Download presentation
Presentation is loading. Please wait.

1
IRB 101: Highlights of the History of Human Subjects Protections
Columbia University Medical Center IRB

2
Objective Provide an overview of the events that have led to the system of protections that are currently in place to protect individuals who volunteer for research. Summarize the applicable regulations for the protection of human subjects.

3
Pre-20th Century No formal, widely-accepted codes
Medical practice developed from medical research No formal, widely-accepted codes Reliance on morals, ethical principles of culture, Hippocratic Oath

5
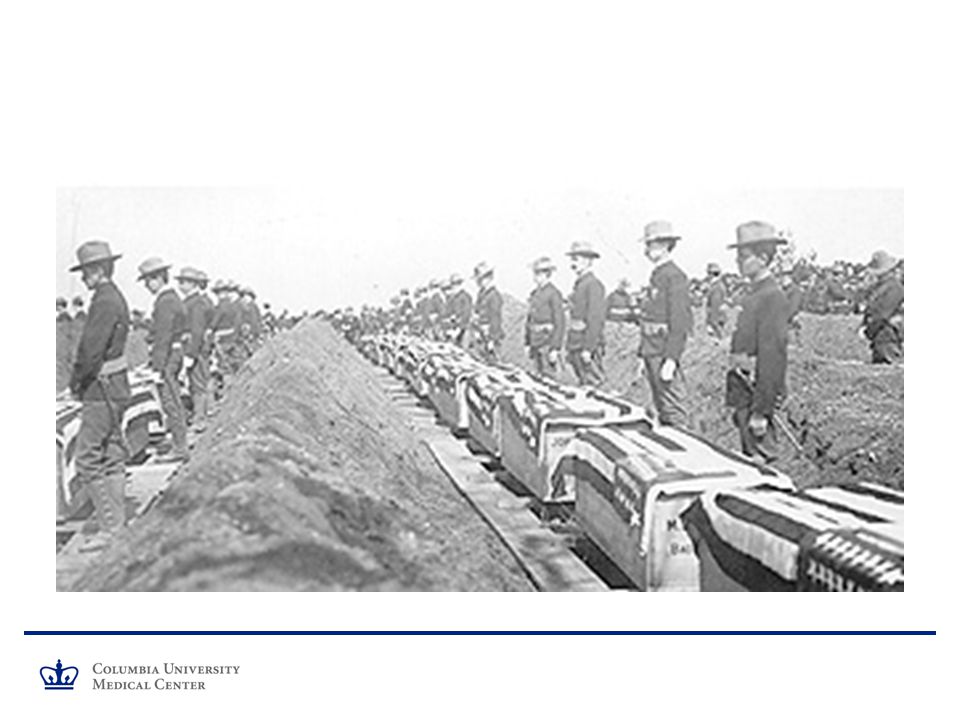
20th Century 1900: Walter Reed’s Yellow Fever experiments
1898: Spanish American War 968 soldiers killed in combat 5000+ died of disease, mostly Yellow Fever United States Army Yellow Fever Commission Major Walter Reed Conducted experiments outside of Havana Proved that the mosquito transmits Yellow Fever First systematic use of informed consent in research

6
Elements present in Yellow Fever Consent Form:
Autonomy (respect for persons): “gives his consent…for the reasons and under the conditions…” Voluntary Participation : “being in the enjoyment and exercise of his own free will” Risks : “In case of the development of yellow fever in him, that he endangers his life to a certain extent.” Benefits : “He will receive from the said commissioner the greatest care and the most skillful medical service.” Compensation: “he will receive the sum of $100 in American gold . . .” Study withdrawal conditions : “The undersigned binds himself not to leave the bounds of this camp during the period of the experiments and will forfeit all right to the benefits named in this contract if he breaks this agreement.”
: gives his consent…for the reasons and under the conditions… Voluntary Participation : being in the enjoyment and exercise of his own free will Risks : In case of the development of yellow fever in him, that he endangers his life to a certain extent. Benefits : He will receive from the said commissioner the greatest care and the most skillful medical service. Compensation: he will receive the sum of $100 in American gold Study withdrawal conditions : The undersigned binds himself not to leave the bounds of this camp during the period of the experiments and will forfeit all right to the benefits named in this contract if he breaks this agreement.")
7
1932: PHS Study of Syphilis Significant health problem
No initial intent to deny treatment Complete physical exam, medical history taken Followed for 6-8 months without treatment New follow-on study started in late 1933 New procedures to strengthen scientific validity, control group No information provided about true nature of study: “government doctors” were examining people for “bad blood” Penicillin accepted as curative treatment in 1943 Not provided Exemption from draft to keep subjects in study

9
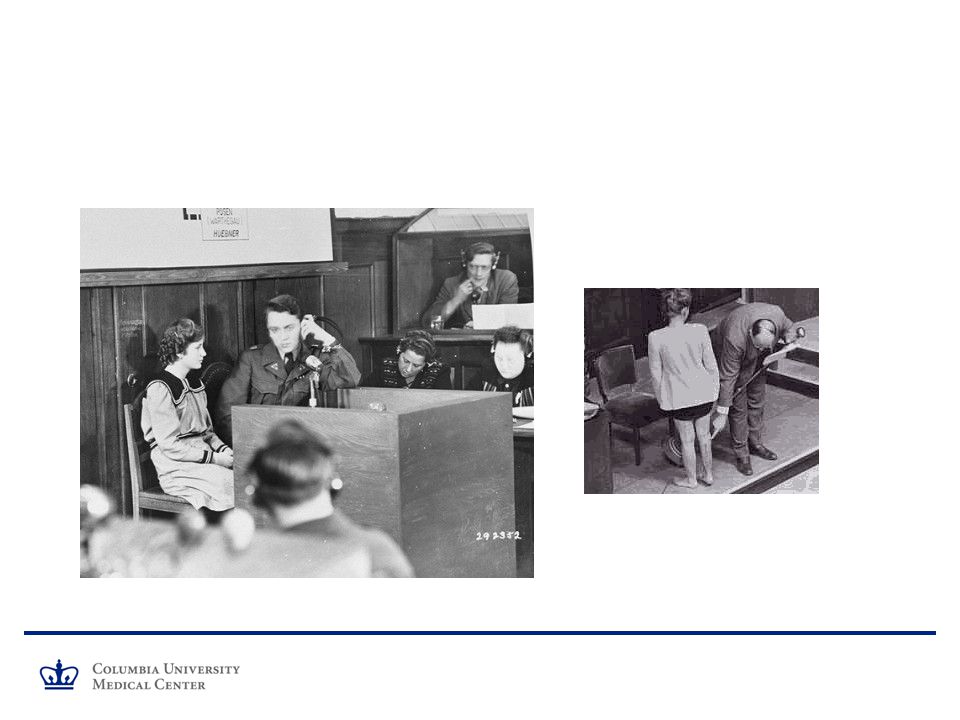
1939-1944 Nazi Experimentation
Findings of the Tribunal: In every single instance appearing in the record, subjects were used who did not consent to the experiments;… In no case was the experimental subject at liberty of his own free choice to withdraw from any experiment. … All of the experiments were conducted with unnecessary suffering and injury and but very little, if any, precautions were taken to protect or safeguard the human subjects from the possibilities of injury, disability, or death. In every one of the experiments the subjects experienced extreme pain or torture, and in most of them they suffered permanent injury, mutilation, or death, either as a direct result of the experiments or because of lack of adequate follow-up care.

10
THE NUREMBERG CODE [from Trials of War Criminals before the Nuremberg Military Tribunals under Control Council Law No. 10. Nuremberg, October 1946–April Washington, D.C.: U.S. G.P.O, 1949–1953.] First Tenet - The voluntary consent of the human subject is absolutely essential.

11
Nuremberg Code and Voluntary Consent
This means that the person involved should: Have legal capacity to give consent Situated as to be able to exercise free power of choice, …; and should have sufficient knowledge and comprehension of the elements of the subject matter involved as to enable him to make an understanding and enlightened decision. This latter element requires that before the acceptance of an affirmative decision by the experimental subject there should be made known to him the nature, duration, and purpose of the experiment The method and means by which it is to be conducted All inconveniences and hazards reasonably to be expected; The effects upon his health or person which may possibly come from his participation in the experiment.

12
Investigator Responsibility
The duty and responsibility for ascertaining the quality of the consent rests upon each individual who initiates, directs or engages in the experiment. It is a personal duty and responsibility which may not be delegated to another with impunity.

14
1946, Fernald School Massachusetts Institute of Technology researchers and Fernald staff members Studies with radioisotopes at the school The first study, in 1946, exposed seventeen students to radioactive iron. The second study exposed fifty seven subjects to radioactive calcium between 1950 and 1953.

15
Fernald Consent Documents
Misleading information implies benefits No mention of radioisotopes Coercive Active consent not required

16
Late 1950’s Thalidomide Tragedy Approved in Europe as sedative
Not approved in U.S. Samples provided to U.S. physicians paid to study safety and efficacy 1962 Amendments to U.S. Food, Drug and Cosmetic Act (Kefauver-Harris Amendments)
")
17
1956-72 Willowbrook New York University researchers
Willowbrook State School for the Retarded, located on Staten Island Residents were injected with a mild form of hepatitis serum The researchers hoped to find a treatment for the virus by studying the disease in it’s earliest stages

18
1961 Milgram Obedience Study
Recruitment by newspaper ad: $4.50 for one hour's work Psychology experiment investigating learning and memory Involved deception Individuals were asked to give what appeared to be real electric shocks to another person The researchers wished to test how far subjects would follow the orders of an experimenter Post-experiment interview

19
1960’s 1964 Declaration of Helsinki – Expansion on Informed Consent
In any research on human beings, each potential subject must be adequately informed of the aims, methods, sources of funding, any possible conflicts of interest, institutional affiliations of the researcher, the anticipated benefits and potential risks of the study and the discomfort it may entail. The subject should be informed of the right to abstain from participation in the study or to withdraw consent to participate at any time without reprisal. After ensuring that the subject has understood the information, the physician should then obtain the subject's freely-given informed consent, preferably in writing. If the consent cannot be obtained in writing, the non-written consent must be formally documented and witnessed. 1966 NIH Policies for the Protection of Human Subjects issued Established the IRB as one mechanism through which human subjects would be protected.

20
1970’s 1972 Syphilis study exposed
Study stopped in March 1973 and treatment provided 1974 National Research Act passed (raised NIH policy to regulation) Required regulations for protection of human subjects Informed consent Institutional Review Boards Created National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research 1979 Belmont Report published by National Commission Respect for persons (informed consent) Beneficence (minimize risk, evaluate risk/benefit ratio) Justice (selection of subjects)
 Required regulations for protection of human subjects. Informed consent. Institutional Review Boards. Created National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research Belmont Report published by National Commission. Respect for persons (informed consent) Beneficence (minimize risk, evaluate risk/benefit ratio) Justice (selection of subjects)")
21
Acknowledgement of History of Violation of Ethical Principles
- Lack of Informed Consent (no respect for persons) Convenience sample bearing burden of research (injustice) Causing harm to subjects (maleficence)
 Convenience sample bearing burden of research (injustice) Causing harm to subjects (maleficence)")
22
1981 Based on Commission’s reports and recommendations:
Significant revisions to HHS and FDA human subject regulations Clarified IRB role No change in general principles of review DHHS regulations codified at Title 45 Part 46 of the Code of Federal Regulations (45 CFR 46) Effective 1/16/81; revised 3/4/83; 6/18/91 1991 revision involved adoption of Federal Policy for Protection of HS – “Common Rule” (Subpart A) – by 16 agencies Subparts B,C,D adopted 1978, 1978, 1983 respectively FDA regulations codified at Title 21 Parts 50 (1980), 56 (1981) Additional regulations for drugs, devices, device classification
 Effective 1/16/81; revised 3/4/83; 6/18/ revision involved adoption of Federal Policy for Protection of HS – Common Rule (Subpart A) – by 16 agencies. Subparts B,C,D adopted 1978, 1978, 1983 respectively. FDA regulations codified at Title 21 Parts 50 (1980), 56 (1981) Additional regulations for drugs, devices, device classification.")
23
Differences between HHS and FDA regulations
Comparison of FDA and HHS Human Subject Protection Regulations: Consult with IRB staff if uncertain about application.

24
Summary Subsequent to abuses of human subjects in research
Formal codes for protection of human subjects relatively recent Subsequent to abuses of human subjects in research Limited in extent of protection

25
IRB 101: IRB Review Criteria and Tips for Submission
Columbia University Medical Center IRB

26
Objectives Describe how submissions are routed for review;
Provide return criteria; Explain the requirements for approval; Demonstrate where in RASCAL information should be entered; Provide tips for a complete and accurate submission. Facilitate more timely review through a better understanding of the IRB review process and review criteria.

27
Submission Process: New Protocols
Protocol submitted to the IRB (“submitted”/Log-in queue); Administrative review conducted by IRB staff: Reviewer form guides review; Performance standards provide timeline; Review comments entered into Notes.
; Administrative review conducted by IRB staff: Reviewer form guides review; Performance standards provide timeline; Review comments entered into Notes.")
28
Submission process: New Protocol (2)
Protocol will be accepted (“logged in”/Chair queue) if complete. PI submits protocol “Submitted” (Log-in queue) Staff review “Logged in” (Chair queue)
 if complete. PI submits protocol. Submitted (Log-in queue) Staff review. Logged in (Chair queue)")
29
Submission process: New Protocol (3)
Return Criteria at log-in stage: Cancer Center is not listed in Facilities section, and the research is cancer-related; PI is not qualified; Consent and/or Assent is not attached, and a waiver has not been requested; Recruitment material is mentioned, but not attached; Study instruments are described, but are not attached; Sponsor’s protocol, IDB, or Package Insert is not attached; Grant, contract, or other documentation of funding agreement is not attached; There is insufficient information to make required determinations.

30
Submission process: New Protocol (4)
Protocol will be returned (“returned”/ Investigator queue) if one or more return criteria are met. PI revises protocol Correspondenc e from Chair to PI PI submits protocol Correspondenc e from team to Chair “Submitted” (Log-in queue) Staff review Correspondenc e from logger to team “Returned” (Investigator queue) PI receives protocol
 if one or more. return criteria. are met. PI revises protocol. Correspondenc e from Chair to PI. PI submits protocol. Correspondenc e from team to Chair. Submitted (Log-in queue) Staff review. Correspondenc e from logger to team. Returned (Investigator queue) PI receives protocol.")
31
Submission process: New Protocol (4)
Overview PI revises protocol Correspondenc e from Chair to PI PI submits protocol Correspondenc e from team to Chair “Submitted” (Log-in queue) Staff review Correspondenc e from logger to team “Logged in” (Chair queue) “Returned” (Investigator queue) PI receives protocol
 Staff review. Correspondenc e from logger to team. Logged in (Chair queue) Returned (Investigator queue) PI receives protocol.")
32
RASCAL tip: Review IRB Submission Manual
Posted on Columbia University’s Office for Clinical Trials website:

33
RASCAL tip: Clarity Describe clearly and accurately what will be done at this site or under the direction of a Columbia investigator; Identify related procedures that will be or have been done elsewhere or previously; Provide clear descriptions of relationships; Accurately describe funding mechanisms; Consistently and precisely describe data collection.

34
Submission Process: Renewals
Similar process, different form Return criteria: Clean copies of consent documents or study instruments not attached; Enrollment information not provided; Documents or fields not updated; Conditions of previous approval not satisfied; All required attachments not provided.

36
RASCAL tip: Review attachments
Archive superceded, reference, HIPAA documents; Review content of attachments for currency, accuracy, outdated approval stamps, and inclusion of new requirements; Review correspondence from previous approval.

37
Submission Process: Modifications
Similar process, summary of modification, assessment of revision in all applicable documents Return criteria: Clear explanation of changes not provided; Description of modification does not match changes in documentation; Changes are described but not incorporated; Supporting documentation not attached.

38
Submission Process: Adverse Event Reports Review New IRB Unanticipated Problems Policy
Unanticipated problem report: Similar process, reconciliation of investigator assessment with UP policy Return criteria: All required documentation not attached; Event does not meet criteria to be reported individually; Investigator’s assessment does not comport with supporting information.

39
RASCAL tip: Name files logically

40
RASCAL tip: Include Correspondence
Cover letter with initial submission. Correspondence or attached “response” with resubmissions. Attached letter to IRB to explain unusual or complex collaborations, centers, affiliations, procedures, etc.

41
IRB Review Low risk protocols may be eligible for exemption (6 categories) Minimal risk protocols may be eligible for expedited review (9 categories) Protocols that are not exempt or cannot be expedited require review by the full Board Time required for review is dependent upon the type of review, complexity and risk level of procedures, and other factors Chair schedule IRB meeting schedule Completeness of submission Other required approvals Recommendation: Submit as soon as all protocol materials are available Allow 60 days for renewal of full Board protocol
 Protocols that are not exempt or cannot be expedited require review by the full Board. Time required for review is dependent upon the type of review, complexity and risk level of procedures, and other factors. Chair schedule. IRB meeting schedule. Completeness of submission. Other required approvals. Recommendation: Submit as soon as all protocol materials are available. Allow 60 days for renewal of full Board protocol.")
42
Review Process: Overview
“Logged in” (Chair queue) Chair reviews or distributes “Distributed” then “Assigned to Meeting” Exempt or expedited Full Board Approve Approve Return Pending Return Defer Disapprove
 Chair reviews or distributes. Distributed then Assigned to Meeting Exempt or expedited. Full Board. Approve. Approve. Return. Pending. Return. Defer. Disapprove.")
43
Criteria for IRB approval of research: 45 CFR 46.111 and 21 CFR 56.111
(a) In order to approve research covered by this policy the IRB shall determine that all of the following requirements are satisfied:
 In order to approve research covered by this policy the IRB shall determine that all of the following requirements are satisfied:")
44
Criteria for IRB approval of research:
1) Risks to subjects are minimized: (i) by using procedures which are consistent with sound research design and which do not unnecessarily expose subjects to risk, and (ii) whenever appropriate, by using procedures already being performed on the subjects for diagnostic or treatment purposes.
 Risks to subjects are minimized: (i) by using procedures which are consistent with sound research design and which do not unnecessarily expose subjects to risk, and (ii) whenever appropriate, by using procedures already being performed on the subjects for diagnostic or treatment purposes.")
45
New protocol considerations:
Research versus clinical care? Design features? Types of risk: physical, social, psychological, economic? Risks reduced or managed to the extent possible? Safeguards incorporated? Potential for statistical validity demonstrated? Investigators competent? Inclusion and exclusion criteria clearly defined? Renewal: Is it the determination of the IRB, based on an evaluation of reported enrollment, adverse events, and unanticipated problems, that risks are still minimized?

46
Modifications: Risks still minimized? Reports of Unanticipated Problems: Unanticipated, related, and suggests increase in risk? Change to protocol and/or consent form needed to reflect new risks?

47
Modifications: If another subject group is being added, or inclusion/exclusion criteria is being revised, does subject selection remain equitable? Reports of Unanticipated Problems: Unanticipated, related, and suggests increase in risk? Change to protocol and/or consent form needed, i.e., is risk to a particular group increased such that inclusion/exclusion criteria need to be revised or consent documents need to be updated?

48
RASCAL entry: Research Page

49
RASCAL entry: Study Description; attachments
1. Study Purpose and Rationale Study Design and Statistical Procedures Study Procedures Study Drugs or Devices Study Questionnaires Study Subjects Recruitment Confidentiality of Study Data Potential Risks Potential Benefits Alternatives

50
Criteria for IRB approval of research: (2) Risks to subjects are reasonable in relation to anticipated benefits, if any, to subjects, and the importance of the knowledge that may reasonably be expected to result. In evaluating risks and benefits, the IRB should consider only those risks and benefits that may result from the research (as distinguished from risks and benefits of therapies subjects would receive even if not participating in the research). The IRB should not consider possible long-range effects of applying knowledge gained in the research (for example, the possible effects of the research on public policy) as among those research risks that fall within the purview of its responsibility.
. The IRB should not consider possible long-range effects of applying knowledge gained in the research (for example, the possible effects of the research on public policy) as among those research risks that fall within the purview of its responsibility..")
51
New protocol considerations:
Acceptable risk/benefit ratio? Ethically acceptable to expose participants to risk of harm? Available alternatives? Renewals: Is it the determination of the IRB that risks are still reasonable in relation to anticipated benefits? Have any subjects been seriously harmed? Should any new information be provided to subjects?

52
Modifications: Risks still reasonable in relation to anticipated benefits? Reports of Unanticipated Problems: Unanticipated, related, and suggests increase in risk? Change to protocol needed to ensure that risk/benefit ratio is still acceptable? Change to consent process needed to notify participants of new risks?

53
RASCAL entry: Study Description; attachments
1. Study Purpose and Rationale Study Design and Statistical Procedures Study Procedures Study Drugs or Devices Study Questionnaires Study Subjects Recruitment Confidentiality of Study Data Potential Risks Potential Benefits Alternatives

54
RASCAL tip: 11 Elements Ensure that all 11 elements of a research protocol are addressed in the Study Description and/or attached protocol; Study Description may be the “only” protocol or serve as an overview of a sponsor’s protocol; Avoid “See attached protocol” as the Board members will receive the Study Description but not attached protocols.

55
Criteria for IRB approval of research: (3) Selection of subjects is equitable. In making this assessment the IRB should take into account the purposes of the research and the setting in which the research will be conducted and should be particularly cognizant of the special problems of research involving vulnerable populations, such as children, prisoners, pregnant women, mentally disabled persons, or economically or educationally disadvantaged persons.

56
New protocol considerations:
Easy availability, compromised position, or susceptibility to manipulation a factor? If potential benefit, particularly for conditions with no effective treatment, are recruitment methods and enrollment criteria objective? Are ethnic groups neither under- or over-represented? Are women and children included where appropriate? Renewals: Has the actual selection/enrollment of subjects represented an equitable distribution of the benefits and burdens of the research (versus the anticipated study population)?
")
57
RASCAL entry: Subjects Page

58
RASCAL entry: Subjects Page

59
RASCAL tip: Subject Selection
Select “Special Populations” options thoughtfully Understand why/when vulnerability exists Justify inclusion of vulnerable groups Consider and include additional protections, or exclude group, as appropriate Select “Recruitment” options accurately Text or documentation must be included in submission

60
Criteria for IRB approval of research: (4) Informed consent will be sought from each prospective subject or the subject's legally authorized representative, in accordance with, and to the extent required by 45 CFR or 21 CFR 50.
 Informed consent will be sought from each prospective subject or the subject s legally authorized representative, in accordance with, and to the extent required by 45 CFR or 21 CFR 50.")
61
New protocol considerations:
Are procedures for an ongoing process described? When and by whom will consent be obtained? How will competency be addressed? Is surrogate consent proposed, and if so, is it acceptable? Is a waiver of consent* requested, and if so, is justification provided? *Not permitted under most circumstances by FDA. Renewals: Has consent been obtained from enrolled subjects? Is the consent process adequate or are changes required (to the process or the form/forms) before additional subjects may be enrolled? Is there new information that should be, but has not yet been, conveyed to enrolled subjects so that they may make an informed choice about continuing their participation?
 before additional subjects may be enrolled Is there new information that should be, but has not yet been, conveyed to enrolled subjects so that they may make an informed choice about continuing their participation")
62
Modifications: Does the consent form need to be revised to reflect change(s) proposed in the modification? Do enrolled subjects need to be advised of the proposed change, e.g., if there are new procedures? Reports of Unanticipated Problems: Unanticipated, related, and suggests increase in risk? Is there new information that may affect enrolled or prospective subjects’ willingness to enroll or continue participation, and should be incorporated into the consent process/form?

63
Basic elements of informed consent
(1) a statement that the study involves research, an explanation of the purposes of the research and the expected duration of the subject's participation, a description of the procedures to be followed, and identification of any procedures which are experimental; (2) a description of any reasonably foreseeable risks or discomforts to the subject; (3) a description of any benefits to the subject or to others which may reasonably be expected from the research; (4) a disclosure of appropriate alternative procedures or courses of treatment, if any, that might be advantageous to the subject; (5) a statement describing the extent, if any, to which confidentiality of records identifying the subject will be maintained;
 a statement that the study involves research, an explanation of the purposes of the research and the expected duration of the subject s participation, a description of the procedures to be followed, and identification of any procedures which are experimental; (2) a description of any reasonably foreseeable risks or discomforts to the subject; (3) a description of any benefits to the subject or to others which may reasonably be expected from the research; (4) a disclosure of appropriate alternative procedures or courses of treatment, if any, that might be advantageous to the subject; (5) a statement describing the extent, if any, to which confidentiality of records identifying the subject will be maintained;")
64
Basic elements of informed consent (2)
(6) for research involving more than minimal risk, an explanation as to whether any compensation and an explanation as to whether any medical treatments are available if injury occurs and, if so, what they consist of, or where further information may be obtained; (7) an explanation of whom to contact for answers to pertinent questions about the research and research subjects' rights, and whom to contact in the event of a research-related injury to the subject; and (8) a statement that participation is voluntary, refusal to participate will involve no penalty or loss of benefits to which the subject is otherwise entitled, and the subject may discontinue participation at any time without penalty or loss of benefits to which the subject is otherwise entitled.
 for research involving more than minimal risk, an explanation as to whether any compensation and an explanation as to whether any medical treatments are available if injury occurs and, if so, what they consist of, or where further information may be obtained; (7) an explanation of whom to contact for answers to pertinent questions about the research and research subjects rights, and whom to contact in the event of a research-related injury to the subject; and. (8) a statement that participation is voluntary, refusal to participate will involve no penalty or loss of benefits to which the subject is otherwise entitled, and the subject may discontinue participation at any time without penalty or loss of benefits to which the subject is otherwise entitled.")
65
Additional elements of informed consent
(1) a statement that the particular treatment or procedure may involve risks to the subject (or to the embryo or fetus, if the subject is or may become pregnant) which are currently unforeseeable; (2) anticipated circumstances under which the subject's participation may be terminated by the investigator without regard to the subject's consent; (3) any additional costs to the subject that may result from participation in the research; (4) the consequences of a subject's decision to withdraw from the research and procedures for orderly termination of participation by the subject; (5) A statement that significant new findings developed during the course of the research which may relate to the subject's willingness to continue participation will be provided to the subject; and (6) the approximate number of subjects involved in the study.
 a statement that the particular treatment or procedure may involve risks to the subject (or to the embryo or fetus, if the subject is or may become pregnant) which are currently unforeseeable; (2) anticipated circumstances under which the subject s participation may be terminated by the investigator without regard to the subject s consent; (3) any additional costs to the subject that may result from participation in the research; (4) the consequences of a subject s decision to withdraw from the research and procedures for orderly termination of participation by the subject; (5) A statement that significant new findings developed during the course of the research which may relate to the subject s willingness to continue participation will be provided to the subject; and. (6) the approximate number of subjects involved in the study.")
66
RASCAL entry: Consent Form Builder

67
RASCAL tip: Select Layout; Review Form

68
Waiver criteria: 45 CFR 46.116(d)
(1) the research involves no more than minimal risk to the subjects; (2) the waiver or alteration will not adversely affect the rights and welfare of the subjects; (3) the research could not practicably be carried out without the waiver or alteration; and (4) whenever appropriate, the subjects will be provided with additional pertinent information after participation.
 the research involves no more than minimal risk to the subjects; (2) the waiver or alteration will not adversely affect the rights and welfare of the subjects; (3) the research could not practicably be carried out without the waiver or alteration; and. (4) whenever appropriate, the subjects will be provided with additional pertinent information after participation.")
69
Waiver criteria: 45 CFR 46.116(c)
(1) the research or demonstration project is to be conducted by or subject to the approval of state or local government officials and is designed to study, evaluate, or otherwise examine: (i) public benefit or service programs; (ii) procedures for obtaining benefits or services under those programs; (iii) possible changes in or alternatives to those programs or procedures; or (iv) possible changes in methods or levels of payment for benefits or services under those programs; and (2) the research could not practicably be carried out without the waiver or alteration.
 the research or demonstration project is to be conducted by or subject to the approval of state or local government officials and is designed to study, evaluate, or otherwise examine: (i) public benefit or service programs; (ii) procedures for obtaining benefits or services under those programs; (iii) possible changes in or alternatives to those programs or procedures; or (iv) possible changes in methods or levels of payment for benefits or services under those programs; and. (2) the research could not practicably be carried out without the waiver or alteration.")
70
RASCAL entry: Subjects Page

71
Criteria for IRB approval of research:
(5) Informed consent will be appropriately documented, in accordance with, and to the extent required by 45 CFR or 21 CFR
 Informed consent will be appropriately documented, in accordance with, and to the extent required by 45 CFR or 21 CFR")
72
New protocol considerations:
Is use of a written consent document proposed? Does the consent document contain required elements, exclude exculpatory language, and include optional elements where appropriate? Is waiver of written documentation of consent requested, and if so, is justification provided? Will a copy of the form be provided to subjects? If verbal consent will be obtained, are appropriate procedures proposed? Renewals: Has consent been appropriately documented for enrolled subjects? Have subject complaints about the consent process been received?

73
Waiver of written documentation criteria: 45 CFR 46.117(c)
(1) The only record linking the subject and the research would be the consent document and the principal risk would be potential harm resulting from a breach of confidentiality. Each subject will be asked whether the subject wants documentation linking the subject with the research, and the subject's wishes will govern; or (2) The research presents no more than minimal risk of harm to subjects and involves no procedures for which written consent is normally required outside of the research context.
 The only record linking the subject and the research would be the consent document and the principal risk would be potential harm resulting from a breach of confidentiality. Each subject will be asked whether the subject wants documentation linking the subject with the research, and the subject s wishes will govern; or. (2) The research presents no more than minimal risk of harm to subjects and involves no procedures for which written consent is normally required outside of the research context.")
74
Criteria for IRB approval of research:
(6) When appropriate, the research plan makes adequate provision for monitoring the data collected to ensure the safety of subjects.
 When appropriate, the research plan makes adequate provision for monitoring the data collected to ensure the safety of subjects.")
75
New protocol considerations:
Is a data and safety monitoring plan needed? Are proposed data and safety monitoring procedures adequate? Will the consent process be monitored? Renewals: Has the IRB been informed of any unforeseen problems or accidents that may have occurred? Do reports of adverse events and monitoring bodies reflect that the data are being adequately monitored? Should the IRB request that progress reports be submitted at regular intervals, more often than annually?

76
Modifications: Does the modification revise procedures in such a way that the data and safety monitoring plan, or other oversight of the study, needs to be revised? Reports of Unanticipated Problems: Unanticipated, related, and suggests increase in risk? Is more frequent or different monitoring needed as a result of the unanticipated problem?

77
RASCAL entry: Study Description; attachments
1. Study Purpose and Rationale Study Design and Statistical Procedures Study Procedures Study Drugs or Devices Study Questionnaires Study Subjects Recruitment Confidentiality of Study Data Potential Risks Potential Benefits Alternatives

78
Criteria for IRB approval of research:
(7) When appropriate, there are adequate provisions to protect the privacy of subjects and to maintain the confidentiality of data.
 When appropriate, there are adequate provisions to protect the privacy of subjects and to maintain the confidentiality of data.")
79
New protocol considerations:
In what manner will data be gathered and maintained (anonymously, de-identified, coded, identifiable)? Are procedures for collecting and storing identifiable data adequate to reduce risk of breach of confidentiality? If data will be transmitted to another site, are procedures appropriate? Does the consent document adequately reflect data confidentiality issues and potential breaches? Are research personnel trained in privacy practices? Renewals: Have there been complaints from subjects, or reports of unanticipated problems related to privacy and confidentiality?
 Are procedures for collecting and storing identifiable data adequate to reduce risk of breach of confidentiality If data will be transmitted to another site, are procedures appropriate Does the consent document adequately reflect data confidentiality issues and potential breaches Are research personnel trained in privacy practices Renewals: Have there been complaints from subjects, or reports of unanticipated problems related to privacy and confidentiality")
80
Modifications: Is more sensitive information being collected, such that the measures in place to protect confidentiality need to be enhanced? Reports of Unanticipated Problems: Unanticipated, related, and suggests increase in risk? Has a breach of confidentiality occurred, which requires reassessment of plans to protect confidential data?

81
RASCAL entry: Study Description
1. Study Purpose and Rationale Study Design and Statistical Procedures Study Procedures Study Drugs or Devices Study Questionnaires Study Subjects Recruitment Confidentiality of Study Data Potential Risks Potential Benefits Alternatives

82
IRB 101: Vulnerable Populations
Columbia University Medical Center IRB

83
Criteria for IRB approval of research: 45 CFR 46.111 and 21 CFR 56.111
When some or all of the subjects are likely to be vulnerable to coercion or undue influence, such as children, prisoners, pregnant women, mentally disabled persons, or economically or educationally disadvantaged persons, additional safeguards have been included in the study to protect the rights and welfare of these subjects.

84
New protocols considerations:
Is information included for the required determinations of Subparts B (pregnant women, fetuses), C (prisoners), and D (children and minors) to be made? Do consent processes adequately address the needs of vulnerable subjects, e.g., translations, legally authorized representatives? How will competency to provide consent be determined? Are procedures in place to address loss of cognitive ability during the trial? Renewals: Are the determinations required by the Subparts still acceptable? Should competency be reassessed?
, C (prisoners), and D (children and minors) to be made Do consent processes adequately address the needs of vulnerable subjects, e.g., translations, legally authorized representatives How will competency to provide consent be determined Are procedures in place to address loss of cognitive ability during the trial Renewals: Are the determinations required by the Subparts still acceptable Should competency be reassessed")
85
Subpart B: Pregnant Women & Human Fetuses. (46
Subpart B: Pregnant Women & Human Fetuses (46.204) Assessment of risks made by the IRB Where scientifically appropriate, preclinical studies, including studies on pregnant animals, and clinical studies, including studies on non-pregnant women, have been conducted and provide data for assessing potential risks to pregnant women and fetuses. The risk to the fetus is caused solely by interventions or procedures that hold out the prospect of direct benefit for the woman or the fetus; or, if there is no such prospect of benefit, the risk to the fetus is not greater than minimal and the purpose of the research is the development of important biomedical knowledge which cannot be obtained by any other means. Any risk is the least possible for achieving the objectives of the research.
 Assessment of risks made by the IRB. Where scientifically appropriate, preclinical studies, including studies on pregnant animals, and clinical studies, including studies on non-pregnant women, have been conducted and provide data for assessing potential risks to pregnant women and fetuses. The risk to the fetus is caused solely by interventions or procedures that hold out the prospect of direct benefit for the woman or the fetus; or, if there is no such prospect of benefit, the risk to the fetus is not greater than minimal and the purpose of the research is the development of important biomedical knowledge which cannot be obtained by any other means. Any risk is the least possible for achieving the objectives of the research.")
86
In English… If the study involves greater than minimal risk to the fetus, there must be a prospect for direct benefit for the mother or the fetus. There must also be preclinical studies assessing the potential risk, and the study must be designed to minimize risk to the extent possible. If the study involves no benefit to the mother or fetus, the risk to the fetus must be minimal and the least possible to achieve the objectives of the research. Further, the research must be designed to develop important biomedical knowledge that cannot be obtained any other way.

87
Consent Requirements for Research Involving
Consent Requirements for Research Involving Pregnant Women & Human Fetuses If the research holds out the prospect of direct benefit to the pregnant woman, the prospect of a direct benefit both to the pregnant woman and the fetus, or no prospect of benefit for the woman nor the fetus and the risk to the fetus is minimal, consent of ONLY the pregnant woman is required. If the research holds out the prospect of direct benefit to the fetus only, then the consent of the pregnant woman AND the father must be obtained. The father's consent need not be obtained if he is unable to consent because of unavailability, incompetence, or temporary incapacity or the pregnancy resulted from rape or incest. Each individual providing consent is fully informed regarding the reasonably foreseeable impact of the research on the fetus or neonate.

88
Additional Requirements for Research Involving
Additional Requirements for Research Involving Pregnant Women and Human Fetuses For children as defined who are pregnant, assent and permission are obtained in accord with the provisions of subpart D. No inducements, monetary or otherwise, will be offered to terminate a pregnancy. Individuals engaged in the research will have no part in any decisions as to the timing, method, or procedures used to terminate a pregnancy. Individuals engaged in the research will have no part in determining the viability of a neonate.

89
Research Involving Neonates - Non-viable or of Uncertain Viability (46.205) Research involving, after delivery, the placenta, the dead fetus or fetal material (46.206) Additional considerations apply and determinations must be made. Consult with the IRB before submitting for tailored guidance.

90
Research Not Otherwise Approvable (46.207)
The IRB finds that the research presents a reasonable opportunity to further the understanding, prevention, or alleviation of a serious problem affecting the health or welfare of pregnant women, fetuses or neonates; and The Secretary, after consultation with a panel of experts in pertinent disciplines and following opportunity for public review and comment, including a public meeting announced in the FEDERAL REGISTER, agrees with the above determination or disagrees with the IRB’s conclusions and finds the research approvable according to current regulations

91
Subpart C: Prisoners Relevant Definitions
Prisoner - any individual involuntarily confined or detained in a penal institution, including: individuals sentenced to such an institution under a criminal or civil statute; individuals detained in other facilities by virtue of statutes or commitment procedures which provide alternatives to criminal prosecution or incarceration in a penal institution; and individuals detained pending arraignment, trial, or sentencing. In other words….. A resident of a drug rehabilitation center who is in treatment as an alternative to jail would qualify as a “prisoner”. Children in juvenile detention halls qualify as prisoners. If subjects enroll in the research and are then incarcerated, subpart C applies.

92
Subpart C: Prisoners Relevant Definitions
“Minimal risk" is the probability and magnitude of physical or psychological harm that is normally encountered in the daily lives, or in the routine medical, dental, or psychological examination of healthy persons. Minimal risk means that the probability and magnitude of harm or discomfort anticipated in the research are not greater in and of themselves than those ordinarily encountered in daily life or during the performance of routine physical or psychological examinations or tests.

93
Prisoners: IRB Review Prisoner representative must be present.
The majority of the Board must have no association with the prison. For research funded by DHHS, the institution must certify to the Secretary that the required findings under subpart C have been made. The research cannot commence until OHRP has approved the research.

94
Prisoners: Approvable Categories of Research
Study of the possible causes, effects, and processes of incarceration, and of criminal behavior, provided that the study presents no more than minimal risk and no more than inconvenience to the subjects. Study of prisons as institutional structures or of prisoners as incarcerated persons, provided that the study presents no more than minimal risk and no more than inconvenience to the subjects.

95
Prisoners: Approvable Categories of Research
Research on conditions particularly affecting prisoners as a class (for example, vaccine trials and other research on hepatitis which is much more prevalent in prisons than elsewhere; and research on social and psychological problems such as alcoholism, drug addiction, and sexual assaults) provided that the study may proceed only after the Secretary has consulted with appropriate experts including experts in penology, medicine, and ethics, and published notice, in the FEDERAL REGISTER, of his intent to approve such research. All research funded by DHHS must be approved by the Secretary prior to initiation. All research involving prisoners that is greater than minimal risk must also undergo secretarial consultation and published in the federal register before initiation.
 provided that the study may proceed only after the Secretary has consulted with appropriate experts including experts in penology, medicine, and ethics, and published notice, in the FEDERAL REGISTER, of his intent to approve such research. All research funded by DHHS must be approved by the Secretary prior to initiation. All research involving prisoners that is greater than minimal risk must also undergo secretarial consultation and published in the federal register before initiation.")
96
Prisoners: Approvable Categories of Research
Research on practices, both innovative and accepted, which have the intent and reasonable probability of improving the health or well-being of the subject. In cases in which those studies require the assignment of prisoners in a manner consistent with protocols approved by the IRB to control groups which may not benefit from the research, the study may proceed only after the Secretary has consulted with appropriate experts, including experts in penology, medicine, and ethics, and published notice, in the FEDERAL REGISTER, of the intent to approve such research.

97
Prisoners: Required findings by the IRB
The research under review represents one of the previously mentioned categories of research. Any possible advantages accruing to the prisoner through his or her participation in the research, when compared to the general living conditions, medical care, quality of food, amenities and opportunity for earnings in the prison, are not of such a magnitude that his or her ability to weigh the risks of the research against the value of such advantages in the limited choice environment of the prison is impaired.

98
Prisoners: Required findings by the IRB
The risks involved in the research are commensurate with risks that would be accepted by non-prisoner volunteers. Procedures for the selection of subjects within the prison are fair to all prisoners and immune from arbitrary intervention by prison authorities or prisoners. Unless the principal investigator provides to the Board justification in writing for following some other procedures, control subjects must be selected randomly from the group of available prisoners who meet the characteristics needed for that particular research project.

99
Prisoners: Required findings by the IRB
The information is presented in language which is understandable to the subject population. Adequate assurance exists that parole boards will not take into account a prisoner's participation in the research in making decisions regarding parole, and each prisoner is clearly informed in advance that participation in the research will have no effect on his or her parole.

100
Prisoners: Required findings by the IRB
Where the Board finds there may be a need for follow-up examination or care of participants after the end of their participation, adequate provision has been made for such examination or care, taking into account the varying lengths of individual prisoners' sentences, and for informing participants of this fact.

101
Children – Subpart D of 45 CFR 46 and 21 CFR 50
Risk Determination Parental Permission Requirements Assent Requirements Wards?

102
Research with Children
When children or minors will be subjects, the IRB must determine and provide the basis for their determination of: 1. Category of research: §46.404/§50.51 Research not involving greater than minimal risk. § /§50.52 Research involving greater than minimal risk but presenting the prospect of direct benefit to the individual subjects. § /§50.53 Research involving greater than minimal risk and no prospect of direct benefit to individual subjects, but likely to yield generalizable knowledge about the subject's disorder or condition. § /§50.54 Research not otherwise approvable which presents an opportunity to understand, prevent, or alleviate a serious problem affecting the health or welfare of children.

103
Research with Children (2)
2. Requirements for parental permission: One or both parents may provide permission for research in categories §46.404/§50.51 and §46.405/§50.52. Both parents must provide permission for research in categories §46.406/§50.53 and §46.407/§50.54. 3. Whether assent should be obtained: Considering age and maturity of the children Evaluating whether effective alternatives are available 4. Whether wards will be involved: An advocate must be provided for each ward that is enrolled

104
Subpart D: Minimal Risk Research “Section 404 Research”
Risk Determination In order for a study to be categorized under section 404(DHHS) or section 51(FDA), the research has to pose minimal risk to the children involved. The regulators define minimal risk as: the probability and magnitude of harm or discomfort anticipated in the research are not greater in and of themselves than those ordinarily encountered in daily life or during the performance of routine physical or psychological examinations or tests. The CUMC IRB’s interpret this to apply to the daily lives of normal children. The permission of one parent must be obtained unless consent is waived by the IRB. The assent of the child is obtained or the IRB has waived the assent requirements.
 or section 51(FDA), the research has to pose minimal risk to the children involved. The regulators define minimal risk as: the probability and magnitude of harm or discomfort anticipated in the research are not greater in and of themselves than those ordinarily encountered in daily life or during the performance of routine physical or psychological examinations or tests. The CUMC IRB’s interpret this to apply to the daily lives of normal children. The permission of one parent must be obtained unless consent is waived by the IRB. The assent of the child is obtained or the IRB has waived the assent requirements.")
105
Subpart D: Research presenting Greater than
Subpart D: Research presenting Greater than Minimal Risk with potential for Direct Benefit “Section 405 Research” Risk Determination The risk is justified by the anticipated benefit to the subjects; The relation of the anticipated benefit to the risk is at least as favorable to the subjects as that presented by available alternative approaches. Adequate provisions are made for soliciting the assent of the children or the IRB has waived the assent requirements. Permission of one parent is obtained unless waived by the IRB.

106
Subpart D: Research presenting Greater than
Subpart D: Research presenting Greater than Minimal Risk with No anticipated Direct Benefit “Section 406 Research” Risk Determination The risk represents a minor increase over minimal risk; The intervention or procedure presents experiences to subjects that are reasonably commensurate with those inherent in their actual or expected medical, dental, psychological, social, or educational situations; The intervention or procedure is likely to yield generalizable knowledge about the subjects' disorder or condition which is of vital importance for the understanding or amelioration of the subjects' disorder or condition; Adequate provisions are made for soliciting the assent of the children. Permission of BOTH parents is obtained unless one parent is deceased, unknown, incompetent, or not reasonably available, or when only one parent has legal responsibility for the care and custody of the child. WARDS

107
Subpart D: Research Not Approvable according to
Subpart D: Research Not Approvable according to Sections 404, 405 or 406 (FDA 51, 52, or 53) “Section 407 Research” Risk Determination The research presents a reasonable opportunity to further the understanding, prevention, or alleviation of a serious problem affecting the health or welfare of children; and Referral to DHHS for secretarial consultation The Secretary, after consultation with a panel of experts in pertinent disciplines (for example: science, medicine, education, ethics, law) and following opportunity for public review and comment, agrees with the above determination or disagrees with the IRB’s conclusions and finds the research approvable according to current regulations. Adequate provisions are made for soliciting the assent of the children. Permission of BOTH parents is obtained unless one parent is deceased, unknown, incompetent, or not reasonably available, or when only one parent has legal responsibility for the care and custody of the child.
 Section 407 Research Risk Determination. The research presents a reasonable opportunity to further the understanding, prevention, or alleviation of a serious problem affecting the health or welfare of children; and. Referral to DHHS for secretarial consultation. The Secretary, after consultation with a panel of experts in pertinent disciplines (for example: science, medicine, education, ethics, law) and following opportunity for public review and comment, agrees with the above determination or disagrees with the IRB’s conclusions and finds the research approvable according to current regulations. Adequate provisions are made for soliciting the assent of the children. Permission of BOTH parents is obtained unless one parent is deceased, unknown, incompetent, or not reasonably available, or when only one parent has legal responsibility for the care and custody of the child.")
108
Inclusion of Wards in Research
If wards are to be enrolled in sections 406 or 407 research: Detailed information about the proposed informed consent process as well as detailed information regarding the identity and authority of any individual who will provide consent must be provided to the IRB. The research must be: Related to their status as wards; or Conducted in schools, camps, hospitals, etc. in which the majority of the subjects involved in the research are not wards. An advocate for each ward must be appointed to act on behalf of the child. The advocate must have the background and experience to act in the best interest of the child throughout the research and cannot be associated in any way with the research, the investigator or the guardian institution. In NY, the Administration for Children’s Services (ACS) must agree to the inclusion of wards in the research and permission must be obtained from the person designated by ACS for each ward who is enrolled.
 must agree to the inclusion of wards in the research and permission must be obtained from the person designated by ACS for each ward who is enrolled.")
109
Parental Permission – Waiver Options
Parental permission can be waived: If the research a) poses no more than minimal risk; b) does not negatively impact upon the rights and/or welfare of the subjects; c) renders it impracticable to obtain consent; and d) provides for informing subjects of any additional pertinent information upon completion of the research. If the research protocol is designed for conditions or for a subject population for which parental or guardian permission is not a reasonable requirement to protect the subjects (for example, neglected or abused children), and an appropriate mechanism for protecting the children who will participate as subjects in the research is substituted.
 poses no more than minimal risk; b) does not negatively impact upon the rights and/or welfare of the subjects; c) renders it impracticable to obtain consent; and d) provides for informing subjects of any additional pertinent information upon completion of the research. If the research protocol is designed for conditions or for a subject population for which parental or guardian permission is not a reasonable requirement to protect the subjects (for example, neglected or abused children), and an appropriate mechanism for protecting the children who will participate as subjects in the research is substituted.")
110
Assent Requirements In general:
Applies to children 7 and older who are capable of assenting When determining capability, ages, maturity level and psychological state must be taken into account. Ages 7 through 11: Written or verbal Ages 12 through 17: Written A separate age appropriate assent can be provided or the child can co-sign the parental consent.

111
Exceptions from Assent Requirements
Waiver of assent is granted by the IRB in accordance with The intervention or procedure involved in the research holds out a prospect of direct benefit that is important to the health or well-being of the children and is available only in the context of the research.

112
IRB Submissions If your research involves vulnerable subjects:
RASCAL questions Ensure your protocol submission includes adequate information for the IRB to make the determinations required as outlined in the previous slides. As always, call the IRB office (contact information for individual staff on website) with any questions.
 with any questions.")
113
References DHHS OHRP - Subpart B (Pregnant women, human fetuses and neonates) tb DHHS OHRP - Subpart C (Prisoners) tc DHHS OHRP - Subpart D (Children) td FDA - Subpart D (Children) m?CFRPart=50&showFR=1&subpartNode=21:
 tc. DHHS OHRP - Subpart D (Children) td. FDA - Subpart D (Children) m CFRPart=50&showFR=1&subpartNode=21:")
114
Research with Other Vulnerable Individuals
When inclusion of subjects with a specific vulnerability is proposed: Justify selection of this group; Include plans for additional protections relative to vulnerability; If status is variable, include plans for periodic assessment; Clearly describe any special consent procedures; Provide local or expert documentation, as applicable.

115
IRB Actions Approve Require modifications
defer to Chair as “pending” or defer to Board as “returned” Defer Suspend enrollment* Suspend the study* Terminate* *Reportable to OHRP and/or FDA, as applicable, sponsor, subjects, institution

116
An IRB may also: Impose additional precautions or reassess special requirements previously imposed e.g., the IRB has the authority to observe or have a third party observe, the consent process as well as the research itself [45 CFR (e) and 21 CFR (f)]
 and 21 CFR (f)]")
117
Summary IRB Review Criteria Tips for Submitting RASCAL

118
Columbia University Medical Center IRB
IRB 101: Case Study Columbia University Medical Center IRB

119
Initial submission Industry-sponsored, Phase III, double-blind, randomized clinical trial to study the effects of Drug A on Type 2 diabetes mellitus. The subjects will be patients already in the care of either Dr. PI or Dr. Co-I, or will be recruited from patients in the care of other endocrinologists at the medical center. It is anticipated that all subjects will be English-speaking. Subject compensation: Subjects will be paid $1,500 for the entire study. Payment will be received at the end of the entire study after all study procedures have been completed. In each phase of the study, subjects will receive a radioactive isotope to detect a newly identified protein that has been shown to affect insulin production in animal studies. Six out of seven members of the study team have completed required GCP and HIPAA training via the RASCAL online testing center. Level of review? IRB considerations?

120
First modification Revised consent form based on a request from the Radiation Drug Research Committee that a statement required by the FDA to collect an additional blood sample to assess a new toxicity that was found in a phase II study and that is possibly associated with the isotope' regarding the limits for radiation exposure be included. This change was made in the consent form under the “Procedures” and "Risks" sections. Level of review? IRB considerations?

121
Second modification 1) Revision of the blood pressure inclusion criterion to accept patients with blood pressure < 140/90 mm Hg on blood pressure lowering therapy. (The current IRB-approved protocol requires a blood pressure < 130/90 on therapy.) 2) Submission of a recruitment flyer for IRB approval. The flyer will be posted at sites accessible to potential study subjects and will be used to expedite and expand patient recruitment. Level of review? IRB considerations?
 Revision of the blood pressure inclusion criterion to accept patients with blood pressure < 140/90 mm Hg on blood pressure lowering therapy. (The current IRB-approved protocol requires a blood pressure < 130/90 on therapy.) 2) Submission of a recruitment flyer for IRB approval. The flyer will be posted at sites accessible to potential study subjects and will be used to expedite and expand patient recruitment. Level of review IRB considerations")
122
Third modification 1) Spanish patient recruitment flyer.
2) Consent form translated in Spanish. Each of the Spanish documents has been translated from its approved English counterpart by the investigator. Level of review? IRB considerations?
 Consent form translated in Spanish. Each of the Spanish documents has been translated from its approved English counterpart by the investigator. Level of review IRB considerations")
123
Fourth modification 1) Addition of two co-investigators to the study team. 2) Changes to study inclusion and exclusion criteria in order to: a. Require a history of stable diabetes therapy for 6 weeks (instead of 3 months). b. Include patients taking metformin only (without a sulfonylurea). c. Include patients with cardiovascular disease (except Class III-V CHF). d. Include patients taking diuretics e. Include patients with stable, treated thyroid disease. 3) Modification of study protocol and consent to reflect collection of DNA during study. Level of review? IRB considerations?
. b. Include patients taking metformin only (without a sulfonylurea). c. Include patients with cardiovascular disease (except Class III-V CHF). d. Include patients taking diuretics. e. Include patients with stable, treated thyroid disease. 3) Modification of study protocol and consent to reflect collection of DNA during study. Level of review IRB considerations")
124
First renewal Current Status: Open for enrollment and ongoing review of records/specimens. Modifications: Modifications reviewed. Study Summary 2006 attached. Subjects: No Unanticipated Problems (which includes adverse events) reported to date . Level of review? IRB considerations?
 reported to date . Level of review IRB considerations")
125
Fifth modification Revision of inclusion criteria to include youth ages Level of review? IRB considerations?

126
Unanticipated Problem (Adverse Event) Report
Participant was admitted to (facility) for 4 days, from (dates), as per study protocol. Participant completed the study and was discharged from the (facility) during the early afternoon. Approximately one-half hour after discharge, while at a local restaurant the participant began having chest pain which radiated to the back and arm. The participant interpreted the symptoms as being indicative of indigestion and so went home and took bismuth to obtain relief. The symptoms however worsened, so a member of the household called 911, and the participant was taken to (hospital) by ambulance. Results of initial evaluations are forthcoming. The participant underwent cardiac catheterization and coronary artery stenting on (date). The participant was subsequently discharged home in the afternoon on (date) with instructions to follow up as an outpatient with a particular cardiologist. Level of review? IRB considerations?
 for 4 days, from (dates), as per study protocol. Participant completed the study and was discharged from the (facility) during the early afternoon. Approximately one-half hour after discharge, while at a local restaurant the participant began having chest pain which radiated to the back and arm. The participant interpreted the symptoms as being indicative of indigestion and so went home and took bismuth to obtain relief. The symptoms however worsened, so a member of the household called 911, and the participant was taken to (hospital) by ambulance. Results of initial evaluations are forthcoming. The participant underwent cardiac catheterization and coronary artery stenting on (date). The participant was subsequently discharged home in the afternoon on (date) with instructions to follow up as an outpatient with a particular cardiologist. Level of review IRB considerations")
127
Second renewal Current Status: Open for enrollment or ongoing review of records/specimens. Change in Literature noted with references. Oversight Monitoring: 1 Unanticipated Problem (Chest Pain) submitted Level of review? IRB considerations?
 submitted. Level of review IRB considerations")
128
Noncompliance scenario
Dr. PI incorporates data into the study from five of his own patients who were taking Drug A before the protocol was approved. Dr. PI did not seek consent from these patients to enroll in the study. Issues to consider: OHRP Reporting requirements: Industry sponsored study ~ Does the FWA apply to HHS research only, or to all research regardless of funding? What corrective actions might the IRB consider?

129
Third renewal Current status: Closed to enrollment, open for data analysis at main site. Level of review? IRB considerations?

Similar presentations


 is a review committee established to help protect the rights and welfare of human research subjects.>")
>")




 Program Analyst Program for Research Integrity Development and Education.>")

, Informed Consent, and Responsibilities Requirement for IRBs -DHHS: 45 CFR Part 46 -FDA: 21 CFR 56 Requirement for and.>")

, or disapprove all research.>")








