Download presentation
Presentation is loading. Please wait.

1
C1 inhibitor Deficiency: Why does it happen and what does it look like?
Gina Lacuesta, MD FRCPC Allergy and Clinical Immunology Assistant Professor, Dalhousie University Nov 29,2014

2
Disclosure and Thank You
CSL Behring -Berinert® Shire-Firazyr ® and Cinryze® -attended advisory boards, international meetings and worked with sales and medical representatives Board Member of CHAEN

3
objective Review the definition and causes of angioedema – why are your doctors confused about this condition? Review the pathophysiology of C1 inhibitor deficiency – today you are a medical student! Review the clinical presentation of C1 inhibitor deficiency – does this sound like you?

4
Angioedema ANGIO – vessel EDEMA – swelling
Soft tissue swelling usually located around the eyes, lips, face, ears, tongue, hands, feet Usually asymmetrical In C1 inhibitor deficiency, intestinal angioedema is common with abdominal pain and urinary difficulties Laryngeal edema can be life threatening

5
As opposed to….EDEMA Swelling in dependant areas, ie feet, ankles, even sacral swelling, scrotal swelling, at end of day and around the eyes first thing in the morning Related to fluid shifts/fluid retention/salt and water balance Strongly associated with heart disease, liver disease, malnutrition, severe illness, ‘hormonal’ fluctuations

6
Picture of pitting edema

7
Non HAE Angioedema – causes
Allergy Cause is easily identifiable Food, drug, sting Can be life threatening Often associated with hives Often easy to figure out the allergic culprit With avoidance, most patients can live ‘normal’ lives Responds to epinephrine, antihistamines and steroids

8
Non HAE Angioedema - causes
DRUGS Aspirin/NSAIDs/anti-inflammatories ACE- inhibitors Well described phenomena; often forgotten about Quinke’s edema Uvula swelling only, repeatedly Often as a rebound reaction to dryness in the throat Occasionally, surgery used to correct

9
Non HAE Angioedema - causes
Infection Mostly, viral related Common, 1:10 will experience hives or angioedema, unexplained at least once in their lifetime Usually short lived, ie lasting a few months maximum, most often benign

10
Non HAE Angioedema - causes
Chronic spontaneous/autoimmune Often associated with hives Can happen daily for months/years Diagnosis of exclusion, ie. No other cause found Benign, most easily managed with well tolerated medications, ie antihistamines Newer treatments: Xolair ®, rarely immunosuppressants Common condition

11
Angioedema- why are your doctors confused
Compared to the previous, C1 inhibitor deficiency is very rare, and rarely, if at all taught in medical school Doctors ARE aware of the other causes, and are AFRAID of the other causes EVERYONE wants the angioedema to be managed by steroids/antihistamines/epinephrine and AVOIDANCE of food!…but it doesn’t work that way

12
Why is diagnosing C1 inhibitor deficiency an issue?
Documented failure to recognize and diagnose HAE-22 year delay in survey by Frank et. al. (Ann Int Med. 1976;84:580) Delay still observed in recent survey Age at diagnosis: 16.8 yrs (range 1-42 yrs) Age when sx began: 7.8 yrs (range 1-18 yrs) Delay in diagnosis: 9.1 yrs (range 0-32 yrs) Failure to diagnose dramatically increases the risk of significant M&M
 Delay still observed in recent survey. Age at diagnosis: 16.8 yrs (range 1-42 yrs) Age when sx began: 7.8 yrs (range 1-18 yrs) Delay in diagnosis: 9.1 yrs (range 0-32 yrs) Failure to diagnose dramatically increases the risk. of significant M&M.")
13
HAE/C1 inhibitor deficiency

14
What is complement? Part of our INNATE immune system
Present in everyone as a PRIMITIVE defense mechanism against infection As opposed to our ACQUIRED immune system which adapts based on our exposures, either via infection or vaccination COMPLEMENT helps our ACQUIRED immune system do its job, therefore, the term COMPLEMENT

15
Picture of complement cascade

16
Importance of C1 inhibitor
Controls bradykinin formation Bradykinin causes blood vessels to dilate and become permeable, ie leak fluid into the soft tissues, thus, swelling If bradykinin is allowed to produce repeatedly, if it does not get broken down and destroyed, and if its receptor is not blocked….there will be increased chances of swelling, inflammation and pain

18
C1 inhibitor deficiency

20
Complement profiles

21
HAE nomenclature HAE Type 1 – HAE due to C1 deficiency with low levels and functional assay HAE Type 2 – HAE due to C1 dysfunction with normal levels and low functional assay HAE Type 3 – HAE with normal C1 levels and functional assay

22
HAE type 1 and 2 1:50,000 Autosomal dominant; mutations of the SERPING1 gene 25% de novo mutation rate Bradykinin is the main mediator of swelling Bradykinin produced when kallikrein cleaves HMW kininogen. Kallikrein activated by factor XII Kallikrein and factor XII both normally inhibited by C1 inhibitor.

23
Features of HAE-Normal C1INH Compared to HAE-C1INH Deficiency – Bork 2007
Normal C1INH protein level and activity Predominantly women clinically affected Symptom onset in adulthood more common, rarely affects children Less frequent symptoms with longer symptom-free Intervals Facial and lip swelling more frequent Recurrent tongue swelling a cardinal symptom Many patients have only skin swelling Abdominal attacks less frequent Asphyxiation due to airway involvement occurs No erythema marginatum; hemorrhages into skin swelling has been observed

26
How patients present Angioedema without urticaria, can have non-pruritic serpiginous rash Angioedema mostly face, limbs, gut Can have profound pain syndromes, vomiting, diarrhea, voiding difficulties Attacks prolonged but do not occur daily; latency period “Average” untreated patient will swell q10-14 days, lasting 48-72h Enormous range of severity between patients Substantial morbidity seen in patient surveys Risk of death from laryngeal angioedema, mortality rate of 30% if left untreated

27
Most attacks affect the skin or abdomen
Angioedema most commonly involves the abdomen⁴, face, extremities, genitals, and larynx.¹ Skin attacks are the most common and usually manifest as disfiguring, nonpitting, and sometimes painful skin swelling affecting most commonly the extremities, face, and genitals.² Abdominal attacks occur in 70%-80% of patients with recurrent abdominal pain caused by edema in the stomach or intestinal wall and free fluid in the peritoneal cavity.³ Laryngeal attacks occur at least once in a patient’s lifetime in 50% of the cases. These attacks are usually classified as severe—as airway obstruction could be fatal—with mortality rates as high as 30% if left untreated or undiagnosed.2, 4 The probability that a given attack will involve the skin or abdomen is nearly 50% each. All other attack locations, including genitourinary and laryngeal attacks, account for only 3.6% of attacks.⁴ 1. Khan D A, Allergy Asthma Proc 2011; 32:1-10; 2. Banerji A,Allergy Asthma Proc 2011; 32: ; 3. Caballero T, J Investig Allergol Clin Immunol 2011;21(5): 333 ; 4. Bork K. et al. Am J Med 2006; 119:267-74
: 333 ; 4. Bork K. et al. Am J Med 2006; 119:")
28
Frequency of HAE Attacks
Attack frequency, severity, and course vary among patients, and even for a single patient depending on stage of life1,2,3 Less than one attack per year to more than 26 attacks per year Mean of 27 attacks /year Median 12 attacks/ year per patient In some rare cases, patients can experience more than 100 attacks per year No evident correlation between: Attack frequency and plasma levels of C1-INH Number of attacks from one year and the next Frequency of attacks in family members Although precipitated by known factors, attacks may occur without obvious trigger1,3 The frequency at which HAE attacks occur spans a broad range among patients and may also vary in the same patient during different stages of life. Reported rates range from <1 attack per year to >26 attacks per year. A recent study in 457 patients with HAE in the United States found that patients experienced an average of 27 attacks per year. In some cases, patients can experience >100 attacks per year. A survey of untreated patients with HAE in Italy found that nearly one-third had >1 attack per month, 40% had 6 to 11 attacks per year, and the remaining 30% had either no or infrequent attacks. [Agostoni 2004, p S57b; Levy 2006, p 6a] 1 Gompels MM, et al. Clin Exper Immunol ;139(3): Kaplan AP. J Allergy Clin Immunol. 2010;126(5): Frank MM Ann Intern Med. 1976;84:580ñ593
: Kaplan AP. J Allergy Clin Immunol. 2010;126(5): Frank MM Ann Intern Med. 1976;84:580ñ593.")
29
C1 inhibitor deficiency- acquired form AAE-symptoms the same
no family history later onset, usually after age 60 often associated with hematological malignancies, ie lymphoma, monoclonal gammopathy, or autoimmune diseases Often with low C1q levels Mechanism felt to be autoimmune, increased metabolism of C1 inhibitor, unknown Mainstay is to treat the underlying condition, but also to be aware of usual C1 inhibitor treatment, can become resistant to treatment, requiring increasing doses of C1 inh replacement Rarer than HAE

30
Health-Related QOL Decreases in Patients With HAE
Normative Population P<.0001 P<.0001 Patients With HAE 49.6 ± 9.9 49.4 ± 9.8 60 43.7 ± 10.2 42.6 ± 10.1 50 40 Mean SF-12 Score 30 20 10 Physical Component Summary Mental Component Summary In a survey of 457 patients with HAE, patients reported significant reduction in health-related quality of life. One component of the survey, the 12-Item Short Form (SF-12) Health Survey, consisted of 12 questions about health-related functioning over the prior 4 weeks. Survey outcomes included two summary scores: a Mental Component Summary (MCS-12) and a Physical Component Summary (PCS-12). For each, a higher score represents higher functioning. Compared with population norms, patients with HAE had lower mean scores across all components of the SF-12 Health Survey. Patients with HAE had a mean overall PCS-12 score of 43.7 (SD ± 10.2, P<.0001) vs 49.6 (SD ± 9.9, P<.0001) for population norms. Up to 70% of patients with HAE reported that the disease had affected their educational and career goals, possibly due to elevated levels of anxiety and depression. Patients with HAE suffer activity impairment comparable with impairments suffered by patients with severe asthma and Crohn’s disease. Reference Lumry WR, Castaldo AJ, Vernon MK, Blaustein MB, Wilson DA, Horn PT. The humanistic burden of hereditary angioedema: impact of health-related quality of life, productivity, and depression. Allergy Asthma Proc.2010;31(5): Patients with HAE are also significantly more likely to experience symptoms of depression compared with population norms (P<.0001) Up to 70% of patients report that HAE has affected their educational and career goals and that they may be unable to realize their potential due to high levels of anxiety and depression Patients with HAE experience a decline in productivity comparable with patients with severe asthma or Crohn’s disease QOL=quality of life; SF-12=Short Form Health Survey. Adapted from Lumry WR, et al. Allergy Asthma Proc. 2010;31(5): Shire Proprietary & Confidential Information
 Health Survey, consisted of 12 questions about health-related functioning over the prior 4 weeks. Survey outcomes included two summary scores: a Mental Component Summary (MCS-12) and a Physical Component Summary (PCS-12). For each, a higher score represents higher functioning. Compared with population norms, patients with HAE had lower mean scores across all components of the SF-12 Health Survey. Patients with HAE had a mean overall PCS-12 score of 43.7 (SD ± 10.2, P<.0001) vs 49.6 (SD ± 9.9, P<.0001) for population norms. Up to 70% of patients with HAE reported that the disease had affected their educational and career goals, possibly due to elevated levels of anxiety and depression. Patients with HAE suffer activity impairment comparable with impairments suffered by patients with severe asthma and Crohn’s disease. Reference. Lumry WR, Castaldo AJ, Vernon MK, Blaustein MB, Wilson DA, Horn PT. The humanistic burden of hereditary angioedema: impact of health-related quality of life, productivity, and depression. Allergy Asthma Proc.2010;31(5): Patients with HAE are also significantly more likely to experience symptoms of depression compared with population norms (P<.0001) Up to 70% of patients report that HAE has affected their educational and career goals and that they may be unable to realize their potential due to high levels of anxiety and depression. Patients with HAE experience a decline in productivity comparable with patients with severe asthma or Crohn’s disease. QOL=quality of life; SF-12=Short Form Health Survey. Adapted from Lumry WR, et al. Allergy Asthma Proc. 2010;31(5): Shire Proprietary & Confidential Information.")
31
Days Missed During Most Recent HAE Attackb
HAE Attacks Adversely Impact Work, School, and Leisure Activities Patients Affecteda Days Missed During Most Recent HAE Attackb Work Days (n=156) School Days (n=12) Leisure Days (n=271) Work Days (n=308) School Days (n=27) Leisure Days (n=457) 3.3 ±14.4 1.9 ±0.8 2.7 ±3.0 51 44 59 10 20 30 40 50 60 70 Patients Missing Days (%) 2 4 6 Mean Number of Days Missed In a survey of 457 patients with HAE, patients reported that HAE significantly impacted their ability to work and gain an education. 51% of employed patients missed at least 1 day of work due to their most recent HAE attack. 44% of student patients missed at least 1 day of school due to their most recent HAE attack. 59% of patient respondents reported that they missed at least 1 day of leisure activities due to their most recent HAE attack. Across all patients, the most recent HAE attack caused a mean number of 3.3 (SD ± 14.4) days of missed work, 1.9 (SD ± 0.8) days of missed school, and 2.7 (SD ± 3.0) missed leisure days. Reference Lumry WR, Castaldo AJ, Vernon MK, Blaustein MB, Wilson DA, Horn PT. The humanistic burden of hereditary angioedema: impact of health-related quality of life, productivity, and depression. Allergy Asthma Proc. 2010;31(5): aNumber of patients affected during most recent attack of HAE. bMean number of days missed during most recent attack of HAE. Lumry WR, et al. Allergy Asthma Proc. 2010;31(5): Shire Proprietary & Confidential Information
 School Days (n=12) Leisure Days (n=271) Work Days (n=308) School Days (n=27) Leisure Days (n=457) 3.3. ± ± ± Patients Missing Days (%) Mean Number of Days Missed. In a survey of 457 patients with HAE, patients reported that HAE significantly impacted their ability to work and gain an education. 51% of employed patients missed at least 1 day of work due to their most recent HAE attack. 44% of student patients missed at least 1 day of school due to their most recent HAE attack. 59% of patient respondents reported that they missed at least 1 day of leisure activities due to their most recent HAE attack. Across all patients, the most recent HAE attack caused a mean number of 3.3 (SD ± 14.4) days of missed work, 1.9 (SD ± 0.8) days of missed school, and 2.7 (SD ± 3.0) missed leisure days. Reference. Lumry WR, Castaldo AJ, Vernon MK, Blaustein MB, Wilson DA, Horn PT. The humanistic burden of hereditary angioedema: impact of health-related quality of life, productivity, and depression. Allergy Asthma Proc. 2010;31(5): aNumber of patients affected during most recent attack of HAE. bMean number of days missed during most recent attack of HAE. Lumry WR, et al. Allergy Asthma Proc. 2010;31(5): Shire Proprietary & Confidential Information.")
33
Management of C1 inhibitor deficiency
Gina Lacuesta, MD FRCPC Allergy and Clinical Immunology Assistant Professor, Faculty of Medicine Dalhousie University Nov 29, 2014

34
Objectives What are the goals of care?
What did treatment look like BEFORE and what was the problem? What does treatment look like now? What can we do better?

35
Previous goals of care Make the right diagnosis!
Recognize that the condition is hereditary and screen the family Keep the patients ALIVE Keep the patients out of the ER

36
New goals of care Improving quality of life
Treatment should aim to maximize patient health by Aborting acute attacks to prevent morbidity and mortality Minimize significant side effects Avoid disruption of normal life, ie school, work, family life

37
PAST treatment

38
Past treatment: side effects

39
In with the NEW….US data

40
In Canada: June 2010 : Berinert® fully approved for use in HAE
2012: Cinryze® approved in Canada, still waiting for its full release 2014: Firazry® approved in Canada

41
In Maritimes: 2011 First patient on prophylactic Berinert, early Spring 2011 4 patients being arranged In Hospital treatment only…thus far

42
In Maritimes: 2013 NS: 5 patients on prophylaxis( 4 self infusion/1 in hospital ) NB: 1 patient on prophylaxis( line in place, home) PEI: 1 patient on prophylaxis (line in place, in hosp) NS: 1 patient on demand(self), 1 due to be taught NB: 1 patient on demand (self)
 NS: 1 patient on demand(self), 1 due to be taught. NB: 1 patient on demand (self)")
43
In Maritimes: 2013 Still some patients on oral medications for on demand and prophylaxis and this works well for them 5 acquired C1 inhibitor deficiency patients, 1 of which is on prophylaxis.

44
In Maritimes: 2014 NS: 8 patients on Prophylaxis with Berinert
NB: 1 patient on Prophylaxis with Berinert PEI: 1 patient on prophylaxis with Berinert 10 others On Demand Berinert treatment, or prophylaxis with medications 6 with Firazyr On Demand, a few others in the works for approval

46
C 1 inhibitor

47
C1 inhibitor –eliminates the underlying cause by replacing the deficient protein
Berinert®-CSL Behring Cinryze®- Shire 20U/kg, slow IV push <50kg 1000U, >50kg 1500U Indicated for acute attacks Half life 32-47h Well tolerated Off label use with high doses in neonates resulted in thrombotic events 1000U, slow IV push, not based on weight Indicated for long term, routine prevention Half life 48+/- 10h Well tolerated

48
IMPACT2- International Multicenter Prospective Angioedema C1 inhib Craig, T. et al, Allergy, 2011
57 patients, 975 HAE attacks Open label extension of placebo controlled IMPACT1 trial Median time to onset of symptom relief of 15min for laryngeal attacks, 20 min for abdominal attacks, 28 min for facial attacks and 31 minutes for peripheral attacks

49
Nanofiltered C1 inhibitor in HAE- Zuraw, et al, Am J Med, 2012
Open label multi center extension study, 146 patients with HAE treated for 2.6y with prophylaxis Cinryze® 1000U every 3-7 days 93.7% reduction in attacks compared with historical rate of attacks 87.7% had 1 attack or less per month 34.9% had no attacks Twice weekly seemed to have the best control, though sub group responded to once a week, no predictors found

50
C1 inhibitor self infusion-Maritimes
Currently, all teaching has been done by hemophilia nursing, with follow up and support as needed Berinert® does come with option to be taught by private nursing ??Cinryze® to have a comprehensive training program established, based on education and training practices already used in the US, My PathTM, with ongoing support

51
Icatibant

52
Characteristics of Icatibant
Synthetic decapeptide with structure similar to bradykinin Indicated for the treatment of acute attacks of HAE in adults with C1-esterase inhibitor deficiency Delivered by subcutaneous (SC) injection in the abdomen Provided in a single-use, pre-filled syringe containing 30 mg (10 mg/mL) that can be stored at room temperature H 2 N O S C 3 n Shire Human Genetic Therapies (Canada) Inc. Firazyr Product Monograph. June 4, 2014. Shire Proprietary & Confidential Information
 injection in the abdomen. Provided in a single-use, pre-filled syringe containing 30 mg (10 mg/mL) that can be stored at room temperature. H. 2. N. O. S. C. 3. n. Shire Human Genetic Therapies (Canada) Inc. Firazyr Product Monograph. June 4, Shire Proprietary & Confidential Information.")
53
Endpoints Measure Onset and Resolution of Symptoms
Symptom severity of a treated attack Time t=0 Time course of a treated attack Beginning of attack Almost complete symptom relief (All VAS < 10mm) Treatment administration Initial symptom improvement earliest of 3 consecutive measures Onset of symptom relief (VAS ) Shire Proprietary & Confidential Information 53
 Treatment administration. Initial symptom improvement. earliest of 3 consecutive measures. Onset of symptom relief. (VAS ) Shire Proprietary & Confidential Information. 53.")
54
FAST 2: Time to Onset of Primary Symptom Relief Primary endpoint
100% Median 95% CI p-value Icatibant 2.0 <0.001 Tranexamic Acid 12.0 90% 80% 70% 60% Tranexamic Acid % of Patients Not Achieving Symptom Relief 50% 40% 30% 20% In FAST-2, Icatibant was effective in the treatment of acute HAE with primary endpoint showing consistent onset of primary symptom relief in 2 hours compared to median time to onset of 10.1 hours with tranexamic acid, which was statistically significant. To show you consistency of response, let‘s look as some other measures... 10% Icatibant 0% 12 24 36 48 Hours After Treatment Primary symptom relief is defined as a reduction of at least 30% from pre-treatment in the score for primary VAS; has to sustain for 3 consecutive non-missing measurements Cicardi M, et al. N Engl J Med. 2010;363: Erratum in: N Engl J Med. 2010;363:1468. ITT non-laryngeal population VAS Shire Proprietary & Confidential Information

55
FAST-3: Study Design and Patient Disposition
First eligible attack (n=98) Laryngeal attack (n=10) Abdominal and/or cutaneous attack (n=88) Moderate to severe attack Mild to moderate attack Severe attack Double-blind treatment: Icatibant vs placebo (n=43) (n=45) Double-blind treatment: Icatibant vs placebo (n=3) (n=2) Open-label treatment: icatibant (n=5) Treatment of subsequent attacks (cutaneous, abdominal, or laryngeal) Open-label extension phase Icatibant 30 mg SC up to 3 x per attack; no more than 8 injections per month (n=82 pts) Lumry W et al. Ann Allergy Asthma Immunol. 2011; 107: Shire Proprietary & Confidential Information 55
 Laryngeal attack. (n=10) Abdominal and/or cutaneous attack. (n=88) Moderate to severe attack. Mild to moderate attack. Severe attack. Double-blind treatment: Icatibant vs placebo. (n=43) (n=45) Double-blind treatment: Icatibant vs placebo. (n=3) (n=2) Open-label treatment: icatibant. (n=5) Treatment of subsequent attacks (cutaneous, abdominal, or laryngeal) Open-label extension phase Icatibant 30 mg SC up to 3 x per attack; no more than 8 injections per month. (n=82 pts) Lumry W et al. Ann Allergy Asthma Immunol. 2011; 107: Shire Proprietary & Confidential Information. 55.")
56
FAST-3: Time to Onset of Symptom Relief Primary endpoint
100% Median 95% CI p-value Icatibant 2.0 1.5, 3.0 <0.001 Placebo 19.8 6.1, 26.3 90% 80% 70% 60% Placebo (n=45) % of Patients Not Achieving Symptom Relief 50% 40% 30% 20% Icatibant (n=43) We have used Kaplan Meier Curves to show the progress of patients as they respond to treatment over time. This also allows you to see the response of every patient in the trial. The y- axis shows the percentage of patients who have not yet met the target endpoint. So as we move from the left to right, we are showing you each patient as they respond to therapy and hit the target endpoint. This Kaplan- Meier curve from the FAST 3 trial shows the primary endpoint of time to onset of symptom relief based on the composite VAS score, the VAS-3, It shows the rapid drop in the graph for the icatibant treated patients as each patient reaches the endpoint. Icatibant was significantly better than placebo in treatment of HAE attacks. In the analyses of these cutaneous and abdominal attacks, Icatibant patients had onset of symptom relief based on the composite VAS-3 in median 2 hrs compared to placebo patients where relief was not seen for median of 19.8 hr. Next, if you look at the Kaplan Meier curve for time to onset of symptom relief based on the primary single VAS…… 10% 0% 12 24 36 48 Hours After Treatment ITT population VAS 3 (abdominal pain, skin pain, and skin swelling) Onset of symptom relief is defined as a 50% reduction from pre-treatment in VAS 3 score; has to sustain for 3 consecutive non-missing measures Lumry W et al. Ann Allergy Asthma Immunol. 2011; 107: Shire Human Genetic Therapies (Canada) Inc. Firazyr Product Monograph. June 4, 2014. Shire Proprietary & Confidential Information
 % of Patients. Not Achieving Symptom Relief. 50% 40% 30% 20% Icatibant (n=43) We have used Kaplan Meier Curves to show the progress of patients as they respond to treatment over time. This also allows you to see the response of every patient in the trial. The y- axis shows the percentage of patients who have not yet met the target endpoint. So as we move from the left to right, we are showing you each patient as they respond to therapy and hit the target endpoint. This Kaplan- Meier curve from the FAST 3 trial shows the primary endpoint of time to onset of symptom relief based on the composite VAS score, the VAS-3, It shows the rapid drop in the graph for the icatibant treated patients as each patient reaches the endpoint. Icatibant was significantly better than placebo in treatment of HAE attacks. In the analyses of these cutaneous and abdominal attacks, Icatibant patients had onset of symptom relief based on the composite VAS-3 in median 2 hrs. compared to placebo patients where relief was not seen for median of 19.8 hr. Next, if you look at the Kaplan Meier curve for time to onset of symptom relief based on the primary single VAS…… 10% 0% Hours After Treatment. ITT population. VAS 3. (abdominal pain, skin pain, and skin swelling) Onset of symptom relief is defined as a 50% reduction from pre-treatment in VAS 3 score; has to sustain for 3 consecutive non-missing measures. Lumry W et al. Ann Allergy Asthma Immunol. 2011; 107: Shire Human Genetic Therapies (Canada) Inc. Firazyr Product Monograph. June 4, Shire Proprietary & Confidential Information.")
57
FAST-3: Time to Almost Complete Symptom Relief Secondary endpoint
100% Median 95% CI p-value Icatibant 8.0 5.0, 42.5 0.012 Placebo 36.0 29.0, 50.9 90% 80% Placebo 70% 60% % of Patients Not Achieving Symptom Relief 50% 40% Icatibant 30% 20% Icatibant accelerated resolution of attacks as measured by almost complete symptom relief at a median of 8 hr compared to placebo (median 36.0 h) as shown on this Kaplan-Meier that has now been extended to 120 hours on the x-axis. This faster time to near resolution of attacks reduced the amount of time that patients experienced the debilitating symptoms of HAE. Now that we have looked at the most recently completed and definitive trial, 10% 0% 10 20 30 40 50 60 70 80 90 100 110 120 Hours After Treatment ITT population VAS 3 (abdominal pain, skin pain, and skin swelling) Almost complete symptom relief is defined as all VAS scores ≤ 10 mm; has to sustain for 3 consecutive non-missing measurements Lumry W et al. Ann Allergy Asthma Immunol. 2011; 107: Shire Human Genetic Therapies (Canada) Inc. Firazyr Product Monograph. June 4, 2014. Shire Proprietary & Confidential Information
 as shown on this Kaplan-Meier that has now been extended to 120 hours on the x-axis. This faster time to near resolution of attacks reduced the amount of time that patients experienced the debilitating symptoms of HAE. Now that we have looked at the most recently completed and definitive trial, 10% 0% Hours After Treatment. ITT population. VAS 3. (abdominal pain, skin pain, and skin swelling) Almost complete symptom relief is defined as all VAS scores ≤ 10 mm; has to sustain for 3 consecutive non-missing measurements. Lumry W et al. Ann Allergy Asthma Immunol. 2011; 107: Shire Human Genetic Therapies (Canada) Inc. Firazyr Product Monograph. June 4, Shire Proprietary & Confidential Information.")
58
Events including open label extension trial
FAST-3: Icatibant Laryngeal Attack Efficacy Comparable to Abdominal or Cutaneous Laryngeal Treated Events including open label extension trial Icatibant (N=27attacks) Median time to onset of symptom relief as measured by VAS-5; hours (95% CI) 2.2 (1.5, 3.5) Median time to onset of primary symptom relief; hours (95% CI) Median time to almost complete symptom relief; hours (95% CI) 6.2 (3.0, 24.3) Shire Proprietary & Confidential Information
 Median time to onset of symptom relief as measured by VAS-5; hours (95% CI) 2.2. (1.5, 3.5) Median time to onset of primary symptom relief; hours (95% CI) Median time to almost complete symptom relief; hours (95% CI) 6.2. (3.0, 24.3) Shire Proprietary & Confidential Information.")
59
Laryngeal Attacks: Time to Initial Symptom Improvement
% of Patients Not Achieving Symptom Relief First laryngeal attack ISE Table 11.5 Shire Proprietary & Confidential Information

60
FAST OLE: Analysis of HAE Attacks Requiring Reinjection of Icatibant
More than 90% of HAE attacks were treated with a single icatibant injection regardless of location. Icatibant reinjection was infrequent and appeared to be independent of patient age, patient sex, HAE type, and initial attack severity. 0.5% 0.9% 90.4% 8% 91.8% 7.3% 1.1% All attacks Laryngeal Attacks Analysis of pooled data from all FAST OLE studies. Total # pts in FAST OLE: 225. Total # of attacks treated: 1149 Total # pts with laryngeal attacks in FAST OLE: 52. Total # of attacks treated: 110 1 injection 2 injections 3 injections injection + other acute HAE treatment Bernstein JA, et al. Poster presented at: American College of Allergy, Asthma and Immunology (ACAAI) 2013 Annual Scientific Meeting; November 7-11, 2013; Baltimore, MD. Poster P90. Berstein et al. Poster presented at AAAAI 2014
 2013 Annual Scientific Meeting; November 7-11, 2013; Baltimore, MD. Poster P90. Berstein et al. Poster presented at AAAAI")
61
Safety Profile Shire Human Genetic Therapies (Canada) Inc. Firazyr (icatibant) Product Monograph. June 4, 2014.
 Product Monograph. June 4,")
62
Safety Profile The overall incidence of serious adverse events (SAEs) was low in the clinical development program In the Phase I and II studies, only 2 SAEs were reported within 14 days of FIRAZYR treatment (manic episode, HAE); these were judged as not related/probably not related to treatment. In the controlled part of the three Phase III studies, only one SAE (cystitis) was reported within 14 days of dosing with FIRAZYR. This event was judged as not related to treatment. In the repeated treatment part of the Phase III studies, safety was evaluated for up to 15 FIRAZYR-treated attacks for patients. Sixteen patients experienced a total of 22 SAEs that occurred within 14 days of FIRAZYR administration. The only SAE that occurred in more than one patient was worsening or recurrence of HAE. Two SAEs were considered by the investigator as related to FIRAZYR treatment (events of arrhythmia and noncardiac chest pain). Shire Human Genetic Therapies (Canada) Inc. Firazyr (icatibant) Product Monograph. June 4, 2014.
; these were judged as not related/probably not related to treatment. In the controlled part of the three Phase III studies, only one SAE (cystitis) was reported within 14 days of dosing with FIRAZYR. This event was judged as not related to treatment. In the repeated treatment part of the Phase III studies, safety was evaluated for up to 15 FIRAZYR-treated attacks for patients. Sixteen patients experienced a total of 22 SAEs that occurred within 14 days of FIRAZYR administration. The only SAE that occurred in more than one patient was worsening or recurrence of HAE. Two SAEs were considered by the investigator as related to FIRAZYR treatment (events of arrhythmia and noncardiac chest pain). Shire Human Genetic Therapies (Canada) Inc. Firazyr (icatibant) Product Monograph. June 4,")
63
Injection Site Reactions are Common but Transient and Self-resolving
Photos courtesy of Dr M Bas, Klinikum Rechts der Isar der TechnischenUniversität München, Munich, Germany Represents moderate severity reaction 63 Shire Proprietary & Confidential Information

64
Icatibant Safety Profile in Open-Label Use
AEs in open-label extension of phase III controlled trials (N=225) were similar in frequency and nature to those observed in the controlled / blinded phase of the trials Rash, nausea, headache, worsening or recurrence of HAE Self-administered icatibant (N=98) displayed a safety profile similar to that of HCP-administered icatibant No hypersensitivity or anaphylactic reactions were reported in clinical trials No association between anti-icatibant antibodies and efficacy was observed Shire Human Genetic Therapies (Canada) Inc. Firazyr Product Monograph. June 4, 2014. 64 CONFIDENTIAL 64
 were similar in frequency and nature to those observed in the controlled / blinded phase of the trials. Rash, nausea, headache, worsening or recurrence of HAE. Self-administered icatibant (N=98) displayed a safety profile similar to that of HCP-administered icatibant. No hypersensitivity or anaphylactic reactions were reported in clinical trials. No association between anti-icatibant antibodies and efficacy was observed. Shire Human Genetic Therapies (Canada) Inc. Firazyr Product Monograph. June 4, CONFIDENTIAL. 64.")
65
Ecallantide-Kalbitor® not available in Canada

66
Kallikrein inhibitor Inhibits cleavage of HMW kininogen to bradykinin and therefore prevents progression of angioedema attack Ecallantide- Kalbitor®- Dyax. 30mg sc injection, half life 1-2hours Has had reported anaphylaxis

67
Attenuated Androgens Danazol, stanazolol, oxandrolone
Contraindicated in pregnancy, lactation, cancer, hepatitis, childhood Significant side effects of virilization, weight gain, acne, hair growth, altered libido, voice deepening, decreased breast size, menstrual irregularities, HTN, atherosclerosis, increased liver enzymes, cholestasis, HCC Dose varies from 100mg EOD, to 200mg TID, adjusting to clinical response More effective than antifibrinolytic agents

68
Antifibrinolytic agents
Used in more in pediatric population, as a safer alternative to androgens, but evidence of efficacy lacking Side effects mostly GI, theoretical risk of increased thrombosis Dosing 30-50mg/kg in divided doses 2-3 times /day to max of 6g

71
WAO Guideline Consensus meeting in Turkey 2011
Published in WAO Journal DEC 2012

75
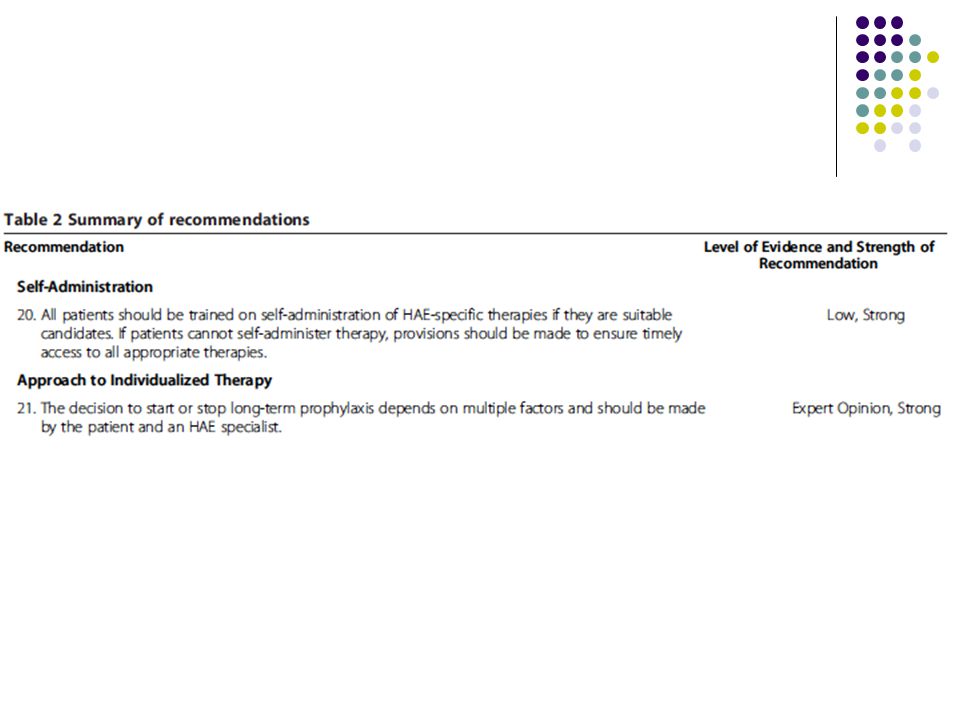
Short term/preprocedural prophylaxis
Evidence is lacking, but generally considered to be a strong recommendation Dental/intraoral surgery, any procedure requiring intubation, with upper airway or pharynx manipulation, bronchoscopy or endoscopy History of frequent swellings, swelling after a similar procedure in the past Stressful periods, concurrent infections C1 inhibitor U/kg 1-6 hours before procedure, with on demand treatment available also Other options: Androgens or tranexamic acid

77
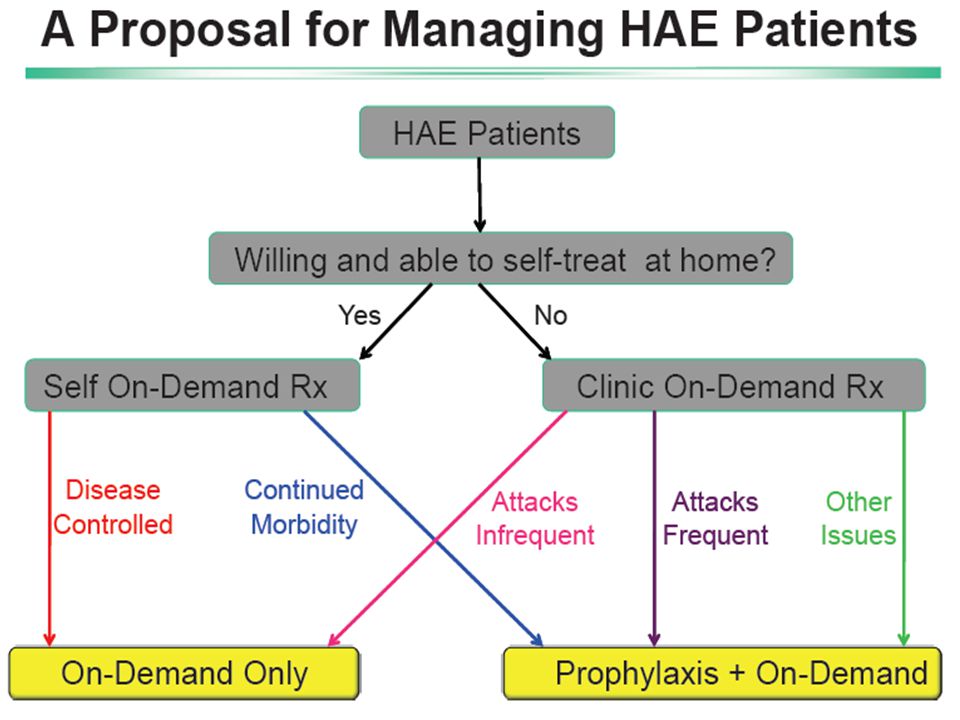
Long term prophylaxis Use of regular medication to prevent episodes of angioedema Takes into consideration severity of disease, frequency of attacks, patients' quality of life, availability of resources, failure to achieve adequate control with on demand therapy If more than 1 severe attack occurs per month, or treatment for severe attack is not sufficiently effective Choice between C1 inhibitor replacement, androgens, antifibrinolytic agents

83
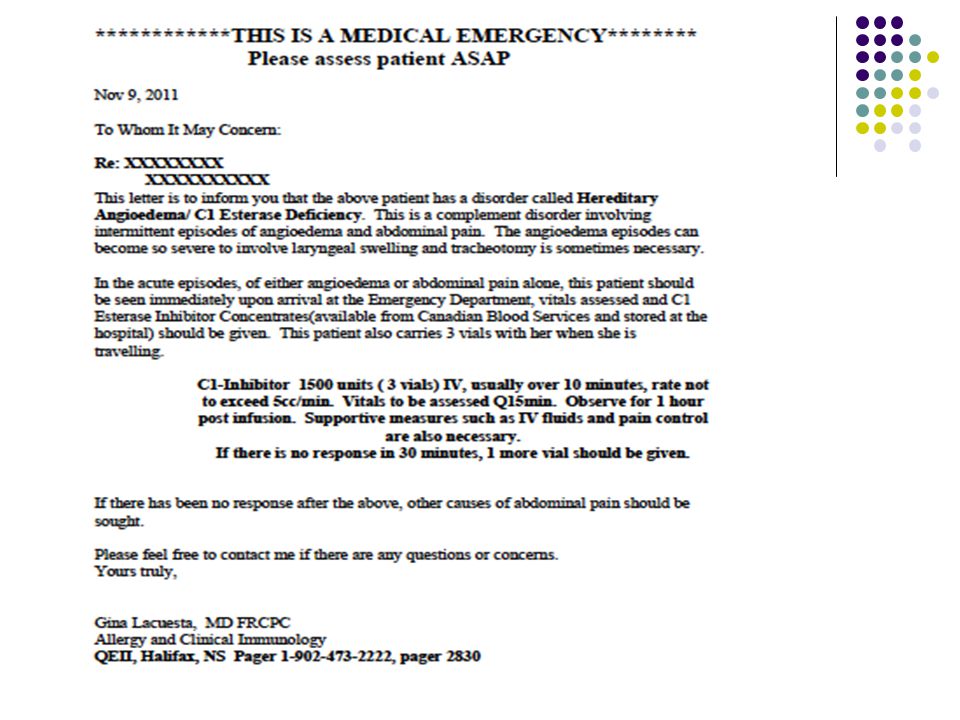
Management Counseling about their disease, genetics
Refer to patient support HAE groups Carry letters identifying them as a C1 inhibitor deficiency patient, urgency and how to treat Baseline viral studies and liver function studies; Hepatitis A and B vaccine, influenza vaccine

86
Management Depending on long term drug treatment- labs and radiology to monitor side effects Education regarding MEDS to avoid ( ACE inhibitors for blood pressure, estrogen supplements/birth control), potentially exacerbating situations(fatigue, stress, dental work, surgery, infection, etoh, menses etc)
, potentially exacerbating situations(fatigue, stress, dental work, surgery, infection, etoh, menses etc)")
87
Management C1 inhibitor to be stocked at home hospital
Patients educated to be vigilant about keeping relations with blood bank, especially in remote areas

88
Long term care for HAE patients
procedures timing Develop action plan Provide with HAE emergency card Provide with 2 doses of on demand therapy Screen family Hep B, C HIV screening Assessment by HAE specialist Influenza vaccine If androgens used: LFT,CBC,Lipids, UA Cardiac RF U/S liver At diagnosis and annually At diagnosis At diagnosis, annually if using blood product Annually Start and q 6 months Start and q6 months Start and q 12 months Craig, et al, WAO Journal, Dec 2012

91
Pediatric population Attacks usually occur during school age years, in 50% of cases between age 5-11 Upper airway is rarely the initial presentation Erythema marginatum is more frequent and often mistaken for urticaria Pre-natal testing is not recommended Testing at birth is not recommended, due to false negative testing

92
Pediatric population If symptomatic, still need a treatment plan and on demand therapy Ecallantide and icatibant are not licensed for use in children C1 inhibitor best choice for on demand therapy Antifibrinolytics(20-40mg/kg) chosen over androgens because of side effect profile. Common triggers include infection and mechanical trauma Vaccination recommended to reduce infection Avoid use of oral estrogen contraception Educate all caregivers
 chosen over androgens because of side effect profile. Common triggers include infection and mechanical trauma. Vaccination recommended to reduce infection. Avoid use of oral estrogen contraception. Educate all caregivers.")
93
Pregnancy Can either mitigate, worsen or not change the frequency of attacks at all C1 inhibitor replacement is the recommended first line therapy. Short term prophylaxis is recommended during any procedures including amniocentesis, chorionic villus sampling, surgical abortion. Not necessary with uncomplicated natural delivery, but should be available for 72hours port partum

94
Pregnancy C1 inhib should be given prophylactically if:
HAE is known to be severe Frequent swellings in 3rd trimester History of vaginal edema with mechanical trauma If intubation necessary With forceps or vacuum extraction needed C- section Androgens not recommended in pregnancy due to effects on the fetus, also not recommended during breastfeeding Tranexamic acid can be used if C1 inhibitor not available

95
AAE management Essentially the same principles, except treatment for underlying condition plays an important role May have some benefit from antihistamines, steroids as can also have an autoimmune histamine mediated angioedema along with AAE Can use either Icatibant or C1 inhibitor -On Demand, though not formally studied If prophylaxis required, can become “resistant” to C1 inhibitor replacement of may need higher than usual dosing

96
After these presentations, you should be able to:
Define and classify HAE Know what tests are ordered to diagnose HAE/AAE. Know what other conditions your drs are thinking about and how to differentiate from them Discuss management strategies, ie on-demand, short term and long term prophylaxis How the appropriate medications and replacement are prescribed What information is important to patients and primary physicians about follow up, meds to avoid, when to be vigilant Discuss special circumstances, ie pediatric population, pregnancy Acquired angioedema Recognize and refer to international and national guidelines Be an EXPERT in HAE

97
What else can we do? 2011: Train and recruit more immunologists
Educate local physicians/ER/nurses Maintain good working relationships with blood banks Set up self treatment program If not a candidate for self treatment program, have a plan for treatment of acute swelling attacks….stay on top of C1 stock in local hospitals 2013: Consider participating in upcoming trials Now there is CHOICE in effective, safe treatments…how do we make those choices? Be responsible with the products that we use

98
What else can we do? EDUCATE, EDUCATE, EDUCATE
Lobby for coverage and access for all patients Comprehensive care clinics Look forward to more sc products, ? Oral products

99
questions How soon into an HAE attack do I take the first Firazyr injection? If I take the first injection early enough, should it stop the attack from worsening? In order to judge if Firazyr is going to be an effective treatment in decreasing an attack, would I have to use it during a couple of HAE attacks to assess the results? I used it once and I was still not well for 2-3 days afterwards.

100
questions If the Firazyr did not decrease my swelling after the first dose, how long should I wait before I go to the hospital? Can I take Berinert between the first dose of Firazry and the second dose of Firazyr when the first dose did not stop or decrease my swelling? If I have to try the second dose of Firazyr before taking berinert, how long do I have to wait after I take the second Firazyr to take Berinert?

101
questions Does Firazyr have the same drug components/ingredients in it as Berinert? I keep Firazyr in the fridge at a temperature above 2 degrees. What temperature should it be at when I administer it? For example, should I let it sit out of the fridge for a little while before I use it?

102
questions What is the experience of patients who have taken Firazyr ? for example how long did it for them to feel the swelling decreasing? How long did it take for the swelling to be gone completely? Have they had any side effects from it? If so what were they? For patients who took long term Danazol and is now off it, are there any tests as follow up that they should have done ?

103
Canadian websites HAE Canada's Physician Website: www.chaen-rcah.ca

Similar presentations























 For the prevention and treatment of acute attacks of Hereditary Angioedema Reid Nakagawa November 31, 2013.>")
 Admission criteria for.>")








 Ulcerative colitis is an inflammatory bowel disease (IBD) that causes chronic inflammation of the digestive tract It is.>")
 Disease (strep throat, necrotizing fasciitis, impetigo) By: Dr. Awatif Alam.>")

