Download presentation
Presentation is loading. Please wait.

1
Does Patient Centered Care Enhance Quality and Safety?
Human Factors, System Issues System Solutions © 2010 Planetree, Inc.

2
Objectives of Presentation
Provide concepts of how the Planetree philosophy can support system changes to enhance a culture of quality and safety Understand safety implications related to human performance Discuss how a patient centered approach can enhance patient and family involvement and patient safety Present outcome measures to demonstrate that a Planetree patient centered environment not only supports a culture of quality but also improves patient and employee satisfaction, and the bottom line

3
What Started Safety Awareness?
To Err is Human – IOM Study showed adverse events happen in 2.9 to 3.7 percent of hospitalizations Extrapolated over 33.6 million admissions per year = 44,000-98,000 deaths due to medical error per year Poor communication and a lack of teamwork was identified as a root cause of most safety problems

4
11 Years After the IOM “To Err is Human…” Report: What Has Changed?
4

5
Safety Hazard Probabilities (events per million opportunities)
Acquiring HIV from 1 unit of transfused blood 0.7 All heads on 20 coin tosses Death of commercial airline passenger Death: general anesthesia Death: motor vehicle Preventable hospital deaths Orlikoff,J. Orlikoff and Associates, Inc. Chicago, IL. Jan. 2010

6
Cost of Medical Errors in U.S.
$17 billion costs associated with preventable errors (IOM, 1999) In the past, third party payers have paid regardless of outcome – changed as of 10/2008! Central Line associated bloodstream infections resulted in an average loss per case of $26,839 in 2006 Shannon et al, “Economics of Central-Line Associated Bloodstream Infections” American Journal of Medical Quality Supplement to Vol.21, No.6 Nov/Dec 2006 Run thru these next few slides to emphasize what’s happening… do they know their numbers for these events?
 In the past, third party payers have paid regardless of outcome – changed as of 10/2008! Central Line associated bloodstream infections resulted in an average loss per case of $26,839 in Shannon et al, Economics of Central-Line Associated Bloodstream Infections American Journal of Medical Quality Supplement to Vol.21, No.6 Nov/Dec Run thru these next few slides to emphasize what’s happening… do they know their numbers for these events")
7
National Health Expenditures per Capita, 1980– 2007
Data: OECD Health Data 2009 (June 2009).
.")
8
What are the “Other” Cost of Errors?
Errors may be career ending events Caregivers don’t intend to harm Trust issues and safety concerns on part of the consumers and payers Frustrated consumers Silence often surrounds issues which may result in malpractice claims Sensational negative media coverage

9
News Headlines SEPT. 2006: “HOSPITAL CHANGES PROCEDURES AFTER PREEMIE DEATHS”: Three preemies die after they receive adult doses of heparin at a hospital in Indianapolis NOV. 2007: “HOSPITAL REPEATS WRONG-SIDED BRAIN SURGERY”: “For the third time this year, doctors at Rhode Island Hospital have operated on the wrong side of a patient’s head – an action that has brought about censure from the state Department of Health and a $50,000 fine.” SEPT. 2010: “BABY DIES AT SEATTLE CHILDREN’S HOSPITAL AFTER OVERDOSE”: …a hospital nurse gave her 10 times the proper dose of a medication, calcium chloride. Five days later, on Sept. 19, after suffering a brain hemorrhage, the baby died.

10
State of Colorado Local TV news coverage on prevention of central line infections Discussed use of central line bundle Shortly thereafter, legislators in the State received a “slew” of s from constituents demanding use of the central line bundle be made into law!

11
Put it in Perspective 25% of US patients state they have experienced a medical error - 50% of those resulting in serious harm 42% of health care workers (HCW) state they have been personally involved in a medical error HCW’s state they fear becoming a patient Seek the best MD – not the MD on call Seek out high volume places for complicated surgeries Seek out clinicians with at least 10 years experience (experienced but not burned out) Avoid hospitalization in July – new interns, medical and nursing students (now proven by research)
 state they have been personally involved in a medical error. HCW’s state they fear becoming a patient. Seek the best MD – not the MD on call. Seek out high volume places for complicated surgeries. Seek out clinicians with at least 10 years experience (experienced but not burned out) Avoid hospitalization in July – new interns, medical and nursing students (now proven by research)")
12
What is Patient Safety Freedom from accidental injury through:
Systems and processes that decrease the likelihood of mistakes and Systems and processes that increase the likelihood of prompt identification and correction of errors and mistakes before they cause harm to a patient

13
What is High Quality Care?
IOM defines quality as: “The degree to which health care services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge.” High quality (evidence based) medicine allows for variation based on patient need, not on physician preferences (patient focused)
 medicine allows for variation based on patient need, not on physician preferences (patient focused)")
14
Evidence Based Care Bundles Hospital Infections are Preventable!
FACT - 80,000 CLABIs per year, cause about 28,000 deaths In 103 ICUs in Michigan median CLABI rate per 1,000 catheter days declined from 2.7 to ZERO HOW? - It’s simple Hand washing; Full Barrier precautions; Chlorhexidine use; Avoid using the femoral site; Removing unneeded catheters. Provonost, et al. New England Journal of Medicine, Dec 28, 2006.

15
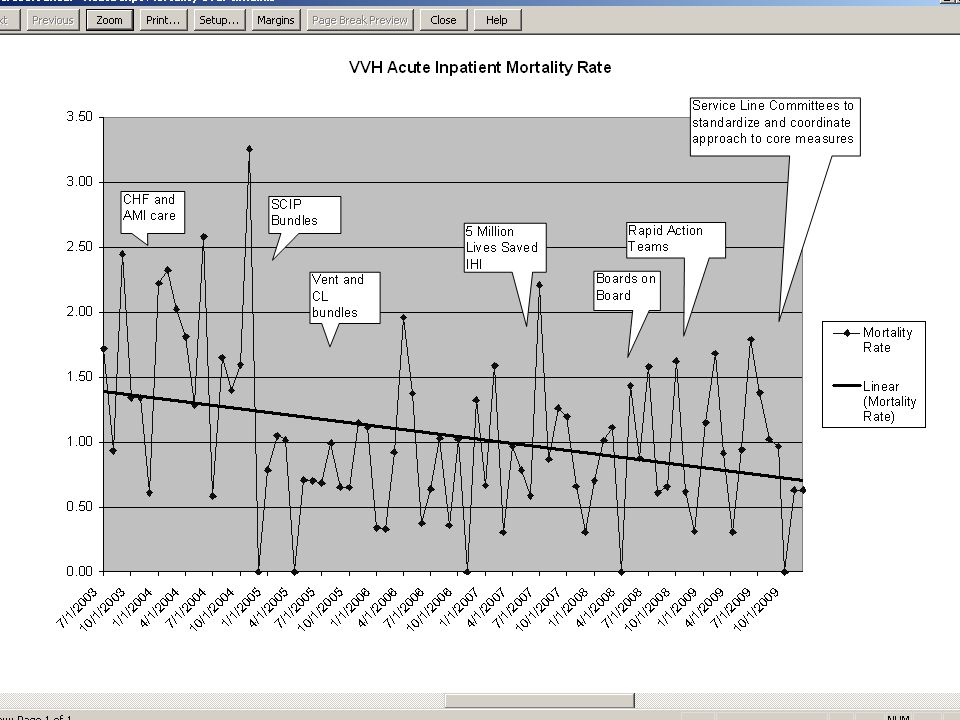
IHI- 5 Million Lives Saved Campaign
Interventions targeted at harm: Prevent Pressure Ulcers... Reduce MDRO/MRSA Infections… Prevent Harm from Medications... Deliver Evidence-Based Care for CHF, AMI, Pneumonia… Prevent ventilator pneumonia Prevent central line infections Detailed How-to Guides on each intervention are available at under the Materials tab. 15

17
“New” Reality of US Healthcare
Evidence Based Care – Core Measures Medicare/insurance no longer pays for defined “never events” (10/08) National versus Local Standards Public reporting of quality data and safety events - transparency AHRQ measures reported to the public Patient Centered Care
 National versus Local Standards. Public reporting of quality data and safety events - transparency. AHRQ measures reported to the public Patient Centered Care.")
18
What is Patient Centered Care?
Defined by the IOM: “…care that is respectful of and responsive to individual patient preferences, needs and values, and ensuring that patient values guide all clinical decisions.“ New 2011 TJC Standards

19
Opportunities for Improvement
Communication challenged Fragmented health care system Complex systems within hospitals Lack of standardization Hierarchies produce steep authority gradients Need better teamwork and communication Product of our success Advanced technology, rapid changes Necessary knowledge exceeds limits to human capacity > 6000 meds, >4000 treatments to choose from Professional craftsman model No longer effective

20
Professional Craftsman Model “The Old Way”
With extensive training Eminence based training – not always evidence based Came “special privileges” Full autonomy= full responsibility Creates a steep authority gradient Others have been there only to assist the MD in the past No recognized group decision making Results in the ‘Perfection Myth’

21
Safety Implications Related to the ‘Perfection Myth’
Safety depends on individuals - myth Safety really depends on teamwork and communication Error is due to carelessness – myth More often a system or process error We have responded in the past with peer review, “be safer next time”, more education, 5 rights Punishment results in fewer errors - myth System Improvements should be the focus

22
Dysfunctional Response to Error
Justification/rationalization “Complications happen” Blame the patients Dishonesty with patients Cover-up/Non-reporting Fear loss of reputation Healthcare workers look the other way when colleagues error

23
Who Is Watching Out For Patients?
46% of physicians failed to report at least one serious medical error, even though 93% of them said they should report ALL significant medical errors they observe. 45% said they did not report impaired or incompetent colleague physicians even though 96% said they should - ANNALS OF INTERNAL MEDICINE, DEC. 4, 2007 67% of physicians have not been involved in collaborative efforts to improve quality – COMMONWEALTH FUND NATIONAL SURVEY OF PHYSICIANS, 2007

24
A Different (Planetree) Approach
Caring for the Caregivers Leadership support for safety Non-punitive reporting systems Set up systems and processes for safety Redundancy and double checks Medication administration vs. blood transfusion Standardization of processes Checklists, pre-printed orders Find out about work-arounds Multidisciplinary quality committees

25
Caring for the Caregivers
Teamwork and communication support Enhanced communication models Robust reporting systems with feedback Errors recognized as system failures Mutual Support – I have your back Nurse Residency Programs Plan for and educate about limitations of human performance

26
Plan for the ‘Human Factor’
Humans make mistakes Fatigue, interruptions, distractions, etc Overestimate abilities, underestimate limitations Goal is to keep inevitable mistakes from becoming consequential Reliable systems combined with effective communication is best practice

27
Human Limitations Limited memory capacity–5 to 7 pieces of information in short term memory Negative effects of stress –increased error rates, tunnel vision Negative influence of fatigue Limited ability to multitask Variable judgments and perceptions

28
Human Error is Inevitable Because:
Inherent human limitations Complex, unsafe systems Safety is often assumed, not assured We count on the expert individual “It won’t happen to me” or “it doesn’t happen here” attitude

29
Build on human factor skills
Standardized (SBAR) communication Telephone order read-backs Starbucks figured it out Create redundancies, double checks Situational awareness Time-outs, include the patient (patient centered) Decrease interruptions Debriefings after emergencies Patient Centered focus Bedside report including the patient/family Hourly rounding Heparin for patient, MD told patient, RN did not know patient going back to surgery….
 communication. Telephone order read-backs. Starbucks figured it out. Create redundancies, double checks. Situational awareness. Time-outs, include the patient (patient centered) Decrease interruptions. Debriefings after emergencies. Patient Centered focus. Bedside report including the patient/family. Hourly rounding. Heparin for patient, MD told patient, RN did not know patient going back to surgery….")
30
A Different (Planetree) Approach
Patient centered approach Knowledge about condition and choices Access to medical records Access to information – library/literature searches Health literacy Care partners Another “ear to hear” Patient and Family Advisory Council Learn from their experiences

31
Planetree Patient Centered Care and Safety
“The patient is one of the most important allies in reducing medical errors.” ISMP Medication Safety Alert Oct.2004 “Research indicates that when patients actively participate in their overall healthcare management, medical errors are reduced.” ISMP Medication Safety Alert Nov. 2004 Patients who have a clear understanding of their instructions, including how to take their medicines and when to make follow-up appointments, are 30 percent less likely to be readmitted or visit the emergency department February 3, 2009, Annals of Internal Medicine

32
Planetree Criteria Promote Quality and Safety
Planetree promotes a healing partnership between patients and caregivers. It’s a model of care that is committed to enhancing healthcare from the patient perspective. Empowers caregivers to do what is right for the patient. 360° data shows us that it is working!

33
Surgical Care Improvement Process Measures

34
Teamwork works! D-T-B times improved!

35
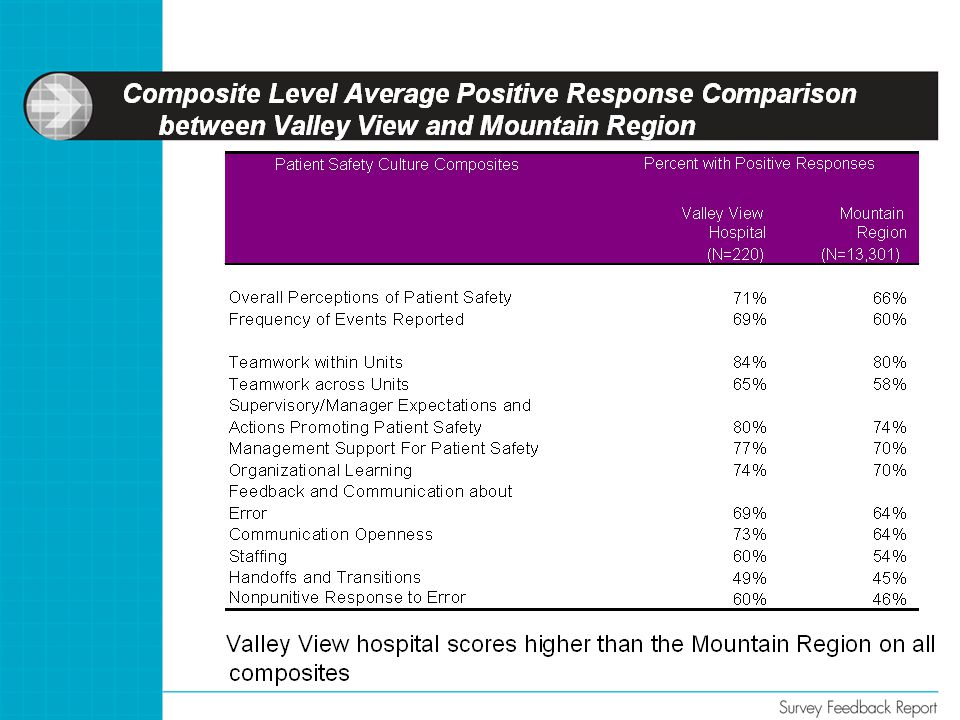
VVH Culture of Safety Survey
Survey done July 2010 Statistical improvements from 2008 Standardized AHRQ survey Designed to measure 4 major areas Overall perceptions of safety Overall patient safety grade Frequency of event reporting Number of events reported

37
Valley View Healthgrades™ Award
Valley View Hospital is rated among the top 5% in patient satisfaction scores The Planetree patient centered philosophy actively supports programs to meet patient and family needs

38
“What Is the Likelihood of Recommending This Hospital?”

39
VVH and Planetree Comparison
39

42
Turnover Rate: All Nurses On Payroll

43
Growth in Equity

44
Lessons learned Safety and quality is not created by counting and control measures We have learned that stories, complex dialogue, and teamwork create safety We thought competent, careful clinicians were sufficient to create safety We have learned safety requires leadership, a supportive environment, a system focus, and solid teamwork Quality and patient safety are supported in a Planetree patient centered environment and the Planetree philosophy promotes a ‘generative’ culture

45
How Different Organizational Cultures Handle Safety Information
Pathological Culture Bureaucratic Generative · Don’t want to know · May not find out · Actively seek it · Messengers (Whistle blowers) are shot · Messengers are listened to if they arrive · Messengers are trained and rewarded · Failure is punished or concealed · Failure leads to local repairs · Failures lead to far-reaching reforms · New ideas are actively discouraged · New ideas often present problems · New ideas are welcomed
 are shot. · Messengers are listened to if they arrive. · Messengers are trained and rewarded. · Failure is punished or concealed. · Failure leads to local repairs. · Failures lead to far-reaching reforms. · New ideas are actively discouraged. · New ideas often present problems. · New ideas are welcomed.")
46
Planetree Creates A Culture of Quality and Safety
An accountable culture A culture of learning A culture of partnership A just culture Mutual Trust The system trusts that you will call out You must trust that the system will listen

Similar presentations