Download presentation
Presentation is loading. Please wait.

1
DISORDERS OF THE THYROID AND PARATHYROID GLANDS

2
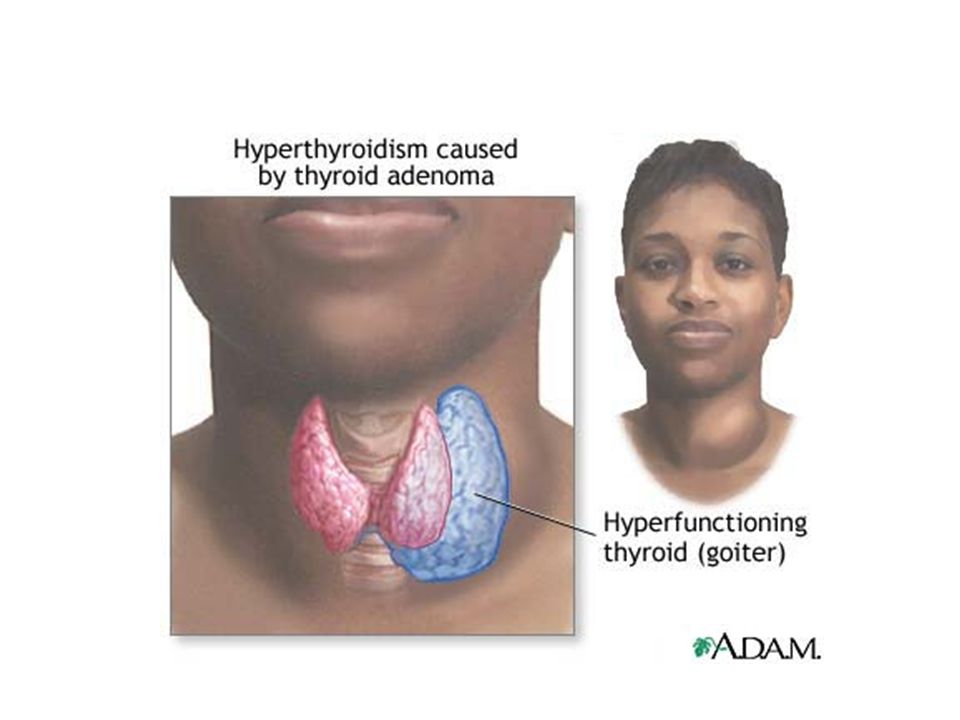
HYPERTHYROIDISM ETIOLOGY/PATHOPHYSIOLOGY
Also called Graves’ disease, or exophthalmic goiter, or thyrotoxicosis DUE TO: Overproduction of the thyroid hormones T3 and T4 Exaggeration of metabolic processes Collective term for a condition marked by increased thyroid activity and overproduction of thyroid hormones thyroxine (T4) and triiodothyronine (T3) Thyroid gland itself may be enlarged Variations are: Graves disease (most common) Parry’s disease Thyrotoxicosis Graves disease generally affects females more than males but tends to affect males more severely Highest incidence in the 20- to 40-year-old group Autoimmune disorder TSIs bind with TSH receptors and abnormally stimulate thyroid functioning
 and triiodothyronine (T3) Thyroid gland itself may be enlarged. Variations are: Graves disease (most common) Parry’s disease. Thyrotoxicosis. Graves disease generally affects females more than males but tends to affect males more severely. Highest incidence in the 20- to 40-year-old group. Autoimmune disorder. TSIs bind with TSH receptors and abnormally stimulate thyroid functioning.")
3
HYPERTHYROIDISM ETIOLOGY/PATHOPHYSIOLOGY cont. Exact cause unknown
Possible genetic factors with precipitive factors of: Infection, ↓ iodine, or extreme physical or emotional stress Affects females more than males May occur during adolesence or pregnancy

4
HYPERTHYROIDISM CLINICAL MANIFESTATIONS:
Edema of the anterior portion of the neck Exophthalmos (bulging eyeballs) SUBJECTIVE ASSESSMENT : Pt. C/o: Inability to concentrate; memory loss Dysphagia Hoarseness Increased appetite Weight loss, insomnia Nervousness, jittery, excitable Manifestations include two obvious physical changes: Thyroid may enlarge 3 to 4 times its normal size (goiter) Accumulation of orbital fluid behind the eyeball forcing protrusion (exophthalmos) Increased thyroid production leads to increased metabolic rate which leads to: Weight loss despite increased appetite Fatigue Poor tolerance to heat Profuse perspiration Client is very nervous leading to: Restlessness Irritability Difficulty concentrating Emotional liability Mood swings Possible personality changes Sleep disturbances Client may have: Fine tremors of the fingers and tongue Shaky handwriting Clumsiness Trouble climbing stairs Dyspnea on exertion and possibly at rest Skin is warm and moist with a velvety texture; may be a characteristic salmon color Hair is fine, soft, prematurely gray; increased hair loss Nails appear fragile with onycholysis May be general or local muscle atrophy and acropachy There is tachycardia (160 beats/minute; down to 80 during sleep); pulse pressure is widened May be muscular weakness and atrophy, osteoporosis, and paralysis May be vitiligo (milky white patches on skin) Decreased libido, impaired fertility, and gynecomastia (abnormal enlargement of one or both breasts in males) Diagnostic tests generally include TSH, T3, T4, radioactive iodine uptake, thyroid scan A major complication is thyrotoxic crisis, also called thyroid storm Medical emergency that can lead to cardiac, hepatic, or renal failure Can be precipitated by stressful situation such as surgery, infection, or trauma Less common causes include cerebrovascular accident, myocardial infarction, etc. Any of these events can lead to overproduction of thyroid hormone causing: Increase in systemic adrenergic activity Overproduction of epinephrine and severe hypermetabolsim leading to: Rapid cardiac, gastrointestinal, and sympathetic nervous system decompensation Severe and rapid manifestations exhibited If nurse suspects thyrotoxic crisis, physician must be informed immediately Client is transferred to ICU; monitored for: Vital signs EKG pattern Cardiopulmonary status Temperature Antithyroid therapy begun immediately
 SUBJECTIVE ASSESSMENT : Pt. C/o: Inability to concentrate; memory loss. Dysphagia. Hoarseness. Increased appetite. Weight loss, insomnia. Nervousness, jittery, excitable. Manifestations include two obvious physical changes: Thyroid may enlarge 3 to 4 times its normal size (goiter) Accumulation of orbital fluid behind the eyeball forcing protrusion (exophthalmos) Increased thyroid production leads to increased metabolic rate which leads to: Weight loss despite increased appetite. Fatigue. Poor tolerance to heat. Profuse perspiration. Client is very nervous leading to: Restlessness. Irritability. Difficulty concentrating. Emotional liability. Mood swings. Possible personality changes. Sleep disturbances. Client may have: Fine tremors of the fingers and tongue. Shaky handwriting. Clumsiness. Trouble climbing stairs. Dyspnea on exertion and possibly at rest. Skin is warm and moist with a velvety texture; may be a characteristic salmon color. Hair is fine, soft, prematurely gray; increased hair loss. Nails appear fragile with onycholysis. May be general or local muscle atrophy and acropachy. There is tachycardia (160 beats/minute; down to 80 during sleep); pulse pressure is widened. May be muscular weakness and atrophy, osteoporosis, and paralysis. May be vitiligo (milky white patches on skin) Decreased libido, impaired fertility, and gynecomastia (abnormal enlargement of one or both breasts in males) Diagnostic tests generally include TSH, T3, T4, radioactive iodine uptake, thyroid scan. A major complication is thyrotoxic crisis, also called thyroid storm. Medical emergency that can lead to cardiac, hepatic, or renal failure. Can be precipitated by stressful situation such as surgery, infection, or trauma. Less common causes include cerebrovascular accident, myocardial infarction, etc. Any of these events can lead to overproduction of thyroid hormone causing: Increase in systemic adrenergic activity. Overproduction of epinephrine and severe hypermetabolsim leading to: Rapid cardiac, gastrointestinal, and sympathetic nervous system decompensation. Severe and rapid manifestations exhibited. If nurse suspects thyrotoxic crisis, physician must be informed immediately. Client is transferred to ICU; monitored for: Vital signs. EKG pattern. Cardiopulmonary status. Temperature. Antithyroid therapy begun immediately.")
5
EXOPTHALMUS Internet picture

6
HYPERTHROIDISM

7
HYPERTHROIDISM CLINICAL MANIFESTATIONS OBJECTIVE ASSESSMENT
Tachycardia; hypertension; bruit over thyroid Warm, flushed skin Fine hair Amenorrhea Elevated temperature/heat intolerance Diaphoresis Hand tremors, clumsiness Hyperactivity for some

8
HYPERTHYROIDISM DIAGNOSTIC TESTS Confirmed by: ↓ TSH and ↑ Free T4
RAIU – radioactive iodine uptake – uptake of 35-95% of the drug

9
HYPERTHYROIDISM Meds reduce symptoms in 6-8 wks.
MEDICAL MANAGEMENT Medications – Block production of thyroid hormone Propylthiouracil / PTU Methimazole/ Tapazole Meds reduce symptoms in 6-8 wks. Goal is to decrease excessive thyroid production; can be a combination of treatment methods First method is to administer antithyroid meds (usually a temporary solution) Radiation therapy Most accepted method is oral administration of radioactive iodine (liquid or capsule) Most commonly used for women past reproductive years or who do not want children If of reproductive age, consent needs to be signed as small amounts could lodge in gonads Antithyroid meds should be stopped 4 to 7 days prior to treatment Inform physician of amiodarone hydrochloride use as it contains large amounts of iodine Oral 131I should not be given to client with severe vomiting or diarrhea This method involves a single dose of 131I orally Destroys some iodine concentrating cells that produce the thyroxine Clinical manifestations decrease in about 3 weeks Effected fully in about 3 months Some may require a second or third dose Safety: Radioactive Iodine No pregnant nurse should care for client Client should expectorate carefully for the first day since saliva is radioactive Drink plenty of fluids for 2 days to help circulate and eliminate iodine Toilet should be flushed at least twice after each use during hospitalization Disposable eating utensils should be used Close contact with children or pregnant women should be avoided for a week afterward Women should avoid pregnancy for 6 months Thyroid hormone antagonist usually resumed 3 to 5 days after 131I therapy until physician determines thyroid to be atrophic (decreased size) Client may continue to take propranolol hydrochloride (Inderal) for tachycardia, tremor, diaphoresis Client requires continued monitoring of thyroid hormone blood levels and physical condition Most common complication is hypothyroidism Occurs about 2 to 4 months after treatment Client placed on thyroid replacement therapy, generally for life Surgical Generally just a portion of the thyroid gland is removed Remaining tissue should provide adequate amounts of hormones A total thyroidectomy may be performed Most expensive option with most risks May be done for respiratory obstruction by a goiter or cancer Lifetime thyroid replacement therapy required Pre-op, client should be given explanations concerning activities after surgery Neck incision with drain May experience sore throat, hoarseness Medications given up to 6 weeks prior to surgery Thyroid function tests and EKG as baseline information prior to surgery Post-op, client placed in high-Fowler’s position to promote venous drainage Client should support head with a hand when moving to prevent strain on incision Respiratory problems may occur Respiratory obstruction can be a result of: Tracheal collapse Tracheal mucous accumulation Laryngeal or local tissue edema Tracheotomy tray or tubes may be kept at bedside in case of emergency Since thyroid so vascular, check drainage frequently Expect about 50 cc of drainage first day If no drainage, check for obstruction of tubing Nurse should encourage voice rest for 48 hours Check voice every 2 to 4 hours to make certain there’s no laryngeal nerve damage Blood calcium levels must be monitored in case of accidental removal of parathyroid glands Analgesics administered as needed Complications of thyroidectomy are: Respiratory distress and hemorrhage Damage to laryngeal nerves affecting voice Thyroid storm (rare) Tetany can occur up to 10 days after surgery: Sharp flexion of wrist and ankle joints Muscle twitchings Cramps (decreased blood calcium) Pharmacological Several drugs may be used for antithyroid therapy Propylthiouracil (PTU) is used frequently, especially for thyroid storm OTC meds must be checked for iodine Avoid foods high in iodine (shellfish, iodized salt) Drugs may be administered up to 2 years May cause agranulocytosis (decreased number of granulocytes) Methimazole (Tapazole) is another preparation; does not have as much consistency in effect Iodine preparations may be given; take effect in 2 days Inderal may be prescribed to counteract tachycardia and peripheral effects of hyperthyroidism Clients should not smoke Abrupt withdrawal can cause hypertension, myocardial ischemia, cardiac arrhythmias Isotonic eye drops may be ordered for exophthalmos Corticosteroids help reduce exophthalmos Antithyroid drugs given during thyrotoxic crisis Diet May require 4,000 to 5,000 calories a day due to greatly increase metabolic rate Need for increased proteins, vitamins, and minerals In addition to 3 meals a day, additional meals or snacks needed Encourage fluids; avoid caffeine Nursing Management Provide high-calorie diet & snacks throughout the day Keep client’s skin dry & clean, change gown & linens as needed Pre Op – Teach client how to support his head while turning or sitting or standing position Inform client that “voice rest” may be enforced for 48 hours and provide paper & pencil for writing notes Post Op – Keep bed in semi-Fowler’s position with head and shoulders supported by pillows Keep suction equipment and tracheotomy tray in client’s room Inspect dressing, sides and back of neck, and shoulders frequently for bleeding Watch for signs of internal bleeding Watch for signs of tetany and for signs of edema in the operative area
 Radiation therapy. Most accepted method is oral administration of radioactive iodine (liquid or capsule) Most commonly used for women past reproductive years or who do not want children. If of reproductive age, consent needs to be signed as small amounts could lodge in gonads. Antithyroid meds should be stopped 4 to 7 days prior to treatment. Inform physician of amiodarone hydrochloride use as it contains large amounts of iodine. Oral 131I should not be given to client with severe vomiting or diarrhea. This method involves a single dose of 131I orally. Destroys some iodine concentrating cells that produce the thyroxine. Clinical manifestations decrease in about 3 weeks. Effected fully in about 3 months. Some may require a second or third dose. Safety: Radioactive Iodine. No pregnant nurse should care for client. Client should expectorate carefully for the first day since saliva is radioactive. Drink plenty of fluids for 2 days to help circulate and eliminate iodine. Toilet should be flushed at least twice after each use during hospitalization. Disposable eating utensils should be used. Close contact with children or pregnant women should be avoided for a week afterward. Women should avoid pregnancy for 6 months. Thyroid hormone antagonist usually resumed 3 to 5 days after 131I therapy until physician determines thyroid to be atrophic (decreased size) Client may continue to take propranolol hydrochloride (Inderal) for tachycardia, tremor, diaphoresis. Client requires continued monitoring of thyroid hormone blood levels and physical condition. Most common complication is hypothyroidism. Occurs about 2 to 4 months after treatment. Client placed on thyroid replacement therapy, generally for life. Surgical. Generally just a portion of the thyroid gland is removed. Remaining tissue should provide adequate amounts of hormones. A total thyroidectomy may be performed. Most expensive option with most risks. May be done for respiratory obstruction by a goiter or cancer. Lifetime thyroid replacement therapy required. Pre-op, client should be given explanations concerning activities after surgery. Neck incision with drain. May experience sore throat, hoarseness. Medications given up to 6 weeks prior to surgery. Thyroid function tests and EKG as baseline information prior to surgery. Post-op, client placed in high-Fowler’s position to promote venous drainage. Client should support head with a hand when moving to prevent strain on incision. Respiratory problems may occur. Respiratory obstruction can be a result of: Tracheal collapse. Tracheal mucous accumulation. Laryngeal or local tissue edema. Tracheotomy tray or tubes may be kept at bedside in case of emergency. Since thyroid so vascular, check drainage frequently. Expect about 50 cc of drainage first day. If no drainage, check for obstruction of tubing. Nurse should encourage voice rest for 48 hours. Check voice every 2 to 4 hours to make certain there’s no laryngeal nerve damage. Blood calcium levels must be monitored in case of accidental removal of parathyroid glands. Analgesics administered as needed. Complications of thyroidectomy are: Respiratory distress and hemorrhage. Damage to laryngeal nerves affecting voice. Thyroid storm (rare) Tetany can occur up to 10 days after surgery: Sharp flexion of wrist and ankle joints. Muscle twitchings. Cramps (decreased blood calcium) Pharmacological. Several drugs may be used for antithyroid therapy. Propylthiouracil (PTU) is used frequently, especially for thyroid storm. OTC meds must be checked for iodine. Avoid foods high in iodine (shellfish, iodized salt) Drugs may be administered up to 2 years. May cause agranulocytosis (decreased number of granulocytes) Methimazole (Tapazole) is another preparation; does not have as much consistency in effect. Iodine preparations may be given; take effect in 2 days. Inderal may be prescribed to counteract tachycardia and peripheral effects of hyperthyroidism. Clients should not smoke. Abrupt withdrawal can cause hypertension, myocardial ischemia, cardiac arrhythmias. Isotonic eye drops may be ordered for exophthalmos. Corticosteroids help reduce exophthalmos. Antithyroid drugs given during thyrotoxic crisis. Diet. May require 4,000 to 5,000 calories a day due to greatly increase metabolic rate. Need for increased proteins, vitamins, and minerals. In addition to 3 meals a day, additional meals or snacks needed. Encourage fluids; avoid caffeine. Nursing Management. Provide high-calorie diet & snacks throughout the day. Keep client’s skin dry & clean, change gown & linens as needed. Pre Op – Teach client how to support his head while turning or sitting or standing position. Inform client that voice rest may be enforced for 48 hours and provide paper & pencil for writing notes. Post Op – Keep bed in semi-Fowler’s position with head and shoulders supported by pillows. Keep suction equipment and tracheotomy tray in client’s room. Inspect dressing, sides and back of neck, and shoulders frequently for bleeding. Watch for signs of internal bleeding. Watch for signs of tetany and for signs of edema in the operative area.")
10
HYPERTHYROIDISM Radioactive iodine/ ablation therapy
MEDICAL MANAGEMENT Medication may be followed by: Radioactive iodine/ ablation therapy Destroys some of the hypertrophied thyroid tissue Low dose – no “radiation” precautions needed

11
HYPERTHYROIDISM MEDICAL MANAGEMENT cont.
Radioactive iodine/ Ablation therapy cont. Outcome: in most pts. hypothyroidism treat with Levothyroxine Adequate medical supervision follow up is important!

12
HYPERTHYROIDISM MEDICAL MANAGEMENT cont.
Surgery: for pts. who cannot tolerate antithyroid drugs; are not good candidates for radiation tx.; have a poss. malignancy; or have large goiters causing tracheal compression Most common surgery: Subtotal Thyroidectomy Removal of 5/6ths of the thyroid gland If too much thyroid tissue is removed gland will not regenerate hypothyroidism

13
HYPERTHYROIDISM MEDICAL MANAGEMENT cont.
Surgery: usually delayed until pt in a normal thyroid state d/t the risk of bleeding during surgery and thyroid crisis (thyroid storm) post op.
 post op.")
15
HYPERTHYROIDISM NURSING ASSESSMENT AND INTERVENTIONS:
Post-operative Subtotal Thyroidectomy Assess for s/sx internal or external bleeding Assess for tetany: Chovstek’s Sign: is + when abnormal spasm of facial muscles occurs when elicited by light tapping on facial nerve in the pt. with low calcium Trousseau’s Sign: is + if there is carpal spasm in the hypocalcemic and hypomagnesemia pt. When BP cuff inflated above pt. normal systolic pressure and held there for 3 min. (3 min 5 sec) (9 min 49sec)
 q=youtube+partial+thyroidectomy+personal+story&FORM=VIRE1#view=detail&mid=613D00F1A54228D D00F1A54228D31139 (9 min 49sec)")
16
HYPERTHYROIDISM NURSING ASSESSMENT AND INTERVENTIONS:
Post-op Subtotal Thyroidectomy (cont.) Assess for Thyroid Crisis/Storm May occur as a result of manipulation of the thyroid gland during surgery releasing large amts of thyroid hormone bloodstream Occurs within the first 12 hrs. S/SX: exaggerated s/sx of hyperthyroidism + n/v, severe tachycardia, severe HTN, severe hyperthermia (106F+), extreme restlessness, dysrhythmias, delirium, heart failure death min 38 sec)Thyroid Storm part 1 (5 min 47 sec) Thyroid Storm part 2
 Assess for Thyroid Crisis/Storm. May occur as a result of manipulation of the thyroid gland during surgery releasing large amts of thyroid hormone bloodstream. Occurs within the first 12 hrs. S/SX: exaggerated s/sx of hyperthyroidism + n/v, severe tachycardia, severe HTN, severe hyperthermia (106F+), extreme restlessness, dysrhythmias, delirium, heart failure death. q=thyroid+storm&FORM=HDRSC3#view=detail&mid=8A8572C304A26127A35A8A8572C304A26127A35A(5 min 38 sec)Thyroid Storm part 1. q=thyroid+storm&FORM=HDRSC3#view=detail&mid=CEB5AB156B2998E95407CEB5AB156B2998E95407 (5 min 47 sec) Thyroid Storm part 2.")
17
HYPERTHYROIDISM Thyroid Storm cont.: DIAGNOSTIC TESTS ↑FT4, ↓TSH
MEDICAL MANAGEMENT goals during thyroid storm: 1. induce a normal thyroid state 2. prevent cardio-vascular collapse 3. prevent ↑ hyperthermia

18
HYPERTHYROIDISM NURSING ASSESSMENT AND INTERVENTIONS:
Post-op Subtotal Thyroidectomy (cont.) Voice rest x48 hrs – provide communication tool Voice checks – q 2-4 hrs. “ahh”; note hoarseness or other changes Bed – semifowler’s position; pillow support for head and shoulders
 Voice rest x48 hrs – provide communication tool. Voice checks – q 2-4 hrs. ahh ; note hoarseness or other changes. Bed – semifowler’s position; pillow support for head and shoulders.")
19
HYPERTHYROIDISM NURSING ASSESSMENT AND INTERVENTIONS:
Post-op Subtotal Thyroidectomy (cont.) Avoid hyperextension of neck; support head during position change Reinforce DB exercises; check with MD re: coughing Tracheotomy tray at bedside and suction Cool mist humidifier prn Nutrition care – watch for dysphagia
 Avoid hyperextension of neck; support head during position change. Reinforce DB exercises; check with MD re: coughing. Tracheotomy tray at bedside and suction. Cool mist humidifier prn. Nutrition care – watch for dysphagia.")
20
HYPERTHYROIDISM NURSING DIAGNOSES: Pre-op
Risk for hyperthermia, related to increased metabolism Imbalanced nutrition:less than body requirements r/t increased metabolism Post-op Impaired swallowing, r/t edema Ineffective breathing,risk for, r/t post-op edema and pain

21
HYPERTHYROIDISM PATIENT EDUCATION
Post op: follow up with medical supervision Thyroid function tests Care incision site Diet: high calorie, CHO’s , and protein PROGNOSIS: normal life with appropriate medical or surgical tx. Expophthalmos may remain to lesser degree

22
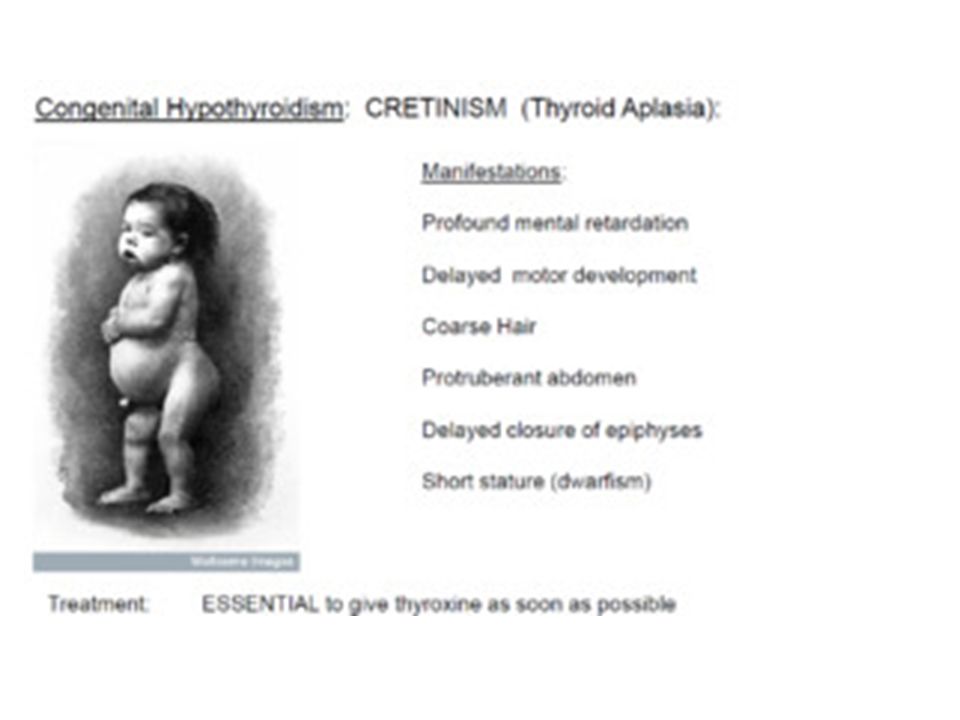
HYPOTHYROIDISM Etiology/pathophysiology
Due to insufficient secretion of thyroid hormones Decreased hormones cause slowing of all metabolic processes R/T Failure of thyroid or insufficient secretion of thyroid-stimulating hormone from pituitary gland Hashimoto talks: (Just to be funny-hehe) Personal Story (5 minutes) Metabolic processes decreased because of deficient thyroid hormone Termed primary if solely a dysfunction of the thyroid Secondary if gland not stimulated to produce normally or if target cells fail to respond More common in females than males Significant increase in incidence between 30 to 60 CRETINISM Congenital condition due to lack of thyroid hormones Causes defective physical development and retardation Occurs in about 1 of 3,000 live births Rare in the U.S. and tested by T4 MYXEDEMA Severe hypothyroidism in adults Variety of abnormalities lead to decreased hormone production including: Surgery or irradiation Hashimoto’s thyroiditis (chronic autoimmune) Inflammatory conditions
 q=youtube+hashimoto&qpvt=youtube+hashimoto&FORM=VDRE#view=detail&mid=BC6F61D1587C BC6F61D1587C Personal Story (5 minutes) q=youtube+hashimoto&qpvt=youtube+hashimoto&FORM=VDRE#view=detail&mid=0A19B271B C210A19B271B C21. Metabolic processes decreased because of deficient thyroid hormone. Termed primary if solely a dysfunction of the thyroid. Secondary if gland not stimulated to produce normally or if target cells fail to respond. More common in females than males. Significant increase in incidence between 30 to 60. CRETINISM. Congenital condition due to lack of thyroid hormones. Causes defective physical development and retardation. Occurs in about 1 of 3,000 live births. Rare in the U.S. and tested by T4. MYXEDEMA. Severe hypothyroidism in adults. Variety of abnormalities lead to decreased hormone production including: Surgery or irradiation. Hashimoto’s thyroiditis (chronic autoimmune) Inflammatory conditions.")
23
HYPOTHYROIDISM Myxedema refers to severe hypothyroidism in adults
Will see edema in hand’s face, feet, and periorbital tissues Inflammation and thickening of the skin Cretinism – congenital hypothyroidism Floppy infant Thick,protruding tongue Poor feeding Choking episodes Constipation Prolonged jaundice Short stature Depression Loss of hair Rough voices Swollen eyelids Hearing problem Fatigue Weight gain Clinical manifestations are vague and varied Develop slowly over a period of time; primarily related to reduced metabolic rate

25
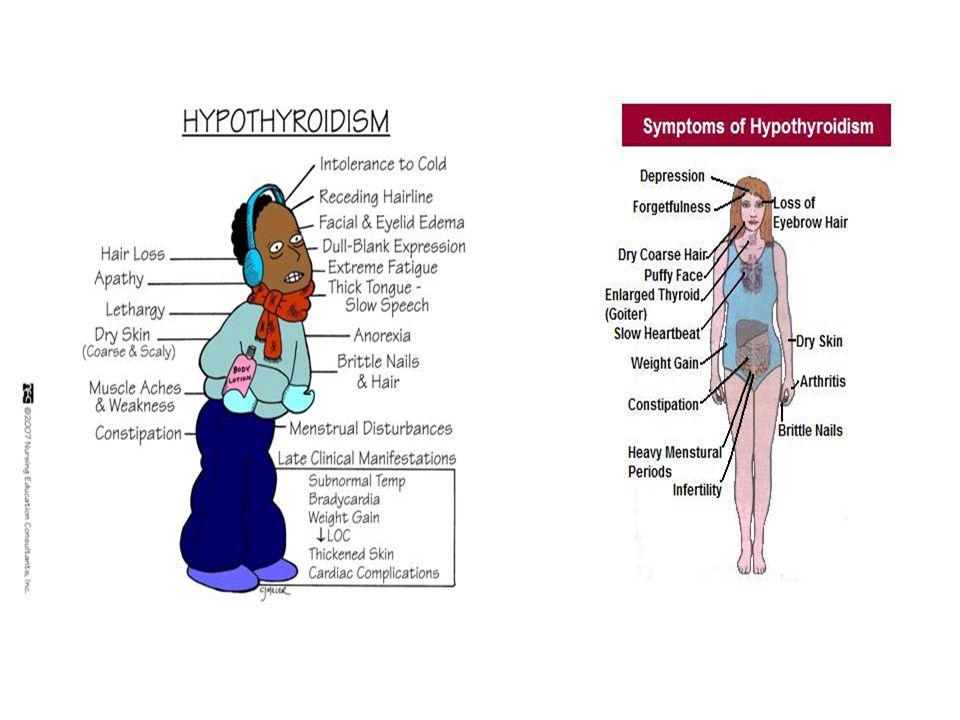
HYPOTHYROIDISM Clinical Manifestations:
Because all metabolism processes slow Hypothermia; intolerance to cold Weight gain ASHD/CAD ↓exercise tolerance + dyspnea on exertion

26
HYPOTHYROIDISM SUBJECTIVE ASSESSMENT:
Mental and emotional assessment may include: Depression; paranoia Impaired memory; slow thought process Hearing/speech impairment Lethargic, forgetful, irritable Anorexia Constipation Cold intolerance Decreased libido; reproductive difficulties

27
HYPOTHYROIDISM OBJECTIVE ASSESSMENT Menstrual irregularities
Thin hair, falls out Skin thick and dry Enlarged facial appearance Low, hoarse voice Bradycardia Hypotension Weakness, clumsiness, ataxia Diagnostic tests generally include TSH, T3, T4, radioactive iodine uptake, thyroid scan Complications effect almost every system including cardiovascular, gastrointestinal, sensorineural, psychiatric, etc. Myxedema coma or hypothyroid crisis is a serious complication; life threatening; characterized by: Severe metabolic disorders Hypothermia Cardiovascular collapse leading to coma Gradual onset but triggered by severe stress (infection, exposure to cold, trauma) Can be caused by withdrawal of thyroid meds or use of narcotics, sedatives, or anesthetics Must be reported to physician immediately Client moved to ICU and monitored closely Often fatal
 Can be caused by withdrawal of thyroid meds or use of narcotics, sedatives, or anesthetics. Must be reported to physician immediately. Client moved to ICU and monitored closely. Often fatal.")
29
HYPOTHYROIDISM Diagnostic tests : TSH, T3, T4, FT4 (low levels of these are the underlying stimuli for TSH) For hypothyroidism: expect ↑TSH (compensatory); ↓T3, T4, and FT4 Thyroid replacement therapy lasts a lifetime Thyroid (Armour Thyroid) is a natural form Levothyroxine sodium (Levothroid, Sythroid) is synthetic Thyroid hormone begins slowly with dosage increased every 2 to 3 weeks until desired response achieved Given in the morning to prevent insomnia Dosage adjusted for diabetics; blood sugar must be closely monitored Anticoagulant therapy and digitalis preparations potentiated by thyroid hormone Due to impaired metabolic rate, may be difficulty in metabolizing meds Other drugs may impair synthesis of thyroid hormone Diet Avoid foods high in iodine or that interfere with treatment: Dried kelp Shellfish Iodized salt Saltwater fish Cabbage Turnips Pears and peaches High-fiber, high-protein, low-calorie diet is given Decrease sodium to prevent fluid retention Dietary consultation for meal planning and a list of foods to avoid should be provided to client Nursing Management Prevent client fatigue by providing rest periods between activities Provide high-fiber diet, encourage intake of oral fluids Administer stool softener, bulk laxative, or enema as ordered HASHIMOTO’S THYROIDITIS Autoimmune disease characterized by production of antiperoxidase antibodies which destroy an essential enzyme necessary for production of T3 and T4 Occurs more often in females, between 30 and 50 Shows a marked hereditary pattern Increased incidence with Down and Turner syndromes Clinical manifestations include: Enlarged thyroid with lumpy surface Goiter is asymptomatic but could cause dysphagia and feeling of local pressure Thymus gland also enlarged Other manifestations similar to hypothyroidism Thyroid hormone replacement therapy is the treatment Chronic disorder, incurable; lifetime therapy
; ↓T3, T4, and FT4. Thyroid replacement therapy lasts a lifetime. Thyroid (Armour Thyroid) is a natural form. Levothyroxine sodium (Levothroid, Sythroid) is synthetic. Thyroid hormone begins slowly with dosage increased every 2 to 3 weeks until desired response achieved. Given in the morning to prevent insomnia. Dosage adjusted for diabetics; blood sugar must be closely monitored. Anticoagulant therapy and digitalis preparations potentiated by thyroid hormone. Due to impaired metabolic rate, may be difficulty in metabolizing meds. Other drugs may impair synthesis of thyroid hormone. Diet. Avoid foods high in iodine or that interfere with treatment: Dried kelp. Shellfish. Iodized salt. Saltwater fish. Cabbage. Turnips. Pears and peaches. High-fiber, high-protein, low-calorie diet is given. Decrease sodium to prevent fluid retention. Dietary consultation for meal planning and a list of foods to avoid should be provided to client. Nursing Management. Prevent client fatigue by providing rest periods between activities. Provide high-fiber diet, encourage intake of oral fluids. Administer stool softener, bulk laxative, or enema as ordered. HASHIMOTO’S THYROIDITIS. Autoimmune disease characterized by production of antiperoxidase antibodies which destroy an essential enzyme necessary for production of T3 and T4. Occurs more often in females, between 30 and 50. Shows a marked hereditary pattern. Increased incidence with Down and Turner syndromes. Clinical manifestations include: Enlarged thyroid with lumpy surface. Goiter is asymptomatic but could cause dysphagia and feeling of local pressure. Thymus gland also enlarged. Other manifestations similar to hypothyroidism. Thyroid hormone replacement therapy is the treatment. Chronic disorder, incurable; lifetime therapy.")
30
HYPOTHYROIDISM MEDICAL MANAGEMENT
Medications: replacement therapy; titration needed Synthroid Levothyroid Proloid Cytomel Symptomatic treatment

31
HYPOTHYROIDISM NURSING INTERVENTION/PT. TEACHING:
For the hospitalized pt. with severe hypothyroidism focus on symptom relief Watch for s/sx hyperthyroidism while adjusting doses of replacement medication Watch for chest pain or dyspnea Keep room 70-74⁰F Avoid the pt. getting chilled BM monitor/protocol

32
HYPOTHYROIDISM NURSING INTERVENTIONS/PT. TEACHING cont.
Diet : ↑protein, fiber, fluid ↓ calories Adequate iodine intake Instruct pt. to take med daily and not to stop without consulting his MD Instruct pt./family – to anticipate clearing of mental slowness as pt. adjusts to dose of med

33
HYPOTHYROIDISM NURSING DIAGNOSES:
Decreased cardiac output r/t decreased metabolism Constipation r/t decreased peristalsis Risk for noncompliance r/t therapy Risk for disturbed body image, r/t altered physical appearance (goiter)
")
34
HYPOTHYROIDISM PROGNOSIS: Pt. will do well with medication and medical supervision. In children, if the T4 replacement begins before the epiphyseal fusion, chance for normal growth is greatly improved (Hypo/hyper/goiter symptoms & treatment 4 min 3 sec)
")
35
SIMPLE (COLLOID) GOITER
ETIOLOGY/PATHOPHYSIOLOGY Enlarged thyroid due to low iodine levels or the gland’s inability to use the iodine properly Enlargement is caused by the accumulation of colloid in the thyroid follicles When blood level of T3 is too low to signal the pituitary gland to reduce TSH secretion, the thyroid gland responds by increased formation of thyroid globulin (colloid) accumulates in the thyroid follicles gland enlargement Usually caused by insufficient dietary intake of iodine overgrowth of thyroid tissue Enlargement of thyroid unrelated to inflammation or neoplasm Three types of goiter: Diffuse toxic goiter found in hyperthyroidism Can be moderate or massively enlarged Varies from soft to firm and rubbery; generally feels smooth Frequently associated with exophthalmos Simple nontoxic goiter develops when thyroid is unable to utilize iodine properly or in response to a low iodine level in the blood More common in females Develop during times of great metabolic demands such as adolescence or pregnancy Large goiter can compress the esophagus or trachea causing dysphagia Dizziness and syncope may occur if goiter impairs venous return from head and neck Diagnosis based on history, clinical manifestations, results of thyroid tests Treatment concentrates on cause Thyroid hormone replacement therapy Iodine supplements Surgery when respiration or swallowing impaired or for cosmetic effect Third type is nodular goiter Palpation reveals multiple nodules causing the enlargement Frequent in females over 40 Usually asymptomatic Treatment varies with age and manifestations
 accumulates in the thyroid follicles gland enlargement. Usually caused by insufficient dietary intake of iodine overgrowth of thyroid tissue. Enlargement of thyroid unrelated to inflammation or neoplasm. Three types of goiter: Diffuse toxic goiter found in hyperthyroidism. Can be moderate or massively enlarged. Varies from soft to firm and rubbery; generally feels smooth. Frequently associated with exophthalmos. Simple nontoxic goiter develops when thyroid is unable to utilize iodine properly or in response to a low iodine level in the blood. More common in females. Develop during times of great metabolic demands such as adolescence or pregnancy. Large goiter can compress the esophagus or trachea causing dysphagia. Dizziness and syncope may occur if goiter impairs venous return from head and neck. Diagnosis based on history, clinical manifestations, results of thyroid tests. Treatment concentrates on cause. Thyroid hormone replacement therapy. Iodine supplements. Surgery when respiration or swallowing impaired or for cosmetic effect. Third type is nodular goiter. Palpation reveals multiple nodules causing the enlargement. Frequent in females over 40. Usually asymptomatic. Treatment varies with age and manifestations.")
36
GOITER

37
SIMPLE (COLLOID) GOITER
CLINICAL MANIFESTATIONS/ASSESSMENT Assessment based on physical manifestations: SUBJECTIVE ASSESSMENT: Enlargement of the thyroid gland Pt. emotional response to the enlargement Interview to determine pt. need for medication, diet, and medical follow up May c/o: Dysphagia, Hoarseness. Dyspnea

38
SIMPLE (COLLOID) GOITER
CLINICAL MANIFESTATIONS/assessment OBJECTIVE DATA: Assess increase of goiter Voice changes Adequate food/fluid intake MEDICAL MANAGEMENT Potassium iodide Diet high in iodine Surgery—thyroidectomy

39
SIMPLE (COLLOID) GOITER
NURSING INTERVENTIONS/GOALS Post Thyroidectomy: prevent complications such as bleeding, tetany, and thyroid crisis Interventions: (discussed previously) NSG. DIAGNOSES Risk for non-compliance with therapeutic regimen Risk for disturbed body image r/t physical appearance
 NSG. DIAGNOSES. Risk for non-compliance with therapeutic regimen. Risk for disturbed body image r/t physical appearance.")
40
Figure 51-10 Simple goiter.

41
Thyroid Cancer ETIOLOGY/PATHOPHYSIOLOGY CLINICAL MANIFESTATIONS
Malignancy of thyroid tissue; rare About 75% are papillary well-differentiated adeno carcinoma- grows slowly, usually contained, doesn’t spread beyond adjacent lymph nodes; cure rates are excellent. CLINICAL MANIFESTATIONS Firm, fixed, small, rounded mass or nodule on thyroid Benign thyroid cyst and adenoma are firm, encapsulated, noninvasive, slowly growing neoplasms of unknown etiology Diagnosis done by needle biopsy Growths do not affect thyroid function (non-functioning) so no treatment other than continued monitoring Functioning adenoma is treated by radioactive iodine or surgery CANCER OF THE THYROID Rare and occurs in all age groups Susceptible with radiation therapy to the neck Four major types: Papillary carcinoma is most common. More common in females of childbearing age Well-differentiated, grows slowly Usually contained; does not spread beyond adjacent lymph nodes Cure rate after thyroidectomy is excellent Follicular carcinoma metastasizes to regional lymph nodes and spreads through blood vessels to: Bone, liver, lungs Very low cure rate Medullary carcinoma is a solid carcinoma associated with pheochromocytoma Curable if detected before signs and symptoms occur Without treatment, metastasizes quickly to bones, liver, kidneys Anaplastic or undifferentiated carcinoma resists radiation Almost never curable by resection Metastasizes rapidly Generally causes death by invasion of the trachea and adjacent structures Generally affects those over 60 Several risk factors: Radiation exposure Prolonged secretion of TSH from radiation or heredity Familial disposition Chronic goiter First clinical manifestation is a painless lump It enlarges destroying the thyroid leading to manifestations of hypothyroidism Although rare, tumor could cause excessive thyroid hormone production Thyroid scan shows “cold” nodule (decreased uptake of 131I) for papillary carcinoma Follicular carcinoma and benign adenomas show a “hot” nodule Thyroid function tests are usually normal Needle biopsy may be done to confirm diagnosis Medical-Surgical Management Surgical All carcinomas can be treated with surgery Radioactive iodine or external radiation therapy may also be used Response depends on early diagnosis and treatment Treatment may be used individually or in combination Client care is the same as for hyperthyroidism Pharmacological Exogenous thyroid hormone may suppress thyroid activity To increase tolerance to surgery, simultaneous exogenous thyroid hormone and adrenergic blocker may be prescribed With widespread metastasis, cancers will be treated with neoplastic chemotherapy Nursing Management Nurse will: Monitor client’s level of anxiety Encourage discussion of feelings about diagnosis and possible surgery Assist in identifying previously successful coping methods Teach new coping methods if needed
 so no treatment other than continued monitoring. Functioning adenoma is treated by radioactive iodine or surgery. CANCER OF THE THYROID. Rare and occurs in all age groups. Susceptible with radiation therapy to the neck. Four major types: Papillary carcinoma is most common. More common in females of childbearing age. Well-differentiated, grows slowly. Usually contained; does not spread beyond adjacent lymph nodes. Cure rate after thyroidectomy is excellent. Follicular carcinoma metastasizes to regional lymph nodes and spreads through blood vessels to: Bone, liver, lungs. Very low cure rate. Medullary carcinoma is a solid carcinoma associated with pheochromocytoma. Curable if detected before signs and symptoms occur. Without treatment, metastasizes quickly to bones, liver, kidneys. Anaplastic or undifferentiated carcinoma resists radiation. Almost never curable by resection. Metastasizes rapidly. Generally causes death by invasion of the trachea and adjacent structures. Generally affects those over 60. Several risk factors: Radiation exposure. Prolonged secretion of TSH from radiation or heredity. Familial disposition. Chronic goiter. First clinical manifestation is a painless lump. It enlarges destroying the thyroid leading to manifestations of hypothyroidism. Although rare, tumor could cause excessive thyroid hormone production. Thyroid scan shows cold nodule (decreased uptake of 131I) for papillary carcinoma. Follicular carcinoma and benign adenomas show a hot nodule. Thyroid function tests are usually normal. Needle biopsy may be done to confirm diagnosis. Medical-Surgical Management. Surgical. All carcinomas can be treated with surgery. Radioactive iodine or external radiation therapy may also be used. Response depends on early diagnosis and treatment. Treatment may be used individually or in combination. Client care is the same as for hyperthyroidism. Pharmacological. Exogenous thyroid hormone may suppress thyroid activity. To increase tolerance to surgery, simultaneous exogenous thyroid hormone and adrenergic blocker may be prescribed. With widespread metastasis, cancers will be treated with neoplastic chemotherapy. Nursing Management. Nurse will: Monitor client’s level of anxiety. Encourage discussion of feelings about diagnosis and possible surgery. Assist in identifying previously successful coping methods. Teach new coping methods if needed.")
42
CANCER OF THYROID

43
Thyroid Cancer Assessment SUBJECTIVE ASSESSMENT OBJECTIVE ASSESSMENT
Pt. coping method and support system Pt. understanding of importance of medical follow up OBJECTIVE ASSESSMENT Progressive enlargement of tumor area Response to 131I tx. Skin care post radiation

44
Thyroid Cancer DIAGNOSTIC TESTS: MEDICAL MANAGEMENT Thyroid scan
Thyroid function tests Needle bx. MEDICAL MANAGEMENT Total thyroidectomy Thyroid hormone replacement If metastasis is present: radical neck dissection; radiation, chemotherapy, and radioactive iodine

45
CANCER OF THE THYROID

46
CANCER OF THE THYROID

47
Thyroid Cancer NURSING INTERVENTIONS/Pt. TEACHING
Per thyroidectomy (previously discusses) Post op: Risk for respiratory distress Risk for laryngeal damage Bleeding S/sx hypothyroidism
 Post op: Risk for respiratory distress. Risk for laryngeal damage. Bleeding. S/sx hypothyroidism.")
48
Thyroid Cancer NURSING DX. Pt. Teaching:
Anxiety r/t situational crisis Ineffective coping r/t personal vulnerability in a crisis Pt. Teaching: Proper medical follow up Monitor thyroid replacement therapy Proper care of surgical incision

49
PARATHYROID GLANDS Website written information resource for students:

50
HYPERPARATHYROIDISM ETIOLOGY/PATHOPHYSIOLOGY
ETIOLOGY/PATHOPHYSIOLOGY Overactivity of the parathyroid glands, with increased production of parathyroid hormone (PTH) Hypertrophy of one or more of the parathyroid glands (usually in the form of an adenoma) Also from: CRF, Pyelonephritis, glomerulonephritis Overactivity of one or more of the parathyroid glands Results in increased secretion of parathyroid hormone (PTH) causing calcium to leave bones and accumulate in blood Occurs twice as often in postmenopausal females than males Occurs frequently between ages of 35 and 65 Hypercalcemia may occur from excessive intake of thiazide diuretics, vitamin D, or calcium supplements X-rays show skeletal decalcification Blood PTH and alkaline phosphate levels increased Serum calcium level elevated Termed primary if enlargement of one or more glands increase secretion of PTH (increases blood calcium) Most common cause is adenoma Other causes include genetics or multiple endocrine neoplasms Termed secondary if excess compensatory production of PTH Stems from hypocalcemia-producing abnormality other than parathyroid gland including: Rickets Chronic renal failure Vitamin D deficiency Osteomalacia due to laxative abuse or phenytoin (Dilantin) Many are asymptomatic; however there are several clinical manifestation: Polyuria Chronic low back pain Bone tenderness Renal calculi May also experience nausea, vomiting, anorexia, constipation, lethargy, drowsiness Changes in level of consciousness Disorientation Stupor Coma Personality changes Loss of initiative and memory Marked muscle weakness and atrophy, etc. Without treatment there can be permanent damage to skeleton or kidneys There can be bone and articular problems Renal complications Stone formations in various organs Cardiac or vascular problems CNS changes
 Hypertrophy of one or more of the parathyroid glands (usually in the form of an adenoma) Also from: CRF, Pyelonephritis, glomerulonephritis. Overactivity of one or more of the parathyroid glands. Results in increased secretion of parathyroid hormone (PTH) causing calcium to leave bones and accumulate in blood. Occurs twice as often in postmenopausal females than males. Occurs frequently between ages of 35 and 65. Hypercalcemia may occur from excessive intake of thiazide diuretics, vitamin D, or calcium supplements. X-rays show skeletal decalcification. Blood PTH and alkaline phosphate levels increased. Serum calcium level elevated. Termed primary if enlargement of one or more glands increase secretion of PTH (increases blood calcium) Most common cause is adenoma. Other causes include genetics or multiple endocrine neoplasms. Termed secondary if excess compensatory production of PTH. Stems from hypocalcemia-producing abnormality other than parathyroid gland including: Rickets. Chronic renal failure. Vitamin D deficiency. Osteomalacia due to laxative abuse or phenytoin (Dilantin) Many are asymptomatic; however there are several clinical manifestation: Polyuria. Chronic low back pain. Bone tenderness. Renal calculi. May also experience nausea, vomiting, anorexia, constipation, lethargy, drowsiness. Changes in level of consciousness. Disorientation. Stupor. Coma. Personality changes. Loss of initiative and memory. Marked muscle weakness and atrophy, etc. Without treatment there can be permanent damage to skeleton or kidneys. There can be bone and articular problems. Renal complications. Stone formations in various organs. Cardiac or vascular problems. CNS changes.")
52
HYPERPARATHYROIDISM CLINICAL MANIFESTATIONS
Hypercalcemia – primary clinical manifestation Calcium leaves the bone serum calcium increases Bones become demineralized formation of renal calculi, pathological fx. Skeletal pain; pain on weight-bearing

53
HYPERPARATHYROIDISM SUBJECTIVE ASSESSMENT
As a result of neuromuscular dysfunction, pts. c/o: Fatigue, drowsiness nausea, anorexia; severe skeletal pain, muscle weakness constipation personality changes, disorientation

54
HYPERPARATHYROIDISM OBJECTIVE ASSESSMENT Skilled observation for:
Skeletal deformity Abnormal movement Urine results Vomiting, weight loss HTN Cardiac dysfunction Bradycardia ↓ LOC

55
HYPERPARATHYROIDISM DIAGNOSTIC TESTS RADIOGRAPHS/XRAYS
PTH blood level (usually ↑) Ca++ levels Bone Density measurements MRI, CT, and US to localize an adenoma
 Ca++ levels. Bone Density measurements. MRI, CT, and US to localize an adenoma.")
58
Hyperparathyroidism

59
HYPERPARATHYROIDISM MEDICAL MANAGEMENT
Removal of tumor Removal of one or more parathyroid glands Autotransplantation NURSING INTERVENTIONS/Pt. TEACHING Assess for hypercalcemia Restore fluid and electrolyte imbalance Diet: low in calcium Medical Management aimed at decreasing overactivity of parathyroid glands Accomplished by med therapy or surgery If severe renal involvement, dialysis may be required Surgical Primary type can be treated by surgical removal of three and one half of the four parathyroid glands Can relieve bone pain but may not reverse renal damage Pre-op care includes: Explanations Encouraging fluids Limiting calcium intake Administering meds to lower blood calcium Post-op care involves administration of magnesium or phosphate Client may receive calcium supplements for several days Nursing care is similar to thyroidectomy Major complication is airway obstruction Pharmacological Aimed toward correcting secondary hyperparathyroidism Meds geared to decreasing calcium level in blood Includes use of diuretics such as furosemide (Lasix) and ethacrynic acid (Edecrin) Phosphate-based drugs lower calcium level Nursing Management Pre Op – Encourage oral fluid intake Strain urine for calculi Offer cranberry juice to acidify the urine Post Op – Assess for signs of hypocalcemia Teach client principles of good body mechanics Reassure client that bone pain will gradually disappear Encourage mild exercise as ordered
 and ethacrynic acid (Edecrin) Phosphate-based drugs lower calcium level. Nursing Management. Pre Op – Encourage oral fluid intake. Strain urine for calculi. Offer cranberry juice to acidify the urine. Post Op – Assess for signs of hypocalcemia. Teach client principles of good body mechanics. Reassure client that bone pain will gradually disappear. Encourage mild exercise as ordered.")
60
HYPERPARATHYROIDISM NURSING INTERVENTIONS/Pt. TEACHING cont.
Postoperatively, assess for hypocalcemia Tetany, cardiac dysrhythmia, carpo-pedal spasms Pain management – skeletal, renal stones NURSING DIAGNOSES Activity intolerance r/t neuromuscular dysfunction Acute pain r/t skeletal – joint pain, renal colic

61
HYPERPARATHYROIDISM PATIENT TEACHING
Body mechanics to prevent pathological fx Mild exercise Urine checks for blood and stones PROGNOSIS: can lead a normal life with proper med-surg tx. With cancer dx. – prognosis is poor

62
http://www.youtube.com/watch?v=E9QvAdxeap0 (2 min 42 sec)
HYPOPARATHYROIDISM (2 min 42 sec) Etiology/pathophysiology Decreased parathyroid hormone Decreased serum calcium levels Most common causes: Inadvertent removal or destruction of one or more parathyroid glands during thyroidectomy Also, can be autoimmune or familial in origin Results from a deficiency of parathyroid hormone (PTH) secretion by the parathyroids or the decreased action of peripheral PTH Results in decreased serum calcium level Can be acute or chronic If idiopathic, may be result of autoimmune disorder or congenital absence of parathyroid glands Acquired hypoparathyroidism is generally irreversible Most common cause is accidental removal during thyroid or other neck surgery Reversible types as well Classic sign is tetany (muscle spasms and tremors caused by lack of calcium) Some other clinical manifestations include: Dry skin Brittle hair; alopecia Stained, cracked, decayed teeth (weak enamel) Personality or EKG changes, etc. Two diagnostic assessment tests: Chvostek’s sign Trousseau’s sign Expected test results include: Decreased serum calcium Increased urinary calcium Increased serum phosphorus Decreased urinary phosphorus Complications related to long-standing hypocalcemia Leads to decreased heart contractility leading to cardiac failure May be cataract formation, papillary edema, bone deformity
 Etiology/pathophysiology. Decreased parathyroid hormone Decreased serum calcium levels. Most common causes: Inadvertent removal or destruction of one or more parathyroid glands during thyroidectomy. Also, can be autoimmune or familial in origin. Results from a deficiency of parathyroid hormone (PTH) secretion by the parathyroids or the decreased action of peripheral PTH. Results in decreased serum calcium level. Can be acute or chronic. If idiopathic, may be result of autoimmune disorder or congenital absence of parathyroid glands. Acquired hypoparathyroidism is generally irreversible. Most common cause is accidental removal during thyroid or other neck surgery. Reversible types as well. Classic sign is tetany (muscle spasms and tremors caused by lack of calcium) Some other clinical manifestations include: Dry skin. Brittle hair; alopecia. Stained, cracked, decayed teeth (weak enamel) Personality or EKG changes, etc. Two diagnostic assessment tests: Chvostek’s sign. Trousseau’s sign. Expected test results include: Decreased serum calcium. Increased urinary calcium. Increased serum phosphorus. Decreased urinary phosphorus. Complications related to long-standing hypocalcemia. Leads to decreased heart contractility leading to cardiac failure. May be cataract formation, papillary edema, bone deformity.")
63
HYPOPARATHYROIDISM CLINICAL MANIFESTATIONS Lab results show:
↓serum Ca++ and ↑ serum phosphorus Neuromuscular hyperexcitability Involuntary and uncontrollable muscle spasms Hypocalcemic tetany

64
HYPOPARATHYROIDISM CLINICAL MANIFESTATIONS cont. Severe hypocalcemia:
Laryngeal spasms Stridor Cyanosis/asphyxia Parkinson-like syndrome Chvostek’s and Trousseau’s signs

65
TROUSSEAU’S SIGN

66
HYPOPARATHYROIDISM ASSESSMENT
SUBJECTIVE DATA – evidence of and/or c/o: Dysphagia Numbness/tingling lips, fingertips Increased muscle tension Parasthesis and stiffness c/o anxiety, irritability, depression Headaches nausea

67
HYPOPARATHYROIDISM ASSESSMENT OBJECTIVE DATA
+ Chvostek’s and Trousseau signs Laryngeal spasm, stridor, cyanosis Decreased cardiac output, dysrhythmias Tetany

68
HYPOPARATHYROIDISM DIAGNOSTIC TESTS Serum PTH, Phosphorus, Calcium
Urinary calcium and phosphorus if + for hypoparathyroidism, results will be: ↓ PTH, and serum Ca++ and ↑ urinary Ca++, with ↑ serum phosphorus and ↓ urinary phosphorus

69
HYPOPARATHYROIDISM MEDICAL MANAGEMENT Blood tests r/t ca levels
Calcium gluconate or calcium chloride will be given IV for hypoparathyroid tetany NURSING: if IV rate is too rapid ↓ BP, serious cardiac dysrhythmias/ cardiac arrest IV may be irritating to vessel wall; watch for s/sx extravasation EKG monitoring Vitamin D orally – improves GI absorption of Ca++ Calcium gluconate or calcium chloride may be given intravenously Too rapid IV calcium infusion can cause cardiac arrest May be given orally after initial IV dose Unless reversible, lifelong calcium replacement required Vitamin D may be given to assist in calcium absorption Best sources of calcium are from the diet Advise that calcium may cause digitalis toxicity Diet Foods high in calcium and low in phosphorus Asparagus Broccoli Collards Tomatoes Fruits such as apricots, bananas, cantaloupe, many berries Kidney and lima beans, brown sugar Avoid high phosphorous foods: most legumes, nuts, cheeses, seafood Nursing Management Monitor for signs of hypercalcemia Assess for respiratory distress Provide diet high in calcium-containing foods Emphasize importance of having blood level of calcium & phosphorus checked

70
HYPOPARATHYROIDISM NURSING INTERVENTIONS Monitor for hypercalcemia:
Vomiting, disorientation, anorexia, abdominal pain, weakness Assess for: Respiratory function VS – bradycardia, syncope, hypotension Renal involvement

71
HYPOPARATHYROIDISM NURSING INTERVENTIONS cont. Preferred medications:
Hytakerol Calcitriol (Rocaltrol) Diet: ↑ dairy, dark green leafy veg., soybeans, tofu, canned fish with bones
 Diet: ↑ dairy, dark green leafy veg., soybeans, tofu, canned fish with bones.")
72
HYPOPARATHYROIDISM NURSING DIAGNOSES:
Risk for injury r/t postop hypocalcemia Imbalanced nutrition, less than body requirements, r/t calcium intake Nearly all interventions r/t ca levels

Similar presentations











 Destruction of thyroid tissue –Radioactive Iodine –Hashimoto’s –Surgical.>")



. It has two lobes that are joined together.>")

 2. Siti Hadijah (14700108) 3. I Putu Adi Styawan (14700120) 4. Jaka Primadhana. R (14700132)>")




