Download presentation
Presentation is loading. Please wait.

1
Causal Diagrams in Psychopathology: Applications in Models of Causality and Clinical Decision-Making Stephen N. Haynes Stephen N. Haynes University of Hawai’i, USA University of Málaga, Spain

2
IV Workshop on Causal Reasoning in Clinical Decision Making April, Gracias a Pedro L. Cobos et Otros Antonio Godoy

3
A presentation about A challenging context for clinical decisions: Understanding complex clinical cases in psychopathology Making appropriate treatment decisions with complex cases Communicating case formulations to others

4
Application of Causal Diagrams in Psychopathology to Aid Causal Reasoning and Clinical Decisions
Idiographic (variance within a person across time) -- the main focus! Nomothetic (variance across persons) Not about what I know, investigate, or teach About what I’m thinking about and learning
 -- the main focus! Nomothetic (variance across persons) Not about what I know, investigate, or teach. About what I’m thinking about and learning.")
5
My Main Points? Causal diagrams Help explain complex behavior problems
Help in functional analysis and Clinical Case Formulation Provide an alternative, more precise, clinically useful language in causal models of psychopathology and in clinical case formulation (CCF)
")
6
Causal Diagrams: Help estimate relative magnitude of effect of various treatment foci, given component causal judgments Encourage Parsimony in causal models in psychopathology and CCF Help detect less obvious functional relations in psychopathology and treatment Guide focus of clinical research

7
Causal Diagrams: Help evaluate between-clinician agreement in CCF judgments Help examine congruence between treatment mechanisms and causal relations for a client

8
Causal Diagrams: Encourage a systematic evaluation by the clinician of component his/her component clinical decisions and judgments Help educate about clinical decisions, psychopathology, CCF (supervision, graduate training, other professionals)
")
9
Causal Diagrams Emphasize importance of Multiple causal paths Bidirectional causal relations Moderator Variables Mediator Variables In psychopathology and clinical case formulation

10
One goal of presentation:
to promote a standardized, formalized, quantitative use of causal diagrams in psychopathology and clinical case formulation Discuss limitations, challenges in use of causal diagrams

11
More on Causal Diagrams
Some examples of causal diagrams--> (some Idiographic (one person, across time), some nomothetic (across persons) Just note--elements and structures of diagrams
, some nomothetic (across persons) Just note--elements and structures of diagrams.")
12
Cognitive CCF Causal Diagram for Depressed Client; Mumma
Example of a CBCF Situational triggers Internal and external Idiosyncratic cognitive schema Distress Others laughed at or ridiculed me/did not appreciate my work. Worthlessness … Concentration difficulties; worry Was reminded about limitations of my job Inadequate/incompetent/ trapped/hopeless job Depression Was reminded about limitations of living in ___ Anger Others hurting/rejecting and can’t be trusted - Talked or thought of talking to others about my feelings. Anger inhibition: “Gentle- men don’t get angry.” Cognitive CCF Causal Diagram for Depressed Client; Mumma

13
Armed conflicts in Nicaragua

14
CCF causal diagram for depressed mood
Χ2(df = 531) = , RMSEA = .083, CFI = .89. Today’s Distress Item Parcels .75***.75*** .75*** GD:Mixed .79***.79*** .79*** .87*** .87*** .87*** Anger ICS 1 Worthlessness ICS 3 Job: Inadequate Trapped ICS 2.1/3 Others Hurtful, Rejecting ICS 2.2 Anger/Inhibition .83*** -.08 .79*** ** .69*** .01 .28* .59*** *** .92*** .57*** .82*** .88*** .98*** .88*** .82*** *** Today’s Cognition Item Parcels dd ee ff aa bb cc gg hh ii GD: Depressed a b i h j d c e f g -.26*** -.19* -.28* -.20** Mumma & Mooney, 2007b: Figure 3. CDFA model for Clinician 1’s CCF for 4 ICS and 3 distress variables: GD: Depressed, GD: Mixed, and Anger: standardized solution. Χ2(df = 531) = , RMSEA = .083, NNFI = .85, CFI = Concurrent regressions from the ICSs to the distress latent variables are shown with straight lines. Dynamic loadings of ICS item parcels are shown with dotted lines. Note: Lagged regressions between the ICSs, disturbances of the ICS and distress factors (and their covariances within each set), and error variances for item parcels are not shown. 14
 = , RMSEA = .083, CFI = .89. Today’s Distress Item Parcels. .75***.75*** .75*** GD:Mixed. .79***.79*** .79*** .87*** .87*** .87*** Anger. ICS 1 Worthlessness. ICS 3. Job: Inadequate Trapped. ICS 2.1/3. Others Hurtful, Rejecting. ICS 2.2. Anger/Inhibition. .83*** *** ** .69*** * .59*** .60*** .92*** .57*** .82*** .88*** .98*** .88*** .82*** .84*** Today’s Cognition Item Parcels. dd ee ff aa bb cc gg hh ii. GD: Depressed. a b i h j d c e f g. -.26*** -.19* -.28* -.20** Mumma & Mooney, 2007b: Figure 3. CDFA model for Clinician 1’s CCF for 4 ICS and 3 distress variables: GD: Depressed, GD: Mixed, and Anger: standardized solution. Χ2(df = 531) = , RMSEA = .083, NNFI = .85, CFI = .89. Concurrent regressions from the ICSs to the distress latent variables are shown with straight lines. Dynamic loadings of ICS item parcels are shown with dotted lines. Note: Lagged regressions between the ICSs, disturbances of the ICS and distress factors (and their covariances within each set), and error variances for item parcels are not shown. 14.")
15
9 yr-old boy; home and classroom problems
CCF Causal Diagram for Oppositional/Defiant Behs

16
Schematic Causal Diagram for comorbidity

17
An example of Functional Analytic Clinical Case Model
Functional Analysis of Violent Behavior in Inpatient Units An example of Functional Analytic Clinical Case Model CCF Causal Diagram for verbal aggression

18
Ahn, Kim et al., 2005

19
CCF Causal Diagram child oppositional/attentional probs
unspecific commands Not complying with adult requests deficits in parenting skills inconsistent reinforce-ments Whining, grumbling (at home) family disorganization high neg. comments/ low pos. comments child poor commun. skills Inattentive and off-task behavior (at school) varied sleep schedule child unprepared for school Incomplete school work Genetic/ Family history of ADHD child inattention
 family disorganization. high neg. comments/ low pos. comments. child poor commun. skills. Inattentive and off-task behavior (at school) varied sleep schedule. child unprepared for school. Incomplete school work. Genetic/ Family history of ADHD. child inattention.")
20
William James

21
From William James: Talk to Teachers
From William James: Talk to Teachers ; Causal Model for Human Behavior

22
Leonardo da Vinci

23
(Causal model proving that
there is water on the moon)
")
24
Common Elements and Characteristics of Causal Diagrams Across Disciplines
Illustrate complex functional relations among multiple variables (sometimes causal) Input variables (causes of behavior problems) Output variables (Behavior problems Illustrate possible causal variables Some show strength of relation Most show direction of causal relation Multiple formats for diagrams
 Input variables (causes of behavior problems) Output variables (Behavior problems. Illustrate possible causal variables. Some show strength of relation. Most show direction of causal relation. Multiple formats for diagrams.")
25
What is necessary in causal diagrams in Psychopathology and Functional Analysis?
Standardized presentation of elements of psychopathology Emphasis on Important elements relevant to the explanation of the behavior problems and clinical decisions Amenability to quantification, to model effects of clinical decisions

26
Causal Diagrams in Functional Analytic Clinical Case Diagrams (FACCD)
FA Focus on “important, modifiable causal variables and functional relations relevant to a person’s behavior problems”

27
FACCD = Causal diagram for a functional analysis a subset of standardized path and causal diagrams; often used in physics, agronomy, economics, oceanography, (informally in mind-mapping).
.")
28
Goal: To help clinician decide where for focus treatment (which causal variables should be the focus of treatment)
")
29
18 Elements In, and Outcomes from, a FACCD (Functional Analytic Clinical Case Diagram) (18 clinical judgments; All Leading to Estimates of the Relative Magnitude of Effect of Various Treatment Foci For an Individual Client; but there are more factors affecting these decisions)
 (18 clinical judgments; All Leading to Estimates of the Relative Magnitude of Effect of Various Treatment Foci For an Individual Client; but there are more factors affecting these decisions)")
30
1. Multiple client behavior problems
Note: Methods of deriving these judgments are discussed in references at end Note: variables are abstractions. Consider Ys = panic episodes, alcohol overuse, nightmares, aggressive behaviors, social anxiety, manic episodes, self-injury,etc.

31
Y1 Y2 Y3

32
2 Relative “Importance” of behavior problems. Estimated by:
Risk of harm to self Risk of harm to others Personal distress Qualitative ratings of importance (by client, therapist, others) Note: relevant to estimating magnitude of effect of intervention
 Note: relevant to estimating magnitude of effect of intervention.")
33
Y1 More Important Y2 Less Important Y3

34
3 Forms of functional relations between behavior problems

35
Y1 Correlated Non-causal Y2 Unidirectional Causal Y3 Bidirectional Causal

36
4. Strength of functional relations among behavior problems
Degree of “Influence” Conditional probability of occurrence Time-lagged correlation Estimated strength of manipulation effects

37
Y1 Stronger Y2 Weaker Y3

38
5. Consequences of behavior problems
Health risks Functional impairment Economic, legal risks Effects on others (e.g., risks associated with financial decisions during manic periods, legal risks associated with drug use)
")
39
Y1 Z1 Y2 Y3

40
Note effect on treatment decisions for just a few elements of FACCD!
If importance, form, direction were different, different focus could be indicated to achieve maximum magnitude of benefit for this client

41
6. Causal Variables Broadly defined: empirically supported variables where changes lead to changes in behavior problem ( or other variables) E.g., positive response contingencies, antecedent stimuli, avoidance, settings/contexts, negative ruminations, elevated adrenal responses, conditional emotional responses, outcome expectations, reduction in aversive states, life stressors, neurotransmitter receptor density, communication skills, etc

42
X4 X1 Y1 Z1 X2 Y2 X3 Y3

43
7. Modifiability of causal variables
“clinical utility” relatively unmodifiable: brain injury, early traumatic life experiences; genetic vulnerability, early learning) no effective treatments (e.g., some medical disorders, some neurological deficits) External factors--cooperation from partner, staff cooperation, unavoidable life stressors) Client factors--cognitive abilities, treatment adherence - interference
 no effective treatments (e.g., some medical disorders, some neurological deficits) External factors--cooperation from partner, staff cooperation, unavoidable life stressors) Client factors--cognitive abilities, treatment adherence - interference.")
44
More Modifiable Less Modifiable Unmodifiable

45
X4 X1 Y1 Z1 X2 Y2 X3 Y3

46
8. Forms of functional relations between causal variables and behavior problems

47
Correlated Unidirectional Bidirectional Noncausal Causal Causal

48
X4 X1 Y1 Z1 X2 Y2 X3 Y3

49
9. Strength of Functional/Causal Relations between causal variables and behavior problems
Stronger Weaker

50
X4 X4 X1 Y1 Z1 X2 Y2 X3 Y3

51
10-11 Form and Strength of causal relations among causal variables

52
X4 X4 X1 Y1 Z1 X2 Y2 X3 Y3

53
12-16: Additional Types of Causal Variable and Causal Relations:
Moderating variable Mediating variable Hypothetical causal variable Interactive causal relations Causal chains

54
Interactive Causal Mediating Variable Causal Chain Hypothetical Causal Variable Moderating Variable

55
Moderating variable (affects the strength of relationship between two other variables; Can be buffering, protective, etc.)
")
56
X4 X4 X1 Y1 Z1 X2 Y2 X5 X3 Y3

57
Mediating Variables: “Explain/account for” the relations between two other variables (e.g., why/how does X1 ---> Y?) X1 Y X3 X2

58
X4 X4 X1 Y1 Z1 X2 Y2 X5 X3 Y3

59
Hypothetical causal variable and relationship (not measured, inferred, to be measured, indicated in Nomothetic research) Hypothetical Causal Variable Hypothetical Causal Relation

60
X6 X4 X4 X1 Y1 Z1 X2 Y2 X5 X3 Y3

61
Causal chains (distal/proximal)
Can be “Mediated” causal variable/relation also (one that “explains” a causal relation) X1 X2 X3 Y1
 X1. X2. X3. Y1.")
62
X6 X4 X4 X1 Y1 Z1 X2 Y2 X5 X7 X3 Y3

63
17. Direction of Functional Relations

64
X6 X4 X4 X1 ( X1 = X2) Y1 - Z1 X2 Y2 X5 X7 X3 Y3
 Y1 - Z1 X2 Y2 X5 X7 X3 Y3")
65
18. Temporal Relations Among Variables
Temporal order flows from left to right, with earlier events to the left of later events. Thus, in the next figure, variable X7 occurs before variable X3 Note the erroneous causal inferences that might result

66
X7 Y2 X3 Y3

68
Benefits of Idiographic Causal Diagrams (FACCDs) for Clinical Decision-Making
Can estimate treatment focus with greatest magnitude of effect for client Can indicate where additional assessment is needed Can indicate potentially important but unmeasured causal variables

69
Qualitative Implications, 2
Emphasizes focus on important, modifiable variables Encourages parsimony in communicating FA to others Models potential effects of interventions: (similar to “modeling” approaches in physics, oceanography, economics, agronomy)
")
70
Qualitative Implications, 3
Indicates omitted variables and functional relations: nomothetically based potential causal relations that are not operational for a particular client Has “face value” for other professionals (They can understand why you want to pursue a particular intervention strategy) Emphasizes importance of good quality assessment for the most valid judgments
 Emphasizes importance of good quality assessment for the most valid judgments.")
71
Qualitative Implications, 4
Can be used in a constructive, positive manner. FACCDs can focus on client goals, values, strengths. Mandates knowledge of treatment mechanisms for various treatments which, in turn, can guide assessment efforts It promotes a logical, sequential, linear approach to clinical case formulation.

72
Qualitative Implications, 5
It requires that the clinician examine his or her individual clinical judgments (e.g., does this patient’s marital conflict strongly affect his use of alcohol) Can suggest possible outcomes if natural changes occur in patients’ environment, behavior, thoughts, emotions
 Can suggest possible outcomes if natural changes occur in patients’ environment, behavior, thoughts, emotions.")
73
Quantification of Causal Diagrams
***Quantification of Causal Diagrams***: Assigning Quantitative Values to the Elements of an Idiographic Causal Diagram (Functional Analytic Clinical Case Diagram)
")
74
Importance of behavior problems
Sample Weights: Importance of behavior problems 1= mild 2=moderate 4=severe Strength of functional relations .2 =weak .4 =moderate .8 =strong Modifiability of Causal variable .2 =mild .8 = strong

75
.2 Y1 X1 (1) .2 X4 .4 Y2 X2 (2) .4 .8 Y3 X3 (4) .8
 .2 X4 .4 Y2 X2 (2) Y3 X3 (4) .8")
76
(except for Sensitivity Analysis, discussed later)
Absolute values have no effect on clinical judgments derived from quantitative analyses within the FACCD Only relative values (ratios) within a FACCD affect the judgments (as long as they are linear transformations), E.g., for modifiability ( ) = ( ) (except for Sensitivity Analysis, discussed later) And, more face value if they approximate expected true functional relations and values (importance, modifiability)
 within a FACCD affect the judgments (as long as they are linear transformations), E.g., for modifiability ( ) = ( ) (except for Sensitivity Analysis, discussed later) And, more face value if they approximate expected true functional relations and values (importance, modifiability)")
77
Assets of Causal Diagram Quantification 1 Estimating Relative Magnitude of Effect in FACCD
Allows the calculation of vector coefficients, to model intervention judgments Relative (within-person) Magnitude of Effect (ME) of one causal variable: ME(xi/yi) = ∑(xi/yi) (sum of all path coefficients from xi)
 Magnitude of Effect (ME) of one causal variable: ME(xi/yi) = ∑(xi/yi) (sum of all path coefficients from xi)")
78
25% increase in expected ME for X2
.8 .2 Y1 3 .2 .8 Y2 1 X2 .2 .8 ME(x1) = (.8 x .2 x 3) + (.8 x .2 x .2 x 1) = .51 ME(x2) = (.2 x .8 x 3) +(.2 x .8 x .2 x ) + (2. X .8 x 1) = .67 25% increase in expected ME for X2
 = (.8 x .2 x 3) + (.8 x .2 x .2 x 1) = .51. ME(x2) = (.2 x .8 x 3) +(.2 x .8 x .2 x ) + (2. X .8 x 1) = % increase in expected ME for X2.")
79
X6 X4 X4 X1 a b Y1 c f d e Z1 h X2 g Y2 X5 X5 i X3 Y3

80
X6 X4 X4 X1 .2 .2 .2 Y1 3 .8 .04 .2 .2 Z1 .8 X2 .8 .8 Y1 X5 .8 X5 .2 X3 Y3

81
Note 3 causal paths from X1 --> Y1 (some moderated and mediated
ME(x1/y1) = Direct Path = (.2 x .2 x 3) + Through X2 = (.2 x .2 x .8 x .2 x 3) + Interaction Path (with X2) = (.2 x .2 x 8 x .2 x 3) (.12) + (.02) + (.02) = .16 (relative magnitude of effect) Can then compare to other Path Coefficients for other causal variables
 = Direct Path = (.2 x .2 x 3) + Through X2 = (.2 x .2 x .8 x .2 x 3) + Interaction Path (with X2) = (.2 x .2 x 8 x .2 x 3) (.12) + (.02) + (.02) = .16 (relative magnitude of effect) Can then compare to other Path Coefficients for other causal variables.")
82
MEs can be estimated by analyzing graphical properties of the diagram (values) or performing symbolic derivations governed by the diagram (using algebra symbols) (Pearls, 1995) A benefit of quantification of causal diagrams (FACCDs): causal variables with multiple causal paths are particularly important in accounting for and modifying behavior problems
: causal variables with multiple causal paths are particularly important in accounting for and modifying behavior problems.")
83
Can estimate the likely effects of planned and unplanned changes in causal variables, or the introduction of new moderator, mediator variables. “What would happen if…?”

84
Adding “Uncertainty” The parameters of the elements in causal models are only estimates based in the best available evidence. Can establish domains of confidence in the outcome of our predictions and interventions Reflects measurement and judgment limitations In addition to “error” components in all causal diagrams (referring to unmeasured causal variables)
")
85
Uncertainty Analysis indicates the degree of uncertainty in the overall magnitude of effect associated with a causal variable (reflects the cumulative uncertainty in the causal model) draws attention to variables about which more information is needed to reduce their degree of uncertainty and increase confidence in the causal model
 draws attention to variables about which more information is needed to reduce their degree of uncertainty and increase confidence in the causal model.")
86
Uncertainty tolerance
the degree of uncertainty that can be tolerated depends on the importance of the judgments Whenever important judgments are being made, or when the negative consequences of an erroneous decision are severe, such as use of an invasive treatment with a patient, additional data should be acquired to reduce uncertainty

87
Uncertainty Analysis (adding confidence limits to parameter estimates)
X1 (.6-.8) (.2-.3) Y1 3 (.2-.6) (.6-8) Y2 1 X2 (.2-.6) (.5.8) ME(x1) = ((.6-.8) x (.2-.3) x 3) + ((.6-.8) x (.2-.3) x (.2-.6) x 1) = ME(x2) = ((.2-.6) x (.6-.8) x 3) +((.2-.6) x (.6-.8) x (.2-.6) x 1) + ((2.-.6) X (.5-.8) x 1) = (compared to .67 assuming no uncertainty)
 (.2-.3) Y1. 3. (.2-.6) (.6-8) Y2. 1. X2. (.2-.6) (.5.8) ME(x1) = ((.6-.8) x (.2-.3) x 3) + ((.6-.8) x (.2-.3) x (.2-.6) x 1) = ME(x2) = ((.2-.6) x (.6-.8) x 3) +((.2-.6) x (.6-.8) x (.2-.6) x 1) + ((2.-.6) X (.5-.8) x 1) = (compared to .67 assuming no uncertainty)")
88
Increasing Acceptability of Causal Diagrams: “Causal Relevance Diagrams”
When quantitative information is encoded in the elements (path coefficients, importance and modifiability ratings) of a causal diagram (Shafer, 1996)
 of a causal diagram (Shafer, 1996)")
89
Given a Legend, this causal path diagram is the same as…
X1 .8 .2 Y1 3 .2 .8 Y2 1 X2 .2 .8 Given a Legend, this causal path diagram is the same as…

90
This causal relevance diagram.
X1 Y1 Y2 X2 This causal relevance diagram. Sometimes more clinically acceptable and computationally identical

91
Assets of Causal Diagram Quantification 3: Illustrating the effects of changes in clinical judgments on MEs and optimal treatment foci

92
Moderating

93
Moderating

94
Moderating

95
Another benefit of quantification of causal diagrams (FACCDs): Makes the clinician question his/her judgments e.g.: Are the communication problems of a distressed couple twice as modifiable as their negative attributions about each other? Is a client’s depressive episodes twice as important as their overuse of alcohol?

96
Assets and Implications of Model Quantification 4
Assuming a content valid FACCD all appropriately focused interventions will be effective (compared to no intervention), but with differential magnitudes of effect Some supporting literature on increased ME with FACCD-focused treatments; only from SIBs
, but with differential magnitudes of effect. Some supporting literature on increased ME with FACCD-focused treatments; only from SIBs.")
97
Assets and Implications of Model Quantification 4
The Effects of Treatments With Multiple Mechanisms/Components Examples of treatment mechanisms/components Automatic negative self-statements in treatment of depression Identifications of emotions with anxiety disorders Communication training with distressed couple Alcohol outcome expectancies Guilt in sex-abuse (or assault) related PTSD Parental use of + reinforcement with child Experiential avoidance Desensitization in social anxiety reduction
 related PTSD. Parental use of + reinforcement with child. Experiential avoidance. Desensitization in social anxiety reduction.")
98
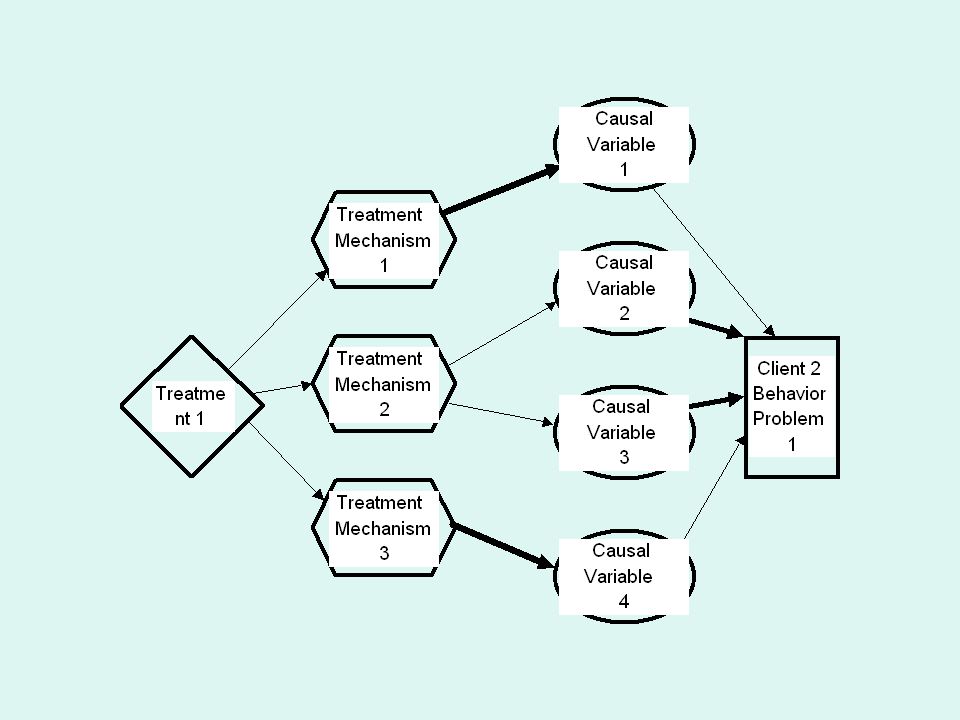
Model 1: A Good Match Between the Functional Analysis and the Treatment

100
Estimating Magnitudes of Effects
Assigning relative values to variables and paths Behavior problem importance: 10 Strong causal/functional relations: .8 Weak causal/functional relations: .2 Modifiability of causal variables: .8 (note; the strength, modifiability and estimates are only judgments by the clinician, informed by the outcome of assessment)
")
101
Solving for Paths for client 1:
Magnitude of Effect of this treatment, for this client, given these clinical judgments, is 10.4 (Note: value has no absolute meaning and is useful only for comparing effects of different clinical judgments using the same values for a client)
")
102
Model 2: A Less-Than-Optimal Match Between the Functional Analysis and the Treatment

104
Changes in Functional Analysis From 1st client
Different client--> Same behavior problem, causal variables, treatments, and treatment mechanisms. Only the strength of causal relations have been changed- Now: Major treatment mechanisms are relevant but do not match (are less congruent with) the most important causal relations
 the most important causal relations.")
105
Solving for Paths for client 2
Magnitude of Effect of this treatment, for this client, given these clinical judgments, is 5.1 About 1/2 of magnitude of effect for client 1

106
Model 3: The Magnitude of Effects for Two More Narrowly focused Treatment

108
Changes in Functional Analysis From Previous clients
Same client, causal variables, causal relations Two treatments, each more narrowly focused (fewer treatment mechanisms) Treatment 2 addresses strong causal relation Treatment 3 addresses weak causal relation
 Treatment 2 addresses strong causal relation. Treatment 3 addresses weak causal relation.")
109
Solving for Both Paths for client; Magnitudes of Treatment Effects:

110
Model 4: The Magnitude of Effects for a Broadly focused Treatment

112
Solving Paths for Broadly Focused Treatment
This treatment is the most effective because it addresses all causal variables Magnitude of effect is % greater than best of more focused treatments

113
Implications All validated treatment programs will be effective if they address any causal variable for a client (noted in “3”), given stability of other factors Relative Magnitudes of treatment effects will be affected by match between treatment mechanisms and causal variables operating for an individual treatment
, given stability of other factors. Relative Magnitudes of treatment effects will be affected by match between treatment mechanisms and causal variables operating for an individual treatment.")
114
Implications 2 Idiographic treatment (a treatment designed to match the clinical case formulation for the client) will often be more effective than standardized treatments
 will often be more effective than standardized treatments.")
115
Implications 3 Magnitude of treatment effect will be affected by match (congruence) between treatment mechanisms and causal variables operating for an individual client
 between treatment mechanisms and causal variables operating for an individual client.")
116
Implications 4 incremental treatment effectiveness for individualized treatment is affected by: The degree to which causes for a behavior problem differ across clients (in causal variables and the strength of relationships) Implications for treatment research Measure causal relations for client Look for match between causal relations and treatment mechanisms Group comparisons without examining treatment mechanisms and treatment-causal variable match are not optimally useful
 Implications for treatment research. Measure causal relations for client. Look for match between causal relations and treatment mechanisms. Group comparisons without examining treatment mechanisms and treatment-causal variable match are not optimally useful.")
117
Implications 5 The identification of potential treatments for a behavior problem can guide assessment foci (Godoy) e.g. if insomnia is problem: clinician should assess presleep thoughts, presleep physiological arousal, sleep hygiene, stimulus control factors (the mechanisms thought to underlie different treatments)
")
118
Assets and Implications of Model Quantification 5
Causal Diagrams and Calculating Inter-Clinician Agreement for FA and CCF Allows for a more refined analysis of specific areas of agreement and disagreement Agreement about client problems Agreement about causal variables Agreement about functional relations

120
Five possible agreements (omitting “modifiability” for this example)
one for each of the three causal variables (B, C, D) identified by both raters one for causal variable A (identified by clinician B) one for causal variable E (identified by clinician A)
 identified by both raters. one for causal variable A (identified by clinician B) one for causal variable E (identified by clinician A)")
121
A sample quantification of the degree of agreement:
“0” for no agreement or congruence “1” for weak agreement or congruence (e.g., Causal Variable C identified by both raters who disagree about its strength of relation with the BP “2” for strong agreement (e.g., Causal variable B; variable and strength of relation).
.")
122
The sum of these agreements 4 out of 10 (40%)
B=2 C=1 D=1 E=0 Can examine overlap of 2 full causal diagrams: see Tufts University site Complication 1: Semantic Similarity Complication 2: Relative strength vs true agreement of functional relations

123
Assets and Implications of Model Quantification 6: Intervention with Proximal vs Distal Causal Variables Intervention with proximal, compared to distal, causal variables will always have greater but often less generalizable magnitude of effects (assuming strength of causal relations are the same)
")
124
David Hume, 1740

125
“The idea, then, of causation must be derived from some relation among objects. . . whatever objects are considered as causes or effects, are contiguous; and that nothing can operate in a time or place, which is ever so little removed from those of its existence. Though distant objects may sometimes seem productive of each other, they are commonly found upon examination to be linked by a chain of contiguous causes”

126
Distal and Proximal Causal Variables
Y2 X3 X2 Distal X1 proximal Y1 Y3 X4

127
Similar to Aristotle’s concept of
Final cause: That cause but for which a thing would not exist; the final purpose of a thing.

128
Relevant for “systems-level functional analysis” (e. g
Relevant for “systems-level functional analysis” (e.g., institutional systems issues affecting aggression in psychiatric units) Relevant to some “personality-based” treatments, with important referral problems Generalized fears of rejection/abandonment, paranoid ideation, irritability, when main target is conflict with partner E.g., X1 = escalation in marital conflict X2 = early learned fears of abandonment Y1 = marital distress Y2, Y3 = other relationship distress
 Relevant to some personality-based treatments, with important referral problems. Generalized fears of rejection/abandonment, paranoid ideation, irritability, when main target is conflict with partner. E.g., X1 = escalation in marital conflict. X2 = early learned fears of abandonment. Y1 = marital distress. Y2, Y3 = other relationship distress.")
129
Effect of X2 on Y1 will always be less than effect of X1 on Y1 because the ME of X2 is modified by path and modifiability coefficients associated with X1 Relative difference in ME of X1 and X2 will be a function of values for X3 and X4 (strength and modifiability), as well as X2 --> X1 paths Therefore, ME of X2 can be greater than X1, given greater importance of generalized effects
, as well as X2 --> X1 paths. Therefore, ME of X2 can be greater than X1, given greater importance of generalized effects.")
130
Should you focus on immediate vs distal (general) causal factors
Should you focus on immediate vs distal (general) causal factors? Amenable to quantifiable analysis. A function of: Relative importance of behavior problem that is down stream from proximal causal variable Relative strength of relations Distal ---> multiple behavior problems Proximal ---> main behavior problem
 causal factors Amenable to quantifiable analysis. A function of: Relative importance of behavior problem that is down stream from proximal causal variable. Relative strength of relations. Distal ---> multiple behavior problems. Proximal ---> main behavior problem.")
131
Generalized vs specific causal variable, consider
X1 = escalation in marital conflict X2 = early learned fears of abandonment, or paranoid tendencies, or fears of rejection, or critical interpersonal style Y1 = marital distress Y2, Y3 = other relationship distress

132
Distal and Proximal Causal Variables
Y2 X3 X2 Distal X1 proximal Y1 Probably, bidirectional relations between causal variables, with treatment Y3 X4

133
Assets and Implications of Model Quantification 7:
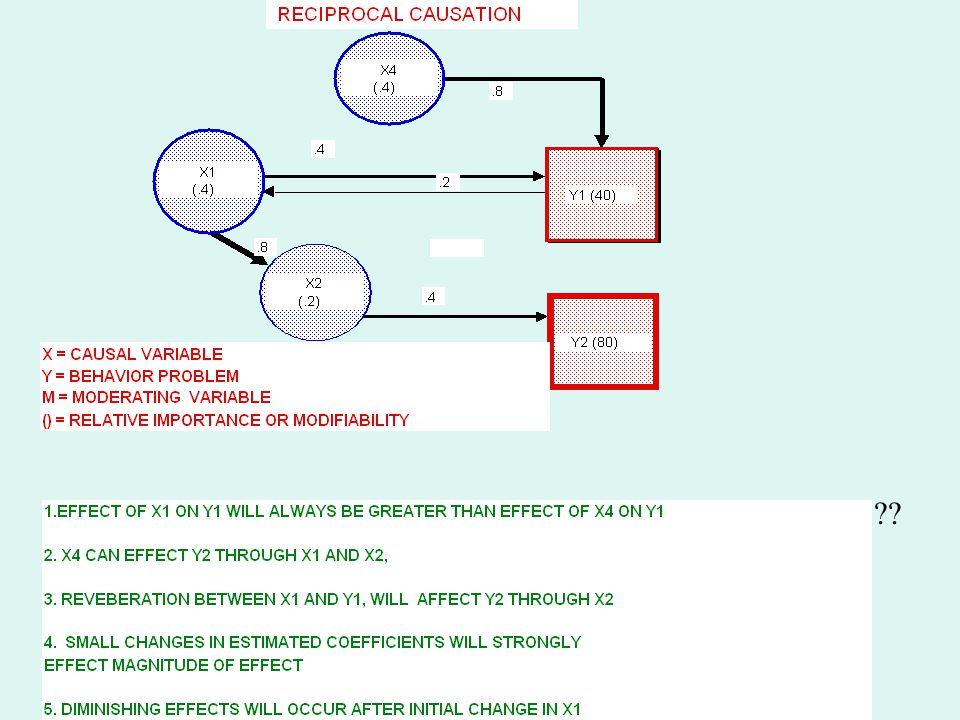
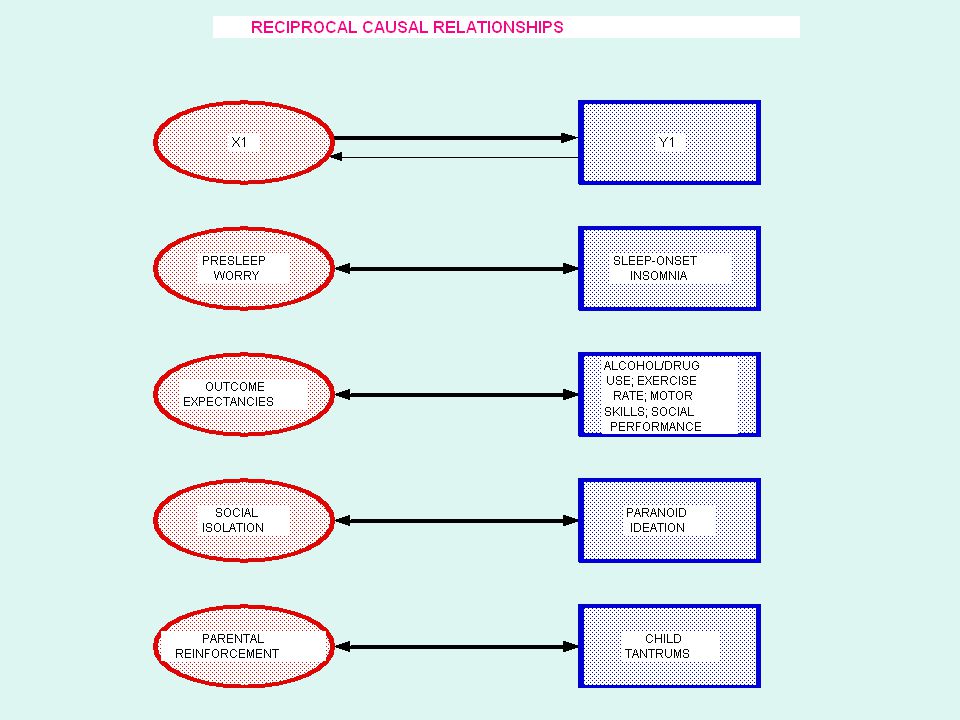
An emphasis on Bidirectional Causal Relations Useful in treatment foci Treatment can focus on either variable Beneficial effects can continue after treatment termination--reverberation e.g., marital distress <---> depression paranoid thoughts <---> social isolation

136
??
138
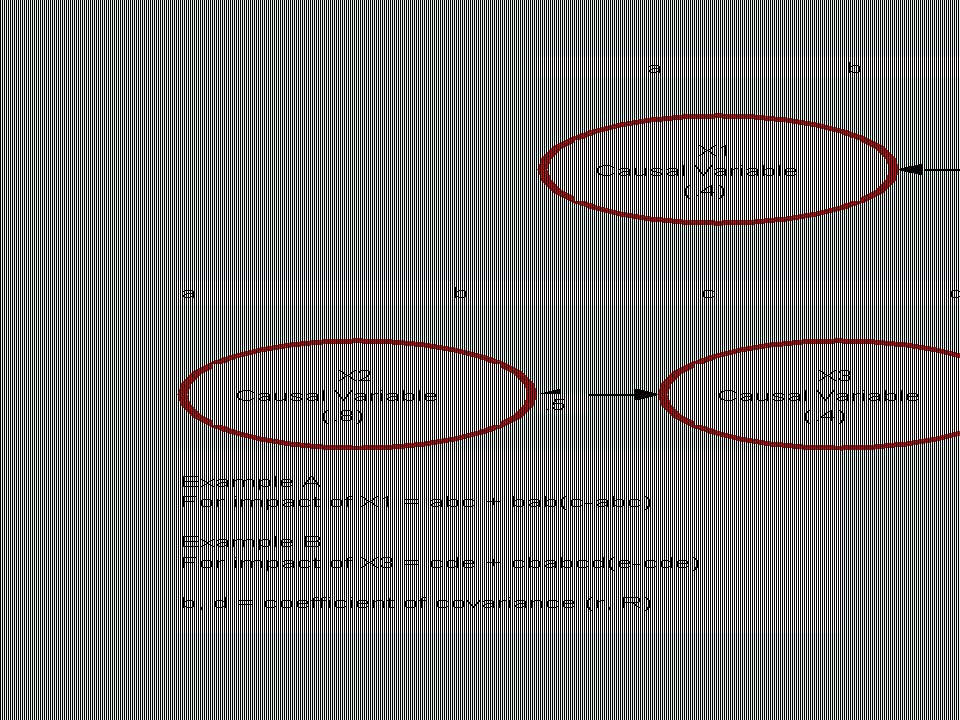
Note relevance of differential calculus
Each slope approaches a maximum (where slope, first derivative, approximates 0) So, can estimate degree to which a focus on a bidirectional relation results in greater magnitude of effect than a focus on a unidirectional causal relation by comparing first derivative with causal path of unidirectional causal relation
 So, can estimate degree to which a focus on a bidirectional relation results in greater magnitude of effect than a focus on a unidirectional causal relation by comparing first derivative with causal path of unidirectional causal relation.")
139
Another benefit of quantification of causal diagrams (FACCDs): Sensitivity analysis
how the variation in the output of a mathematical model can be apportioned, qualitatively or quantitatively, to different sources of variation in the input of a model what proportion of variance in behavior problems does the causal model (the clinician think) can be controlled?) Requires that functional relations affecting a BP assume true “proportions of variance” (different than the relativistic approach discussed thus far)
 can be controlled ) Requires that functional relations affecting a BP assume true proportions of variance (different than the relativistic approach discussed thus far)")
140
Limitations of Causal Diagrams and FACCD (Idiographic causal models)
Validity limited by validity of assessment data; often limited assessment strategies Are “hypothesized” “clinical judgments” and reflect biases of clinician Causal relations can be unstable across time, validity is time-limited

141
Dynamic aspects of behavior problems are not modeled Bipolar shifts
Borderline personality disorders -- emotional lability (the dimension of interest) Latency of causal effects (arrows not proportional to latency of causal effects; are ordinal, rather than ratio in terms of strength) Consider problem of selecting weaker but quicker causal relation vs. stronger but delayed causal relation?
 Latency of causal effects (arrows not proportional to latency of causal effects; are ordinal, rather than ratio in terms of strength) Consider problem of selecting weaker but quicker causal relation vs. stronger but delayed causal relation")
142
Semantic ambiguity overlap/imprecision in variables
Consider “different”? causal variables such as Marital conflict - marital distress Reinforcement - response contingency Contextual- setting - antecedent factors Arousal - Physiological arousal- tension, Monitoring deficits - inattention, attention deficit

143
Pseudo-precision: Quantification increases the patina of precision (because of measurement/inferential limitations) Better to use “ß” (reflecting units of change, rather than “R”?)
")
144
FACCD’s (+ some nomothetic causal diagrams are overidentified)
>100% of variance accounted for in behavior problem Causal variables necessarily related/dependent Semantic overlap? Different response modes (activity, thinking, physiological) But, can still search for greatest ME
 But, can still search for greatest ME.")
145
Incomplete--Do not contain all causal variables; often omit variables between a cause and a behavior problem

146
Nonlinear functional relations
Many medication effects Pleasant/unpleasant events --> mood (functional plateaus) Physiological arousal --> cognitive functioning Life stressors --> psychological symptoms (catastrophic functions) use of algebraic functions in paths? Or unnecessary?
 Physiological arousal --> cognitive functioning. Life stressors --> psychological symptoms (catastrophic functions) use of algebraic functions in paths Or unnecessary")
148
Modeling nonlinear functional relations?
X1 Y1 Y2 X2 a Modeling nonlinear functional relations? a: y = aX23 (parabolic function between X and Y)
")
149
References and Sources
( for copies of the PP presentation) Website with behavioral assessment definitions, clinical case examples of FACCDs, manuscripts. Login: behavioral; Password: assessment For visual graphics, diagramming software:
 Website with behavioral assessment definitions, clinical case examples of FACCDs, manuscripts. Login: behavioral; Password: assessment. For visual graphics, diagramming software:")
150
Causation, Prediction, and Search, 2nd Edition, (2001), by P
Causation, Prediction, and Search, 2nd Edition, (2001), by P. Spirtes, C. Glymour, and R. Scheines ( MIT Press) Causality: Models, Reasoning, and Inference, (2000), Judea Pearl, Cambridge Univ. Press Computation, Causation, & Discovery (1999), edited by C. Glymour and G. Cooper, MIT Press Causality in Crisis?, (1997) V. McKim and S. Turner (eds.), Univ. of Notre Dame Press. The Art of Causal Conjecture (1996). Glenn Shafer. MIT Press.
, by P. Spirtes, C. Glymour, and R. Scheines ( MIT Press) Causality: Models, Reasoning, and Inference, (2000), Judea Pearl, Cambridge Univ. Press. Computation, Causation, & Discovery (1999), edited by C. Glymour and G. Cooper, MIT Press. Causality in Crisis , (1997) V. McKim and S. Turner (eds.), Univ. of Notre Dame Press. The Art of Causal Conjecture (1996). Glenn Shafer. MIT Press.")
151
Haynes, S. N. and O’Brien. W. O. (2000)
Haynes, S. N. and O’Brien. W. O. (2000). Principles of Behavioral Assessment: A Functional Approach to Psychological Assessment. New York: Plenum/Kluwer Press.. Haynes, S. N. & O'Brien, W. O. (1990). The functional analysis in behavior therapy. Clinical Psychology Review, 10, Haynes, S. N., Uchigakiuchi, P., Meyer, K., Orimoto, Blaine, D., and O’Brien, W. O. (l993). Functional analytic causal models and the design of treatment programs: Concepts and clinical applications with childhood behavior problems. European Journal of Psychological Assessment, 9, l O’Brien, W. H. & Haynes, S. N. (1995). A functional analytic approach to the conceptualization, assessment and treatment of a child with frequent migraine headaches. In Session., l,
. Principles of Behavioral Assessment: A Functional Approach to Psychological Assessment. New York: Plenum/Kluwer Press.. Haynes, S. N. & O Brien, W. O. (1990). The functional analysis in behavior therapy. Clinical Psychology Review, 10, Haynes, S. N., Uchigakiuchi, P., Meyer, K., Orimoto, Blaine, D., and O’Brien, W. O. (l993). Functional analytic causal models and the design of treatment programs: Concepts and clinical applications with childhood behavior problems. European Journal of Psychological Assessment, 9, l O’Brien, W. H. & Haynes, S. N. (1995). A functional analytic approach to the conceptualization, assessment and treatment of a child with frequent migraine headaches. In Session., l,")
152
Haynes, S. N. , Richard, D. , & O’Brien, W. B. (l996)
Haynes, S. N., Richard, D., & O’Brien, W. B. (l996).The Functional Analysis in Behavior Therapy: Estimating the Strength of Causal Relationships for the Design of Treatment Programs. Gedrags-therapie, 4, 289-3l4. O’Brien, S. N., & Haynes, S. N. (1997) Functional analysis. In: Gualberto Buela-Casal (Ed): Handbook of Psychological Assessment. Madrid: Sigma Floyd, F., Haynes, S. N., & Kelly, S. (1997). Marital assessment: A dynamic and Functional analytic Perspective. In: W. K. Halford, & H. J. Markman (Eds.). Clinical handbook of marriage and couples intervention (pp ). New York: Guilford Press Nezu, A., Nezu, C., Friedman, & Haynes, S. N. Case formulation in behavior therapy. T. D. Eells (Ed.) (l997). Handbook of psychotherapy case formulation. NY: Guilford. Haynes, S. N., Leisen, M. B., & Blaine, D.D. (1997). Functional Analytic Clinical Case Models and Clinical Decision-Making. Psychological Assessment, 9,
.The Functional Analysis in Behavior Therapy: Estimating the Strength of Causal Relationships for the Design of Treatment Programs. Gedrags-therapie, 4, 289-3l4. O’Brien, S. N., & Haynes, S. N. (1997) Functional analysis. In: Gualberto Buela-Casal (Ed): Handbook of Psychological Assessment. Madrid: Sigma. Floyd, F., Haynes, S. N., & Kelly, S. (1997). Marital assessment: A dynamic and Functional analytic Perspective. In: W. K. Halford, & H. J. Markman (Eds.). Clinical handbook of marriage and couples intervention (pp ). New York: Guilford Press. Nezu, A., Nezu, C., Friedman, & Haynes, S. N. Case formulation in behavior therapy. T. D. Eells (Ed.) (l997). Handbook of psychotherapy case formulation. NY: Guilford. Haynes, S. N., Leisen, M. B., & Blaine, D.D. (1997). Functional Analytic Clinical Case Models and Clinical Decision-Making. Psychological Assessment, 9,")
153
Haynes, S.N. (1998). The assessment-treatment relationship and functional analysis in behavior therapy . European Journal of Psychological Assessment, 14 (1), pp Haynes, S. N., & Williams, A. W. (2003). Clinical case formulation and the design of treatment programs: Matching treatment mechanisms and causal relations for behavior problems in a functional analysis. European Journal of Psychological Assessment,19, Haynes, S. N. (2005). La formulacion cliniaca conductual de caso: pasos para la elaboracion del analisis funcional [Behavioral clinical case formulation: guidelines on the construction of a functional analysis]. In V. E. Caballo (ed.), Manual para la evaluacion clinica de los trastornos psicologicos: Estrategias de evaluacion, problemas infantiles y trastornos de ansiedad [Handbook for the clinical assessment of psychological disorders: Assessment strategies, childhood problems and anxiety disorders] (pp ). Madrid: Piramide. Virus-Ortega, J., & Haynes, S. N. (2005). Functional analysis in behavior therapy: Behavioral foundations and clinical application. International Journal of Clinical and Health Psychology, 5,
. Clinical case formulation and the design of treatment programs: Matching treatment mechanisms and causal relations for behavior problems in a functional analysis. European Journal of Psychological Assessment,19, Haynes, S. N. (2005). La formulacion cliniaca conductual de caso: pasos para la elaboracion del analisis funcional [Behavioral clinical case formulation: guidelines on the construction of a functional analysis]. In V. E. Caballo (ed.), Manual para la evaluacion clinica de los trastornos psicologicos: Estrategias de evaluacion, problemas infantiles y trastornos de ansiedad [Handbook for the clinical assessment of psychological disorders: Assessment strategies, childhood problems and anxiety disorders] (pp ). Madrid: Piramide. Virus-Ortega, J., & Haynes, S. N. (2005). Functional analysis in behavior therapy: Behavioral foundations and clinical application. International Journal of Clinical and Health Psychology, 5,")
154
Haynes, S. N. & Kaholokula, J. K. (2007). Behavioral assessment
Haynes, S. N. & Kaholokula, J.K. (2007). Behavioral assessment. In: Hersen and A. M. Gross Handbook of Clinical Psychology John Wiley and Sons, New York. Raimo Lappalainen, R., Timonen, T, & Haynes, S. N. (2009). The functional analysis and functional analytic clinica case formulation--a case of anorexia nervosa. In P. Sturmey (Ed.). Clinical case formulation Kaholokula, J. K., Bello, I. Nacapoy, A. H., Haynes, S. (in press). Behavioral assessment and functional analysis. D. Richard & S. Huprich (Eds): Clinical Psychology: Assessment, Treatment, and Research
. Behavioral assessment. In: Hersen and A. M. Gross Handbook of Clinical Psychology John Wiley and Sons, New York. Raimo Lappalainen, R., Timonen, T, & Haynes, S. N. (2009). The functional analysis and functional analytic clinica case formulation--a case of anorexia nervosa. In P. Sturmey (Ed.). Clinical case formulation. Kaholokula, J. K., Bello, I. Nacapoy, A. H., Haynes, S. (in press). Behavioral assessment and functional analysis. D. Richard & S. Huprich (Eds): Clinical Psychology: Assessment, Treatment, and Research.")
155
The End

Similar presentations


















,>")







