Download presentation
Presentation is loading. Please wait.

1
The Multiple Trauma Patient
Shawn Dowling, PGY-2 Preceptor: Rhonda Ness

2
Objectives Will not go over these topics in great detail Head trauma
C-spine trauma Chest trauma Abdo trauma Pediatric trauma

3
Why it’s important Leading Cause of Death for those aged 1-44yrs (in developed countries) MVC’s account for most injuries Followed by assaults, drownings, falls, burns

4
Distribution of Death

5
What is ATLS? Structured algorithm designed to prioritize management issues Designed as a team-based approach Applicable to both Academic and Rural Settings It’s useful – take it.

6
What ATLS isn’t? A substitute for clinical acumen – trust your instinct Most up-to-date, most evidence based approach (revised q4yrs, most recently 2004)
")
7
Why is the ATLS protocol so nice?
Overall, the tenets are Greatest threats to life are identified and treated 1st Lack of definitive Tx should never impede the application of an indicated Tx Detailed Hx was not essential to begin the evaluation of the acutely injured patient

8
ATLS overview Preparation Triage Primary Survey (ABCDE’s)
Resuscitation Adjuncts to primary survey and Resus Secondary Survey Adjuncts to Secondary survey Continued post-resus monitoring and R/A Definitive Care

9
ATLS Overview Primary Survey Adjuncts Secondary Survey CANNOT MOVE ON
UNTIL YOU ADDRESS THE PROBLEM!!! Primary Survey Reassess Adjuncts Reassess Secondary Survey

10
ATLS – Primary Survey Airway & C-spine Immobilization Breathing
Circulation Disability Exposure/Environmental Control Full Vital Signs

11
Case 1 60ishM Coming in by STARS, ETA 10 mins MVC – no more details
Facial fractures, unable to intubate Significant Chest trauma, hypotense Great...I’ll just go see this LBP patient and wait till I hear the call to the Trauma Bay

12
ATLS overview Preparation Triage Primary Survey (ABCDE’s)
Resuscitation Adjuncts to primary survey and Resus Secondary Survey Adjuncts to Secondary survey Continued post-resus monitoring and R/A Definitive Care

13
Organizing the Trauma Bay
What do you want? Who do you want?

14
What do you want prepare before he arrives?
1° SURVEY Airway: Intubation equipment incl difficult airway cart, drugs, +/- anasthesia Breathing: RT, bilateral CT set-up Circulation: fluids hung, blood ready, level 1 infuser primed, +/- central access Adjuncts X-ray, FAST, B.W., U/S

15
What’s the best way to mobilize the right people…
Soil your scrubs and hope someone notices and calls for help Call Trauma Code Consult Hospitalist

16
Who do you want? RT, RN’s – 3 ideal, DI techs, U.C. ER res/doc
+/- Level 1 Call-out (trauma, gen surg, ICU) FAST provider – ER IP or Radiology Others: Ortho, NA, SW, Trauma Team Activation 6. ER doc discretion
 FAST provider – ER IP or Radiology. Others: Ortho, NA, SW, Trauma Team Activation. 6. ER doc discretion.")
18
ER #1 FAST ICU Rez Muco Man ER #2/TTL

19
Organizing the Trauma Bay
ONE leader: only leader should be talking and giving orders FMC ER doc 1o survey and stabilization THEN trauma junior/ortho/plastics 2o survey Small rural centers you’re it Be decisive Short window of opportunity for sick patients Rapid decision making important Err on the side of being aggressive Thanks Trevor

20
Learn names and use them Be directive Minimize noise/people in room
Close the Loop Verbalize your findings and thought process. i.e. I think he has a tension PTX – I’m gonna fix it

21
Now what? What do you want to know from EMS?

22
Important Historical Features
MVC Wgt/size vehicle Speed Location of pt in veh ?ejected Mech’m of accident Amt of damage (esp windshield, steering wheel) ?seatbelt (type) Airbag ?Other deaths
 seatbelt (type) Airbag. Other deaths.")
23
Motorcycle Pedestrian vs MVC Assault GSW’s Same + ?helmet Type of gun
Speed Damage to windshield Assault Weapon used ?trajectory ?sexual assault GSW’s Type of gun Handgun: low velocity Rifles: high velocity Type of Ammunition Distance shot from Route of Entry

24
Injury Patterns Frontal/Side Impact Side Impact Rear Impact
MVC versus pedestrian Adult Peds

25
Frontal/Side Impact C-spine Injury Chest: PTX, flail, AoD Abdo: liver/spleen PelvisHip/knee #/disloc Rear Impact Soft-Tissue Injury Neck

26
Ejection No specific pattern, but significant risk of severe injury to all systems MVC versus Pedestrian Adults triad of Tib/fib/femur Truncal injury Craniofacial injury Peds: tend to be run over

27
ATLS overview Preparation Triage Primary Survey (ABCDE’s)
Resuscitation Adjuncts to primary survey and Resus Secondary Survey Adjuncts to Secondary survey Continued post-resus monitoring and R/A Definitive Care

28
Airway LOOK LISTEN FEEL MANAGE A I R W Y Thanks Trevor/Rob LOC
Facial trauma UAW burn Stridor Gurgling Hoarseness Crepitus Tenderness Edema Trachea midline Cervical Collar Temporize: Suction Jaw Thrust OP/NP airways Remove FB Prepare and perform ETT: draw meds, start iv, get BP/ tools Thanks Trevor/Rob

29
Breathing LOOK LISTEN FEEL MANAGE B R E A T H I N G Thanks Trevor/Rob
Resp effort Resp rate Cyanosis Chest wall movements Flail segment AE = Crepitus Tenderness Chest mvmt 100% oxygen BVM Pulse ox Decompress chest Seal open chest wounds Thanks Trevor/Rob

30
Circulation LOOK LISTEN FEEL MANAGE Thanks Trevor/Rob C I R U L A T O
Pale Sweaty LOC External Bleeding JVD Heart Sounds Murmur Pulse rate, Quality Quick feel of abdomen, pelvis, femurs Obtain HR, BP Cardiac and BP monitors Two large iv.s Pressure to external bleeding Bolus crystalloid Blood Consider SOURCE OF BLEEDING Thanks Trevor/Rob

31
Exposure/Environment/Full VS
Disability GCS Pupils Exposure/Environment/Full VS Fully Expose patient Prevent heat loss, warm blankets, warm fluids*

32
*NABISH II (Pre-hospital Enrolment)
")
33
*NABISH II (ED Enrollment)
3. w/i 2 hrs of injury Goal is moderate hypothermia (32-33°) for 48 hr
 for 48 hr.")
34
ATLS overview Preparation Triage Primary Survey (ABCDE’s)
Resuscitation Adjuncts to primary survey and Resus Secondary Survey Adjuncts to Secondary survey Continued post-resus monitoring and R/A Definitive Care

35
Adjuncts X-rays: which ones do you want
Blood Work: which ones do we get routinely Foley, NG: do we need the NG? FAST/dpl: Who can do it? More to come in the future.

36
X-rays CXR C-spine(we’ll come back to this) Pelvis
Do we need to this in every trauma patient? Order others you deem necessary (but if unstable prioritize them until after secondary survey)
")
37
Routine pelvic radiography in severe blunt trauma: is it necessary?
ALL STUDIES ARE LEVEL II or III, so interpret w/caution… Civil ID, Ross SE, Botehlo G and Schwab CW. Ann Emerg Med 17(5): (1988) All patients were classified as unconscious; impaired; awake, alert, and symptomatic; or alert, oriented, and asymptomatic for pelvic fracture on admission. All underwent a plain anterior- posterior radiograph of the pelvis. N=265, 26 pelvic #. 7/26 were unconscious,11/26 were impaired, 8/36 Sx. No fractures were identified in 110 awake, alert, oriented, and asymptomatic patients (P less than .0001). They conclude that pelvic radiographs are required in unconscious or impaired victims of severe blunt trauma and those with signs or symptoms of pelvic fractures but are not required in the awake, alert, and asymptomatic patient. CONCLUSION: Err on the Side of Caution
: (1988) All patients were classified as unconscious; impaired; awake, alert, and symptomatic; or alert, oriented, and asymptomatic for pelvic fracture on admission. All underwent a plain anterior- posterior radiograph of the pelvis. N=265, 26 pelvic #. 7/26 were unconscious,11/26 were impaired, 8/36 Sx. No fractures were identified in 110 awake, alert, oriented, and asymptomatic patients (P less than .0001). They conclude that pelvic radiographs are required in unconscious or impaired victims of severe blunt trauma and those with signs or symptoms of pelvic fractures but are not required in the awake, alert, and asymptomatic patient. CONCLUSION: Err on the Side of Caution.")
38
Preserve clot - minimal movement, gentle handling, minimum of rolling
Preserve clot - minimal movement, gentle handling, minimum of rolling. Punch anyone who tries to 'spring' the pelvis. Fit pelvic belt (elasticated version of the old 'many-tailed-bandage' with velcro fastening) on basis of mechanism of injury. Minimal iv fluid to preserve systolic of 70 (90 mmHg if associated head injury). Take to a hospital that understands the condition! Timothy J Coats MD FRCS FFAEM Senior Lecturer in Accident and Emergency/Pre-Hospital Care Royal London Hospital, UK.
 on basis of mechanism of injury. Minimal iv fluid to preserve systolic of 70 (90 mmHg if associated head injury). Take to a hospital that understands the condition! Timothy J Coats MD FRCS FFAEM Senior Lecturer in Accident and Emergency/Pre-Hospital Care Royal London Hospital, UK.")
39
Trauma/B.W. What blood work do we get when this is ordered?
If you had only one blood test what would it be Sultana or Heather?

40
Trauma/B.W. What blood work do we get when this is ordered?
If you had only one blood test what would it be Sultana or Heather? T&S, T&C What’s the diff? Unmatched – immediate (F: 0-, M: 0-/+) T&S – approx 10 min (screens for ABO &Rh) T&C- approx 30min-1 hr (screens for ABO, Rh, other antibodies)
 T&S – approx 10 min (screens for ABO &Rh) T&C- approx 30min-1 hr (screens for ABO, Rh, other antibodies)")
41
Utility of CBC

42
Utility of CBC Coags Hgb – helpful if low, not helpful if N
Initial hgb fxns more as baseline WBC- who cares Plts-helpful if low Coags Probably useful, some good evidence for HI, ?elderly

43
Lytes 913 Trauma pts bw – 54 had clinically significant abN, only 6 changed Tx (all hypokalemia) authors concluded that a history of hypertension, age older than 50, and a Glasgow Coma Scale (GCS) score less than or equal to 10 appeared to be useful criteria Tortella B, Lavery R, Rekant M. Utility of routine admission serum chemistry panels in adult trauma patients. Acad Emerg Med 1995;2: Cr/BUN No evidence but likely worthwhile, esp if potential for CT and contrast EtOH Allows you to correlate clinical picture with EtOH
 score less than or equal to 10 appeared to be useful criteria. Tortella B, Lavery R, Rekant M. Utility of routine admission serum chemistry panels in adult trauma patients. Acad Emerg Med 1995;2: Cr/BUN. No evidence but likely worthwhile, esp if potential for CT and contrast. EtOH. Allows you to correlate clinical picture with EtOH.")
44
Amylase LFT’s Lactate/Base Deficit Trop No role
Mure A, Josloff R, Rothberg J, et al. Serum amylase determination and blunt abdominal trauma. Am Surg 1991;57: LFT’s No Role in detecting liver injuries Lactate/Base Deficit Multiple studies showing that the higher/more –ve these values are the sicker the patients are and more aggr mngmt is needed – DUHH! Trop No helpful, unless you think it’s the cause of accident For cardiac contusion – may be a role, but not likely in the ED

45
?Trops

46
Case 2 64M, Farmer Brought in by STARS
Bucked off horse, c/o of mild lower abdo/pelvis pain, walked to his house to get help What do you want to do? What do you think is going on?

47
Airway/Breathing N Circulation: BP140/50, HR 80 Disability: GCS- 14, PERLA Exposure - N Rest of vitals N Now what?

48
What films? CXR – Yes Pelvis – Yes (symptomatic)
Can you clear his C-spines clinically? According to CCR? According to NEXUS?

49
Canadian C-spine Rule Stiell. NEJM Dec 2003; 349:

50
S P I N E NEXUS ensorium altered ain the the midline
njury that is distracting N eurologic deficits E tOH, Rx Hoffman et al. NEJM 2000

52
Missed C-spine #’s

53
ATLS overview Preparation Triage Primary Survey (ABCDE’s)
Resuscitation Adjuncts to primary survey and Resus Secondary Survey Adjuncts to Secondary survey Continued post-resus monitoring and R/A Definitive Care

54
Secondary Survey Look, listen and feel when possible
Finger (only one)/tubes in every orifice AMPLE Hx: Systematic: head to toe HEENT Abdomen + GU Maxillofacial Pelvis Neuro (incl CNS/PNS, CN, M/S/R) Vertebral Column (C/T/L) Chest Back CVS Extremeties
/tubes in every orifice. AMPLE Hx: Systematic: head to toe. HEENT. Abdomen + GU. Maxillofacial. Pelvis. Neuro (incl CNS/PNS, CN, M/S/R) Vertebral Column (C/T/L) Chest. Back. CVS. Extremeties.")
55
Back to the Case The trauma jr asks the nurse to put a foley in and she notes Scrotal hematoma Blood at meatus Perineal Ecchymosis Rectal N (and I’ve got short fingers) What do you want to do?
 What do you want to do")
56
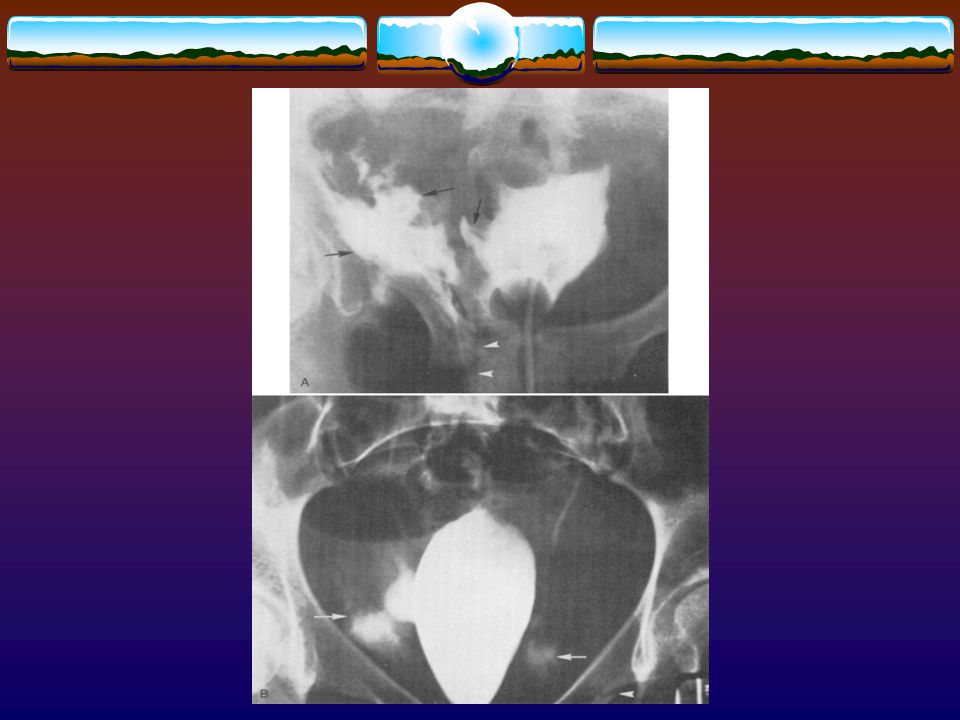
Retrograde Urethrogram
What is it? Retrograde injection of contrast urethral integrity and x-ray How do you do it? Plain KUB 1st Sterile, insert foley 1-2cm, inflate baloon w/2-4cc H20 OR Insert 60cc syringe with x-mas tree adaptor Slowly inject 60cc of radio-opaque dye (avoid forceful inj) Ensure not to spill any (spurious results) Two x-rays, one AP, one lateral/oblique when 10cc left to inject
 Ensure not to spill any (spurious results) Two x-rays, one AP, one lateral/oblique when 10cc left to inject.")
60
Partial tear Complete tear
+/- talk to urology, attempt to pass 12-14F foley If resistance/difficulties, speak to urology – may need suprapubic catheter Complete tear Talk to urology (actually, page them, wait 6 hours and then talk to them) and they’ll likely need a suprapubic catheter
 and they’ll likely need a suprapubic catheter.")
61
Retrograde Cystogram KUB Foley
Gravity fill bladder with 400cc of contrast (age + 2) x 30 for peds AP and Oblique/Lateral x-rays Then AP post-evacuation X-ray
 x 30 for peds. AP and Oblique/Lateral x-rays. Then AP post-evacuation X-ray.")
63
Case # 18M, Story from EMS Brought in from Coventry Hills by STARS who “Scooped and Ran” with him Hx: MVC (car vs cement abutment), prolonged extrication (>1hr), hwy speeds, couldn’t intubate P/E: hypotense, pale, concerned about chest/abdo, bilateral femur #, L humerus
, prolonged extrication (>1hr), hwy speeds, couldn’t intubate. P/E: hypotense, pale, concerned about chest/abdo, bilateral femur #, L humerus.")
64
What do you want to do? Airway: Breathing: Do you want to do anything?
How, ?Rx Breathing: Post-intubation - L DDx: Intervention What if the CXR is N, can they still have a PTX

65
103 PTX, 57 (55%) were not seen on AP CXR
Likely of little significance in the non-ventilated pt But for those who are intubated or going to OR- thought that they may progress One small study, RCT of CT or nothing for oPTX (ventilated and non-ventilated) – NO difference J Trauma Jun;46(6):987-90
 – NO difference. J Trauma Jun;46(6):")
66
Primary Survey What are six(seven) life-threatening injuries you need to identify and Tx in the primary survey?
 life-threatening injuries you need to identify and Tx in the primary survey")
67
Primary Survey What are six(seven) life-threatening injuries you need to identify and Tx in the primary survey? Airway: Obstruction Breathing: Tension PTX Open PTx Massive Hemothorax +/-Flail Circulation Cardiac Tamponade (?Beck’s) Life-Threatening Bleeds
 Life-Threatening Bleeds.")
68
Where’s he bleeding from?
Circulation BP - unable to measure But palpable radials – what’s his BP?, Only Femorals, Only Carotid? Where’s he bleeding from? What are the three big areas you can bleed into? How about kids?

69
Fluid Resus Crystalloids 2 L then blood Level 1 infuser
Goal is sBP 90ish What do you want to do know? RA

70
Summarizing What next? Intubated, needle thoracostomy, no CT yet
L humerus, bilateral femurs, VS pelvic # FAST –ve Gross blood from Foley BP still very tenuous What next? Let the TTL decide - OR

71
What about the kidneys? When do you worry enough about renal injuries to image the kidneys?

72
Nicholaisen G, McAninch J, Marshall G, et al
Nicholaisen G, McAninch J, Marshall G, et al. Renal trauma: Re-evaluation of the indications for radiographic assessment. J Urol 1985;133:

73
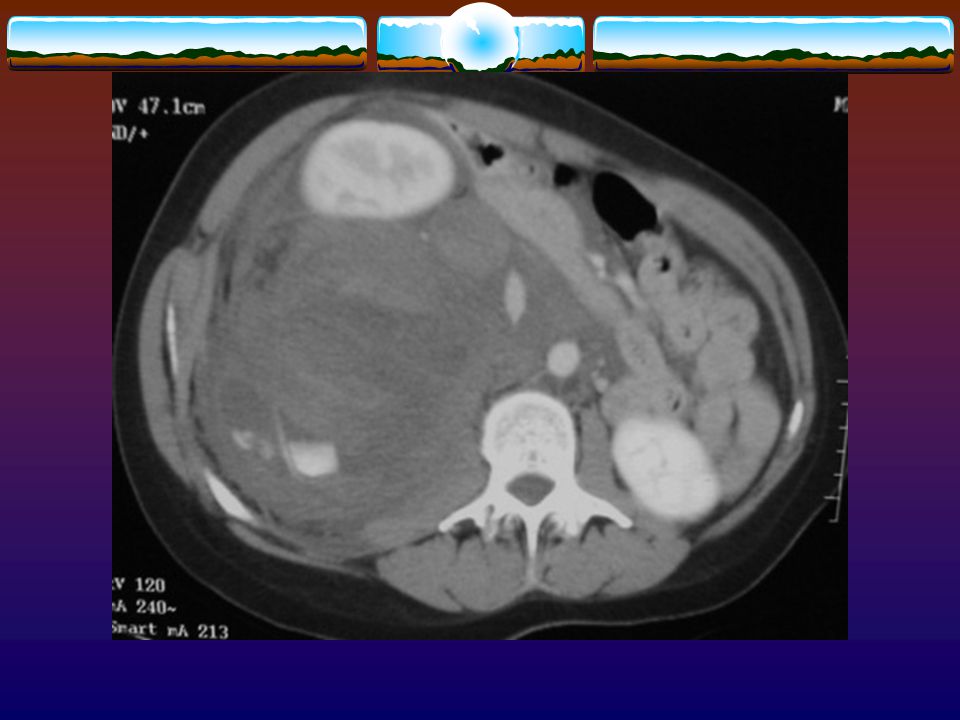
What Grade of Renal Injury?
CT Renal What Grade of Renal Injury?

74
Renal Injury Classification
Grade 1: subcapsular hematoma – non-operative Grade 2: superficial renal laceration with perirenal hemorrhage – non-operative Grade 3: deep laceration w/o extension into the collecting system of the kidney – serial exams, usu non-op Grade 4: parenchymal injury: deep laceration that extends into collecting system, – serial exams, usu non-op, +/- embolization/OR Grade 5: parenchymal injury: multiple deep lacerations that result in a shattered kidney OR Renal Artery Avulsion - OR Harris A., Zwirewich C CT Findings in Blunt Renal Trauma, Radiographics, 2001

75
CT Chest

76
Case #3 27M Transferred from 8th and 8th –
Single stab wound to the right chest. Chest had been needle decompressed Intubated in ED for hypotension Chest Tube on R side.

77
Move onto your secondary survey? CT scanner?
After chest tube (which is not draining any blood) and intubation, his vitals are… BP80/40, HR 120, Sats 100% on vent What do you want to do? Move onto your secondary survey? CT scanner?
 and intubation, his vitals are… BP80/40, HR 120, Sats 100% on vent. What do you want to do Move onto your secondary survey CT scanner")
78
CANNOT MOVE ONTO THE NEXT STEP UNTIL YOU’VE DEALT WITH ALL THE ISSUES.
WHAT ABOUT LOG ROLLING?

81
Case # 4 23F, 28wks pregnant Brought into trauma bay pt begins to c/o of severe cramping VS – 70/30,HR-100, RR-12, sats 94%, c/s-N What do you want to do?

82
Supine Hypotension Syndrome
IVC compression May have vasovagal bradycardia 90% of term pregnant women have COMPLETE obstruction of IVC when supine Mx: tilt spine board, towel roll under on hip, manually displace uterus Thanks Rob

83
PEARL Pregnant patient may lose up to 40% of blood volume before manifesting typical signs of shock. The fetus is compromised before signs of shock.

84
So you put her into the LLD position and she goes into asystolic arrest.
What do you do?

85
Perimortem C-section Indications
Gestation must be at least wks - progress if fundal hgt 25wks ?Less if doing for mom CPR w/no response to other Tx modalities (LLD, fluids, needle chest, ACLS Tx, ) w/i four minutes Ideal, start by four minutes/finish 5 minutes Mother hemodynamics improve considerably
 w/i four minutes. Ideal, start by four minutes/finish 5 minutes. Mother hemodynamics improve considerably.")
86
Procedure Do not stop CPR Don’t prep/drape
Vertical incision from epigastrium to pubis right through peritoneum Scapel to upper uterus, extend with scissors Deliver baby NRP for baby

87
Perimortem C-Section Results
Katz VL. Obstet Gynecol 61 cases b/w that survived TIME NUMBER NORMAL NEUROSQL < >

88
Case #5 69F MVC, restrained driver, hwy speeds PMHx – o
Stable, A & O x 3, ++ agitated

90
When to order CT abdo? Stable: CT abdomen +/- FAST
Abnormal vitals Abdominal pain/tender Unreliable physical examination (EtOH, Rx, HI, SCI, sedated). Inability to do serial examinations Dangerous mechanism of injury Gross Hematuria Stable: CT abdomen +/- FAST Unstable: FAST or DPL
. Inability to do serial examinations. Dangerous mechanism of injury. Gross Hematuria. Stable: CT abdomen +/- FAST. Unstable: FAST or DPL.")
91
What Injuries does CT abdo miss?
Diaphragmatic Pancreatic Bowel Should we add Telebrex then?

92
Oral Contrast in Trauma CT

93
Case #6 57M, working in the Foothills Industrial Area
Working inside a metal structure welding, when a explosion occurred Pt was found unresponsive inside EMS has intubated the patient (for GCS of 3)
")
94
Blast Injuries What injury patterns are seen in Blasts?
What bodily structures would you expect to be involved? What do you want to know about accident scene?

95
Incidence In NA tend to be industry related, accidental (fireworks), bombings/Sept.11
, bombings/Sept.11")
96
1° blast injury is caused solely by the direct effect of blast overpressure on tissue. Air is easily compressible, unlike water. As a result, a primary blast injury almost always affects air-filled structures 2° blast injury is caused by flying objects that strike people.

97
3° blast injuries occurs when people fly through the air and strike other objects.
Miscellaneous blast-related injuries encompass all other injuries caused by explosions, i.e. fires

98
Location is important An explosion that occurs in an enclosed space tends to cause more serious injury. Intensity of an explosion pressure wave declines increasing distance from the explosion. Blast waves are reflected by solid surfaces; thus, a person standing next to a wall may suffer increased primary blast injury.

99
Complications Injuries from projectile objects,
Barotrauma TM’s: perforation, hemotympanum, ossicle # Lungs: PTX, contusion, ARDS GI: pneumoperitoneum, hemotoma, solid organ damage Acute Gas embolism - ?Tx DIC Injuries from projectile objects, Injuries from being thrown (MSK, CNS) Inhalational, Burns, Toxins (CN, CO)
 Inhalational, Burns, Toxins (CN, CO)")
100
Work-Up Look at their TM’s
B.w. – CO/CN if explosion/fire and entrapped, lytes, CXR (PA and Lat) preferred) Urine Serial Abdo Exams or AXR/CT abdo if abdo pain Other tests PRN – CT head as PRN CT head rule
 preferred) Urine. Serial Abdo Exams or. AXR/CT abdo if abdo pain. Other tests PRN – CT head as PRN CT head rule.")
101
Management TM’s – avoid putting stuff in their ears,
Lung – manage PTX as per N If PTX, probably worth monitoring to ensure no contusion develops Belly: high index of suspicion for bowel hematoma – may need to be Admitted for serial exams AGE – LL decubitus, 100% O2, hyperbaric 02, ASA

102
PEA/Asystole 75M MVC, prolonged extrication Lost vitals en route
EMS Unable to intubate What do you want to do? What’s you Ddx for PEA/Asystole? What can we reverse?

103
Intubate Bilateral CT 2L wide open FAST ABG – correct lytes CXR Then decide whether to continue

104
Suicide/Jump from a building
Attempted suicide by jumping off a local seven story downtown building, landed feet first. Brought in by EMS Combative, hypotense, c/o pain at lower extremeties

105
What injury patterns do you look for in this situation?
What x-rays do you want to order? What’s the likelihood of dying from a 4 story fall? 7 story fall? If feet first.

106
Now what? Any other films to order?

107
Where do you usually see spinal #’s
What other films?

109
Why is she hypotense Neurologic shock – but she’s moving here legs
Belly – her abdo FAST is –ve, where else could the blood be Heart – Autopsy study: 33/61 had cardiac injuries and in 16/33, the heart was felt to be cause of death – pericardial /transmural tears, epicardial tears SO, WE SHOULD AT THE HEART w/FAST Blunt Cardiac Trauma Caused by Fatal Falls From Height: An Autopsy-Based Assessment of the Injury Pattern. Journal of Trauma-Injury Infection & Critical Care. 57(2): , August Turk, E E. MD; Tsokos, M MD
: , August Turk, E E. MD; Tsokos, M MD.")
110
Missed injuries

111
Important because… Missed cuz… Long-term disability (i.e. scaphoids)
Litigation Overshadow our heroic measures, “sure they saved my life, but they missed my sprained ankle” Missed cuz… Tx life-threatening stuff 1st Altered sensorium Distracting injuries Inadequate p/e Misinterpretation of investigations

112
MI defined as injury detected >24hrs after A or missed by 3° survey
Intervention: 3° form required to be filled out for ever patient admitted to the TICU or trauma service Results: significant decrease in MI’s post intervention

113
Results

114
Missed Injuries Unavoidable to some extent To prevent… Think of MOI
3° Exam – no studies in ED, but makes sense D/c instructions Interpret your x-rays If they’re not going to trauma – ENSURE NOTHING ELSE IS GOING ON

Similar presentations












>")
 advance ET tube B) needle thoracostomy.>")












