Download presentation
Presentation is loading. Please wait.

1
Presented by Lutheran Services Florida Health Systems
Critical Incidents / IRAS Incident Reporting and Analysis System A training for SAMH providers in Circuits 3, 4, 5, 7, 8 Presented by Lutheran Services Florida Health Systems Good morning everybody, this is Bryan Mingle, quality improvement specialist at LSF and your presenter for the hour. I’ll do a roll call in a couple more minutes … give everybody who said they’d be calling in today a chance to log in. ALLOW SILENCE ….. OK, let’s get started with our training today on Critical Incident Reporting into the IRAS. Some introductions, first. Here with me is Clinical Care Manager Erin Whitaker-Houck, whose name you may have seen flash as the GotoMeeting presenter. I am borrowing her meeting license October 2014

2
Please mute your phone and monitor area – unless you’re speaking
Hold most questions until the end of the presentation, but they are encouraged during the FAQ portion This PowerPoint will be posted on the LSF web site – – under Resources tab Staff training offsite; QI staff onboarding Before we get started, a few housekeeping items … A lot of what we’re going to be going over today we first looked at last October –we’ve all learned a lot since then, sometimes from mistakes and often those are the best lessons. I reached out to DCF’s IRAS liaison in the last year – a lot -- and she provided an FAQ addressing many areas we’re going to look at today. I think you’ll find that really helpful – I’ve gone over a lot of this material with many of you individually. We also are going to ask that new staffers be trained with this information; LSF will be posting this under the RESOURCES tab of the new web site https//:lsfhealthsystems.org . If you need it soon, I can you this PowerPoint; shoot me an requesting it for staff trainings in October. Housekeeping

3
DCF’s mission: Protect the vulnerable and promote recovery and resiliency
The State of Florida has developed an entire operating procedure around IRAS and critical incident reporting (CFOP 215-6). CFOP adherence = compliance The Department’s contract with the M.E. requires that we support and manage the critical incident reporting in our region. We are all held accountable contractually. Bottom line, what we all know: compliance with critical incident reporting is very important in the System of Care. If you do it inadequately, consumer safety and welfare are at risk, and then so is your ability to deliver services. Why We Care
. CFOP adherence = compliance. The Department’s contract with the M.E. requires that we support and manage the critical incident reporting in our region. We are all held accountable contractually. Bottom line, what we all know: compliance with critical incident reporting is very important in the System of Care. If you do it inadequately, consumer safety and welfare are at risk, and then so is your ability to deliver services. Why We Care.")
4
Incident Reporting & Analysis System
Timely notification of critical incidents to LSF/DCF 24 HOURS, 24 HOURS, 24 HOURS to Submit into the Incident Reporting & Analysis System Details of the incident and the immediate actions taken. Tracking and analysis of incident data. IRAS is only as good as the data we put in it. Today we’ll be going over what defines a critical incident – the categories. We’ll also look at what kind of detailed information we are looking for in order to analyze data and identify trends and gaps in care. In the last year, I’ve worked with many of you in deciding what meets the definition of a critical incident. As a result, data is changing in the numbers alone. Example: one agency before this year was reporting all transports from their facility to hospitals. Broken toes, flu, etc. NO. Significant Injury to Clients or Staff means life-threatening or potential loss of life or limb. Let’s look closer at the data collected from the last year. What IRAS Provides

5
Reporting and Analysis
Your reports and data identify trends and can lead to improvements in policy and procedures. Again, big picture: What you document can make a difference in the process change that will occur in the behavioral health system of Florida. You guys have done a great job all year with policy changes and reporting improvements.

6
PROVIDER DATA – ACCURACY COUNTS
Type of Incident July Aug Sept Oct Nov Dec Jan Feb Mar Apr May June FY 13-14 Adult Death Child Arrest Child Death Child-on-Child Sexual Assault Elopement Employee Arrest Employee Misconduct Escape Missing Child Security Incident-Unintentional Sexual Abuse/Sexual Battery Significant Injury to Client Significant Injury to Staff Suicide Attempt Other Monthly Total: Fiscal Year Total: 278 As a Managing Entity, we track INCIDENT TYPES entered into IRAS. Which you cannot edit or correct once you select a category. Please doublecheck your IRAS screen many times befeore you hit CONTINUE, please. The dropdown bar can pull up without you noticing it. Edit yourself, please, because once saved, information cannot be changed. The data reports become skewed and less meaningful. Here is the fiscal year breakdown. Total 278. OF THESE 278, 26 were not reportable. They included minor injuries, reports of sexual abuse that were historic, mandatory for an Abuse Hotline call but not a critical incident today. Also included were altercations or minor injuries. Yes, they are internal incident reported to your supervisor and onto risk management, but not critical to report to DCF. PROVIDER DATA – ACCURACY COUNTS

7
Contract Requirement: SUBMIT WITHIN
Here’s an example from last fiscal year’s 3rd and 4th quarters. There were 86 critical incident reports each of those quarters. In 3rd quarter, 20 failed timeliness. That wasn’t one of our most compliant quarters. It improved in the 4th quarter – when 12 of 86 incidents reported were entered after the 24 hour requirement. This year we are focusing heavily on 24-HOUR timeliness WHICH INCLUDES WEEKENDS AND HOLIDAYS – invitations to improve, a.k.a. Corrective Action Plans, are being issued after 2 failed timeliness reports. When you don’t make compliance, we don’t either as an agency. Contract Requirement: SUBMIT WITHIN 24 HOURS, including weekends and holidays or Date of Discovery

8
Don’t let the IRAS software system scare you out of your seat
If you are new to IRAS, LSF, DCF and your IT Desk are here to troubleshoot problems you may have and provide guidance to help you master this reporting system. Let’s back up a bit. For any new people on the call today and for supervisors who will train backups: The first step is getting registered to use IRAS. Your contract requires you to have a designated IRAS reporter and a backup. We have found it works to have a weekend manager on duty with access to IRAS or an IRAS reporter when Friday night or Saturday critical incidents occur. This is where we have the most failed timeliness. When all else fails, you can call the LSF Access to Care Line, 24/7 on weekends, too, and we will work to make sure the report is entered within the 24-hour window.

9
Registration for Users: a Step-by-Step Process
You must be registered before you can report online into IRAS. Follow the steps on Plan ahead; it can take several days/weeks depending on DCF data office’s workload. Aventail must be installed on your desktop. How do you get access and what are your responsibilities? This web page is very helpful to new users. It outlines what to do step by step. Basically you must complete 2 online courses – Security Awareness and DCF’s HIPAA online course. And there’s an enrollment form to complete and get signed by your supervisor. You attach these to an to DCF’s Janice McIntyre. If you are in a situation where you are having technical issues and/or no one is yet registered, call me at the LSF office number weekdays and you can dictate the incident to me and I can enter it into IRAS. We do our due diligence so this doesn’t happen, but it will on occasion. On the weekends, call the Access to Care Line, please It’s on a slide coming up, too

10
IMPORTANT REMINDER: Once DCF’s data liaison specialist (Janice McIntyre) sends you the Aventail and DCF Web Portal password to use IRAS, you must sign in with it within 3 days or that password expires. You don’t want this to happen. There is a RESET password button for when you forgot or misplaced your password. However, after 30 days it will expire (tip: LOG IN AT LEAST ONCE A MONTH TO THE IRAS SYSTEM) and you will need to call the HELPDESK. Save yourself that call! 72-HOUR WARNING!
 and you will need to call the HELPDESK. Save yourself that call! 72-HOUR WARNING!")
11
Now that you’re registered…
Provider contractual responsibilities Report directly into IRAS within 24 hours of the incident occurring or, in some off-site situations, within discovering that the incident occurred. This includes weekends and holidays. In addition, if a consumer death occurs on-site, providers must notify LSF by telephone within 24 hours. Calling also applies to three more categories of incidents: elopement of a child, elopement of a court-ordered adult and any incident involving active media involvement. CALL (the LSF Access to Care Line) and an LSF Clinical staffer will answer after business hours The CFOP still states one business day, but the Managing Entity is requiring 24 hours to ensure reporting on weekends and holidays. This is because the language in OUR contract with DCF states 24 hour, so we are passing onto providers so we all can be in compliance. Timeliness – we can’t stress its significance enough. Also, it is a provider responsibility to notify the Managing Entity when your agency’s designated IRAS reporter leaves and a new one has been assigned. Please or call me. Now that you’re registered…
 and an LSF Clinical staffer will answer after business hours. The CFOP still states one business day, but the Managing Entity is requiring 24 hours to ensure reporting on weekends and holidays. This is because the language in OUR contract with DCF states 24 hour, so we are passing onto providers so we all can be in compliance. Timeliness – we can’t stress its significance enough. Also, it is a provider responsibility to notify the Managing Entity when your agency’s designated IRAS reporter leaves and a new one has been assigned. Please or call me. Now that you’re registered…")
12
Tools Lots of training for IRAS, beyond what we’re doing today even. (ABOVE) We won’t repeat what the online webinar tool (found once you gain access to the DCF Web Portal) does so well. About this video, I urge you to take 38 minutes of your day for it. How many of you have seen this? There is no image for about 2 minutes and then the screen appears and leads you through each IRAS screen. Since we’re here in a training, there are some common mistakes which I am going to review now because they keep happening. RECOMMENDED: A 38-minute video that takes you tab by tab through entering an IRAS report. A helpful User Guide is on the DCF IRAS site. You can link to it once signed on. OR you can print it out and keep it near your computer.
 We won’t repeat what the online webinar tool (found once you gain access to the DCF Web Portal) does so well. About this video, I urge you to take 38 minutes of your day for it. How many of you have seen this There is no image for about 2 minutes and then the screen appears and leads you through each IRAS screen. Since we’re here in a training, there are some common mistakes which I am going to review now because they keep happening. RECOMMENDED: A 38-minute video that takes you tab by tab through entering an IRAS report. A helpful User Guide is on the DCF IRAS site. You can link to it once signed on. OR you can print it out and keep it near your computer.")
13
The proper use of Date of Discovery as Incident Date (above):
Off-site only, within the last 30 days of treatment/service

14
This shows the order you enter information after the BRIEF DESCRIPTION on Face Sheet. Remember to add PEOPLE INVOLVED. When entering additional relevant data (diagnoses, last date of service, clinical response, who was notified etc) type in Comments box and SAVE COMMENTS. Then, in order to SEND this report to DCF/LSF, you must click on NOTIFICATIONS (highlighted above). If you don’t send, no one is notified by for review.
 type in Comments box and SAVE COMMENTS. Then, in order to SEND this report to DCF/LSF, you must click on NOTIFICATIONS (highlighted above). If you don’t send, no one is notified by for review..")
15
If there are no notifications records, this report has not been sent to DCF/LSF. You must click on SEND INITIAL INCICDENT REPORT

16
Your screen should then look like this after you click on NOTIFICATIONS and click on Initial Incident Report. Then you will see this (next screen)
.")
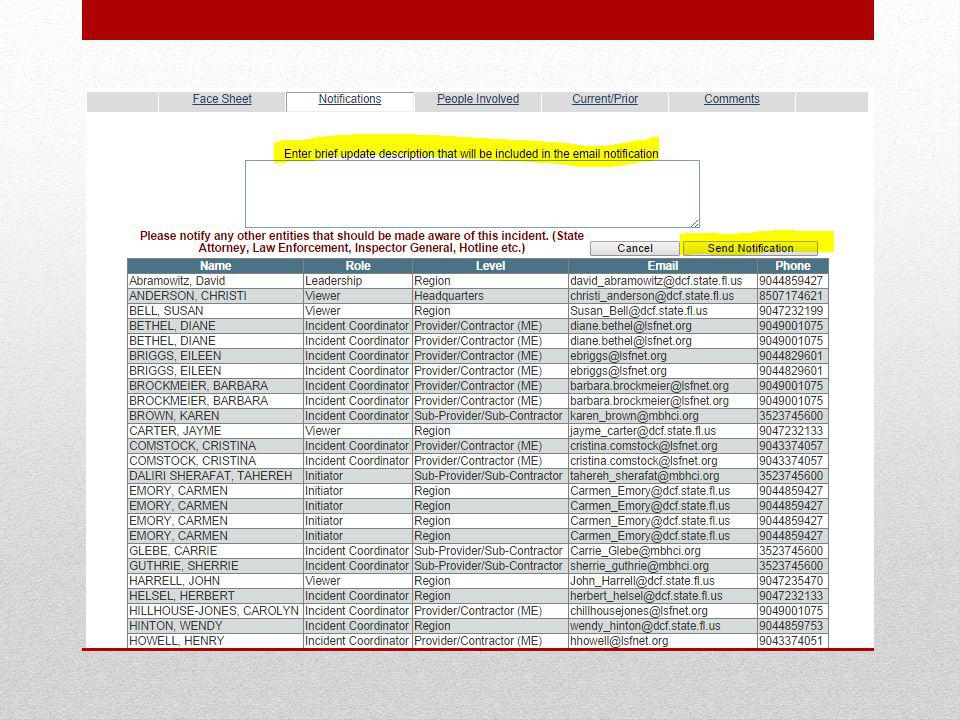
17
You will see a long list of names from your agency, DCF, LSF who received the notification. This means it was sent. IF YOU want to add new relevant information days later, you go to this page in NOTIFICATIONS, click on SEND UPDATE and type in comments in a box that will appear. Click on SEND NOTIFICATION box and the update will be sent to DCF/LSF/your agency.

19
Important Reminder Take action to ensure the health, safety and welfare by all individuals involved in an incident. THIS IS NUMBER ONE Contact law enforcement or emergency responders when appropriate, and/or the Florida Abuse Hotline. THEN follow IRAS procedures that your facility and the M.E. have established. (Remember, within 24 hours of incident) OK, enough technical instruction – I am available to help you with any questions as you enter a report, call me please! This slide is to take a step back to remind everybody that your first priority when a critical incident occurs is to ensure the health, safety and welfare of any consumers involved in a critical incident or observing one on-site. This should be written into every INCIDENT REPORTING policy and procedure.
 OK, enough technical instruction – I am available to help you with any questions as you enter a report, call me please! This slide is to take a step back to remind everybody that your first priority when a critical incident occurs is to ensure the health, safety and welfare of any consumers involved in a critical incident or observing one on-site. This should be written into every INCIDENT REPORTING policy and procedure.")
20
Reportable Critical Incidents
Adult Death years or older consumer whose life ends while receiving services or when it is known that an adult died within 30 days of discharge or last treatment / visit / service received. Manner of Death. Suspected Overdose. Seclusion and Restraint – IRAS will prompt you for all of these. Answer as they apply. There are 15 categories of INCIDENT TYPES. … we are going to go over all of them. First up are ADULT DEATH and CHILD DEATH.

21
Adult and Child Deaths Natural expected, NATURAL UNEXPECTED Accident – a death due to the uNINtended actions of one’s self or another Homicide – A death due to the deliberate actions of another Suicide – The intentional and voluntary taking of one’s own life Undetermined – the manner of death has not yet been determined Unknown – The manner of death was not identified or made known Child Death is under 18 years old. The system will prompt you on Manner of Death for adult and child death. While the final classification of an adult’s death is determined by the medical examiner, in the interim, the manner of death will be reported as one of these. Let’ see how the dropdowns look in IRAS. Next slide.

22
What happens if the official Medical Examiner ruling weeks later says a death you initially reported as UNDETERMINED was a SUICIDE? Can we go back in and change it in IRAS? NO. But let me know, and I can change it internally for the M.E.’s data trending reports. As you may guess, the most common manners of death entered in IRAS are Undetermined and Unknown.

23
More Dropdowns for Deaths
Suspected Overdose Non-prescription – illicit Prescribed – methadone Prescribed – buprenorphine (suboxone) Other – an overdose not mentioned above Unknown Drug Is Death Related to Seclusion or Restraint? Yes should be checked if any of these circumstances applies: Death occurs while a person is restrained or secluded Within 24 hours of release from seclusion or restraint Within one week after seclusion or restraint where it is reasonable to assume it contributed directly or indirectly to consumer’s death. You can also provide additional information about the death in comments at the end of your report in IRAS More Dropdowns for Deaths
 Other – an overdose not mentioned above. Unknown Drug. Is Death Related to Seclusion or Restraint Yes should be checked if any of these circumstances applies: Death occurs while a person is restrained or secluded. Within 24 hours of release from seclusion or restraint. Within one week after seclusion or restraint where it is reasonable to assume it contributed directly or indirectly to consumer’s death. You can also provide additional information about the death in comments at the end of your report in IRAS. More Dropdowns for Deaths.")
24
FAQ’s provided by the Department of Children and Family Services
Death Q: Are methadone clinics required to report the death of an individual receiving outpatient methadone maintenance? A: Yes, all Substance Abuse providers that are licensed by the State are required to report in IRAS. I’ve included in this PowerPoint Frequently Asked Questions compiled by DCF’s lead state IRAS official. They speak to several scenarios many of you have asked about.. FAQ’s provided by the Department of Children and Family Services

25
Death Q: Do the managing entities (MEs) have the right to access records on non-Department clients? A: No, ME's cannot access non-DCF funded client information. If a non-DCF client is receiving services at a facility and there is an incident involving that individual, the Licensed Substance Abuse Provider would have to enter the incident report, but they would NOT release non-DCF funded client information to their ME. Summary: Enter all SA critical incidents into IRAS. Enter Lutheran Services Florida when it is a state-funded consumer. For non-DCF consumers, pull down to your agency’s name for Provider and Subcontractor. For MH critical incidents, report to Lutheran for DCF-funded consumers. Do not report at all into IRAS for non-DCF consumers unless there is media coverage of the event. Do NOT enter names or PHI for these special cases.) KEY DIRECTION HERE: What this means is that for a consumer whose SA treatment is being funded by Medicaid or another insurer, they would report into IRAS but not pull down to Lutheran Services Florida at the PROVIDER/ME/SUBCONTACTOR dropdown. You would pull down to your provider name a second time. For MH consumers, only incidents with DCF payees are reported. EXCEPT for any incident that has media involvement. Report on those and pull down to your agency’s name twice.
 have the right to access records on non-Department clients A: No, ME s cannot access non-DCF funded client information. If a non-DCF client is receiving services at a facility and there is an incident involving that individual, the Licensed Substance Abuse Provider would have to enter the incident report, but they would NOT release non-DCF funded client information to their ME. Summary: Enter all SA critical incidents into IRAS. Enter Lutheran Services Florida when it is a state-funded consumer. For non-DCF consumers, pull down to your agency’s name for Provider and Subcontractor. For MH critical incidents, report to Lutheran for DCF-funded consumers. Do not report at all into IRAS for non-DCF consumers unless there is media coverage of the event. Do NOT enter names or PHI for these special cases.) KEY DIRECTION HERE: What this means is that for a consumer whose SA treatment is being funded by Medicaid or another insurer, they would report into IRAS but not pull down to Lutheran Services Florida at the PROVIDER/ME/SUBCONTACTOR dropdown. You would pull down to your provider name a second time. For MH consumers, only incidents with DCF payees are reported. EXCEPT for any incident that has media involvement. Report on those and pull down to your agency’s name twice.")
26
Death Q: Does reporting deaths apply to individuals who die while receiving outpatient services? A: Yes, if they are receiving outpatient services you would report their death (just as you would if they were receiving inpatient services). The difference between the two is that you would report the death of a client that left a residential program if they died within 30 days of leaving the residential program. The day a client discharges or walks out of outpatient services, you no longer have to report. Continue to submit reports of deaths of clients actively receiving outpatient care -- in between sessions or even after a phone call was made regarding a no-show in the last 30 days. If your agency DISCHARGES that client, and you learn they have died by whatever manner in the next 30 days, this clarification from DCF clearly states do not enter in IRAS.
. The difference between the two is that you would report the death of a client that left a residential program if they died within 30 days of leaving the residential program. The day a client discharges or walks out of outpatient services, you no longer have to report. Continue to submit reports of deaths of clients actively receiving outpatient care -- in between sessions or even after a phone call was made regarding a no-show in the last 30 days. If your agency DISCHARGES that client, and you learn they have died by whatever manner in the next 30 days, this clarification from DCF clearly states do not enter in IRAS.")
27
Death Q: If a provider hears a rumor of a death, what responsibility, if any, do they have for investigating or verifying the rumor? A: While they are receiving outpatient services, you are responsible for reporting a client's death. Most likely after a staff member receives information that a current client has died, "confirmation" would come from some type of case management follow-up; with a phone call or contacting the medical examiner.

28
Death Q: Is there a time limit beyond which a death should not be reported? A: Document the death of a current client receiving inpatient or outpatient services. If a client receiving residential services dies within 30 days of discharging from services, document it. If a client dies after receiving outpatient services, do not document.

29
Child-on-Child Sexual Abuse
Any sexual behavior between children which occurs without consent, without equality, or as a result of coercion. This applies only to children receiving services from the Department or by a licensed contracted provider. For example: children in foster care placements or in residential treatment. Child-on-Child Sexual Abuse

30
Child on Child Sexual Abuse
Q: Does this apply to SAMH case management services? A: This applies to any child receiving services.

31
Child on Child Sexual Abuse
Q: Does this apply to SAMH outpatient services in general? A: This applies to any child receiving services.

32
Child on Child Sexual Abuse
Q: If abuse is alleged, does it need to be determined whether it actually occurred in order to report under this category? A: Currently the way IRAS is set up as a notification system, you would enter allegations. You could enter follow-up information as soon as you receive it, indicating whether or not allegations were confirmed.

33
Child on Child Sexual Abuse
Q: Is it possible for a minor to consent to sexual activity, as applicable to this definition? A: As a minor they cannot consent to sexual activity.

34
Child on Child Sexual Abuse
Q: Is this limited to children receiving services from the Family Safety program? A: This applies to any child receiving services.

35
CHILD ARREST 5b. The arrest of a child in the custody of the Department

36
Child Arrest Q: Does this apply to children in the custody of other agencies, such as DJJ, who are receiving SAMH services? A: Yes, if they are receiving any services from SAMH and get arrested a report needs to be entered into IRAS.

37
Child Arrest Q: What is meant by "custody of the Department?" A: A child who has been adjudicated as dependent.

38
The unauthorized absence beyond four hours of an adult during involuntary civil placement within a Department-operated, Department-contracted or licensed provider The unauthorized absence of a forensic client on conditional release in the community Unauthorized absence of any individual in a Department contracted or licensed residential SA and/or MH program I want to share a helpful tip : while in the IRAS system, definitions of each critical incident exist for you to refer to – click on the question box next to the INCIDENT TYPE on the first screen. Here is a big one: ELOPEMENTS. Several guidelines surround this category. And I’ve got some big clarification for you today. Elopement

39
Elopement Q: Can a minor consent to leaving AMA or is this automatically elopement? A: A minor cannot consent.

40
Voluntary clients in residential have the right to leave treatment against medical advice. Do not report. UNLESS they leave/disappear from the facility without notifying any one, when there has been no intervention or AMA discharge process. Or, for example, if a client deviates during a medical appointment and does not return to the campus. Court-ordered (diversion sentencing) or Marchman Act involuntary clients in residential who leave AMA must be reported into IRAS regardless of the funding source. Remember, pull down to Lutheran Services for a DCF-funded consumer; pull down to your agency’s name twice if non-DCF. AMA vs. Elopement
 or Marchman Act involuntary clients in residential who leave AMA must be reported into IRAS regardless of the funding source. Remember, pull down to Lutheran Services for a DCF-funded consumer; pull down to your agency’s name twice if non-DCF. AMA vs. Elopement.")
41
Elopement Q: How would we define a client absent in the community? Does this include outpatient? A: Don't track outpatient clients if they don't show up, they are free to roam. However, if you were concerned for someone such as an elderly person, you need to follow up with them.

42
“Missing Child” as identified in CFOP 215-6
i. Missing Child. When the whereabouts of a child in the custody of the Department are unknown and attempts to locate the child have been unsuccessful.

43
Missing Child Q: What is meant by "custody of the Department?" A: A child that has been adjudicated as dependent.

44
Missing Child Q: How long does a child have to be missing before they must be reported as missing? A: If a child in a residential program is thought to be missing, report it immediately after you have searched the facility and determined the child is in fact missing.

45
Missing Child Q: Does this include all children receiving services? (E.g., outpatient services?) A: No, this incident type refers to children receiving residential services (or a similar type of placement), not for outpatient.
 A: No, this incident type refers to children receiving residential services (or a similar type of placement), not for outpatient.")
46
ESCAPE – The unauthorized absence of a client who is committed by the court to a state mental health treatment facility.

47
“Employee Arrest” as identified in CFOP 215-6
f. Employee Arrest. The arrest of an employee of the Department or its contracted or licensed service providers for a civil or criminal offense.

48
Employee Arrest Q: How is this different from “g. Employee misconduct?” A: If an employee is arrested, enter a report in IRAS under "Employee Arrest.” Although this could be considered employee misconduct, it should be entered as an Employee Arrest.

49
Employee Arrest Q: Does this apply to all employees or only those who qualify for a Level 2 Background screening? A: This applies to all employees.

50
Employee Arrest Q: What does "civil" mean? A: It means that the person was not charged with a criminal act. Civil involves legal remedies - such as injunctions etc.

51
“Employee Misconduct” as identified in CFOP 215-6
g. Employee Misconduct. Work-related conduct or activity of an employee of the Department or its contracted or licensed service providers that results in potential liability for the Department; death or harm to a client; abuse, neglect or exploitation of a client; or results in a violation of statute, rule, regulation, or policy. This includes, but is not limited to, misuse of position or state property; falsification of records; failure to report suspected abuse or neglect; contract mismanagement; or improper commitment or expenditure of state funds.

52
Employee Misconduct Q: Does this include any alleged incident or only those somehow verified to have occurred? A: Report the alleged incident and follow up with verified information.

53
Employee Misconduct Q: Regarding "policy" does this include DCF policy, provider policy, both or neither? A: In CFOP 215-6, under "Employee Misconduct", the term "Policy" refers to DCF Policy.

54
“Sexual Abuse/Sexual Battery” as identified in CFOP 215-6
k. Sexual Abuse/Sexual Battery. Any unsolicited or non-consensual sexual activity by one client to another client, a DCF or service provider employee or other individual to a client, or a client to an employee regardless of the consent of the client. This may include sexual battery as defined in Chapter 794 of the Florida Statutes as “oral, anal, or vaginal penetration by, or union with, the sexual organ of another or the anal or vaginal penetration of another by any other object; however, sexual battery does not include an act done for a bona fide medical purpose.” This includes any unsolicited or non-consensual sexual battery by one client to another client, a DCF or service provider employee or other individual to a client, or a client to an employee regardless of consent of the client. We’ll look at a few FAQs from the Department on this, and please know that I am waiting for clarification about on-site vs off-site in this category. Several of you have asked about this and I have forwarded the question to Tallahassee.

55
Sexual Abuse/Sexual Battery
Q: Are all allegations included or only those that are somehow substantiated? A: Currently the way IRAS is set up as a notification system, you would enter allegations. You could enter follow-up information as soon as you receive it, indicating whether or not allegations were confirmed.

56
Sexual Abuse/ Sexual Battery
Q: Are incidents prior to provider involvement included in IRAS reporting? A: There is no time frame for this, however, incidents that occurred 1 year ago, 2 years ago or 10 years ago do not need to be reported in IRAS. Clients may disclose being sexually assaulted in their intake assessment or in a therapeutic session, which is an appropriate time to be disclosed. However, if it has happened since they have been receiving services, it needs to be reported. If that is the reason they are receiving services, it needs to be reported.

57
“Suicide Attempt” as identified in CFOP 215-6
n. Suicide Attempt. A potentially lethal act which reflects an attempt by an individual to cause his or her own death as determined by a licensed mental health professional or other licensed healthcare professional.

58
Suicide Attempt Q: What if it’s a drug overdose and we don't know whether it was deliberate? A: If you have credible evidence from which one could conclude that this was a suicide attempt, then document it as such. If there is not sufficient evidence that suggests a suicide attempt, but the client had to be taken to the hospital for immediate medical attention due to the overdose, then you would document the incident as a significant injury to client.

59
“Significant Injury to Clients” as identified in CFOP 215-6
Significant Injury to Clients. Any severe bodily trauma received by a client in a treatment/service program that requires immediate medical or surgical evaluation or treatment in a hospital emergency department to address and prevent permanent damage or loss of life.

60
Significant Injury to Clients
Q: What is meant by "serious?" Is it interchangeable with "severe?” A: An injury that causes great discomfort, damage, or distress, one that's serious, dangerous or harmful.

61
Significant Injury to Clients
Q: Does this include medication errors? A: Yes I read this as the Medication Error must have caused damage and is dangerous in its dose and harmful effects.

62
Significant Injury to Clients
Q: Is there a distinction between inpatient and outpatient? A: No Keep in mind within 30-day of service timeframe

63
“Significant Injury to Staff” as identified in CFOP 215-6
M. Significant Injury to Staff: Any serious bodily trauma received by a staff member as a result of work-related activity that requires immediate medical or surgical evaluation or treatment in a hospital emergency to prevent permanent damage or loss of life.

64
“Security Incident - Unintentional” as identified in CFOP 215-6
J. Security Incident - Unintentional: An unintentional action or event that results in compromised data confidentiality, a danger to the physical safety of personnel, property or technology resources; misuse of state property or technology resources; and/or denial of use of property or technology resources. There is more action to be taken for potential HIPAA breaches of consumer information. Stemming from a new operating procedure in Florida. Today we’ll look at it. It’s fairly straightforward.

65
Establishes a uniform process for notification to the state’s HIPAA Privacy Officer, Office of Civil Rights Suspected or known breach is reported as soon as possible, in addition to submitting an IRAS report Call Privacy Officer at (850) Complete HIPAA - Privacy or Security Incident Reporting Form (available from DCF Forms on its web site) and fax to (850) The Office of Civil Rights’ Privacy Officer will review and may ask you to fill out a Risk Assessment to gauge the risk of compromise. This Office and LSF will guide you on breach notification requirements pursuant to the Florida Information Protection Act of 2014. Simple process, and very important. I have copies of these forms if you can’t locat e them. Let me know and I can you in an attachment. Can anyone on the call name some examples of potential security breaches that you have self-reported? (I can name some if they can’t.) Lost and stolen work cell phones, laptops, burgled clinics with unlocked file cabinets with consumer charts etc. The office will decide if a locked screen is a low or high risk and if consumers should be notified. Training can help by reminding staff about policies of not leaving laptops in cars, or office keys in unsecure spots. CFOP 60-17, Chapter 7 January 6, 2014
 Complete HIPAA - Privacy or Security Incident Reporting Form (available from DCF Forms on its web site) and fax to (850) The Office of Civil Rights’ Privacy Officer will review and may ask you to fill out a Risk Assessment to gauge the risk of compromise. This Office and LSF will guide you on breach notification requirements pursuant to the Florida Information Protection Act of Simple process, and very important. I have copies of these forms if you can’t locat e them. Let me know and I can you in an attachment. Can anyone on the call name some examples of potential security breaches that you have self-reported (I can name some if they can’t.) Lost and stolen work cell phones, laptops, burgled clinics with unlocked file cabinets with consumer charts etc. The office will decide if a locked screen is a low or high risk and if consumers should be notified. Training can help by reminding staff about policies of not leaving laptops in cars, or office keys in unsecure spots. CFOP 60-17, Chapter 7 January 6,")
66
“Other” as identified in CFOP 215-6
o. Other. Any major event not previously identified as a reportable critical incident but has, or is likely to have, a significant impact on client(s), the Department, or its provider(s). These events may include but are not limited to: (1) Human acts that jeopardize the health, safety, or welfare of clients such as kidnapping, riot, or hostage situation; (2) Bomb or biological/chemical threat of harm to personnel or property involving an explosive device or biological/chemical agent received in person, telephone, in writing, via mail, electronically, or otherwise; (3) Theft, vandalism, damage, fire, sabotage, or destruction of state or private property of significant value or importance; (4) Death of an employee or visitor while on the grounds; (5) Significant injury of a visitor (who is not a client) while on the grounds of the Department or one of its contracted or licensed providers; or, (6) Events regarding Department clients or clients of contracted or licensed service providers that have led to or may lead to media reports. Name some others: positive TB testing of staff or clients in residential; closure of building, bug infestation, anything that falls outside of the other categories and is major.
, the Department, or its provider(s). These events may include but are not limited to: (1) Human acts that jeopardize the health, safety, or welfare of clients such as kidnapping, riot, or hostage situation; (2) Bomb or biological/chemical threat of harm to personnel or property involving an explosive device or biological/chemical agent received in person, telephone, in writing, via mail, electronically, or otherwise; (3) Theft, vandalism, damage, fire, sabotage, or destruction of state or private property of significant value or importance; (4) Death of an employee or visitor while on the grounds; (5) Significant injury of a visitor (who is not a client) while on the grounds of the Department or one of its contracted or licensed providers; or, (6) Events regarding Department clients or clients of contracted or licensed service providers that have led to or may lead to media reports. Name some others: positive TB testing of staff or clients in residential; closure of building, bug infestation, anything that falls outside of the other categories and is major.")
67
Other Q: If an incident is reportable to the Abuse Hotline, but doesn't fall into the definition of any IRAS critical incident, should it be reported as other? A: Without knowing specific examples, it is difficult to answer this question; however, if the incident is likely to have an impact on the client, provider and/or Department, report it.

68
Other Q: Should reports that clients have brought drugs into a residential facility be reported as OTHER? A: Yes

69
Other Q: What is meant by "significant impact?" A: If the event/incident posed any threat, harm or elevated concern for the client, provider and/or Department, report the incident.

70
Other Q: Regarding media reports, if a provider is mentioned in an article, but it's not problematic in any obvious way, is that reportable? A: No

71
Quality Improvement Is Ongoing. It Never Ends.
OK, that is enough from me. That was more information than I thought it would be. Any QUESTIONS? I hope you find this helpful in your training of other staff members also. Thank you for participating today. For support, LSF Continuous Quality Improvement Specialist Bryan Mingle at or call direct at Quality Improvement Is Ongoing. It Never Ends.

Similar presentations

![Critical Incident Reporting System [CIRS] Other Incidents A/N/EFraud.](/2/758026/big_thumb.jpg "Critical Incident Reporting System [CIRS] Other Incidents A/N/EFraud.>")









 VUMC Privacy Website www.mc.vanderbilt.edu/privacy.>")







