasive or non invasive positive pressure ventilation is an established treatment of severe cardiogenic pulmonary edema TREATMENT OF SEVERE CARDIOGENIC PULMONARY EDEMA WITH CONTINUOUS POSITIVE AIRWAY PRESSURE DELIVERED BY FACE MASK Weaning-induced pulmonary edema may develop and may be a cause of weaning failure in predisposed patients

3
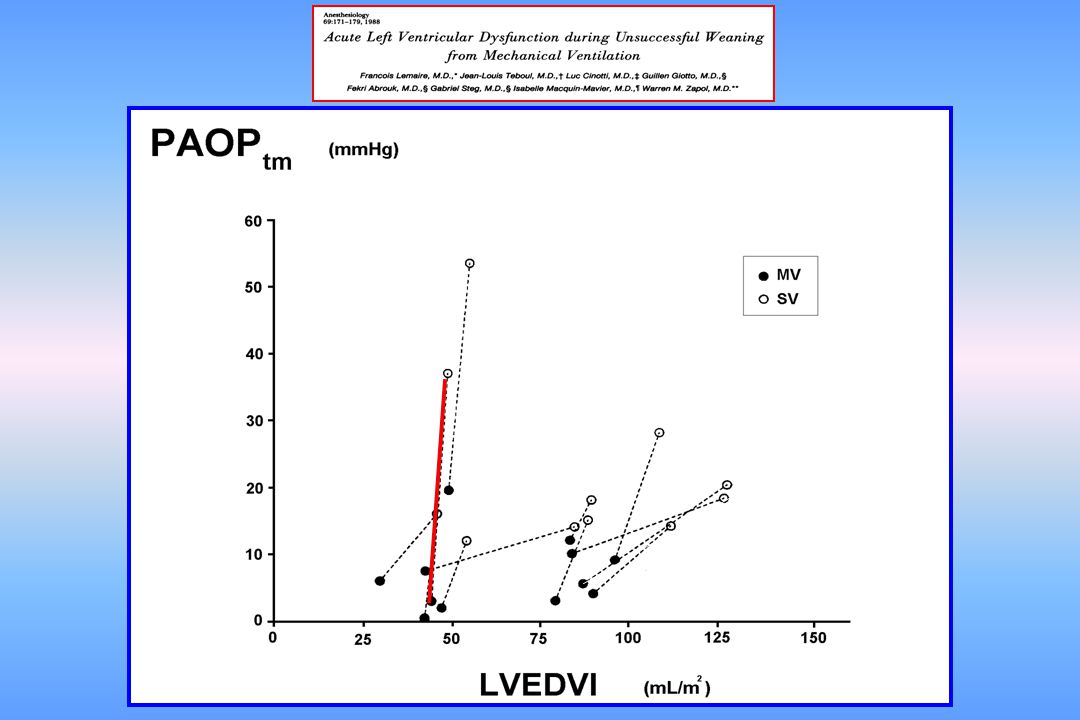
PAOPtm mmHg 60 50 40 30 20 10 MV SB

4
Weaning-induced increase in PAOP

9
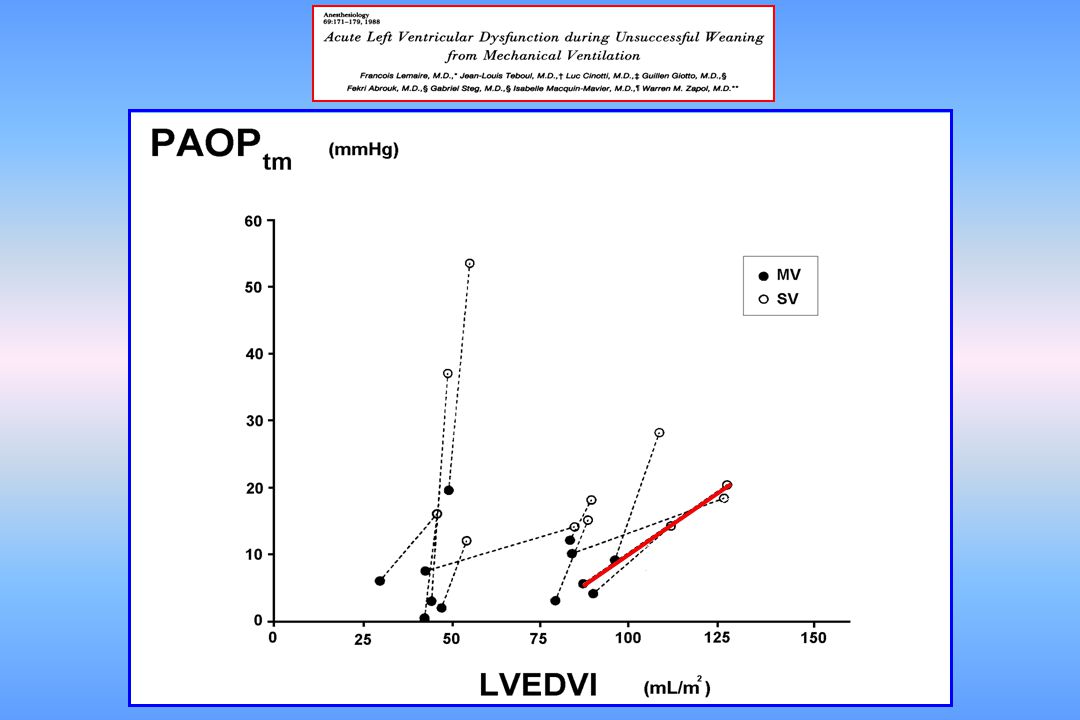
LV end diastolic pressure
B LV end diastolic volume

13
Radionuclide angiocardiography
Left ventricular function during weaning of patients with COPD Richard C, Teboul JL, Archambaud F et al. Intensive Care Med 1994; 20 : 181-6 LVEF (%) Radionuclide angiocardiography during weaning in COPD patients without CAD MV1 SV MV2
 Radionuclide angiocardiography. during weaning. in COPD patients. without CAD. MV1 SV MV2.")
15
LV end diastolic pressure
reduced compliance normal compliance A C B LV end diastolic volume

20
Who are the patients at risk of weaning failure
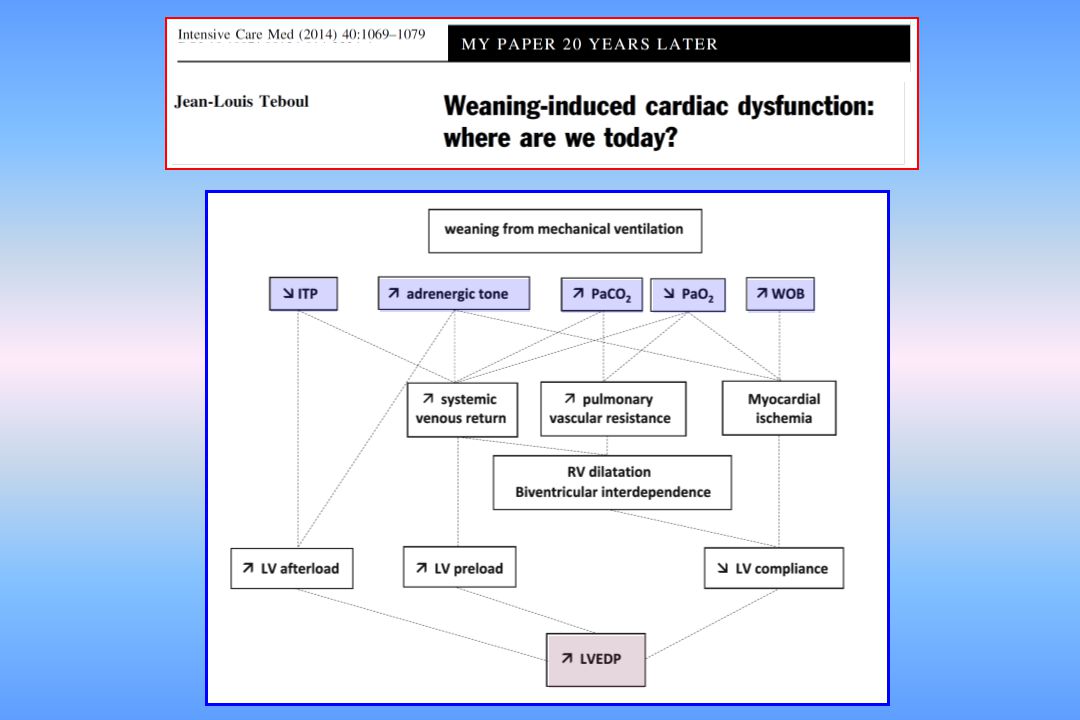
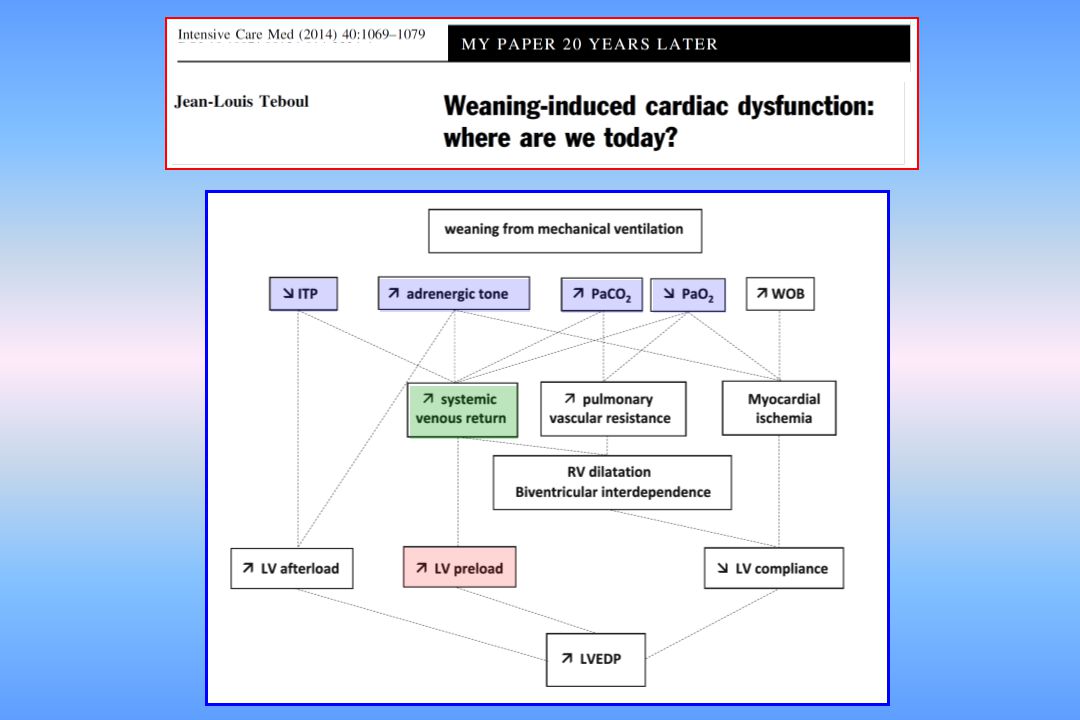
from cardiac origin ? Patients with LV disease (CAD) Increased RV and LV preload and increased LV afterload and associated COPD Deep inspiratory fall in intrathoracic pressure and elevated WOB airway obstruction Increased cardiac work and thus, increased risk of myocardial ischemia biventricular interdependence Decreased LV compliance
 Increased RV and LV preload. and increased LV afterload. and associated COPD. Deep inspiratory fall in intrathoracic pressure and elevated WOB. airway obstruction. Increased cardiac work. and thus, increased. risk of myocardial ischemia. biventricular interdependence. Decreased LV compliance.")
21
When should cardiac-related weaning failure be suspected?
. when CHF and COPD coexist . when other obvious causes of weaning failure have been discarded

22
How to diagnose weaning-induced pulmonary edema?
Weaning trial: T-piece or low level of Pressure support PA catheter ? increase in PAOP

23
How to diagnose weaning-induced pulmonary edema?
Weaning trial: T-piece or low level of Pressure support PA catheter ? Transpulmonary thermodilution? Elevation of EVLW

24
Crit Care Med 2014 Cut-off: 6% AUC = 0.89

25
How to diagnose weaning-induced pulmonary edema?
Weaning trial: T-piece or low level of Pressure support PA catheter ? Transpulmonary thermodilution? Doppler-echo ? E/A and E/E’ assumed to reflect PAOP

26
E A A’ E’ Apical 4-chamber view Pulsed wave Doppler Tissue Doppler or
Doppler criteria for classification of diastolic function. Modified with permission from Redfield et al.15 A’ E’ or 26

27
E E’ E A A’ E’ LV filling pressure determinants LV relaxation reflects
Doppler criteria for classification of diastolic function. Modified with permission from Redfield et al.15 A’ E’ or 27

28
Can E/A and E/E’ at the end of a Spontaneous Breathing Trial
identify weaning failure from cardiac origin defined as a weaning-induced increase in PAOP > 18 mmHg?

29
of each of these variables was not sufficiently acceptable
E/A at the end of the SBT E/E’ at the end of the SBT The predictive value of each of these variables was not sufficiently acceptable to diagnose weaning-induced pulmonary edema 4.0 20 18 3.5 16 3.0 14 2.5 12 2.0 10 8.5 8 1.5 0.95 6 1.0 4 0.5 2 PE - PE + PE - PE +

30
Combination of E/A > 0.95 and E/E’ > 8.5 at the end of a SBT
PE + defined as a PAOP > 18 mmHg at the end of a SBT Se = 82% Sp = 91% PPV = 88% NPV = 87% PE - 20 20 20 18 18 18 Combination of E/A > 0.95 and E/E’ > 8.5 at the end of a SBT predicted weaning-induced pulmonary edema with a high accuracy 16 16 16 14 14 14 the end of the SBT 12 12 12 10 10 10 8.5 at 8 8 8 E/E’ 6 6 6 4 4 4 0.95 2 2 2 - - - 1 1 1 1 1 1 2 2 2 3 3 3 4 4 4 E/A E/A at at the end of the SBT

31
How to diagnose weaning-induced pulmonary edema?
Weaning trial: T-piece or low level of Pressure support PA catheter ? Transpulmonary thermodilution ? Doppler-echo ? BNP or NT-proBNP ?

32
* MV SB MV SB Crit Care Med 2014 weaning-induced pulmonary edema
no weaning-induced pulmonary edema

33
Crit Care Med 2014 AUC = 0.76 BNP

34
How to diagnose weaning-induced pulmonary edema?
Weaning trial: T-piece or low level of Pressure support PA catheter ? Transpulmonary thermodilution ? Doppler-echo ? BNP or NT-proBNP ? Hemoconcentration ?

35
Increase in plasma protein concentration during weaning could detect
Hydrostatic pulmonary edema Increase in plasma protein concentration during weaning could detect weaning-induced pulmonary edema Hemoconcentration

36
59 52 Weaning-induced PO defined as intolerance to SB
and a PAOP > 18 mmHg 59 52

37
SBT-induced change in plasma protein concentration (%)
20 18 16 Se = 85 % Sp= 100 % 14 12 10 8 6 4 2 -2 No weaning-induced P0 Weaning-induced PO Anguel et al Intensive Care Med 2008

38
Crit Care Med 2014 Hb Plasma Protein EVLW BNP

39
Which therapy? Phamacological agents
. Diuretics: if pulmonary edema is assumed to be related to increased preload secondary to increased venous return

40
Am J Respir Crit Care Med 2012; 186:1256-63

41
Am J Respir Crit Care Med 2012; 186:1256-63

42
Time (hrs) to successful weaning
Am J Respir Crit Care Med 2012; 186: Time (hrs) to successful weaning
 to successful weaning.")
43
Which therapy? Phamacological agents
. Diuretics: if pulmonary edema is assumed to be related to increased preload secondary to increased venous return . Nitrates: if suspicion of myocardial ischemia

44
Control day Systolic Arterial Pressure PAOP MV SBTstart SBTend MV
mmHg Control day MV SBTstart SBTend MV SBTstart SBTend

45
Control day PAOP mmHg Study day IV nitrates starting at the beginning
Systolic Arterial Pressure mmHg SBTstart MV SBTend PAOP mmHg Control day Study day IV nitrates starting at the beginning of the SBT

46
Which therapy? Phamacological agents
. Diuretics: if pulmonary edema is assumed to be related to increased preload secondary to increased venous return . Nitrates: if suspicion of myocardial ischemia . Vasodilators: if suspicion of increased LV afterload

47
Which therapy? Phamacological agents
. Diuretics: if pulmonary edema is assumed to be related to increased preload secondary to increased venous return . Nitrates: if suspicion of myocardial ischemia . Vasodilators: if suspicion of increased LV afterload . Inotropes: not logical!

48
PS + PEEP Which therapy? Ventilatory modalities
. Decremental levels of PS and keeping 5 to 8 cmH2O of PEEP . Continue after extubation (facial mask)
")
49
Conclusion weaning failure from cardiac origin is not uncommon
. In case of preexisting cardiac disease, weaning failure from cardiac origin is not uncommon . Complex and intricate mechanisms (vicious circle) generated by marked increased respiratory muscles activity . Its recognition is important since a specific therapy (after individualized evaluation) can result in successful weaning Thank you
 generated. by marked increased respiratory muscles activity. . Its recognition is important since a specific therapy. (after individualized evaluation) can result in successful weaning. Thank you.")
Similar presentations