Download presentation
Presentation is loading. Please wait.

1
Surgery on Crohn’s Disease
Joint Hospital Surgical Grand Round Dennis KY Ngo Department of Surgery Prince of Wales Hospital

2
Background Chronic transmural inflammatory process that can affect GI tract anywhere, also associated with extraintestinal manifestation Commonly : ileal, ileocolic, colonic and perianal disease Diagnosis based on macroscopic, histologic and radiological features

3
Incidence More common in Caucasian Rate is lower in Asia.
5-6 per population ( North American, northern Europe ) Rate is lower in Asia. However, there is increasing trend 1 per population ( Hong Kong ) 3 fold over the past decade Leong at el. Inflammatory Bowel Diseases. 10(5):646-51, 2004 Sep.
 Rate is lower in Asia. However, there is increasing trend. 1 per population ( Hong Kong ) 3 fold over the past decade. Leong at el. Inflammatory Bowel Diseases. 10(5):646-51, 2004 Sep.")
4
What is the surgeons’ role in treating this benign disease ?
Increasing incidence of Crohn’s disease annually, more and more people will keep an eye on the treatment modality, esp in these young age group population. Apart from medical therapy, What is the surgeons’ role in treating this benign disease ?

5
M/22 Good past health Presented in March 2006 with right iliac fossa pain associated with diarrhoea and weight loss for 1 month

6
Colonoscopy on 8 March 2006 Inflammation and ulcers at caecum and ileocaecal valve Terminal ileum could not be intubated because of swollen ileocaecal valve Biopsy: Crohn’s disease Seen by Gastroenterologists on 10 March 2006; Salofalk 1 g TDS and prednisolone started

7
Readmission as Emergency
Readmission on 12 March 2006 Increased right iliac fossa pain for 1 day Fever C Pulse rate: 100/minute CXR: no infradiaphragmatic free gas WCC: 13.5 x 109/L

8
Thickened terminal ileum and caecum

9
Pockets of free gas

10
Pocket of free gas

11
Ileocaecal Crohn’s disease with peritonitis and suspected perforation
Emergency laparoscopic-assisted right hemicolectomy

12
Cobblestone appearance

13
~ 80% will require surgery irrespective of its site
Farmer et al. Gastroenterology 1985; 30:990-5 Bernell et al. Ann Surg 2000; 231:38-45 Surgery Curative ( potentially involve the entire intestine ) Recurrence (invariable) Potential benefits of surgery Symptoms relief Improved nutritional status Reduced dependence of medication Development of Surgical procedures focus on treating the complications as well as conserving the bowel length
 Recurrence (invariable) Potential benefits of surgery. Symptoms relief. Improved nutritional status. Reduced dependence of medication. Development of Surgical procedures focus on treating the complications as well as conserving the bowel length.")
14
Indications of Surgery
Failed medical treatment Growth retardation (Children) Complication of steriod and other medical therapy Complications Obstruction Perforation Fistula formation Abscess formation Bleeding Toxic colitis Malignancy
 Complication of steriod and other medical therapy. Complications. Obstruction. Perforation. Fistula formation. Abscess formation. Bleeding. Toxic colitis. Malignancy.")
15
Management of Stenosis
Non-operative Balloon dilatation Operative Bypass Strictureplasty Resection

16
Balloon dilatation 55 patients, managed by endoscopic dilatation
18mm balloon, followed by 20/25mm Inflated for 2min ( repeat 2-6 inflations) 90% successful dilatation 8% perforation rate Mean FU time : 33.6 months 18 patient need second dilatation at 1.5 year Long term successful rate : 62% Operation rate : 38% Couckuyt H, et al. Gut 1995;36:
 90% successful dilatation. 8% perforation rate. Mean FU time : 33.6 months. 18 patient need second dilatation at 1.5 year. Long term successful rate : 62% Operation rate : 38% Couckuyt H, et al. Gut 1995;36:")
17
Bypass Popular in the past (1930-1950) Problems :
Active disease in the retained segment Abscess / Fistula / Perforation / increased rate of malignancy of bypassed segment No place in modern day surgery, Except Gastroduodenal Crohn’s with hostile adhesions to adjacent organs preventing a safe excision

18
Strictureplasty Mainly used for small bowel
Good symptomatic relief and bowel sparing Aim at conserving small bowel for the fear of short bowel Ideal for short stricture Can be performed for single or multiple strictures

19
Contraindication Perforation of bowel
Present of abscess, inflammation and fistula Multiple strictures over a short segment of bowel Inability to perform tension-free suture line Profound hypoalbuminemia Generally not to be performed on large bowel High recurrence rate High risk of malignancy

20
Technique Longitudinal incision with extension to normal looking bowel
Inspection of lumen, biospy of suspicious lesion ( R/O malignancy ) Stricture < 10cm : close in Heineke-Miculicz fashion Stricture 10-20cm : repaired with Finney strictureplasty
 Stricture < 10cm : close in Heineke-Miculicz fashion. Stricture 10-20cm : repaired with Finney strictureplasty.")
21
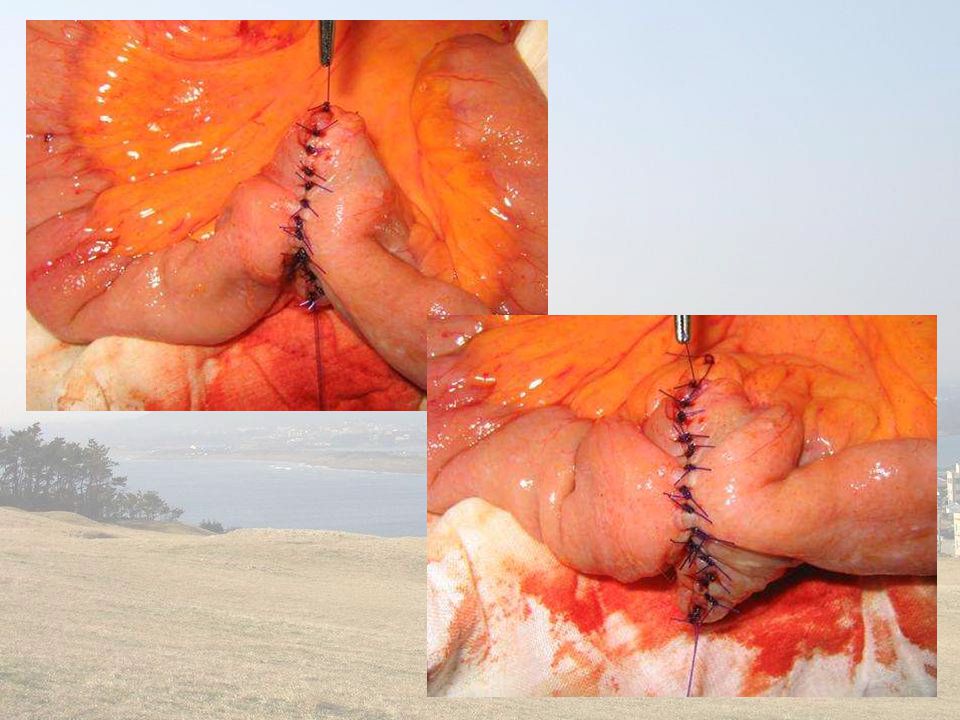
Heineke Miculicz Strictureplasty

24
Recurrence & Reoperation
100 patients included for strictureplasty Mean FU 85.1 months ( months ) Overall reoperation rate : 56% N. S. Fearnhead et al. British Journal of Surgery 2006;93: 162 patients Reoperative rates (5 years) : 31% Ozuner et al Dis Colon Rectum 1996
 Overall reoperation rate : 56% N. S. Fearnhead et al. British Journal of Surgery 2006;93: patients. Reoperative rates (5 years) : 31% Ozuner et al Dis Colon Rectum")
25
Majority – new segments of stricture
Recurrence at strictureplasty site is rare – 3.7% Stebbing et al Br J Surg 1995

26
Resection Limited resection to achieve the goal of symptomatic relief, while preserving the bowel length Resect macroscopically diseased bowel without concern for microscopic disease Recurrence is unaffected the width of the margin of resection from marcroscopically involved bowel Recurrence rate not increase when microscopic disease still present in the resection margin Fazio et al. Annals of Surgery 1996;224:

27
Intestinal Fistula Internal fistula (30-40% CD)
Ilijevski et al Eur J Surg 1997 General surgical principle Resect the 10 diseased segment Close the 20 involved organs

28
Colonic operation Intractable disease ( failed medical therapy )
Severe colitis Bleeding Malignancy Involving entire colon and rectum Gold standard : proctocolectomy and ileostomy

29
Less extensive resection
Subtotal colectomy + mucous fistula Total colectomy + ileorectal anastamosis Segmental colonic resection

30
Role of laparoscopic surgery
Longer operation Higher cost Faster recovery Less scarring

31
Application of laparoscopic technique to Crohn’s disease
Benign disease Relatively young patients (back to normal duty with economic consideration) Better cosmesis Risk of adhesive intestinal obstruction / incisional hernia Possibility of multiple surgery Ozuner D et al Dis Colon Rectum 1996; 39:
 Better cosmesis. Risk of adhesive intestinal obstruction / incisional hernia. Possibility of multiple surgery. Ozuner D et al Dis Colon Rectum 1996; 39:")
32
Development Stoma creation (ileostomy / colostomy) Earliest indication
Braga M et al Ann Surg 2002; 236: Limited segmental SB resection Ileocaecal resection More complex / recurrent disease (fistula, phlegmon, etc) Emergency setting
 Emergency setting.")
33
Meta-analysis for ileocaecal resection in Crohn’s
783 patients (Lap: 338) 15 studies ( ) 1 RCT; 6 prospective; 8 retrospective Conversion rate: 6.8% Tilney HS et al Surgical Endos May 2006
 15 studies ( ) 1 RCT; 6 prospective; 8 retrospective. Conversion rate: 6.8% Tilney HS et al Surgical Endos May")
34
Significant difference Lap vs Open
OT time (longer in Laparoscopic group) ~30 mins Post-op recovery (faster in Laparoscopic group) Tolerates full diet (1.47 days) First flatus (0.68 days) First bowel motion (0.58 days) Shorter hospital stay (2.97 days)
 ~30 mins. Post-op recovery (faster in Laparoscopic group) Tolerates full diet (1.47 days) First flatus (0.68 days) First bowel motion (0.58 days) Shorter hospital stay (2.97 days)")
35
Similar outcome Blood loss Post-op complications Return to work
Anastomotic leakage Wound infection Bowel obstruction Intra-abd abscess Return to work

36
Issues addressed Technical feasibility Safety
Immediate operative outcomes

37
Postoperative course ( our case )
First bowel motion: D3 Fluid diet resumed: D4 DAT: D6 Full ambulation: D4 Home: D9 No complication Wound length: 8 cm

38
Conclusion Surgical role in Crohn’s disease is
Not to cure the disease treat the complications with improvement of quality of life of these young group of patient Development of laparoscopic surgery Better cosmesis and body image Faster recovery Less adhesion for ease of reoperation latter

39
Thank you

Similar presentations



,>")
















