Download presentation
Presentation is loading. Please wait.

1
Alzheimer’s disease: Changing views of Pathophysiology
Gordon Wilcock Professor of Clinical Geratology University of Oxford CoI statement: GW has received research support and honoraria from companies developing Rx for AD and other dementias, and has led or participated in many clinical trials of anti-dementia drugs.

2
Outline of talk This presentation will concentrate on AD, rather than Dementia in general: Where is the amyloid hypothesis taking us? Are Tangle related strategies a therapeutic option? The role of vascular factors The role of systemic inflammation and cytokines

3
Modifying disease processes in AD: Beta amyloid

4
Alzheimer’s Plaques – “Amyloid”

5
Anti-Amyloid Strategies
These include: Preventing amyloid formation Blocking its harmful effects Removing it from the brain

6
Amyloid Precursor Protein Cleavage
b-amyloid peptide b-secretase -secretase -secretase Neuronal plasma membrane Cytoplasm

7
Anti-amyloid strategies Gamma-secretase modulators and inhibitors
Modulation v. inhibition Modulation Tarenflurbil – only secretase compound with completed Phase III data – Trials negative Inhibition – many compounds in development or evaluation Lilly: Semagacestat – Ph 3 Trials halted Aug 2010. Treated group did worse than those on placebo AE’s worse, e.g. skin cancer Bristol-Myers Squibb: BMS – phase 2

8
Activities of Daily Living — ADCS-ADL ITT Analysis – Mild AD
p=0.479 Preliminary analysis 8

9
Anti-amyloid strategies: β-Secretase (BACE-1*) Inhibition
CoMentis Phase I study of CTS-21166 reduced plasma Aβ levels by up to 80% no CSF data Other companies e.g. Merck, Eli Lilly and Co., Takeda (* β-site of APP cleaving enzyme )
")
10
Anti-amyloid strategies Alpha-secretase stimulation
e.g. EHT 0202: Phase IIa in France Inhibitor of cyclic 3'5-nucleotide phosphodiesterase and subtype-selective GABAA receptor modulator stimulates α-secretase pathway. 159 mild/moderate AD; 3 months; 40 & 80 mg doses bd; ChEIs allowed Safe and well tolerated Efficacy: ADAS-cog encouraging ApoE e4 +ve patients responded better (strange!) Moving to Phase IIb for dose finding/efficacy
 Moving to Phase IIb for dose finding/efficacy.")
11
Anti-amyloid strategies Anti-aggregants
Tramiprosate (Alzhemed) trials negative: Binds to soluble Aß, reducing production of fibrillar form Mild to moderate AD Inadequate phase II evaluation US phase III negative and European phase III discontinued PBT2 phase 2 study: Affects Cu and Zn mediated toxic oligomerisation of Aß More promising
 trials negative: Binds to soluble Aß, reducing production of fibrillar form. Mild to moderate AD. Inadequate phase II evaluation. US phase III negative and European phase III discontinued. PBT2 phase 2 study: Affects Cu and Zn mediated toxic oligomerisation of Aß. More promising.")
12
Immunotherapy: Autopsy and clinical findings in the AN1792 trial
8 autopsies from treated group and an aged matched control group of non-immunised AD brains Aß load measured (= % of cortical area with Aß) and scored for specific evidence of plaque removal Aß load was compared with mean antibody response, survival time, and MMSE score before death Plaque removal correlated to some extent with antibody response No clinical benefits observed with plaque clearance This concept still under evaluation, mainly with more specific monoclonal antibodies (Holmes et al 2008)
 and scored for specific evidence of plaque removal. Aß load was compared with mean antibody response, survival time, and MMSE score before death. Plaque removal correlated to some extent with antibody response. No clinical benefits observed with plaque clearance. This concept still under evaluation, mainly with more specific monoclonal antibodies. (Holmes et al 2008)")
13
Evidence of extensive and/or patchy removal of plaques
Unimmunized AD Temporal lobe Immunised Temporal lobe Case 1 Prof. J Nicoll

14
Decreased Clearance of CNS ß-Amyloid in AD
12 late onset AD and 12 control subjects Production/clearance of Aß40 & Aß42 Intravenous 13C6 - Leucine – crosses BBB and labels proteins, then measured in CSF Reported a 30% impairment in clearance rate of both Aß40 & Aß42 Estimates based on this 30% decrease in clearance suggest that brain Aß accumulates over 10 years in AD Controversial at present: No control protein Only 12 subjects CSF not brain measurements Is the mathematical modelling method correct? ? Over-interpreted But if correct, has implications for understanding pathology and therapeutic strategies Mawuenyega et al 2010 Science

15
Future questions: Is “plaque amyloid” harmful?
Is “plaque amyloid” helpful? Is it loss of APP function rather than a gain of pathological function that is important? Do we need to rethink trial design? Do we need a basic rethink e.g. Are tangles a more relevant target? Is there a vascular factor contribution?

16
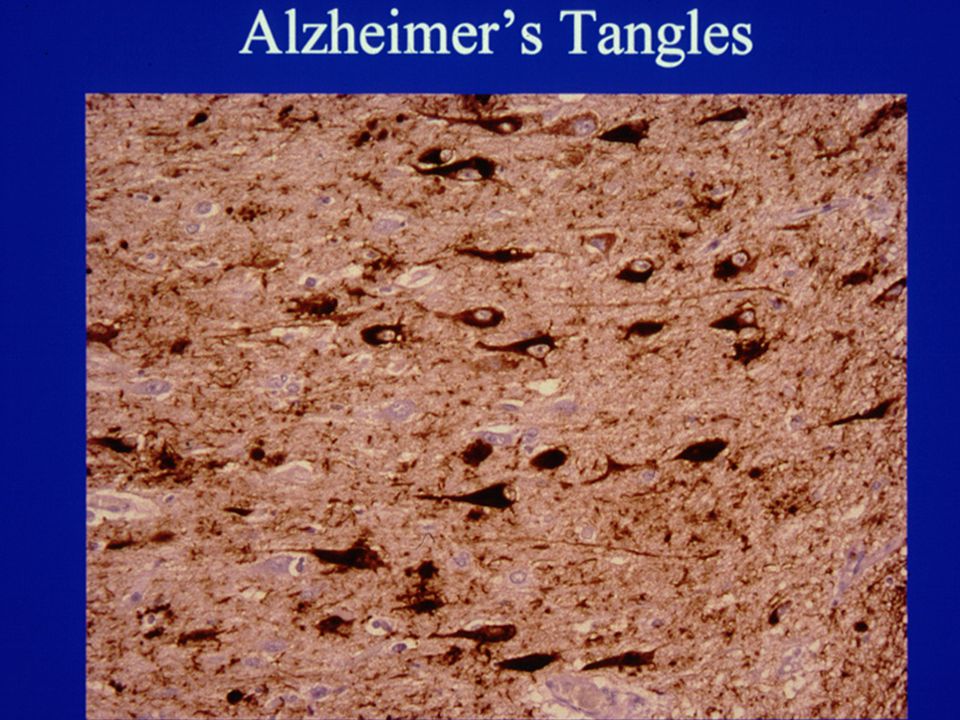
Neurofibrillary Tangle Pathology

18
Neurofibrillary Tangles – Therapeutic Aspects
TAU PHF tau P P P P TAU P NFT HYPER-PHOSPHORYLATION

19
Tau targeted strategies: Methylthioninium (MTC)
Dissolves PHF from AD brain and prevents tau aggregation in cellular models Dose ranging phase 2 RCT in 332 mild/moderate AD At 24 weeks: Mild subjects: no placebo decline, so no analysis Moderate subjects on 60 mg: ADAS-cog score 5.4 points better than placebo At 50 weeks: Mild and moderate AD: -6.8 ADAS cog points cf 7.8 in placebo secondary outcomes also positive Supported by nested SPECT and PET scan data, and further extension to 84 weeks Justifies further evaluation, but limited data published so far (Wischik et al ICAD 2008)
")
20
Vascular Factors and Alzheimer’s disease

21
CVD and cerebral hypo-perfusion as risk factors for AD
Cortical micro-infarcts occur in 32% of people with AD, but only in 2.5% of controls (Suter et al 2002) AD was more likely to develop in a cohort (1015) of non demented yr olds in the presence of silent infarcts (Vermeer et al 2003) “MCI” patients with hypoperfusion (SPECT) in: hippocampal-amygdaloid structures more likely to convert to AD within 3 years cf those with normal perfusion patterns (Johnson & Albert, 2000) Others have reported similarly, e.g. posterior cingulate hypoperfusion (Rodriguez et al 2000)
 AD was more likely to develop in a cohort (1015) of non demented yr olds in the presence of silent infarcts (Vermeer et al 2003) MCI patients with hypoperfusion (SPECT) in: hippocampal-amygdaloid structures more likely to convert to AD within 3 years cf those with normal perfusion patterns (Johnson & Albert, 2000) Others have reported similarly, e.g. posterior cingulate hypoperfusion (Rodriguez et al 2000)")
22
Inflammation and AD

23
The role of systemic inflammation and cytokines (Holmes et al 2009)
Inflammatory markers associated with the pathology of AD A number of pro-inflammatory cytokines have been implicated in the pathogenesis of AD, e.g. by activating microglia 300 community dwelling subjects with mild to severe AD Assessed at 2, 4 and 6 months with ADAS-cog Acute systemic inflammatory events, e.g. infections, surgery, MI, occurred in about 50% Inflammatory events associated with: increased serum TNF-alpha 2 fold increase in rate of cognitive decline over 6 months High baseline TNF–alpha associated with a 4 fold increase in rate of cognitive decline Subjects with low levels of TNF–alpha throughout the study did not decline cognitively Thus both acute and chronic systemic inflammation increased serum TNF-alpha and the rate of cognitive decline

24
Clinical Implications

25
Revised diagnostic criteria for AD - 1 (Dubois et al., 2007)
Diagnosing AD before Dementia onset: Presence of an early and significant episodic memory impairment that includes the following features: Gradual and progressive change in memory function reported by patients or informants over more than 6 months Objective evidence of significantly impaired episodic memory on testing: generally consists of a recall deficit that does not improve significantly or does not normalise with cueing or recognition testing AND other supportive features and exclusion criteria

26
“Biomarkers” to identify those with predementia AD :
Psychometric traditional and computer based Imaging Structural and functional CSF (and Blood based) Abeta 42, tau and phospho-tau, and many others (see review by Hampel et al 2010) (Also needed as outcome measures in trials and clinical practice)
 Abeta 42, tau and phospho-tau, and many others (see review by Hampel et al 2010) (Also needed as outcome measures in trials and clinical practice)")
27
In Conclusion: Traditional views of pathophysiology are under review
Especially the role of Amyloid Tangle pathology now being targeted as a potential therapeutic strategy Newer concepts include: Vascular disease (really an old concept!) Inflammation And others not covered, e.g Cu, Zn, oxidative damage etc This has implications for day to day practice
 Inflammation. And others not covered, e.g Cu, Zn, oxidative damage etc. This has implications for day to day practice.")
Similar presentations












 observations/experiences.>")


>")



