Download presentation
Presentation is loading. Please wait.

1
Non-Invasive Echo Assessment of Valvular Regurgitation Part 1 MR
Dr. Essam El Garhy Consultant Cardiologist - KFMMC 5th ,April 2012

2
You are now watching: 7 golden rules of echocardiography
1. Echo is an art, so practice! In order for you to become an expert, you need to practice, practice, practice. But how do you know if your reports are true and valid? This question takes us straight to the second rule… 2. Get an adviser to guide your way. Mentors are important for two reasons: Firstly, they can correct and assist you in your clinical judgment. Secondly, they will guide your echo practice. 3. Be interested and always ask “why”. Curiosity is one of the driving factors of successful diagnosticians. always ask why…“Why is the ventricle enlarged?” – “Why is the jet eccentric?” – “Why is RVF poor?” – “Might this be PE ?” etc. Also: play around! Use abnormal views and see what happens when you manipulate the transducer.

3
4. You are allowed to talk to the patient!
This will ease the patient and make the exam more pleasant. 5. Study cardiology and cardiothoracic surgery. Put yourself into the driving seat of patient management. Your echocardiogram is often key to the treatment strategy. 6. Measure and quantify but only trust reliable values. Everybody likes facts and numbers to base decisions on. However, many studies have found that eyeballing performed by an experienced echocardiographer is just as good, if not better, as a measurement. 7. Store digitally and compare with previous studies! That’s what radiologist do all the time. You can easily miss subtle changes simply based on measurements, which have a large measurement error. Left ventricular function and pericardial effusion are good examples. The eye will give you a better appreciation. If you can stick to these rules, your echo skills will significantly improve.

4
Major Factors That Affect Flow Across Any Valvular Lesion
The valve area The square root of the hydrostatic pressure gradient across the valve The time duration of transvalvular flow (applies to both systole and diastole)
")
5
Valvular Heart Disease
Increasing any of the major factors that affect flow across the valve increases transvalvular flow. Conversely, decreasing any of these major factors decreases transvalvular flow.

6
Goals in Management of Various Valvular Lesions
Regurgitant Lesions Reduce or minimize regurgitant flow across the mitral or aortic valve. Stenotic Lesions Maximize and enhance stenotic flow across the mitral or aortic valve

7
Goals in Management of Various Valvular Lesions
The valve area in regurgitant lesions can respond to changes in loading conditions (preload, afterload) The valve area with stenotic lesions is generally fixed
 The valve area with stenotic lesions is generally fixed.")
8
Mitral Regurgitation Valve leaflets Chordae tendineae
Papillary muscles Rheumatic disease Endocarditis Mitral valve prolapse Mitral annular enlargement Ischemia Myocardial infarction Trauma Fenfluramine diet suppressants

10
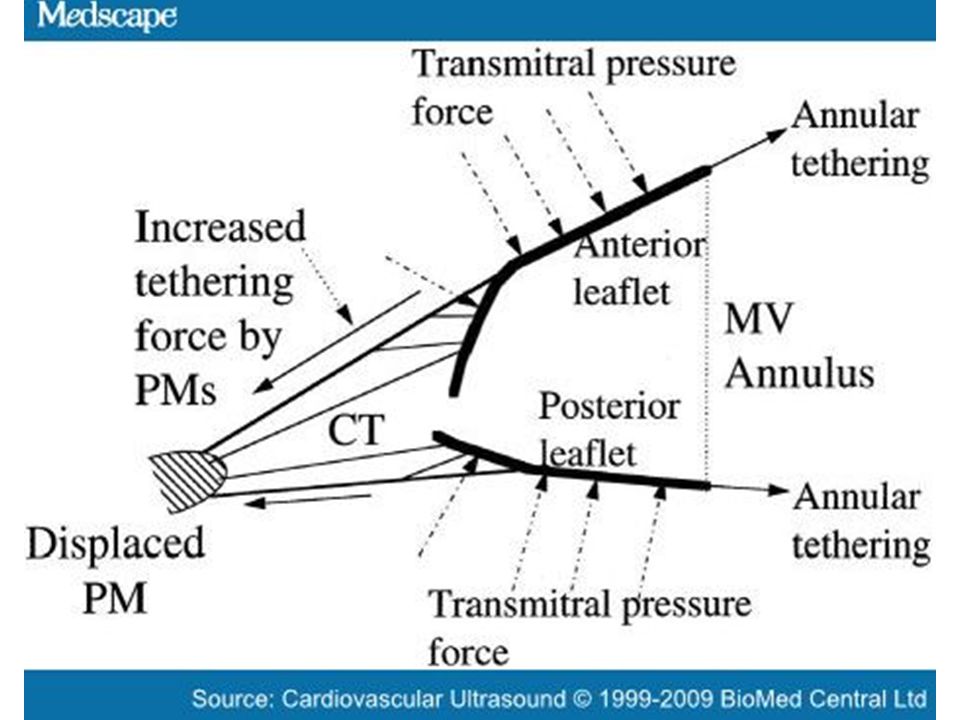
Mechanism of functional mitral regurgitation. A, normal mitral valve
Mechanism of functional mitral regurgitation. A, normal mitral valve. B, ischemic mitral valve with pronounced posterior restriction in P3 after an episode of ventricular ischemia. LV, left ventricle.

11
Pathophysiology of Mitral Regurgitation
Backward flow of blood from LV to LA (Systolic) Left atrial enlargement Increased LA volume and pressure Increased pulmonary venous pressures Increased LV filling (Increased LVEDV) Pulmonary edema Increased SV Blood ejected into aorta
 Left atrial enlargement. Increased. LA volume and. pressure. Increased. pulmonary. venous pressures. Increased LV filling. (Increased LVEDV) Pulmonary. edema. Increased SV. Blood ejected into aorta.")
12
Pathophysiology LV “unloads” itself into left atrium
Chronic left atrial overload Chronic overload on left ventricle Volume of regurgitant flow determined by: Ventriculo-atrial gradient Diastolic time Size of the regurgitant orifice Measurements of LV function tend to be slightly elevated Moderately depressed ejection fraction in a patient with MR may be indicative of a severely depressed inotropic state

13
Natural History MR consequences
The consequences of MR on the left ventricle and right ventricle pressures will depend on its acuteness and mechanism. Acute MR -reduction of forward stroke volume -increase in end-diastolic volume → hyperkinetic LV → reduced LA compliance→ elevation LA pressure→ pulmonary edema → elevation RVSP Chronic MR - LA dilatation - hyperkinetic LV - LV dilatation (increased diastolic volume) - elevation RVSP
 - elevation RVSP.")
14
HEMODYNAMIC GOALS IN MR:
Preload Increased or Decreased Best level of preload for an individual patient must be based on their response to fluid load. Heart Rate Increased Increased HR leads to a decrease in LV volume, increased forward flow, and decreased regurgitant fraction. Contractility Increased or Maintain Increased contractility tends to increase forward flow and may reduce regurgitant fraction by constricting mitral annulus. SVR Decreased Afterload reduction is helpful in improving forward flow. PVR Frequently have elevated PA pressures. Avoid acidosis, hypercarbia, and/or hypoxemia.

15
Types and Etiology Of MR

16
Marfan syndrome TEE (A) and color Doppler flow (B) from a 27 year-old man, with Marfan syndrome. Note severe mitral valve regurgitation from: annulus dilatation, lengthening of the chordae tendineae and a redundancy of the leaflets, especially of the posterior one.
 and color Doppler flow (B) from a 27 year-old man, with Marfan syndrome. Note severe mitral valve regurgitation from: annulus dilatation, lengthening of the chordae tendineae and a redundancy of the leaflets, especially of the posterior one.")
17
(A) In normal mitral valve, the coaptation (red point) occurs beyond the mitral annular plane (line); (B) billowing mitral valve is observed when a part of the mitral valve body protrudes into the left atrium (arrow); (C and D) mitral valve prolapse is defined as abnormal systolic displacement of one (C: posterior prolapse) or both leaflets into the left atrium below the annular (D: bileaflet prolapse); (E) flail of the anterior leaflet (arrow). (A) In normal mitral valve, the coaptation (red point) occurs beyond the mitral annular plane (line); (B) billowing mitral valve is observed when a part of the mitral valve body protrudes into the left atrium (arrow); (C and D) mitral valve prolapse is defined as abnormal systolic displacement of one (C: posterior prolapse) or both leaflets into the left atrium below the annular (D: bileaflet prolapse); (E) flail of the anterior leaflet (arrow). Lancellotti P et al. Eur J Echocardiogr 2010;11: Published on behalf of the European Society of Cardiology. All rights reserved. © The Author For permissions please
 In normal mitral valve, the coaptation (red point) occurs beyond the mitral annular plane (line); (B) billowing mitral valve is observed when a part of the mitral valve body protrudes into the left atrium (arrow); (C and D) mitral valve prolapse is defined as abnormal systolic displacement of one (C: posterior prolapse) or both leaflets into the left atrium below the annular (D: bileaflet prolapse); (E) flail of the anterior leaflet (arrow). Lancellotti P et al. Eur J Echocardiogr 2010;11: Published on behalf of the European Society of Cardiology. All rights reserved. © The Author For permissions please")
18
Transthoracic echocardiography:
parasternal long axis view from a patient with isolated mitral valve cleft: note preoperative severe mitral valve regurgitation (on color flow Doppler: the regurgitant jet passes through the cleft of the anterior mitral valve leaflet, and it is directed posteriorly) (A); and postoperative, after repairing the cleft, a mild mitral valve regurgitation (B).
 (A); and postoperative, after repairing the cleft, a mild mitral valve regurgitation (B).")
19
Adult patient with severe mitral valve regurgitation on shortened cordae tendineae (note: posterior mitral leaflet with limited mobility - arrow, and eccentric regurgitant jet orriented to posterior atrial wall)
")
20
AS

21
Parasternal long axis view with colour M mode Doppler echocardiography from a patient with hypertrophic cardiomyopathy and a high (90 mmHg) outflow tract gradient. Parasternal long axis view with colour M mode Doppler echocardiography from a patient with hypertrophic cardiomyopathy and a high (90 mmHg) outflow tract gradient. Notice the occurrence of systolic anterior motion of the mitral valve at the same time as the presence of outflow turbulence (arrow), and later into systole, the presence of mitral regurgitation. Prasad K et al. Heart 1999;82:III8-III15 Copyright © BMJ Publishing Group Ltd & British Cardiovascular Society. All rights reserved.
 outflow tract gradient. Notice the occurrence of systolic anterior motion of the mitral valve at the same time as the presence of outflow turbulence (arrow), and later into systole, the presence of mitral regurgitation. Prasad K et al. Heart 1999;82:III8-III15. Copyright © BMJ Publishing Group Ltd & British Cardiovascular Society. All rights reserved.")
22
Assessment of the severity of MR
Quantitative parameters Vena contracta ( VC ) Regurgitant Volume (RV) Regurgitant Fraction (RF%) Effective Regurgitant Orifice Area (ERO)
 Regurgitant Volume (RV) Regurgitant Fraction (RF%) Effective Regurgitant Orifice Area (ERO)")
23
Visual assessment of MR jet using colour-flow imaging
Visual assessment of mitral regurgitant jet using colour-flow imaging. Examples of two patients with severe mitral regurgitation. (A) Large central jet. (B) Large eccentric jet with a clear Coanda effect. CV, four-chamber view. Lancellotti P et al. Eur J Echocardiogr 2010;11: Published on behalf of the European Society of Cardiology. All rights reserved. © The Author For permissions please
 Large central jet. (B) Large eccentric jet with a clear Coanda effect. CV, four-chamber view. Lancellotti P et al. Eur J Echocardiogr 2010;11: Published on behalf of the European Society of Cardiology. All rights reserved. © The Author For permissions please")
24
A vena contracta 3 mm indicates mild MR whereas a width ≥7 mm defines severe MR. Intermediate values are not accurate at distinguishing moderate from mild or severe MR (large overlap); they require the use of another method for confirmation.
; they require the use of another method for confirmation.")
25
VC EROA mm2 R V mL E m/s < 3 <1 < 20 < 30 >=7 >1.4
Width (mm) TVI TVI MV / TVI AV EROA mm2 R V mL E m/s MV inflow MILD < 3 <1 < 20 < 30 A wave dominate SEVERE >=7 >1.4 >=40 >=60 E wave > 1.5 m/s
 TVI. TVI MV / TVI AV. EROA mm2. R V mL. E m/s. MV inflow. MILD. < 3. <1. < 20. < 30. A wave. dominate. SEVERE. >=7. >1.4. >=40. >=60. E wave. > 1.5. m/s.")
26
Moderate MR EROA EROA 30-39 mm2 20 – 29 mm2 R Vol R Vol 45-59 mL
Moderate to severe Mild to moderate EROA 30-39 mm2 R Vol 45-59 mL EROA 20 – 29 mm2 R Vol mL

27
Grading organic MR severity

28
TVI MV/AV 0.7 TVI MV/AV 1.0 TVI MV/AV 1.7
In severe MR, CWD signal of the MRJ is truncated, triangular and intense . Notching of the continuous wave envelope (cut-off sign) can occur in severe MR.
 can occur in severe MR.")
29
Normal pulmonary vein flow pattern;
(B) Blunt forward systolic pulmonary vein flow in a patient with moderate MR; (C) Reversed systolic pulmonary flow in a patient with severe MR.
 Blunt forward systolic pulmonary vein flow in a patient with moderate MR; (C) Reversed systolic pulmonary flow in a patient with severe MR.")
30
Stepwise analysis of MR: (A) Apical four-chamber view
Quantitative assessment of MR severity using the proximal isovelocity surface area method. Stepwise analysis of MR: (A) Apical four-chamber view (B) colour-flow display; (C) zoom of the selected zone; (D) downward shift of zero baseline to obtain an hemispheric proximal isovelocity surface area; (E) measure of the proximal isovelocity surface area radius using the first aliasing; (F) continuous wave Doppler of MR jet allowing calculation the effective regurgitant orifice area (EROA) and regurgitant volume (R Vol). TVI, time-velocity integral. Quantitative assessment of mitral regurgitation (MR) severity using the proximal isovelocity surface area method. Stepwise analysis of MR: (A) Apical four-chamber view (CV); (B) colour-flow display; (C) zoom of the selected zone; (D) downward shift of zero baseline to obtain an hemispheric proximal isovelocity surface area; (E) measure of the proximal isovelocity surface area radius using the first aliasing; (F) continuous wave Doppler of MR jet allowing calculation the effective regurgitant orifice area (EROA) and regurgitant volume (R Vol). TVI, time-velocity integral. Lancellotti P et al. Eur J Echocardiogr 2010;11: Published on behalf of the European Society of Cardiology. All rights reserved. © The Author For permissions please
 Apical four-chamber view. (B) colour-flow display; (C) zoom of the selected zone; (D) downward shift of zero baseline to obtain an hemispheric proximal isovelocity surface area; (E) measure of the proximal isovelocity surface area radius using the first aliasing; (F) continuous wave Doppler of MR jet allowing calculation the effective regurgitant orifice area (EROA) and regurgitant volume (R Vol). TVI, time-velocity integral. Quantitative assessment of mitral regurgitation (MR) severity using the proximal isovelocity surface area method. Stepwise analysis of MR: (A) Apical four-chamber view (CV); (B) colour-flow display; (C) zoom of the selected zone; (D) downward shift of zero baseline to obtain an hemispheric proximal isovelocity surface area; (E) measure of the proximal isovelocity surface area radius using the first aliasing; (F) continuous wave Doppler of MR jet allowing calculation the effective regurgitant orifice area (EROA) and regurgitant volume (R Vol). TVI, time-velocity integral. Lancellotti P et al. Eur J Echocardiogr 2010;11: Published on behalf of the European Society of Cardiology. All rights reserved. © The Author For permissions please")
31
Proximal Isovelocity Surface Area (PISA)
")
32
Measurements Required for PISA Method
radius of flow convergence hemisphere (cm) aliasing velocity on color bar (cm) peak regurgitant velocity (cm) TVI of regurgitant CW jet (cm)
 aliasing velocity on color bar (cm) peak regurgitant velocity (cm) TVI of regurgitant CW jet (cm)")
33
PISA Method Shift color baseline in direction of flow MR ↓
Aliasing velocity will vary (20-40cm) ideal: an aliasing velocity that creates a hemispheric shape Measure the radius (r) in mid-late systole {peak MR velocity} and take note of the aliasing velocity (Va)
 ideal: an aliasing velocity that creates a hemispheric shape. Measure the radius (r) in mid-late systole {peak MR velocity} and take note of the aliasing velocity (Va)")
34
To avoid the underestimation of the regurgitant
volume the ratio of the aliasing velocity (Va) to peak orifice velocity (vel) is maintained <10%.
 to peak orifice velocity (vel) is maintained <10%.")
35
PISA Method Using CW doppler, obtain optimal regurgitant jet
Measure peak regurgitant velocity (V) Trace regurgitant VTI PISA Calculation: Flow (cc/sec) = 6.28 x [r (cm.)2] x Va (cm/sec) ERO (cm2) = Flow (cc/sec) V (cm/sec) RV (cc) = ERO (cm2) x VTI (cm)
 Trace regurgitant VTI. PISA Calculation: Flow (cc/sec) = 6.28 x [r (cm.)2] x Va (cm/sec) ERO (cm2) = Flow (cc/sec) V (cm/sec) RV (cc) = ERO (cm2) x VTI (cm)")
36
MR by PISA

38
4 examples of flow convergence zone changes during systole using colour M-Mode. (A and B) Functional mitral regurgitation (A: early and late peaks and mid-systolic decreases; B: early systolic peak), (C) rheumatic mitral regurgitation with a end-systolic decrease in flow convergence zone, (D) M mitral valve prolaspe (late systolic enhancement).
, (C) rheumatic mitral regurgitation with a end-systolic decrease in flow convergence zone, (D) M mitral valve prolaspe (late systolic enhancement).")
39
Illustration of the variation of the PISA and hence ERO during systole
Illustration of the variation of the PISA and hence ERO during systole. In early and late systole, closing forces are relatively low and so the ERO and PISA relatively large. In midsystole, coincident with peak regurgitant velocity closing forces are maximal and so the ERO and PISA contract as the tips of the leaflets are forced closer together.

40
CW Doppler of MRJ Peak MR jet velocities by CW Doppler typically range between 4and 6 m/s. This reflects the high systolic pressure gradient between the LV and LA. The velocity itself does not provide useful information about the severity of MR. Conversely, the signal intensity (jet density) of the CW envelope of the MR jet can be a qualitative guide to MR severity. A dense MR signal with a full envelope indicates more severe MR than a faint signal. The CW Doppler envelope may be truncated (notch) with a triangular contour and an early peak velocity (blunt). This indicates elevated LA pressure or a prominent regurgitant pressure wave in the LA due to severe MR. In eccentric MR, it may be difficult to record the full CW envelope of the jet because of its eccentricity, while the signal intensity shows dense features.
 of the CW envelope of the MR jet can be a qualitative guide to MR severity. A dense MR signal with a full envelope indicates more severe MR than a faint signal. The CW Doppler envelope may be truncated (notch) with a triangular contour and an. early peak velocity (blunt). This indicates elevated LA pressure or a prominent regurgitant pressure wave in the LA due to severe MR. In eccentric MR, it may be difficult to record the full CW envelope of the jet because of its eccentricity, while the signal intensity shows dense features.")
41
CW Doppler Assessment of MR
Shape: symmetrical or asymmetrical Chronic vs. Acute MR Density of signal

42
Consequences of mitral regurgitation
The presence of severe MR has significant haemodynamic effects, primarily on the LV , LA and SPAP .

43
The LV contractility can thus decrease silently and irreversibly.
LV size and function The LV dimensions and EF reflect the heart’s ability to adapt to increased volume load. In the chronic compensated phase (the patient could be asymptomatic), the forward SV is maintained through an increase in LVEF . Such patients typically have LV EF 65%. In the chronic decompensated phase (the patient could still be asymptomatic or may fail to recognize deterioration in clinical status), the forward SV decreases and the LAP increases significantly. The LV contractility can thus decrease silently and irreversibly.
, the forward SV is maintained through an increase in LVEF . Such patients typically have LV EF 65%. In the chronic decompensated phase (the patient could still be asymptomatic or may fail to recognize deterioration in clinical status), the forward SV decreases and the LAP increases significantly. The LV contractility can thus decrease silently and irreversibly.")
44
However, the LV ejection fraction may still be in the low normal range despite the presence of significant muscle dysfunction. current guidelines, surgery is recommended in asymptomatic patients with severe organic MR when the LV ejection fraction is ≤60%. In the end-systolic diameter .45 mm (or ≥40 mm or .22 mm/m2, AHA/ACC), also indicates the need for mitral valve surgery.
, also indicates the need for mitral valve surgery.")
45
A systolic tissue Doppler velocity measured at the lateral annulus,10
A systolic tissue Doppler velocity measured at the lateral annulus,10.5 cm/s has been shown to identify subclinical LV dysfunction and to predict post-operative LV dysfunction in patients with asymptomatic organic MR. Strain imaging allows a more accurate estimation of myocardial contractility than tissue Doppler velocities.

46
Left atrial size and pulmonary pressures
The LA dilates in response to chronic volume and pressure overload. A normal sized LA is not normally associatedwith significantMR unless it is acute, in which case the valve appearance is likely to be grossly abnormal. LA remodelling (diameter 40–50 mm or LA volume index .40 mL/m2) may predict onset of AF and poor prognosis in patients with organic MR.
 may predict onset of AF and poor prognosis in patients with organic MR.")
47
Conversely, MV repair leads to LA reverse remodelling, the extent of which is related to preoperative LA size and to procedural success. The excess regurgitant blood entering in the LA may induce acutely or chronically a progressive rise in pulmonary pressure. The presence of TR even if it is mild, permits the estimation of systolic pulmonary arterial pressure. Recommendation for mitral valve repair is a class IIa when PASP is 50 mm Hg at rest.

48
Key point When MR is more than mild MR, providing LVD , LVV , LVEF as well as the LAD (preferably LAV) and the PASP in the final echocardiographic report is mandatory. The assessment of regional myocardial function (systolic myocardial velocities, strain, strain rate) is reasonable particularly in asymptomatic patients with severe organic MR and borderline values in terms of LV EF(60–65%) or LV ESD (closed to 40 mm or 22 mm/m2).
 and the PASP in the final echocardiographic report is mandatory. The assessment of regional myocardial function (systolic myocardial velocities, strain, strain rate) is reasonable particularly in asymptomatic patients with severe organic MR and borderline values in terms of LV EF(60–65%) or LV ESD (closed to 40 mm or 22 mm/m2).")
49
Exercise Echo in Ischemic MR
Exercise Echocardiography in Ischemic Mitral RegurgitationApical 4-chamber views of color-flow Doppler and proximal flow-convergence region (left panels) are shown in a patient with ischemic mitral regurgitation (MR) along with the systolic tricuspid regurgitation velocity (right panel). With exercise, there is a major increase in both the severity of mitral regurgitation and the estimated pulmonary artery systolic pressure. ERO = effective regurgitant orifice measured by the proximal isovelocity surface area; R Vol = regurgitant volume; TTPG = systolic transtricuspid pressure gradient. Exercise Echo in Ischemic MR Picano, E. et al. J Am Coll Cardiol 2009;54: Copyright ©2009 American College of Cardiology Foundation. Restrictions may apply.
 are shown in a patient with ischemic mitral regurgitation (MR) along with the systolic tricuspid regurgitation velocity (right panel). With exercise, there is a major increase in both the severity of mitral regurgitation and the estimated pulmonary artery systolic pressure. ERO = effective regurgitant orifice measured by the proximal isovelocity surface area; R Vol = regurgitant volume; TTPG = systolic transtricuspid pressure gradient. Exercise Echo in Ischemic MR. Picano, E. et al. J Am Coll Cardiol 2009;54: Copyright ©2009 American College of Cardiology Foundation. Restrictions may apply.")
50
Key point Exercise echocardiography is useful in asymptomatic
patients with severe organic MR and borderline values of LV ejection fraction (60–65%) or LV end-systolic diameter (closed to 40 mm or 22 mm/m2). The absence of contractile reserve could identify patients at increased risk of cardiovascular events. Moreover, exercise echocardiography may also be helpful in patients with equivocal symptoms out of proportion of MR severity at rest.
 or LV end-systolic diameter. (closed to 40 mm or 22 mm/m2). The absence of contractile. reserve could identify patients at increased risk of cardiovascular events. Moreover, exercise echocardiography. may also be helpful in patients with equivocal symptoms. out of proportion of MR severity at rest.")
51
Echocardiographic parameters used to quantify MR severity ,recording , advantages and limitations

52
Other abnormalities are non-specific of significant MR
Parameters Recording Usefulness/ Advantages Limitations MV Morphology • Visual assessment • Multiple views • Flail valve or ruptured PMs are specific for significant MR Other abnormalities are non-specific of significant MR Colour – flow MR jet • Optimize colour gain / scale • Evaluate in two views • Need BP evaluation • Ease of use • Evaluate the spatial orientation of MRJ • Good screening test for mild vs severe MR • Can be inaccurate for estimation of MR severity • Influenced by technical and hemodynamic factors • Underestimate eccentric jet

53
Vena Contracta ( VC ) width Parameters Recording Usefulness/
Advantages Limitations Vena Contracta ( VC ) width • 2 orthogonal planes PT-LAX ,AP-4CV • Optimize colour gain / scale • Identify the 3 components of MRJ VC,PISA,MRJ in LA • Reduce the colour sector size and imaging deapth to maximum frame rate • Zoom • Use the cine – loop to find the best frame for measurement • Measure the smallest VC •Relatively quick and easy • Relatively independent of hemodynamic and instrumentation factors • Not affected by other valve leak • Good for extremes MR mild vs severe • Can be used for eccentric jet • Not valid for multiple jets • Small values , small errores lead to large %error • Intermediate values need confirmation • Affected by systolic changes in regurgitant flow
 width. • 2 orthogonal planes PT-LAX ,AP-4CV. • Optimize colour gain / scale. • Identify the 3 components of MRJ VC,PISA,MRJ in LA. • Reduce the colour sector size and imaging deapth to maximum frame rate. • Zoom. • Use the cine – loop to find the best frame for measurement. • Measure the smallest VC. •Relatively quick and easy. • Relatively independent of hemodynamic and instrumentation factors. • Not affected by other valve leak. • Good for extremes MR mild vs severe. • Can be used for eccentric jet. • Not valid for multiple jets. • Small values , small errores lead to large %error. • Intermediate values need confirmation. • Affected by systolic changes in regurgitant flow.")
54
PISA Method Parameters Recording Usefulness/ Advantages Limitations
•AP-4CV •Optimize CFI of MR •Zoom the image of the MR Valve •Decrease the Nyquist limit (CF zero baseline) •With the cine mode select the best PISA •Display the colour off and on to visualize the MRO •Measure the PISA radius at mid systole •Measure MR peak velocity and TVI (CW ) •Calculate flow rate ,EROA, R Volume • Can be used in eccentric jet • Not affected by aetiology of MR or other valve leak • Quantitative estimate lesion severity ( EROA ) • Quantitative estimate volume overload R Volume • Flow convergence at 50 cm/s alerts to significant MR •PISA shape affected by:- ─Aliasing velocity ─Non circular orifice ─ Systolic changes in regurgitant flow ─Adjacent structure •PISA is more a hemi-ellipse •Errors in PISA radius measurements are squared •Inter – observer variability •Not valid for multiple jets
 •With the cine mode select the best PISA. •Display the colour off and on to visualize the MRO. •Measure the PISA radius at mid systole. •Measure MR peak velocity and TVI (CW ) •Calculate flow rate ,EROA, R Volume. • Can be used in eccentric jet. • Not affected by aetiology of MR or other valve leak. • Quantitative estimate lesion severity ( EROA ) • Quantitative estimate volume overload R Volume. • Flow convergence at 50 cm/s alerts to significant MR. •PISA shape affected by:- ─Aliasing velocity. ─Non circular orifice. ─ Systolic changes in regurgitant flow. ─Adjacent structure. •PISA is more a hemi-ellipse. •Errors in PISA radius measurements are squared. •Inter – observer variability. •Not valid for multiple jets.")
55
• Quantitative estimate lesion severity (EROA )
Parameters Recording Usefulness/ Advantages Limitations Doppler Volumetric Method ( PW ) Flow across the MV ( AP- 4CV ) • Measure the mitral inflow by placing the PW sample volume at MV annulus • Measure the MV annulus diameter at the maximal opening of the MV ( 2-3 frames after the end – systole ) • Quantitative estimate lesion severity (EROA ) And Volume overload = RV • Valid in multiple jets •Time consuming •Requires multiple measurements sources of errors • Not applicable in case of significant AR ( use PVF ) • Difficult to asses MAD and MV inflow in case of calcific MV or MAC •Affected by SV location MV inflow
 Flow across the MV. ( AP- 4CV ) • Measure the mitral inflow by placing the PW sample volume at MV annulus. • Measure the MV annulus diameter at the maximal opening of the MV ( 2-3 frames after the end – systole ) • Quantitative estimate lesion severity (EROA ) And. Volume overload = RV. • Valid in multiple jets. •Time consuming. •Requires multiple measurements sources of errors. • Not applicable in case of significant AR ( use PVF ) • Difficult to asses MAD and MV inflow in case of calcific MV or MAC. •Affected by SV location MV inflow.")
56
• Quantitative estimate lesion severity (EROA )
Parameters Recording Usefulness/ Advantages Limitations Doppler Volumetric Method ( PW ) Flow across the AV • Measure the LVOT flow by placing the PW SV 5 mm below the aortic cusp (AP – 5 CV ) • Measure the LVOT diameter ( PT-LAX View ) • Quantitative estimate lesion severity (EROA ) And Volume overload = RV • Valid in multiple jets •Time consuming •Requires multiple measurements sources of errors • Not applicable in case of significant AR ( use PVF ) • Difficult to asses MAD and MV inflow in case of calcific MV or MAC
 Flow across the. AV. • Measure the LVOT flow by placing the PW SV 5 mm below the aortic cusp (AP – 5 CV ) • Measure the LVOT diameter ( PT-LAX View ) • Quantitative estimate lesion severity (EROA ) And. Volume overload = RV. • Valid in multiple jets. •Time consuming. •Requires multiple measurements sources of errors. • Not applicable in case of significant AR ( use PVF ) • Difficult to asses MAD and MV inflow in case of calcific MV or MAC.")
57
Simple , easily available
Parameters Recording Usefulness/ Advantages Limitations CW MR jet profile A 4 CV Simple , easily available • Qualitative , complementary finding • Complete signal difficult to obtain in eccentric jet Peak E velocity • Apical 4 – CV • SV of PW places at MV leaflet tips • Simple , easily available • Dominant A- wave almost exclude severe MR • Affected by LAP ,AF, LV relaxation •Complementary finding

58
Pulmonary vein flow LA and LV size Parameters Recording Usefulness/
Advantages Limitations Pulmonary vein flow • A 4 CV SV of PW places into the Pulmonary Vein • Interrogate the different PV when possible • Simple • Systolic flow reversible is specific for severe MR • Affected by LAP and AF • Not accurate if MRJ directed into sampled vein LA and LV size Use preferably the Simpson method • Dilatation sensitive for chronic significant MR • Normal size almost exclude chronic significant MR • Dilatation observed in other conditions ( non-specific ) • May be normal in acute MR
 • May be normal in acute MR.")
59
MCQs

60
VC width and or PISA method Color – flow MRJ PVF and Peak E velocity
In patients with MR and AF the most reliable method for assessment of severity are the following except : VC width and or PISA method Color – flow MRJ PVF and Peak E velocity

61
VC width and or PISA method Color – flow MRJ PVF and Peak E velocity
In patients with MR and AF the most reliable method for assessment of severity are the following except : VC width and or PISA method Color – flow MRJ PVF and Peak E velocity

62
VC width and or PISA method Doppler Volumetric method PW
In patients with MR and significant AR the most reliable method for assessment of severity are the following except : VC width and or PISA method Doppler Volumetric method PW Color – flow MRJ

63
VC width and or PISA method Doppler Volumetric method PW
In patients with MR and significant AR the most reliable method for assessment of severity are the following except : VC width and or PISA method Doppler Volumetric method PW Color – flow MRJ

64
In patients with MR eccentric jet the method which can be used for assessment of severity is :
VC width and or PISA method Doppler Volumetric method ( PW ) Color – flow MRJ
 Color – flow MRJ.")
65
In patients with MR eccentric jet the method which can be used for assessment of severity is :
VC width and or PISA method Doppler Volumetric method ( PW ) Color – flow MRJ
 Color – flow MRJ.")
66
Doppler Volumetric method PW Color – flow MRJ
In patients with multiple jets the valid method for assessment of severity is : VC width PISA method Doppler Volumetric method PW Color – flow MRJ

67
Doppler Volumetric method PW Color – flow MRJ
In patients with multiple jets the valid method for assessment of severity is : VC width PISA method Doppler Volumetric method PW Color – flow MRJ

68
Mild MR Moderate Moderate to severe Severe
In patient with MR and VC = 5 mm TVI Mit /TVI Ao =1.2 EROA= 25 mm2 Rvol 35 Ml the severity is : Mild MR Moderate Moderate to severe Severe

69
Mild MR Moderate Moderate to severe Severe
In patient with MR and VC = 5 mm TVI Mit /TVI Ao =1.2 EROA= 25 mm2 Rvol 35 Ml the severity is : Mild MR Moderate Moderate to severe Severe

70
Mild Moderate Moderate to severe Severe
In patient with MR and VC = 6 mm TVI Mit /TVI Ao =1.4 EROA= 35 mm2 Rvol 75 mL the severity is : Mild Moderate Moderate to severe Severe

71
Mild Moderate Moderate to severe Severe
In patient with MR and VC = 6 mm TVI Mit /TVI Ao =1.3 EROA= 35 mm2 Rvol 55 mL the severity is : Mild Moderate Moderate to severe Severe

72
Mitral regurgitation Simultaneous pressure recording High LVEDP
Giant V wave max Pressure 85 mmHg Systolic PG LV-LA =15 mmHg

73
What cardiac catheterization will give us more informations in MR ?

74
Thank you

Similar presentations





 CPP = aortic diastolic.>")


 FOR MITRIAL REGURGITATION>")






 For Broker/Dealer Use Only.>")



