Download presentation
Presentation is loading. Please wait.

1
History Of Oesophageal Surgery
Mr Dipankar Mukherjee Consultant Upper GI & Laparoscopic surgeon QUEENS UNIVERSITY HOSPITAL UK

2
This talk is not about Basic science Non surgical treatment
Benign surgery unless relevant Endoscopic therapy

3
Wide geographical variation
United States 5 cases per United Kingdom 7-10 cases per Iran, China, and Russia over 500 cases per Blot WJ. Epidemiology of esophageal cancer. In Roth JA, RuckdeschelJC, Weisenburger TH, eds. Thoracic oncology. Philadelphia: WBSaunders, 1989;295

4
Rise of adenocarcinoma in Barretts…
30 years ago 10% of oesophageal cancers, it now represents approximately 50% to 70% in the western world

5
Edwin Smith papyrus 3000 to 2500 BC ….The first report
1862 Edwin Smith papyrus 3000 to 2500 BC ….The first report Case 28 of the 48 cases described in this work was entitled "A Gaping Wound of the Throat Penetrating the Gullet" "...if thou examinest a man having a gaping wound in his throat, piercing through to his gullet; if he drinks water he ‘chokes’ (and) it comes out of the mouth of his wound; if it is greatly inflamed so that he develops fever from it, thou shouldst draw together that wound with stitching..."
 it comes out of the mouth of his wound; if it is greatly inflamed so that he develops fever from it, thou shouldst draw together that wound with stitching...")
6
Greece Rome Dark age Islam

7
Paul of Aegina (about 620-690)Alexandrian school
Byzantine Era Paul of Aegina (about )Alexandrian school amputation of the breast for cancer, extirpation of the uterus Tonsillectomy tracheotomy Removal of foreign body from oesophagus some of his descriptions of complicated and difficult operations have been little improved upon even in modern times
Alexandrian school. amputation of the breast for cancer, extirpation of the uterus. Tonsillectomy. tracheotomy. Removal of foreign body from oesophagus. some of his descriptions of complicated and difficult operations have been little improved upon even in modern times.")
8
Challenges: The anatomic remoteness of the thoracic oesophagus Physiologic challenge of intraoperative control of respiration h The history of oesophageal surgery is the tale of men repeatedly losing to a stronger adversary yet persisting in this unequal struggle until the nature of the problems became apparent and the war was won. Emslie 1988 Perspectives in the Development of Oesophageal Surgery

9
1633 Ambrose Pare when the oesophagus was being sutured great care should be taken.

10
Cervical oesophagotomy for FB removal
Hermann Boerhaave ( ) post-mortem examinations to find the cause of fatal illnesses use of the Fahrenheit thermometer The syndrome that is named after him he described in 1724 when Grand Admiral of the Dutch Fleet and Prefect of Rhineland Baron J van Wassenaer died soon after developing chest and abdominal pain after vomiting on a full meal. Boerhaave performed a post-mortem and identified an oesophageal rupture with spillage of gastric contents into the mediastinum (Boerhaave's syndrome 1738 Goursaud and Roland Cervical oesophagotomy for FB removal
 post-mortem examinations to find the cause of fatal illnesses. use of the Fahrenheit thermometer. The syndrome that is named after him he described in when Grand Admiral of the Dutch Fleet and Prefect of Rhineland Baron J van Wassenaer died soon after developing chest and abdominal pain after vomiting on a full meal. Boerhaave performed a post-mortem and identified an oesophageal rupture with spillage of gastric contents into the mediastinum (Boerhaave s syndrome Goursaud and Roland. Cervical oesophagotomy for FB removal.")
11
Leeuwen howek1670 microscope

12
Ignaz Semmelweis Vienna1848
Observation:Friend died of autopsy wound Measurement:Physicians 10% Midwives 3% Hypothesis :"cadaveric particles." Smell not removed by hand washing, but calcium hypochlorite: Result:Ca(OCl)2 reduced puerperal fever death rate 12.4% to 1.27%.
2 reduced puerperal fever death rate 12.4% to 1.27%.")
13
Joseph Lister 1860 antisepsis

14
Late 19th century Age of the German Titans ……Charite ` Berlin lineage
Anesthesia 1846 Langenbeck, Billroth, Kocher Czerny, Polya, Mikulicz, Sauerbruch The pleasure of a physician is little, the gratitude of patients is rare and even rarer is material reward, but, these things never deter the student who feels the call within him"

15
Bernhard Rudolf Konrad von Langenbeck (1810 – 1887):Father of surgical residency
Franko Prussian war of 1870–71 Militär-ärztliche Gesellschaft A forum of military surgeons of all nationality "father of the surgical residency". Berlin a system whereby new medical graduates would live at the hospital as they gradually assumed a greater role in the day-to-day care and supervision of surgical patients. Among his most well-known "house staff" were such illustrious surgeons as Billroth and Emil theodore Kocher

16
…..And the great nephew of Langenbeck Theodor Billroth (1829-1894)
First oesophagectomy in animal Adenoma carcinoma sequence 1855 First laryngectomy1874 Billroth I gasrectomy1881 Prolonged apprenticeship Animal and cadaveric dissection Study of surgical literature Polya Czerny Mikulicz sauerbruch Halstead

17
Theodor Kocher ( ) Vincenz Czerny (1842 – 1916) 1877, first “surgeon” to successfully resect a cervical oesophageal cancer
 Vincenz Czerny (1842 – 1916) 1877, first surgeon to successfully resect a cervical oesophageal cancer.")
18
Johann von Mikulicz-Radecki 1850-1905
Skin tube 1886 oesophagoscope Listerism Respiratory studies

19
(Ernst) Ferdinand Sauerbruch..The Dark Lord..
German surgeon, Marburg, Zürich, München, Berlin , born in Bremen, died in Berlin Sauerbruchs chamber 1904 Limb prosthesis Tuberculosis diet

20
William Halstead (1852-1922) John Hopkins
William Halstead ( ) John Hopkins.. Brings experimental surgery and apprenticeship to America Student of John Dalton a pioneering experimental physiologist Theodore billroth 1889 technique of inguinal hernia repair early 1890s radical mastectomy for breast cancer 1892 he described ligation of the subclavian artery. Early 1900s he published on autotransplantation of the parathyroid gland.. Fallen Hero
 John Hopkins.. Brings experimental surgery and apprenticeship to America. Student of. John Dalton a pioneering experimental physiologist. Theodore billroth technique of inguinal hernia repair. early 1890s radical mastectomy for breast cancer he described ligation of the subclavian artery. Early 1900s he published on autotransplantation. of the parathyroid gland.. Fallen Hero.")
21
Story of anaesthesia AD 220 the Chinese surgeon Hua
surgical anaesthesia. In 1526 Paracelsus ether (which he knew as oleum vitreoli dulce) could quieten chickens and relieve pain. In Birmingham in 1772 Priestley, a Unitarian minister, discovered nitrous oxide 1825Charles Waterton Published wanderings in South America accurate account of curare.
 could quieten chickens and. relieve pain. In Birmingham in 1772 Priestley, a Unitarian. minister, discovered nitrous oxide. 1825Charles Waterton. Published wanderings in South America. accurate account of curare.")
22
1677 Robert hooke maintained life in dogs by bellows
1775 John Hunter two way air flow 1846 Morton 1853 simpson Magill & Rowbotham Sauerbruch Negative pressure airtight chamber Brauer and Peterson CPAP Positive pressure chamber Endotracheal anaesthesia

23
…Penicillin saga Fleming A. On the antibacterial action of cultures of a penicillium with special reference to their use in the isolation ofB influenzae. BrJExp Pathol 1929;10: Chain E, Florey HW, Gardner AD, Heatley NG, Jennings MA, Orr-EwingJ, Sanders AG. Penicillinasa chemotherapeutic agent. Lancet 1940;ii:226-8.

24
FirstTransthoracic resection Endotracheal anaesthsia Oesophagectomy
Franz Torek 1913 FirstTransthoracic resection Endotracheal anaesthsia Oesophagectomy without reconstruction 12 year survival Torek F. The first successful case of resection of the thoracic portion of the esophagus for carcinoma. Surg Gynecol Obstet, 1913;16:614

25
Attempts at Reconstruction
1907 Dr. Cesar Roux (famous for the Roux-Y operation) use of jejunum as a substitute for the esophagus 1911, Kelling fi rst successful case of cervical oesophagocolostomy usimg transverse colon 1920, Kirschner successful oesophago gastrostomy in the neck, pulling up a gastric pedicle through a subcutaneous route. in a patient who had swallowed lye and had a stricture
 use of jejunum as a substitute for the esophagus. 1911, Kelling. fi rst successful case of cervical oesophagocolostomy usimg transverse colon. 1920, Kirschner. successful oesophago gastrostomy in the neck, pulling up a gastric pedicle through a subcutaneous route. in a patient who had swallowed lye and had a stricture.")
26
Between the great wars Ohsawa 1933
series of resections with immediate anastomosis‘ Over a period of seven years, in a series of 101 cases, he found 18 in which the growth involved the lower oesophagus or cardia and in which he was able to carry out resection and oesophago gastric anastomosis. Eight of these patients survived.

27
Between the great wars…..
Grey Turner 1933: prodigious writer and a lone Ranger Transhiatal Resection Vice-President Royal College of Surgeons of England, HunterianOrator and Hunterian Trustee. President of the Association of Surgeons United States : Murphy Oration Balfour Oration Only British surgeon to be awarded the Bigelow Medal. GREY TURNER AND THE EVOLUTIONOF OESOPHAGEAL SURGERY R. H. FRANKLIN F.R.!C.S. Ann. Roy. Coll. Surg. Engl. 1971, vol. 49)
")
28
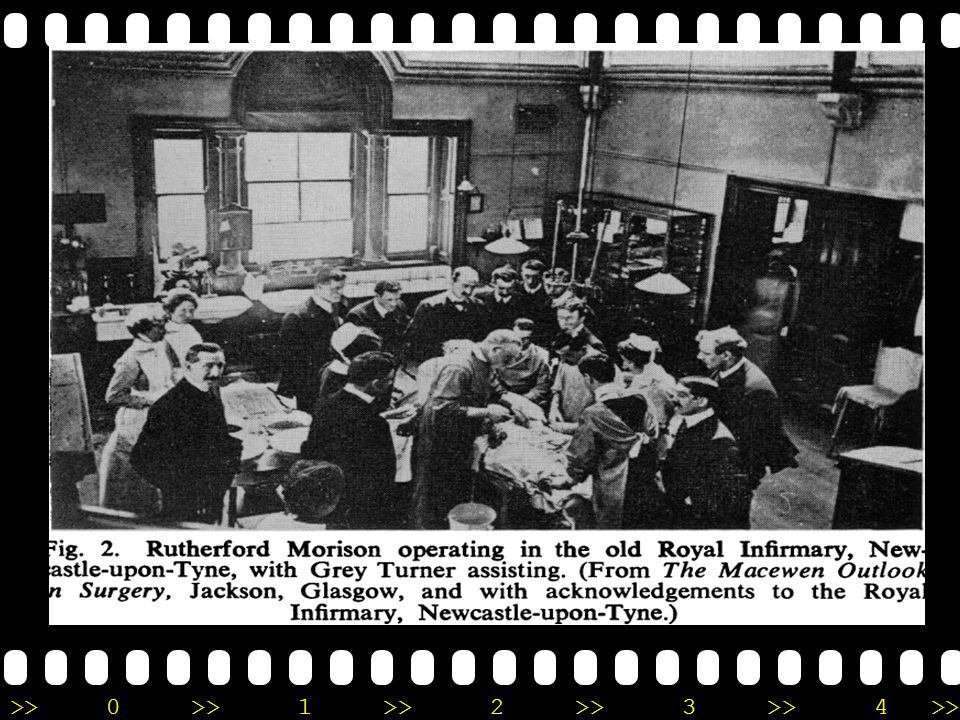
End of the old era and the opening of a new one.
'Finally came the great day of my long-looked-for pilgrimage to Glasgow. In 1901 my appendix had to be removed, As soon as I entered the operating theatre where Macewen was about to start work, it seemed like a new world to me; and I have never forgotten the tall, handsome figure standing by the basin washing his hands with the most punctilious care. To me it seemed wonderful that in those days someone should come in and inoculate culture media from beneath the surgeon'sthe surgeon's nails. 'It was not that the work in Newcastle-upon-Tyne was of a poor standard, for I yield to no one in my esteem for Rutherford Morison. But our theatre was not a sacred place, withoutany of the ritual associated with a surgical operation as we know it to-day, or as Macewen knew it and practised it in those days. All our sterilisation was by immersion in strong antiseptics, nothing was boiled and the arrangements were of the simplest.

30
Grey Turner 1933 successful Transhiatal resection
Radicalism 'better todo too much than too little' care Better a living problem than a dead certainty Patient focus 'Gentlemen, you are probably saying to yourselves this is only anAppendicectomy -but I can assure you that this is the most important operation being carried out to-day-for this particular patient.‘ decimalization and metrication. vision 'One day they will operate on the heart-mark my words'; 'We shall never overcome cancer by surgery, it will be by something we shall inject Grey Turner successful Transhiatal resection

31
Following Grey turner & Ohsawa
1938, Adams and Phemister lower oesophagectomy and immediate oesophagogastrostomy through open thoracotomy1933,Osawa at Kyoto University First successful cases worldwide of the same procedure Garlock 1944 Sweet1948 worldwide leaders of oesophageal surgery in the middle of the twentieth century, succeeded in oesophago gastrostomy in the thoracic cavity Oshawas left thoracoabdominal technique remained a dangerous procedure for mid oesophageal tumoursGARLOCK, J. H. (1944) Surg. Gynec. Obstet. 78, 23.
 Surg. Gynec. Obstet. 78, 23.")
32
Status of surgical treatment for esophageal cancer worldwide, 1965
T. Kakegawa, MD · H, Fujita, Gen Thorac Cardiovasc Surg (2009) 57:55–63 Cases of resection (%) Operative mortality (%) Cases of 5-year survival (%) Garlock (39.6%) % (21.2%) Sweet (52.1%) % (12.1%) Ellis (27.0%) % (17.2%) Logan (59.7%) % (23.0%) Petrov (19.0%) % (11.5%) Berezov (29.2%) % Wu (40.1%) % (23.7%) Kuo (12.7%) % Lortat-Jacob 308 (54.8%) % (6.2%)
 57:55–63. Cases of resection (%) Operative mortality (%) Cases of 5-year survival (%) Garlock 181 (39.6%) 31.5% 11 (21.2%) Sweet 303 (52.1%) 17.5% 18 (12.1%) Ellis 245 (27.0%) 15.9% 20 (17.2%) Logan 418 (59.7%) 30.0% 57 (23.0%) Petrov 123 (19.0%) 50.0% 7 (11.5%) Berezov 770 (29.2%) 33.5% Wu 152 (40.1%) 18.4% 6 (23.7%) Kuo 150 (12.7%) 9.3% Lortat-Jacob 308 (54.8%) 32.8% 13 (6.2%)")
33
…..Joining up the gullet : the War years folowers of ohsawa and Grey Turner
1937 Nissen First successful anastomosis reported a case of transthoracic cardio-oesophageal resection for penetrating ulcer, and this was probably the first successful anastomosis in Europe and the Americas. 1938 Adams and Phemister : First one stage resection but most oesophageal surgeons continued to practise the twostage procedure, ADAMS, W. E., and PHEMISTER, D. B. (1938) J. thorac. Surg. 7, 621. 1942 Brock: The first follower carried out a successful one-stage resection and anastomosis for a patient with a large myoma. BROCK, R. C. (1942) Brit. J. Surg. 30, 146. 1945 Vernon Thompson: First UK success The first patient with a carcinoma to be treated successfully in this way in the UK THOMPSON, V. C. (1945) Brit. J. Surg. 32, 377.
 J. thorac. Surg. 7, Brock: The first follower. carried out a successful. one-stage resection and anastomosis for a patient with a large myoma. BROCK, R. C. (1942) Brit. J. Surg. 30, Vernon Thompson: First UK success. The first patient with a carcinoma to be treated successfully in this way in the UK. THOMPSON, V. C. (1945) Brit. J. Surg. 32, 377.")
34
Post war years

35
1946, The watershed: Transthoracic resection
Lewis I. Hunterian lecture The surgical treatment of carcinoma of the oesophagus with special reference to a new operation for growths of the middle third. Br J Surg, 1946;34:18 Inspiration to be a doctor severe attack of acute appendicitis at the age of I2-being operated upon by David Ellis of Aberystwyth 1939First successful pulmonary embolectomy in the UK

36
Olympus: Going Where no Camera has Gone Before
The Pain in the Butt Camera Olympus gastrocamera 1960

37
Ronald Belsey TO Fistula Zenkers Diverticulum Antireflux procedure
Belsey R. Reconstruction of the esophagus with left colon. J Thorac Cardiovasc Surg 1965;49:33-55. Zenkers Diverticulum The American Association for Thoracic Surgery in 1966, emphasized a dysfunction of the cricopharyngeal muscle as the underlying cause series of 45 patients, the majority of them treated with myotomy and diverticulopexy Antireflux procedure Belsey Mark IV Cancer “cure is an accident"

38
1976 :Total oesophagectomy
McKeown KC. Total three stage oesophagectomy for cancer of the oesophagus. Br J Surg, 1976;63:259

39
Poor results : Earlam R, Cunha-Melo Jr. Oesophageal squamous cell carcinoma. 1. A critical review of surgery. Br J Surg, 1980;67:381 Muller JM, Erasmi H, Stelzner M, Zieren U, Pichlmaier H. Surgi cal Therapy of Oesophageal Carcinoma. Br J Surg, 1990;77:845

40
Rt Vs Left Thoracotomy Similar results mortality and survival
Launois P, Lygidakis C, Malledant G. Results of the surgical treatment of carcinoma of the esophagus. Surg Gynecol Obtet, 1983;156:753 Similar results mortality and survival reflux more in left

41
Total vs Subtotal stricture more in cervical anastomosis
Chasseray VM, Kiroff GK, Buard JL, Launois B. Cervical or thoracic anastomosis for esophagectomy for carcinoma. Surg Gynecol Obstet, 1989;169:55 stricture more in cervical anastomosis

42
Which conduit? Gastric Colon Greater curve tube

43
Anastomosis:Staples or handsewn
Stricture more in stapled

44
How radical is radical? Skinner DB, Dowlatashy KD, DeMeester TR.
80 patients radical Enbloc resection 9 (11%) 30 day mortality Potentially curablecancer of the esophagus. Cancer, 1982;50:2571 Wong J. Esophageal resection for cancer: the rationale of current practice. Am J Surg, 1987;153:18
 30 day mortality. Potentially curablecancer of the esophagus. Cancer, 1982;50:2571. Wong J. Esophageal resection for cancer: the rationale of current. practice. Am J Surg, 1987;153:18.")
45
20 years in Chiba University
Seo and OsawaJapan surgical society 1932 Review of world literature before 1942 worldwide incidence of operative mortality up to 1932 144 (95.4%) of the 155 patients No sucessful reconstruction Hiroshi Akiyama Nakayama Japan Surgical Society 1951 incidence of operative mortality was only 5 (16.6%) of 30 patients who underwent subtotal esophagectomy followed by esophagogastrostomy through a subcutaneous route for cancer in the upperor middle thoracic esophagus .
 of the 155 patients. No sucessful reconstruction. Hiroshi Akiyama Nakayama Japan Surgical Society incidence of operative mortality. was only 5 (16.6%) of 30 patients who underwent subtotal. esophagectomy followed by esophagogastrostomy. through a subcutaneous route for cancer in the upperor middle thoracic esophagus. .")
46
Three Japanese masters 1951-1966
Nakayama and Sato Chiba University : Multistage procedure The operativemortality rate oesophagectomy % of 30 patients % of 2053 patients Katsura at Tohoku University 8/15 55% mortality using positive pressure 0/21 0% using endotrachaeal anaesthesia Akakura at Keio University, 1966 JATS presidential lecture : average operative mortality rate in Japan was 15.6% ,861 of 5327 average 5-year survival rate was 12%

47
Problems to be resolved in oesophageal surgery
Akakura keio University : Problems to be resolved in oesophageal surgery 1. Causes of short-term mortality 1) Incorrect indication for surgery 2) Incorrect adoption of surgical procedures 3) Incorrect surgical maneuver Postoperative complications a. Anastomotic leakage b. Pulmonary complication(s) c. Circulatory failure 2. Causes of long-term mortality 1) Non-curative surgery a. Incomplete resection of a local tumor b. Lymph node metastasis c. Distant organ metastasis 2) Malnutrition 3) Diseases of the elderly
 Incorrect indication for surgery. 2) Incorrect adoption of surgical procedures. 3) Incorrect surgical maneuver. Postoperative complications. a. Anastomotic leakage. b. Pulmonary complication(s) c. Circulatory failure. 2. Causes of long-term mortality. 1) Non-curative surgery. a. Incomplete resection of a local tumor. b. Lymph node metastasis. c. Distant organ metastasis. 2) Malnutrition. 3) Diseases of the elderly.")
48
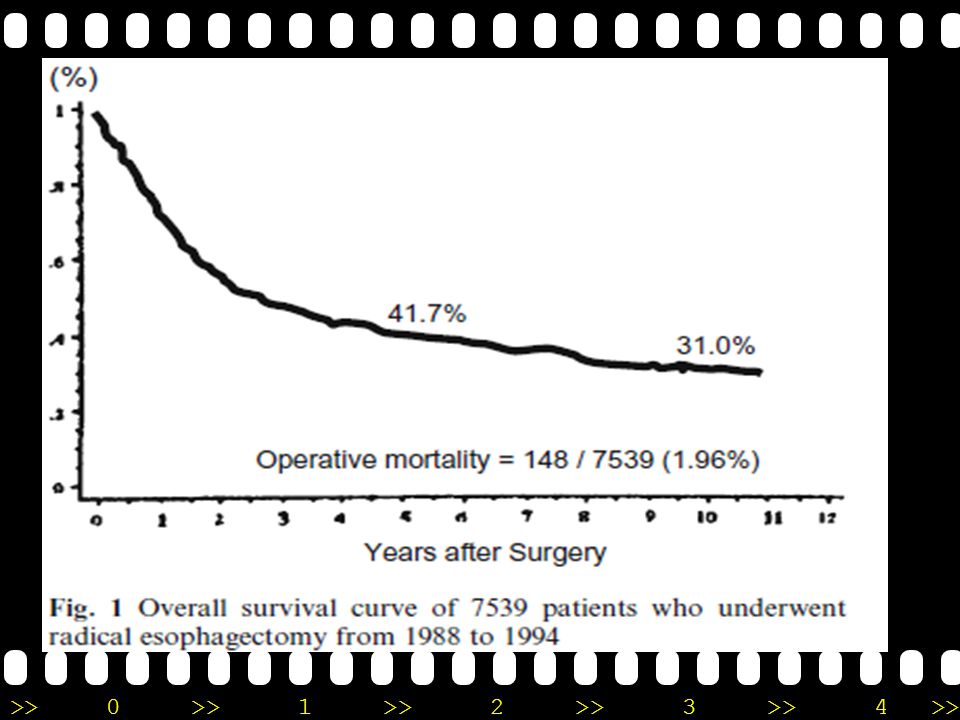
Specialisation JSED : oesophageal Registry 5-year survival rate % 41.9% 10-yearsurvival rate 1994: 31.0 % operative mortality 1994: 2% of 7539 patients

50
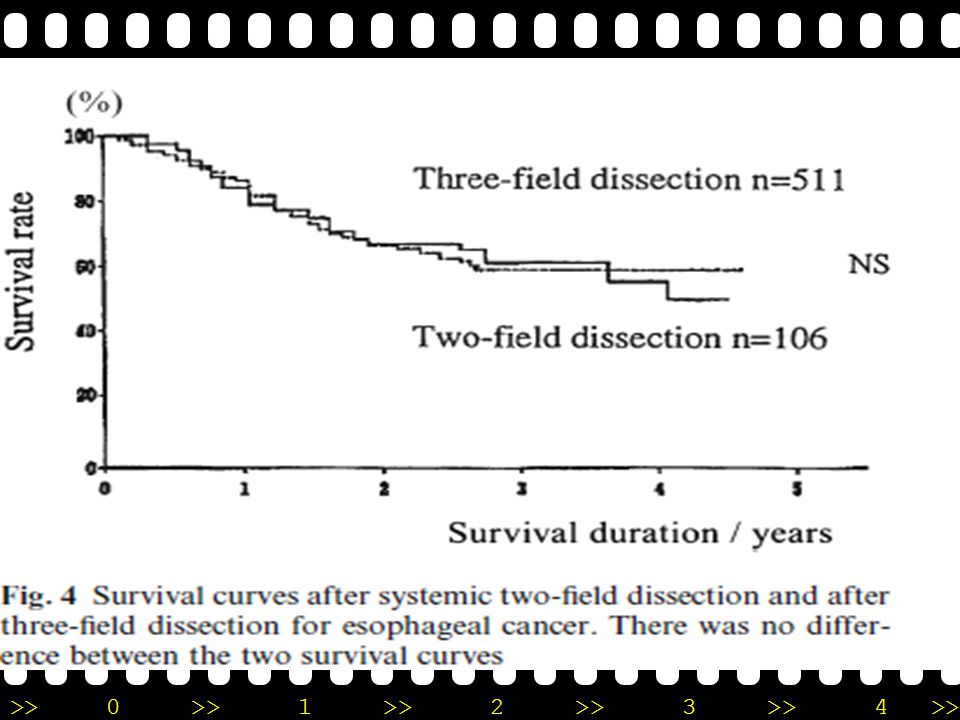
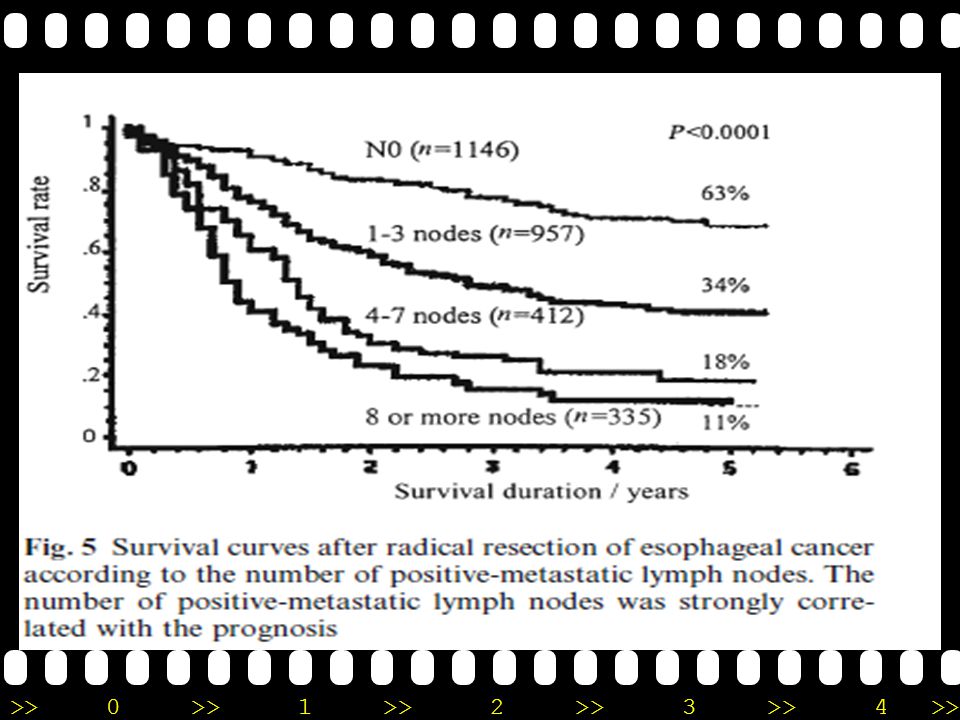
Early Vs Advanced: Lymph Nodal spread Recurrent laryngeal and paracardiac sentinel nodes? Kakegawa 1994

51
Lymphadenectomy Recurrent laryngeal chain

54
Transhiatal Resection
Denk in 1913, Refined by Turner in 1931 Popularised by Orringer 1978

55
Transhiatal oesophgectomy
University of Michigan Hospitals,Ann Arbor, MI. 1.Orringer MB, Sloan H: Esophagectomy without thoracotomy. J Thorac Cardiovasc Surg 76:643, 1978 2. Orringer MB, Orringer JS: Esophagectomy without thoracotomy: a dangerous operation? J Thorac Cardiovasc Surg 85:72, 1983 3. Omnger MB: Transhiatal blunt esophagectomy without thoracotomy. In Cohn LH (ed): Modem Technics in Surgery: Cardio-Thoracic Surgery. Mt. Kisco, NY, Futura, 1983, vol 62, installment 9 4. Omnger MB: Partial median sternotomy: anterior approach to the upper thoracic esophagus. J Thorac Cardiovasc Surg 87:124, 1984 Mark Orringer
: Modem Technics in Surgery: Cardio-Thoracic Surgery. Mt. Kisco, NY, Futura, 1983, vol. 62, installment Omnger MB: Partial median sternotomy: anterior approach. to the upper thoracic esophagus. J Thorac Cardiovasc Surg. 87:124, Mark Orringer.")
56
Orringer MB, Orringer JS: Esophagectomy without thoracotomy:
a dangerous operation? J Thorac Cardiovasc Surg 85:72, 198

57
Orringer MB, Orringer JS: Esophagectomy without thoracotomy:
a dangerous operation? J Thorac Cardiovasc Surg 85:72, 198

58
200 patients AverageBlood loss <1000 ml Hospital mortality 6%.

59
11 years of Laparoscopic oesophageal surgery
1991, Dallemagne et al and Geagea Laparoscopic fundoplication 1991 Shimi et al Laparoscopic esophageal myotomy. 1993, Cuschieri et al outcome of Laparoscopic fundoplication > 100 patients multicenter study

60
Antoon Lerut Leuven Student of Ronald Belsey Bristol James Luketich philadelphia

61
Staging : Evolution in the west
CT and EUS Tio TL, Cohen P, Coene PP. Endosonography and computed tomographyof esophageal carcinoma. Gastroenterology, 1989;96:1478 Grimm H, Soehendra N, Hamper K. Contribution of endosonographyto preoperative staging in esophageal and stomach cancer. Chirurg, 1989;60:684 Gastroenterology, 1989;96:1478 Rankin SC, Taylor H, Cook GJ, Mason R. Computed tomographyand positron emission tomography in the pre-operative staging of oesophageal carcinoma. Clin Radiol, 1998;53:659 Thoracoscopy Krasna MJ, Reed CE, Jaklitsch MT. Thoracoscopic staging of esophageal cancer: a prospective, multiinstitutional trial. Cancer and Leukemia Group B Thoracic Surgeons. Ann Thorac Surg, 1995;60:1337

62
MDT Ajani JA. Current status of new drugs and multidisciplinary approaches in patients in patients with carcinoma of the esophagus. Chest, 1998;113:112S

63
Collaboration not competition
Ando N, Iizuka T, Kakegawa T. A randomized trial of surgery wit hand without chemotherapy for localized squamous carcinoma of the thoracic esophagus. J Thorac Cardiovasc Surg, 1997;114:205 Teniere P, Hay JM, Fingerhut A. Postoperative Radiation does no t increase survival after curative resection for squamous cell cancer ofthe middle and lower oesophagus as shown by a multicenter controlled trial. Surg Gynecol Obstet, 1991;173:123 Leprise E, Etienne PL, Meunier B. A randomized study of chemotherapy, radiation therapy, and surgery versus surgery for localizedsquamous cell carcinoma of the esophagus. Cancer, 1994;73:1779

64
Chemoradiation increased survival
Walsh TN, Noonan N, Hollywood D. A comparison of multimodaltherapy and surgery for esophageal adenocarcinoma. N Engl J Med 1996;335:462 Forastiere AA, Orringer MB, Perez-Tamayo C, Urba SG, ZahurakM. Preoperative chemoradiation followed by transhiatal esophagectomy for carcinoma of the esophagus: final report. J ClinOncol, 1993;11:1118

65
Junctional tumour: Siewert Type

66
Today Minimal access EMR ESD PDT Chemoradiation Biological therapy
Multimodality treatment New treatments?

67
Please do not walk away when you stumble onto it…
Introduction of modern surgical techniques should lead to a paradigm shift in the mindset of the referring clinicians Things do not change; we change

Similar presentations