Download presentation
Presentation is loading. Please wait.

1
TRACHEOSTOMY Dr. Manorama Mittal Dr. Namita Arora

2
55yr.old man with Ca. larynx
Q1: What comes to our mind first? Q2: What are the relevant points in the history? Q3: What do you see on examination?

3
Tracheostomy for Ca Lx Q1: What are the advantages of a pre-op. traecheostomy? Q2: What are the disadvantages of pre-op.traecheostomy? Q3: Traecheostomy done in ward & patient suddenly dies. What is the likely cause? How can we prevent it? Q4: What are the problems with post-op. traecheostomy? Q5: For how long is humidification required in these patients?

4
Heat & Moisture Exchanger (artificial nose)
Q1: What is HME? Q2: How does it work?

5
Tracheostomy in a patient of chronic bronchitis with CO2 narcosis.
Q1: Take a hypothetical case of chronic bronchitis with CO2 narcosis with traecheostomy.He was put on ventilator following which he became conscious & then suddenly died.Why?

6
Tracheostomy vs Prolonged intubation in paediatric patient
Q1: What are the problems of traecheostomy in children? Q2: What should be method of suctioning & the interval in between the two suctions? Q3: What are the methods of humidification? Q4: What are the problems with humidification?

7
Weaning in paediatric patient with tracheostomy
Q1: Why is weaning difficult? Q2: What is ward decannulation?

8
Q1: What are the different types of cuffs?
Patient on ventilator Q1: What are the different types of cuffs?

9
Indications of Tracheostomy
Q1: What are the indications of preoperative Tracheostomy? Q2: What are the indications of post-op Tracheostomy? Q3: What are the other indications of elective Tracheostomy? Q4: What are the indications of emergency Tracheostomy?

10
Cricothyroidotomy Q1: What are the indications of cricothyroidotomy?
Q2: What are the advantages of cricothyroidotomy? Q3: What are the disadvantages of cricothyroidotomy? Q4: What is an absolute contra-indication to jet ventilation through needle cricothyroidotomy?

11
Percutaneus Dialational Tracheostomy (PDT)
Q1: Enumerate the steps of PDT? Q2: What are the advantages of PDT? Q3: What are the disadvantages of PDT? Q4:Complications of PDT?

12
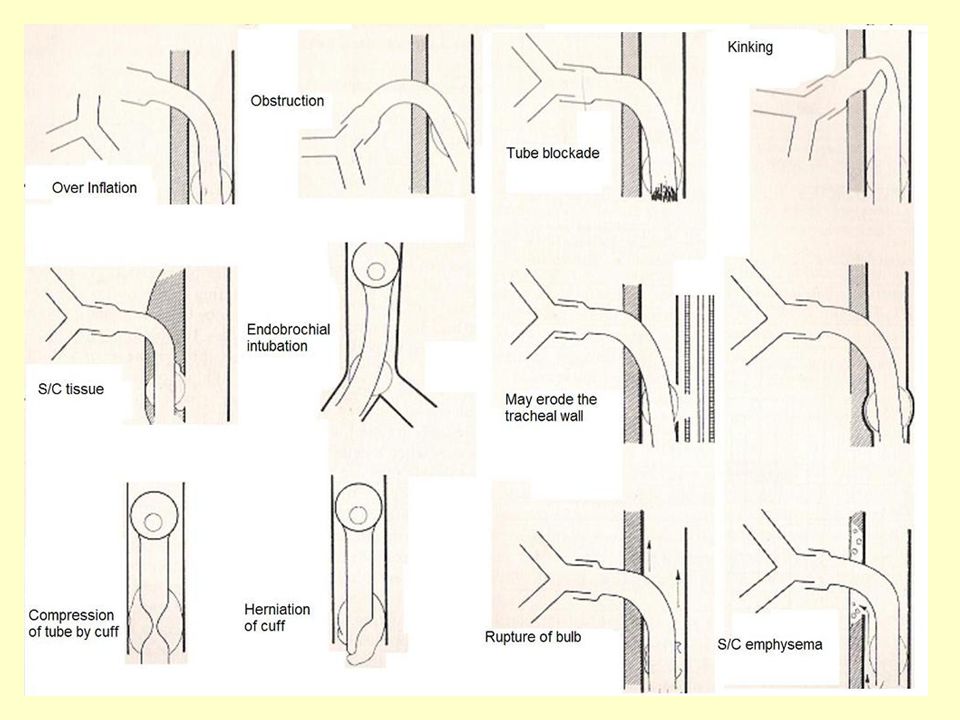
Complications of Tracheostomy
Q1: What is the cause of massive hemorrhage following Tracheostomy? Q2: What is the cause of mediastinal emphysema? Q3: What is a persistant stoma? Q4: Usually how long does a stoma take to close?

14
Q1: What comes to our mind first?
This patient must have been a smoker Does he have an airway compromise? Would he need a tracheostomy to overcome the airway compromise prior to surgery?

15
Q2: What are the relevant points in the history?
· Smoking, tobacco chewing,alcohol intake · Dyspnoea, dysphagia, loss of weight & appetite,fever · Hoarseness of voice · Cough: dry/productive

16
Q3: What do you see on examination?
GPE Vitals Anemia ,waxy look ,toxic ,cachectic,/anxious Cervical lymphadenopathy. II. Systemic Examination Respiratory System

17
Q1: What are the advantages of a pre-op. traecheostomy?
For the anaesthetist the biggest advantage is that problems of difficult airway are bypassed

18
Q2: What are the disadvantages of pre-op.traecheostomy?
Local infection & inflammation that occurs does not allow the surgeon to demarcate the clear area for resection.

19
Q3:. Traecheostomy done in ward & patient suddenly dies
Q3: Traecheostomy done in ward & patient suddenly dies. What is the likely cause? How can we prevent it? Asphyxia i.e, hypoxia with hypercarbia get corrected when obstruction is relieved.The stimuli for respiration are hence abolished leading to respiratory arrest & death. VVagal stimulation due to excessive movement of trachea may cause death during the tracheostomy. DDeath can be prevented by monitoring the ECG & having means to ventilate the patient in the ward.

20
Q4: What are the problems with post- op. traecheostomy?
Patient is unable to communicate if any problem arises. We need to have a bell switch /light switch/nurse by the side of the patient.

21
Q5: For how long is humidification required in these patients?
This is especially relevant here as these patients have a permanent traecheostomy.Humidification required for one week after which the columnar ciliated epithelium changes into pseudo-stratified squamous epithelium that is resistant to drying.

22
Q1: What is HME? It is an equipment which helps in preserving the moisture & heat of the expired breath.

23
Has minimal dead space (8 to 9ml.)
Q2: How does it work? It contains a Nylon coil. During expiration water condenses on the coil & heats it. During inspiration the cold dry air picks up water vapour & gets heated up while passing through the HME. Has minimal dead space (8 to 9ml.) Has very low resistance to flow(I to2cm H2O).
 Has very low resistance to flow(I to2cm H2O).")
24
Q1:. Take a hypothetical case of chronic bronchitis
Q1: Take a hypothetical case of chronic bronchitis with CO2 narcosis with traecheostomy.He was put on ventilator following which he became conscious & then suddenly died.Why? CO2 tissue stores in such patients are very high. Marked hypercarbia leads to high levels of circulating catecholamines but also desensitizes the myocardium to their action.Sudden lowering of CO2 levels leads to regaining of sensitivity of myocardium but since circulating catecholamine levels are still high, there is fibrillation followed by cardiac arrest & death.

25
Q1: What are the problems of tracheostomy in children?
Performing a tracheostomy is very difficult, a specialist’s job False passage is very likely It has to be a planned procedure under general anaesthesia in an intubated child Subglottic oedema & stenosis are very common Weaning is difficult

26
The interval in adults is 10 to 15 sec.
Q2: What should be method of suctioning & the interval in between the two suctions? The interval in adults is 10 to 15 sec. The duration of suctioning should also be the same. In children there should be 3 to 4 breaths in between the two suctions even if the child is drowning in secretions. Answer .doc

27
Q3: What are the methods of humidification?
· Wet gauze /Saline drip · Droplet delivery (mechanical/ultrasonic) · Hot water humidification · HME Answer .doc
 · Hot water humidification. · HME. Answer .doc.")
28
Q4: What are the problems with humidification?
· Over hydration – especially with nebulization · Over heating -When using hot water humidification By temporary disconnection of a pressure cycled ventilator because flow suddenly increases. Thermostat failure.

29
Q1: Why is weaning difficult?
As a well fitting tube is put in children, they are unable to breathe when the tracheostomy tube is occluded. Hence we need to use a fenestrated tube for weaning. Suprastomal collapse & granulation are common. Psychological attachment to the tracheostomy tube Hence more controlled process called ward decannulation is used. Fenestrated tube Ans .doc

30
Q2: What is ward decannulation?
Child is kept in the ward for decannulation. Tracheostomy tube is progressively down sized.Usually one size smaller each day till the smallest size of T’ tube has been tolerated. Tracheostomy tube is then blocked for 12 hrs during the day & then 24hrs next day & night. The tube is now safely removed & stoma covered. Child observed for further 5 days.

31
Q1: What are the different types of cuffs?
Low volume High Presssure Large vol. Low pressure Foam cuff · Low vol. high pr, cuff: Introduction is easy · High vol. cuff : Difficult to introduce.Chance of aspiration is high if tube is big & cuff not fully inflated. · Polyurethane (foam) cuff:self inflating · Double cuff:The two cuffs are alternately inflated & deflated. · Pressure adjusting cuff:When N20 is used, it diffuses into the cuff leading to increase in intra cuff pressure but in this tube the change in volume of cuff is shifted to the pilot balloon which in turn is big, pliable & thin walled from where N20 diffuses out thus preventing any rise in intra cuff pressure Pic. Ans from .doc
 cuff:self inflating. · Double cuff:The two cuffs are alternately inflated & deflated. · Pressure adjusting cuff:When N20 is used, it diffuses into the cuff leading to increase in intra cuff pressure but in this tube the change in volume of cuff is shifted to the pilot balloon which in turn is big, pliable & thin walled from where N20 diffuses out thus preventing any rise in intra cuff pressure. Pic. Ans from .doc.")
32
Q1: What are the indications of preoperative Tracheostomy?
Massive cystic Hygroma Ludwig’s Angina Massive Thyroid enlargement (with respiratory difficulty) Add answer Carcinoma maxilla
 Add answer. Carcinoma maxilla.")
33
Q2: What are the indications of emergency Tracheostomy?
Angioneurotic oedema Croup Diphtheria failed intubation Picture?? Add answer from.doc

34
Q3: What are the indications of postoperative Tracheostomy?
Ca.larynx following laryngectomy Massive thyroid enlargement: if more than 3 tracheal cartilages are eroded or calcified. Picture?? Add answer from.doc

35
Q4: What are the other indications of elective Tracheostomy?
· Prolonged ventilation · Pulmonary hygiene/toilet (as in a respiratory cripple) Picture?? Add answer from.doc
 Picture Add answer from.doc.")
36
Q1: What are the indications of cricothyroidotomy?
Add answer Cannot intubate, cannot ventilate: needle cricothroidotomy for ventilation Difficult intubation: needle cricothroidotomy for reterograde intubation

37
Q2: What are the advantages of cricothyroidotomy?
Simple Takes less than 1min to perform Ambulance/casualty/emergency personnel/nurses can perform it Add answer

38
Q3: What are the disadvantages of cricothyroidotomy?
Subglotic oedema & stenosis are very likely Add answer

39
Complete/near complete obstruction at glottic/supraglottic level
Q4: What is an absolute contra-indication to jet ventilation through needle cricothyroidotomy? Complete/near complete obstruction at glottic/supraglottic level Add answer

40
Q1: Enumerate the steps of PDT?
Trachea punctured with needle Guide wire passed Graded dilators passed over the guide wire Tracheostomy tube passed The whole procedure can be done while visualizing the trachea with a fibrescope through the endotracheal tube. Add answer

41
Q2: What are the advantages of PDT?
· Easy to learn · Shorter procedure · Elimination of scheduling difficulty · Precludes necessity to shift critical patient to OT · Half as expensive as surgical Tracheostomy Add answer

42
Q3: What are the disadvantages of PDT?
· Needs special equipment · Can be done only in intubated patients · Contra indicated in children · Contraindicated in cervical spine fractures as neck cannot be hyper extended. Add answer

43
Q4: Complications of PDT?
False passage P Puncture through side & B back wall of trachea Add answer

44
Q1: What is the cause of massive hemorrhage following Tracheostomy?
Tracheo-innominate artery fistula. This happens when tube’s not in line with trachea. Add answer

45
Q2: What is the cause of mediastinal emphysema?
Too small a tracheal tube Excessive coughing & straining on the tube Add answer

46
Q3: What is a persistant stoma?
Stoma that persists for more than 2 months & requires surgical closure Large stoma may require perichondral flap from thyroid cartilage Add answer

47
Q4: Usually how long does a stoma take to close?
UUsually takes few days to a week Add answer

Similar presentations





 – Oral-tracheal – Naso-tracheal Tracheostomy (trach) 1.>")













